
Abstract
Background:
Advance care planning can improve patient and family outcomes; however, minoritised ethnic communities experience access barriers. Co-production offers a way to design culturally appropriate information and support, but evidence is needed to understand its implementation in palliative care.
Aim:
To explore and describe how two charities used co-production to develop and deliver community-based advance care planning workshops for South Asian elders.
Design:
Workshops were co-produced by two charities. In parallel, a multi-component qualitative study was conducted comprising workshop observations, semi-structured interviews with charity staff and focus groups with workshop participants, facilitated by community co-researchers in English, Hindi, Urdu and Punjabi. Data were analysed using thematic analysis.
Setting/participants:
Four workshops were held in a London (UK) community setting (each with 5–30 participants); four interviews were conducted with charity staff members, and three focus groups with 16 workshop participants.
Results:
We describe three main themes: Co-production in action: organic origins and trusted foundations; Co-production processes embedded in equal partnership; and Impact of the workshops. Fundamental to co-production processes was the community-led approach of the local charity, the trust of the local South Asian community and the relationship between the charities, including transparent communication and mutual respect. The workshops were reported to be useful and enjoyable, engendering a sense of agency and connection and helped disseminate awareness and knowledge through the community, benefitting the wider system.
Conclusions:
Co-production can help widen access to advance care planning. Findings offer an in-depth example of co-production-in-action to inform intervention development and research.
Keywords
Co-production with community members can help widen access to information and support, design appropriate services and conduct appropriate research; however, there is little practical guidance on what co-production entails in palliative and end-of-life care.
Uptake rates for Advance Care Planning are low, especially for people from minoritised ethnic communities, who experience barriers to accessing information and resources.
Voluntary, community, faith and social enterprise organisations are sources of informational, psychosocial, cultural and emotional support for minoritised ethnic communities.
Using the example of advance care planning workshops co-produced with South Asian elders in a London (UK) borough, we identified key requirements of co-production, including flexibility, language skills and building and maintaining community trust; collaboration with a community organisation were essential to fulfilling these requirements.
The co-produced workshops responded to the expressed needs and preferences of South Asian elders, and led to knowledge gain, empowerment and raising local community awareness through cascading information.
South Asian elders wanted information in accessible, shareable, visual formats; short videos about advance care planning in community languages were co-produced as project outputs.
Co-production can reach and engage minoritised communities, enabling community members to receive information they want, in the way they want and widening access to information and support.
Co-produced research in palliative and end-of-life care can be achievable and effective; this study provides an exemplar which can inform future research.
Study findings, implications and recommendations can inform policy guidelines to ensure information is accessible in diverse ethnic communities and raise awareness of its utility and value.
Background
In recent years, the need to prioritise equity in palliative care and bereavement services (and the recognition that professional services are themselves implicated in creating access barriers 1 ) has led to calls for co-production approaches to adapt and improve access to formal support.2 –4 Co-production is defined in different ways, and there are debates about its value, power structures and who the key stakeholders are.5 –8 It is also at times poorly implemented; for example, its prioritisation of levelling power structures and fostering mutually beneficial agendas might be de-emphasised or neglected. 9 In this article we understand co-production as an approach that aims to work with ‘service users’ or members of a community in equal partnership and for equal benefit. In successful co-production, relationships are developed on the basis of close engagement and trust. Professional stakeholders (e.g. healthcare providers) work with members of specific communities to change how care and support are designed, offered and evaluated, 10 and ensure that power and responsibility are shared with community organisations and ‘service users’ in a collaborative, iterative process. 11 ‘Co-design’, sometimes formalised as Experience-based Co-design, is a component of co-production where multiple stakeholders work together to design solutions, for example to improve healthcare quality.12,13 In high income countries, health policy guidance now advocates a co-production approach,14,15 including in palliative care.16 –19
While often not explicitly labelled as such, pioneers in new public health approaches to end-of-life care and bereavement have been following co-production principles for decades. 20 However, with some exceptions,21 –23 there has been little attention to generating evidence of how to conduct meaningful co-production in palliative care. A review of co-design within palliative care services has highlighted the need to investigate ways to engage with people with lived experience and develop strategies to address key challenges. 24 Specific challenges include topic sensitivity, the emotional nature of personal experiences of illness and loss, the limited time and capacity of patients and caregivers and power imbalances. 22 Using co-production may create safe spaces and build trusting relationships, helping to overcome barriers; it may also build confidence by highlighting or foregrounding participants’ assets, 25 in contrast to deficit models which may contribute to people’s disenfranchisement. 26 Evidence of good practice in co-production in palliative care is therefore essential.
