
Abstract
Background:
Little is known about the last phase of life of patients with implantable cardioverter defibrillators and the practice of advance care planning in this population.
Aim:
To describe the last phase of life and advance care planning process of patients with an implantable cardioverter defibrillator, and to assess relatives’ satisfaction with treatment and care.
Design:
Mixed-methods study, including a survey and focus group study.
Setting/participants:
A survey among 170 relatives (response rate 59%) reporting about 154 deceased patients, and 5 subsequent focus groups with 23 relatives.
Results:
Relatives reported that 38% of patients had a conversation with a healthcare professional about implantable cardioverter defibrillator deactivation. Patients’ and relatives’ lack of knowledge about device functioning and the perceived lack of time of healthcare professionals were frequently mentioned barriers to advance care planning. Twenty-four percent of patients experienced a shock in the last month of life, which were, according to relatives, distressing for 74% of patients and 73% of relatives. Forty-two to sixty-one percent of relatives reported to be satisfied with different aspects of end-of-life care, such as the way in which wishes of the patient were respected. Quality of death was scored higher for patients with a deactivated device than those with an active device (6.74 vs 5.67 on a 10-point scale, p = 0.012).
Conclusions:
Implantable cardioverter defibrillator deactivation was discussed with a minority of patients. Device shocks were reported to be distressing to patients and relatives. Relatives of patients with a deactivated device reported a higher quality of death compared to relatives of patients with an active device.
Keywords
Guidelines recommend to discuss implantable cardioverter defibrillator deactivation before implantation, at different moments during the follow-up phase, and at the start of the palliative and terminal phase, and to deactivate the device when this is in line with patients’ goals of care.
Studies of hospital medical record data suggest that advance care planning conversations about implantable cardioverter defibrillator deactivation are conducted with up to 21% of patients, implantable cardioverter defibrillators are deactivated in about 30%, and about 10% experienced potentially inappropriate shocks in the last month of life.
However, hospital medical records might lack information about the last phase of life of the patient, for instance about the decision-making process regarding implantable cardioverter defibrillator deactivation, especially for those patients who die outside the hospital.
Relatives reported that implantable cardioverter defibrillator deactivation was discussed with 38% of patients, and 55% had their implantable cardioverter defibrillator deactivated. Numerous barriers towards having advance care planning conversations were identified, such as a lack of knowledge about the functioning of the device by patients as well as relatives, and a perceived lack of time of healthcare professionals.
Twenty-four percent of patients experienced shocks in the last month of life. These shocks were reported to be distressing for up to 73% of patients and relatives.
Only half of relatives were satisfied with different aspects of treatment and care at the last phase of life, such as the way in which the wishes of the patients were respected. Quality of death was rated rather low, but somewhat higher when the implantable cardioverter defibrillator was deactivated.
To prevent inappropriate shocks in the last phase of life, healthcare professionals should be educated in having advance care planning conversations with patients with an implantable cardioverter defibrillator.
Attention should be paid to barriers of patients with an implantable cardioverter defibrillator and their relatives towards discussing implantable cardioverter defibrillator deactivation, and healthcare professionals should take the initiative to start these conversations and to explain the negative consequences of having an active implantable cardioverter defibrillator at the end of life.
Attention should be paid to tailoring advance care planning conversations to the willingness of patients and relatives to engage in these conversations.