Advance care planning enables person-centred care, and is associated with increased care satisfaction among dying people27,28 and bereaved family members.29,30 However, uptake rates remain low internationally, especially for people from minoritised ethnic communities.31,32 Barriers to accessing advance care planning include lack of translation services and resources; perceptions of planning ahead; language; patients’, family members’ and clinicians’ discomfort talking about serious illness, death and dying; cultural taboos in specific groups; and clinicians’ pre-conceptions regarding or poor confidence engaging with cultural values.21,33 –38 Evidence suggests most advance care planning is medicalised, focussing on documentation rather than communication and broader discussions of ‘what matters most’, hindering engagement. Informal communication-focussed approaches to advance care planning (through facilitated discussions and community education) are more cross-culturally acceptable, 17 laying the foundations of death literacy 31 and potentially reducing unwanted hospital admissions. 39 For many people, voluntary and community sector organisations (including grassroots community groups) are crucial sources of psychosocial, emotional and practical support in serious illness.40,41 With high levels of understanding and reciprocal trust between established community organisations and community members, 42 they play a key role in community engagement with advance care planning education and discussion.43,44
This study’s research question was: what co-production processes and principles are used by a community-based organisation and a national charity to develop and deliver advance care planning workshops, resources and outputs for South Asian elders in a London (UK) borough? Its primary aim is to contribute to the evidence base on co-production in palliative care; a secondary aim is to inform methods to engage South Asian elders with advance care planning.
Methodology
We used a qualitative, exploratory approach, informed by social constructionism, 45 to describe the development, delivery and impact of four workshops on advance care planning for South Asian elders in London. The research study itself was co-produced with charity staff from partner organisations (TS/NA/SK/UG/VH) in order to ensure aims were appropriate, methods feasible, and outputs valuable. We followed COREQ reporting guidelines 46 and the Reflexive Thematic Analysis Reporting Guidelines (RTARG). 47 The timeline of the workshop development and delivery and data collection for the research study is available in the Supplemental material.
Setting
The setting was a single London borough (population 360,400 48 ), which included neighbourhoods in the most socio-economically deprived 10% in England. 49 Ethnic diversity is high (with 69.3% identifying as Asian, Black, Mixed or Other) and c.8% are 65 years+. 48 In 2020, the local council developed an ‘End-of-Life Care Strategy’ and established an ‘End-of-Life Care Board’ comprising stakeholders from the local voluntary and community sector, health and social care and local authority. 50
Advance care planning workshops
One of the collaborating organisations is a national charity helping people to prepare for the end-of-life through community-outreach and phone-based support with planning ahead, Advance Decisions and Advance Statements (National Org). The other collaborating organisation is a London-based charity aiming to improve the lives of vulnerable South Asian elders, their carers and the local community (Local Org). Local Org has a membership of approximately 250 South Asian elders, who are offered a range of services including meals, daytrips, social activities, health information provision, health advocacy and carer support.
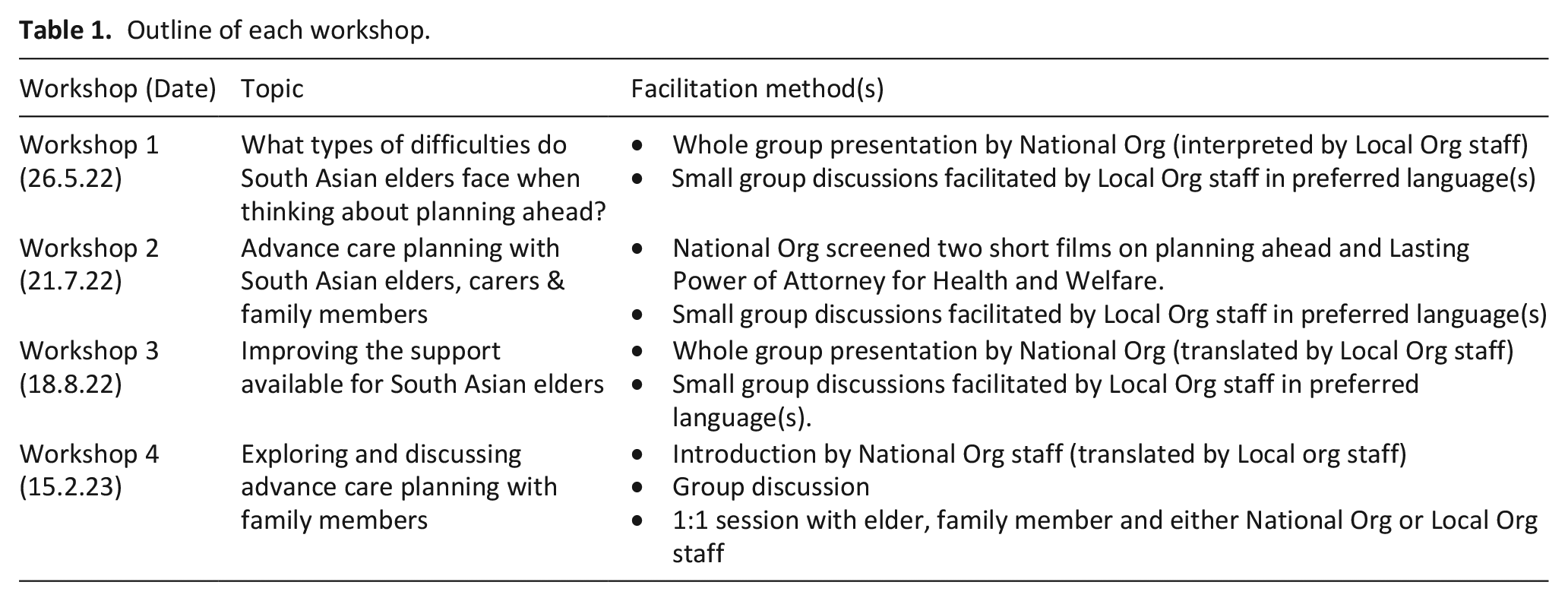
Over an 8-month period (May 2022–February 2023), staff from both organisations co-produced workshop content and materials for and with Local Org members (South Asian elders) about advance care planning. Four workshops took place during existing daycentre services at Local Org. Workshop duration ranged from 60 to 90 min, with attendance ranging from 12 to 30 elders (workshops 1–3) and 5 family members (workshop 4).
Two staff from the national charity (National Org), experts in advance care planning, delivered the training content in English. At the same time, co-author (NA), a British Pakistani female staff member at Local Org with 30 years+ experience of group facilitation, social and community work, interpreted content from English into attending elders’ preferred languages (Urdu/Hindi/Punjabi/Gujarati). Feedback was sought from the South Asian elders who attended at the end of each session and used to inform subsequent workshop development (Tables 1 and 2)
Outline of each workshop.
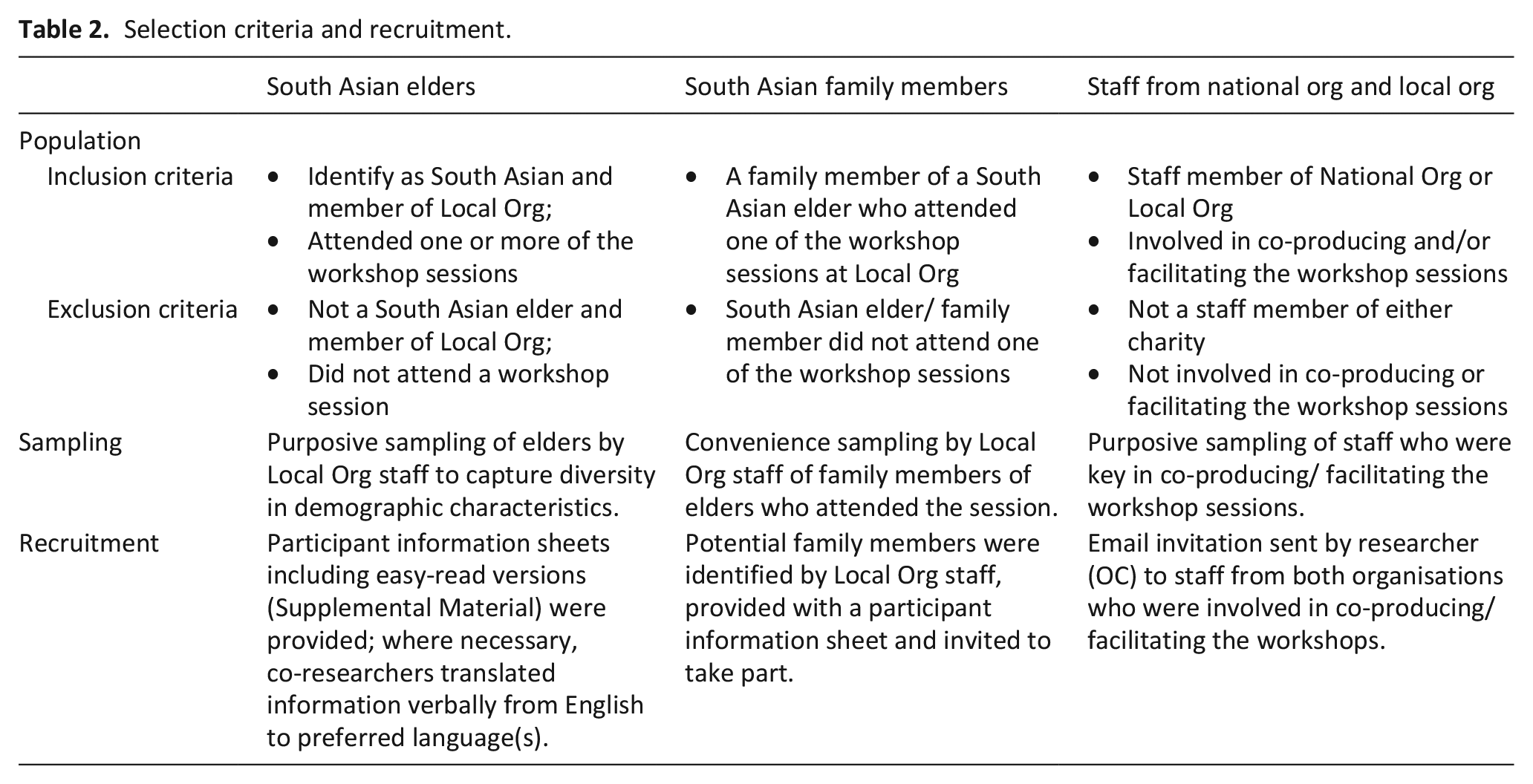
Selection criteria and recruitment.
Data collection
Our data collection methods comprised reflexive researcher fieldnotes, semi-structured interviews with staff involved in workshop development and delivery, and focus groups with workshop attendees conducted by trained community co-researchers. In collecting demographic data from focus group participants, we were guided by Local Org co-authors to ensure cultural sensitivity and minimise process burden.
Researcher fieldnotes were written in a reflective journal (OC), during/after workshops, visits to the centre and interviews.