Introduction
An implantable cardioverter defibrillator treats potentially lethal arrhythmias by delivering electrical shocks, thereby prolonging life. 1 At the end of life, shocks may no longer be appropriate, since prolonging life might also mean possible prolongation of suffering. This can be prevented by deactivating the device. Guideline recommendations assert that there should be timely and frequent discussion of implantable cardioverter defibrillator deactivation with the patient and relatives throughout the disease trajectory.1,2 Advance care planning, the process of defining, discussing and reviewing goals and preferences for future medical treatment and care, 3 might help patients and relatives making a well-informed decision about device deactivation. Previous research showed that these conversations are conducted in up to 21% of patients,4,5 devices are deactivated in 30%, and 7% of patients experience shocks in the last month of life. 5 However, studies often rely on data from hospital medical records, 6 which may not be complete. They may lack important information about the end of life of patients, especially of those who die outside the hospital, and about the underlying reasons for why device deactivation was discussed. Relatives usually have an important role in the care for patients, and are usually an important partner in making decisions about care and treatment in the last phase of life.3,7 –9 Examining their views and experiences will give unique insight into the last phase of life of the patient, including the decision-making about implantable cardioverter defibrillator deactivation.4,10
We performed a mixed-methods study, including a survey and focus groups among relatives of deceased implantable cardioverter defibrillator patients to examine the advance care planning process, device management and occurrence of shocks in the last phase of life of patients with an implantable cardioverter defibrillator and to assess relatives’ satisfaction with care.
Methods
Study design
This study had a mixed-methods design. Approval of the ethical committee of the Erasmus University Medical Center Rotterdam (MEC-2017-357) was obtained before starting the data collection. All participants provided written informed consent. By combining quantitative with qualitative methods we obtained an in-depth understanding of the experiences with and content of the conversations and satisfaction with treatment and care. We used an explanatory sequential design in integrating the findings, in which both the quantitative and qualitative data was considered equally contributing to our aim. 11
Survey study
Sample
Relatives were identified in the medical records of implantable cardioverter defibrillator patients deceased between 2012 and 2017 from a university hospital and a general hospital in the Netherlands. Relatives were contacted by a member of the research team (BV) via phone between December 2017 and March 2018 to inform them about the study, and establish whether the respondent fulfilled the inclusion criteria and was knowledgeable about the patients’ illness trajectory. A respondent was considered to have mental capacity when there were no indications during the telephone conversation regarding lack of capacity, and when the informed consent form was signed. Participants were eligible when they were the relative of the deceased patient, were able to speak Dutch, were older than 18 years, and were able to provide written consent. Relatives who were interested in participating received additional information including an informed consent form and the survey by postal mail. Those who did not return the survey, received a reminder 1 month after the initial mailing. A total of 419 relatives were identified in the medical records of 297 deceased patients.
Measurements
The survey included 52 questions. Questions were based on a previously conducted phone survey by Goldstein et al., 4 which was adapted from the After-Death Bereaved Family Interview. 12 Questions were translated into Dutch by the research team. Self-constructed questions on the impact of implantable cardioverter defibrillator shocks on both the patient and the relative were added. The survey was pilot tested in eight patients and adjusted to fit to the Dutch context and culture. The last phase of life was operationalized as the last month preceding death. 4 The survey consisted of eight sections (see Supplemental Appendix 1), including sections about the last phase of life and death of the patient, advance care planning conversations about the implantable cardioverter defibrillator, and statements on satisfaction about care in the last phase of life (on a five point Likert scale, one meaning totally agree, five totally disagree) and quality of death (rated on a scale from 1 to 10).
Data analysis
One-hundred-seventy relatives participated in the survey study, reporting on 154 patients. For 15 of the 154 patients more than one relative responded (for 14 patients, two relatives responded, for one patient, three relatives responded). For these 15 patients, we used the survey of the relative closest to the patient based on their relationship (in order: spouse, child) for analyses. For the analyses of questions related to the personal opinion of the respondents (e.g. questions on satisfaction with treatment and care), we used all 170 respondents. Descriptive statistics were used to present the data. For the statements on satisfaction, scores of 1 (‘totally agree’) and 2 (‘agree’) represented the category ‘agree’. Reported quality of death was compared by reported shocks in the last month of life, occurrence of advance care planning conversations and device deactivation with student t-tests. A p-value of <0.05 was considered statistically significant. Analyses were performed using SPSS version 24.
Focus group study
Sample
Qualitative in-depth focus groups using a phenomenological approach 13 were conducted with a selection of interested relatives, to examine their experiences and to explore relevant topics. Focus groups were held in the Erasmus University Medical Center. Relatives received the study information sheet prior to participating in the focus groups. Those participating received a €25 gift card and travel reimbursement.