Semi-structured interviews were conducted online by OC, an experienced health services and community researcher, between November 2022 and January 2024. The interview topic guide (Supplemental Material) was developed by the research team (including academic social scientists with expertise in palliative care and co-production and National Org/Local Org staff), based on study aims and the literature, and covered: community views and attitudes, the origin and design of the workshops, relationship between the organisations, reflections on the workshops and workshop development, delivery and impact. Interviews were digitally audio-recorded and professionally transcribed. Before analysis, transcripts were checked for accuracy and pseudonymised.
Focus groups
Two Local Org staff members were co-researchers in the study (NA/SK) and facilitated the focus groups in English, Hindi, Urdu and Punjabi between March and April 2023. Both were provided with approximately 3 h training and ongoing support (OC). Focus groups followed a topic guide developed for the study and covered expectations of the workshops, and reflections on the workshops, including their development and impacts (Supplemental Material). Focus groups were held at Local Org and digitally audio-recorded. Recordings were professionally transcribed and translated into English, and pseudonymised prior to analysis.
Ethical approvals were given by the Faculty of Health Science Research Ethics Committee at the University of Bristol (ref:11581). All participants provided written informed consent, with co-researchers translating consent forms verbally as needed.
Data analysis
We analysed all data using thematic analysis.51,52 Fieldnotes were analysed alongside the qualitative interview and focus group data to add context and aid interpretation. Interview transcripts were analysed first, with reading for familiarisation followed by initial coding (OC) before team development of a coding framework (LS/TS/OC) and application of the framework to all transcripts (OC). To analyse the focus group data, the co-researchers first listened back to the recordings and translated salient experiences and verbatim quotes, integrating these into anonymised written summaries sent to the academic team. Initial familiarisation was achieved through interrogation of these written summaries followed by multiple readings of each transcript, generating initial notes and codes(OC). The research team (LS/TS/OC) discussed preliminary codes and interpretations of the data, with a coding framework developed and refined as the analysis progressed, and applied by OC.
A combination of inductive coding (identifying themes from participant accounts) and deductive coding (based on the study aims) were used in creating the coding frameworks. Initial themes were then scrutinised and discussed by all co-authors. To add richness and context to findings, in later analytical stages, we compared codes generated inductively with several models of co-production identified in the literature.8,53,63 All co-authors reviewed and refined the narrative of findings. Nvivo12© software was used for data management. 54
Results
Sample
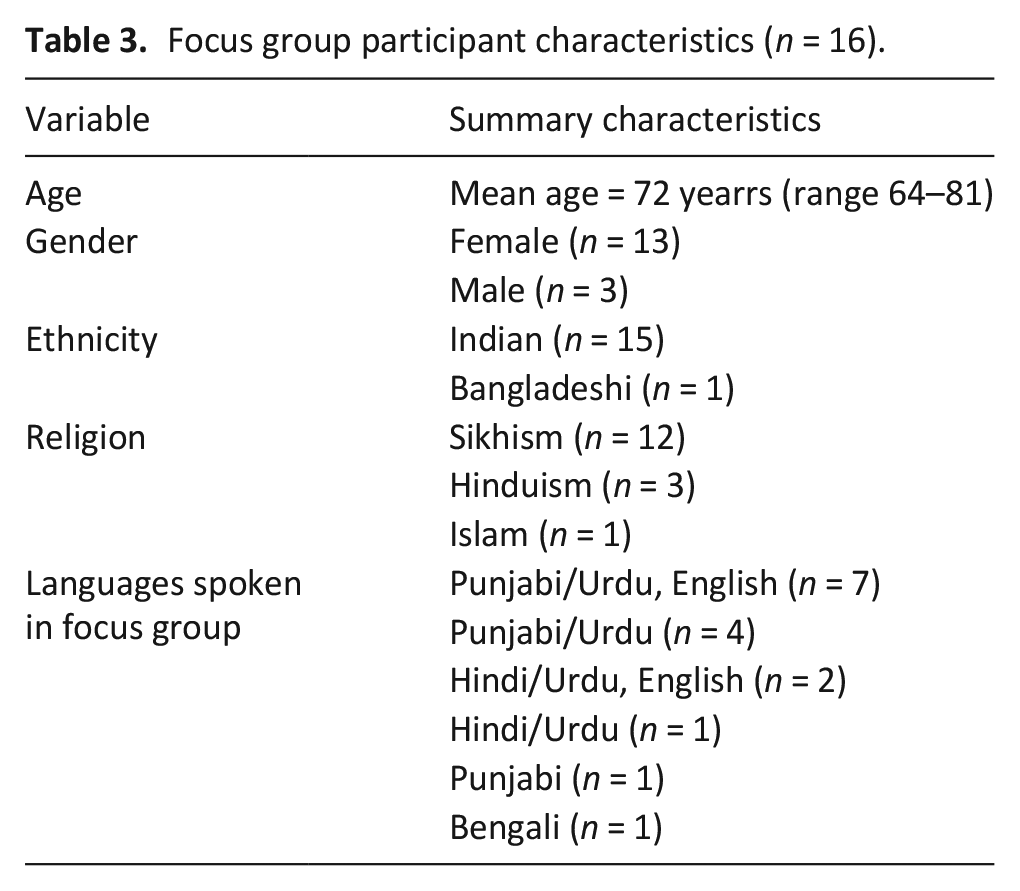
Four staff members were interviewed (two each from Local Org and National Org) and 16 South Asian elders took part in a focus group, with 4 elders attending more than one (Table 3). Interviews lasted 53–65 min (mean = 57 min); focus groups lasted 25–49 min (mean 35 min).
Focus group participant characteristics (n = 16).
Findings
We describe three main themes: 1. Co-production in action: organic origins and trusted foundations; 2. Co-production processes embedded in equal partnership; and 3. Impact of the workshops (personal, family and community; on collaborating organisations; on the wider system). Unique participant ID codes are used; P = interview participant; focus group participants’ gender (M = male/F = female) and focus group number (e.g. FG2) are indicated. Quotations were in English unless stated otherwise.
Co-production in action: Organic origins and trusted foundations
Workshops originated from the wishes of Local Org ‘members’ – the South Asian elders who accessed their service. Prompted by the pandemic, organic conversations arose between elders and Local Org staff about advance care planning and future wishes. Building on their prior relationship, both organisations collaborated to meet elders’ needs for information on advance care planning:
Because we’ve always done bits and pieces on and off with [National Org], it seemed quite opportune, and because we’re also working on quite a lot, in developing a video during Covid around advance planning that [Local Org] were involved in.
Essential to the project were long-standing relationships, respect and trust between elders and Local Org:
The staff are really engaged with their members and are, obviously, really well respected, and have such a good knowledge of them
[Hindi] You take care of everyone, cater to everyone according to their language [. . .] There’s Gujarati, Hindi, Urdu, English. You have staff that can help us.
These relationships were supported by Local Org’s integration of co-production principles into its working practices, which reflected inclusion, respect, engagement, flexibility, compassion, cultural sensitivity and a holistic, person-centred approach. Their ground-up methods included working with their members at every level, including management:
All the things that we do are based on what service users have told us, and that’s how we’ve developed our services. So, we have a strong input from service users on the management committee, I think over 95% are service users and over the age of sixty-five, the majority of whom actually are involved in day-to-day support groups or services [as] participants, but . . . some of them are mentors as well and provide peer support.
They also consulted their wider membership regularly via annual surveys and informal discussions, with this feedback leading directly to funding applications for specific projects. This structure and process meant they were held accountable:
So, it is really trying to be in tune, and because they are part of that decision-making process as well, you know, it works, I think. It’s not just rhetoric at the end of the day, we do what we say and we’re held accountable, yeah.
Members and their families appreciated that Local Org staff acted as trusted gatekeepers, advocating on their behalf and cascading information, with Local Org described as the only place they could get the information they needed:
[Urdu] But this care plan [. . .] the information about it, or how to fill it out, I mean, have you understood where you can find the information about it?
[Urdu] We get it from [Local Org].
[Urdu] It is available at [Local Org]
[Urdu] It isn’t available anywhere else, just here.
[Punjabi] We get everything here.
Information from external sources (e.g. National Org) is first vetted by Local Org. Aware of this, community members are receptive, deeming information shared to be useful and trustworthy, which helps mitigate a lack of trust arising from previous experiences of healthcare:
I think that a lot of the communities we work with have often, historically, had not very good experiences with healthcare [. . .] it takes a long time to build trust, as well, in terms of us as an organisation or our partner organisations.
Members’ trust was particularly important given the workshop subject matter:
The [Local Org] staff that were working with them, they already knew them, and so, I think confidentiality is a big thing, really, in the community, because you’re thinking, oh, well, if we say something, it’s going to get out into the wider community about this person’s life or that person’s life. But that didn’t actually happen. . . it was quite surprising that everyone was quite comfortable. . . the trust and the confidence was there right from the outset, really.
Local Org representatives discussed how the well-being of their members and staff was a priority and built in ways to ensure that their emotional support needs could be met:
We talk about what happened, how it happened, how we could support that individual, but also for staff and volunteers, it brings back memories and feelings as well, that can be quite emotional. So for them to know that they can talk about it in a safe environment as well. . . For members, it’s also then looking at who is the best person that can support that individual for that conversation, both language-wise, but also sometimes in terms of their experiences about that particular area. So, for instance, if it’s around cancers or dementia or stroke, so people understand the condition of what that person went through, and then the individual knows that [person] understands.
Trust between organisations was another essential foundation to the advance care planning workshops, built up over time:
It takes quite a long time to build that trust as well, and I think I said, because we’ve dipped out and we had another project before, you know, they’ve come in and they’ve done things with us, they know some of the staff team, they know some of the service users and they know how we work, and vice versa, and it’s been a symbiotic relationship really, yeah.
Successful collaboration between organisations depended on staff members’ relationships and mutual trust. Key factors sustaining their relationships were awareness of how each organisation operates; transparent communication; openness; and mutual respect of knowledge, skills and strengths:
I think it is the openness, the friendliness, being available, having regular meetings and being listened to [. . .] normally it’s when people don’t say anything or are very aggressive that things fall apart, and then I think we always talk about this critical friend, but critical constructive friend is my new phrase now [. . .] each has their own strengths and we’re learning from each other all the time, and if you’re in the position where “We’re still learning” rather than “We know it all”, I think that just makes such a big difference for both partners really.
Co-production processes embedded in equal partnership
Co-production with South Asian elders was integrated into the way the advance care planning workshops were developed, ensuring they were tailored and responsive to elders’ needs. After each workshop, National Org staff created summary notes and sent these to Local Org staff to check accuracy, clarify and add detail. Notes included detail of the topics covered, and questions and responses from workshop attendees, including participants’ suggestions or requests for future topics and workshops. The two organisations used these notes to co-design subsequent workshops. A participant from Local Org reflected on how the allocation of tasks between the organisations demonstrated equal partnership:
Having [National Org staff member] there who then writes up everything, and it’s not [us] who’s having to do that, so it’s [National Org] who’s taking away the information from the focus groups, and all the flipchart notes and the, you know, sticky notes, and putting it into themes and writing it up. That’s been really good, because again, that is very time consuming. So, we’re doing the very practical stuff and they’re doing the more administrative stuff as well as helping us to deliver the workshops.
The co-production process ensured elders’ views and preferences shaped the workshops. For example, elders expressed concerns regarding communicating with family members about end-of-life topics:
[Punjabi] They would start crying, they would walk out, then I would be left alone. I would think, ‘how do I get them to understand?’ Then I took the [ACP] form from here.
In response, a session for family members was developed, attended by five family members. The workshop provided elders with resources and gave them skills to broach advance care planning with their children:
[Punjabi] The kids would tell us, “no, no, no”. They would say themselves, “no”. So, when we did the workshop, we also got to know a little bit. We also went and told them a few things. They were still saying, “no, no, no”. [English] But I think it’s very important [Punjabi] that whatever information is given, take that home on paper. What is on paper, show it to them. “These are leaflets, read them”. So that they understand thoroughly.
The format of the workshop was also informed by elders’ preferences. Sessions started with a recap and combined in-person didactic presentations with one-to-one and group discussion:
We kind of followed up as well. So, we would say, “well, last time we spoke about this, and people said X, Y, Z, now we’re looking at this.” So, they knew there was like, a sequence, you know? Sometimes you go “we spoke about something” and they’ve probably half-forgotten, but just recapping and then following up in the next workshop helped them to remember what happened last time or what we spoke about. So, “do you remember we said this?” That was quite important, just reminders, recaps, and continuous conversations.
Face-to-face information – I can see the person, I can explain properly face-to-face, you can see facial expressions/body language – we can remember this better.
Using visual methods and interactive sessions and providing flexibility in terms of attendance also reflected elders’ needs. Local Org staff described how engaging, entertaining and creating community among members was fundamental to all their work:
Part of the session is pure information. . . developing skills around whether it’s long-term conditions, whether it’s around dementia, whether it’s about end-of-life care, whether it’s something that’s happening in the local authority or the health services that we think they should know about. And the other part of the time is about. . . fun, being able to talk, to chat, to sing, to dance, be creative. . . We have a calendar of activities. . . people can dip in and dip out.
Concurrent interpretation from English into preferred languages by Local Org staff meant elders could immediately access content presented by National Org staff and ask questions:
[Urdu] I think they [National Org staff] listened to us. Not sure how much understanding they had from our side. But what they told us, you [Local Org staff] would explain to us all, in your own words. So, we understood what it was.
Having a trusted translator/simultaneous interpreter is essential if the session is to be productive and meaningful.
This process helped to foster a positive atmosphere, that allowed workshop participants to be engaged and enthusiastic:
The members are, I mean, you saw for yourself, just always ready to engage, and always have a lot to say.
I’m always just totally in awe of how up for being open about all of this [Local Org] members are.
Impact of the workshops
Personal, family and community impact
Elders enjoyed hearing and learning about advance care planning, which was a new topic for most. The workshops stimulated conversations between sessions and some members pursued formal care planning:
People talking about it in smaller groups, in other group sessions, and asking questions as well. Not necessarily on the day when we had the workshops/focus groups, but on different days, throughout the weeks and months ahead.
[Urdu] It was useful. Got to learn a lot. Then our minds also changed, about what to do. We thought about it, and also acted on it.
Participants gained valuable knowledge which facilitated their own thinking about end-of-life issues, enhanced sense of agency and enabled them to consider, express and document future care preferences:
[Urdu] Earlier we did not know what it is. And now that we know, it feels good doing something for ourselves. If we plan ahead, then our children will also not have any problem. And the doctors will also not have any problems as what we say, they will only do that [advance care planning]. So, it will be better. Sometimes there is a problem regarding religion, sometimes. . . there is a problem regarding food. If we sort it out, then it would be better.
Participants benefited from discussion with peers during workshops, which enabled different views and experiences to be shared, as discussed in FG1:
[Punjabi] Now we can talk to each other, whereas before we could not. . . we’d say, “Forget it, who knows why they are talking [about] all this information. . .” But now, we get to know, that we should sit together and discuss.
[English] Good experience.
[Punjabi] Also we become aware of another person’s problem, and how they solved it.
[Punjabi] Everyone pays attention.
Impact rippled outwards beyond the immediate workshop setting into the wider community. As described during FG2, newly acquired knowledge and awareness about advance care planning was shared with friends, family and neighbours:
Impact on collaborating organisations
Both organisations gained insight to inform the development of new resources. Elders reported challenges accessing advance care planning due to format or language, often relying on others to translate information:
To overcome barriers, alternative formats were suggested such as voice recordings or videos that could be shared with healthcare professionals, family members and between community members (e.g. via WhatsApp, which was flagged as major communication channel):
Short videos really help to convey key messages.
[Punjabi] You can talk in your own tongue. If there is no video, we can record audio.
As a result, the organisations and elders co-produced two short information videos on advance care planning in South Asian languages, promoting accessibility of information for others:
Thinking about videos, if we had a link, we could send it to people. We have a WhatsApp group for our Thursday group. So, I was thinking, if we put the link on there, that’s quite simple. They can just tap on the link and then it’s in a community language, then they would understand the information. They can listen, hear the information, rather than actually reading any information, because like I said, not everyone can read.
Impact on the wider system
The borough’s End-of-Life Care Board provided opportunities to cascade learning and benefit the local community:
[. . .] And they’re [End-of-Life Care Board] asking us sometimes as [Local Org] to come and share in community learning sets about what we’re doing, how we’re doing it and why we think we’re successful in certain areas, and how we’ve met some of those challenges, and then what is left to learn about and how we work together.
The co-produced videos were designed as collective community resources to complement existing local initiatives:
I think [name] has mentioned that as well. Saying how it’s feeding into the wider work of [borough], generally, around advance care planning, and how it benefits other communities.
However, barriers to embedding this work were acknowledged. Interviewees described how community projects often took place in isolation, restricting impact and highlighted a need for better alignment between local stakeholders across sectors to bring about culture change and community action:
If there’s no major shift within systems, and the embedding side of things, I worry that that kind of culture change isn’t going to happen. I’m hoping that, at the end of the year, advance care planning will be much more on people’s radars, and people will be much more open to having conversations.
There’s a big job of work to do in terms of medical culture and getting to the point where people are supported in the right way to have conversations.
To achieve wider impact in the community and across sectors, mutual respect, transparency and a shared vision of working collaboratively to improve end-of-life care were seen as critical:
I do think that as a sector, sometimes people can be unhelpfully proprietary, and so our ultimate aim is to shift culture towards one where people understand more their rights to make decisions and plan ahead, and so, however that happens, we’re happy with that [. . .] If that means people adopt our messaging and use it as their own, fine. Ultimately, the more people doing it, the better.
Discussion
Main findings
This study represents one of the first in-depth examinations of community co-production in practice in UK palliative care. Fundamental to the co-production process was the ground-up, community-led approach of the local organisation and its established relationship with the local South Asian community. South Asian elders directed the content and format of sessions, which involved concurrent interpreting and the opportunity for small group and one-to-one discussions; this helped to create a safe environment where elders could be engaged and responsive. Equally important was the relationship between the community-based organisation and the national organisation with subject expertise in advance care planning: time, transparent communication and mutual respect were key. The co-production process involved note-taking at each workshop, with reflection to design the content and format of subsequent workshops and video outputs. These tasks were shared equitably between the two organisations.
South Asian elders reported that the workshops were useful and enjoyable and that they engendered a sense of agency and connection. New awareness and knowledge of advance care planning were disseminated through friends, family and neighbours, indicating organic, longer-term community impact. Collaborating organisations received valuable information to develop advance care planning resources and educational sessions for South Asian communities. Workshop participants recommended the development of videos, shareable via WhatsApp and the organisations co-produced two such videos as part of this project. In the wider system, the borough’s local End-of-Life-Care Strategy enabled sharing of learning and integration of outputs in existing initiatives. However, barriers to achieving meaningful system change were highlighted, including the need for better cross-sector collaboration.
What this study adds?
Given the growing focus on co-production as a method of improving service delivery and design, 18 the need for co-production case studies and ‘live examples’ of effective strategies has been highlighted.55 –62 Our findings offer practical guidance in co-production, adding to the emerging literature on involving stakeholders and public contributors in palliative and end-of-life care. 62 The topic sensitivity and previous experiences of discriminative interactions with healthcare meant that trust, confidentiality and prioritisation of well-being (among both elders and staff) were particularly important. This highlights the importance of psychological safety, which is rarely discussed as a core principle in healthcare co-production, but has received attention in the development of trauma-informed approaches. 63 Local Org’s organisational structure and working practices provided the ‘involvement-friendly organisational culture’ identified in Chambers et al.’s 22 evidence synthesis as a key facilitator of public involvement. South Asian elders influenced all Local Org’s activities from the point of inception through to workshop design and content, with the organisation accountable to its members. This type of approach and culture might be difficult to establish in healthcare settings, in which risk aversion64,65 and professionals’ vulnerability 66 when power is shared can stymie true co-production. In this context, there is therefore great value in collaborating effectively with community-based organisations with established relationships with specific seldom-heard groups. However, as our findings demonstrate, it is essential that collaboration is equitable, based on respect, of mutual benefit and not extractive in nature.67,76 The established partnership between Local Org and National Org was based on mutual trust and equitability, harnessing respective expertise and working together to ensure the workshops met participants’ needs, reflecting key co-production principles from the wider literature.68,69
Our findings support evidence from the USA that advance care planning education and discussion can be effectively nurtured through collaborations with trusted community-based organisations, increasing awareness of advance care planning benefits, community members’ confidence and readiness to engage with the process of completing documentation.43,70 Facilitation by someone from the same or similar cultural background seems to play a key role, reinforcing trust. 43 One UK study developed a peer-educator advance care planning programme with written resources 71 ; however, in this South Asian community where English was rarely a preferred spoken or written language, videos were considered a more useful means of sharing information and countering misperceptions. While videos have been previously highlighted as a popular and effective method of encouraging advance care planning,72 –74 until now, the focus has been on educational videos produced by clinical services and made available online. 48 For example, a study of older hospitalised patients with kidney failure in Hawaii found that advance care planning documentation rates increased from 3% to 40% after a video intervention. 72 However, language barriers and digital exclusion can prevent access to online resources. Short videos designed for community members, by community members, sharable with friends, families and neighbours, may offer a more acceptable, feasible and effective method of informing and engaging people on end-of-life topics such as advance care planning. Further testing of such interventions in specific minoritised ethnic communities is warranted.
Strengths and weaknesses
The primary strengths of this study relate to its co-designed nature. Staff from the local and national collaborating organisations, together with academic team members, co-designed the study protocol, documentation and recruitment processes and contributed to data analysis and interpretation. This helped ensure that the methodology was feasible, respectful and egalitarian. Local Org staff (NA/SK) are from South Asian communities and facilitated workshops and focus groups, enabling the collection of authentic data from seldom-heard South Asian elders in the UK. However, this meant that facilitators invited focus group participants, and participants knew the facilitators, which may have influenced their responses in favour of the workshops. This study focussed on a specific collaborative project, based in a single London borough, with a distinct community of South Asian elders who were already engaged with participating Local Org. Most focus group participants were women of Indian ethnicity. Findings may not be transferrable to other community-based interventions, or to other South Asian communities (and of course to ‘minoritised ethnic communities’ in general) across the UK. In particular, South Asian elders who are not engaged with community groups might have different experiences and wishes; further research is needed in this area. Guided by Local Org collaborators, we did not collect demographic data on focus group participants’ sexual identity or health conditions, so we were unable to explore intersectional disadvantage. Finally, we did not assess the number of elders who completed advance care planning as a result of the workshops. Rather, we conceptualised it as a process on a continuum for which preparation is required 75 ; as such, quantitative metrics would offer a crude measure of workshop effectiveness.
Implications
Findings contribute to evidence on co-production in palliative care and can inform future intervention development and cross-sector collaboration. Co-production in palliative care must foster trust, respect, confidentiality and psychological safety and ideally be embedded within nurtured relationships with communities. Cultural sensitivity, and a holistic, person-centred approach which is flexible and adaptable, are essential. Findings also highlight the important role of the UK voluntary, community, faith and social enterprise sector in supporting co-production in palliative care. Longstanding relationships between organisations and their communities contribute towards high levels of mutual trust, shared knowledge and embedded intelligence. 42 Effective inter-organisational collaboration can play a central role in mitigating inequities in palliative care as well as supporting the development of compassionate communities and associated community-led models of care for the dying and bereaved. 76 The utility of community-generated advance care planning resources in the form of shareable videos in preferred languages warrant further research.
This study also demonstrates the value and feasibility of co-production in palliative and end-of-life care research. In particular, co-production enabled the collection of rich and authentic data from non-English speaking communities. Lessons from conducting this research include the need to prioritise time to build trust and mutual understanding; co-designing a project which is achievable without over-burdening community partners; reciprocal skills-sharing, including providing appropriate training and support for community co-researchers; and flexibility regarding research processes.
Conclusion
Co-production is a key method to widen access to information and support and ensure palliative and end-of-life care resources and services are appropriate for diverse ethnic groups. Findings from this in-depth study of co-production in action can inform research with community partners and minoritised groups in palliative and end-of-life care as well as future advance care planning interventions.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241302678 – Supplemental material for Co-production in practice: A qualitative study of the development of advance care planning workshops for South Asian elders
Supplemental material, sj-docx-1-pmj-10.1177_02692163241302678 for Co-production in practice: A qualitative study of the development of advance care planning workshops for South Asian elders by Oliver Clabburn, Tracey Stone, Naheed Anwar, Taskin Saleem, Salim Khan, Verena Hewat, Usha Grieve, Lesel Dawson, Michelle Farr, Sabi Redwood and Lucy E Selman in Palliative Medicine
Footnotes
Acknowledgements
Our thanks to the South Asian elders who engaged with the workshops and shared their experiences throughout the focus groups, and to the staff and volunteers from both organisations for their support.
Author contributions
LS (PI): led funding application, co-designed and supervised all aspects of the study and wrote the paper. OC (researcher): co-designed project, obtained ethical approval, trained community co-researchers, conducted interviews, data analysis and wrote the first draft of the paper. TS: co-analysed data and advised on the project with MF/LD/SR/TS/NA/SK/UG/VH. Project and workshop development was led by VH/UG (National Org) and TS (Local Org). NA/SK (Local Org): co-developed/facilitated workshops, recruited and conducted focus groups. All authors contributed to reviewing and providing feedback on the final version of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was part of Good Grief Connects, funded by The National Lottery Community Fund’s Bringing People Together Programme. This research was supported by the National Institute for Health and Care Research Applied Research Collaboration West (NIHR ARC West). The views expressed in this article are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.