Measurements
An aide memoir was used in conducting the focus groups. Topics discussed were (1) information provision and communication about device deactivation; (2) experiences with patient’s last phase of life; and (3) suggestions for improving end-of-life care. Focus groups were led by experienced moderators (JR, AS or RS), and supported by AS, RS or HE.
Data analysis
Transcripts were analyzed using the constant comparative method. 14 Meaningful themes were identified and a coding tree was inductively developed a priori (based on the aide memoir). The coding tree was discussed with the research team, and subsequently tested and refined until no more new themes arose. Transcripts were analyzed by RS, and discussed with AS and JR. The three researchers met frequently to discuss the transcripts. Consensus was sought and found in case of disagreements.
Results
Study population
Survey study
Of the 419 identified relatives, we contacted 289; 247 agreed to participate and 170 returned a completed survey (response rate 59%) (Figure 1). They reported on 154 unique patients who died a median of 27 months (IQR 17–44) before completion of the survey, at a median age of 74 (IQR 66–79). Eighty-seven percent of patients were male. Relatives had a median age of 62 years (IQR 50–75) and 22% were male (Table 1). Of the relatives, 52% were spouses, 33% children, 13% other relatives, 1% friends and 1% neighbors.

Inclusion flowchart.
Characteristics of relatives of deceased patients with an implantable cardioverter defibrillator (N = 170), and the patients they report about (n = 154) (survey study).

IQR: inter quartile rate; WHO: World Health Organization.
One response missing.
Low: Primary school or lower general secondary education; Medium: Intermediate vocational education or pre-university education; High: University or university of applied sciences.
Two responses missing.
Other places of death were: rehabilitation centre (n = 2); care hotel (n = 1).
Focus group study
Twenty-three of 58 interested relatives participated in a focus group. We held five focus groups with respectively four, five, five, seven and two relatives. Relatives were most often the child (48%) or spouse (39%) of the deceased patient. Mean age was 56 years (SD 14.1) and 22% were male.
Advance care planning in patients with an implantable cardioverter defibrillator
Survey study
Fifty-eight of 170 relatives (34%) indicated having had a conversation with the patient about implantable cardioverter defibrillator deactivation (Table 2). According to the relatives, 59 of 154 patients (38%) had had a conversation about device deactivation with a healthcare professional, 15 (25%) in the last month and 11 (19%) in the last week of life. Forty-seven (80%) relatives were present during these conversations. In 11% of the patients who did not have a conversation about device deactivation the relative indicated that such a conversation would have been appreciated. Relatives reported that 18 patients (12%) had recorded their preferences for medical treatment and care in an advance care directive. Five of these documents addressed device deactivation.
Advance care planning in patients with an implantable cardioverter defibrillator (N = 154) (survey study).

DNR: do-not-resuscitate.
All 170 relatives were included in calculating this variable.
Three responses missing.
Only patients who did not have a device deactivation discussion were included in calculating this variable (n = 95).
One response missing.
Home care nurse.
Not including DNR-order.
Focus group study
In the focus groups, barriers and facilitators towards advance care planning conversations were discussed (Table 3). We categorized these into patient and relative related factors, as well as healthcare provider and system related factors. Some relatives reported that the patient’s willingness to discuss deactivation and their level of curiosity regarding understanding their device were important facilitating factors in having advance care planning conversations, as one relative described: “As a patient, at a certain moment, you do have the obligation to ask a little more proactively about what a certain product does, what it is, and how to deal with certain things [. . .] I think he did not even have the implantable cardioverter defibrillator for a month when we already had that conversation (about device deactivation – RS). And that makes you aware about the implantable cardioverter defibrillator, how it works and what it does” – Focus group 4, participant F032, 33 y/o son
Other facilitating factors were a good patient-doctor relationship, and the involvement of relatives to empower them to be involved in the decision-making process about device deactivation. Some relatives reported that a lack of knowledge about the functioning of the device, and a focus on its lifesaving capacity could act as barriers.
Barriers and facilitators of advance care planning conversations with the healthcare professional, according to relatives of deceased patients with an implantable cardioverter defibrillator (focus group study).
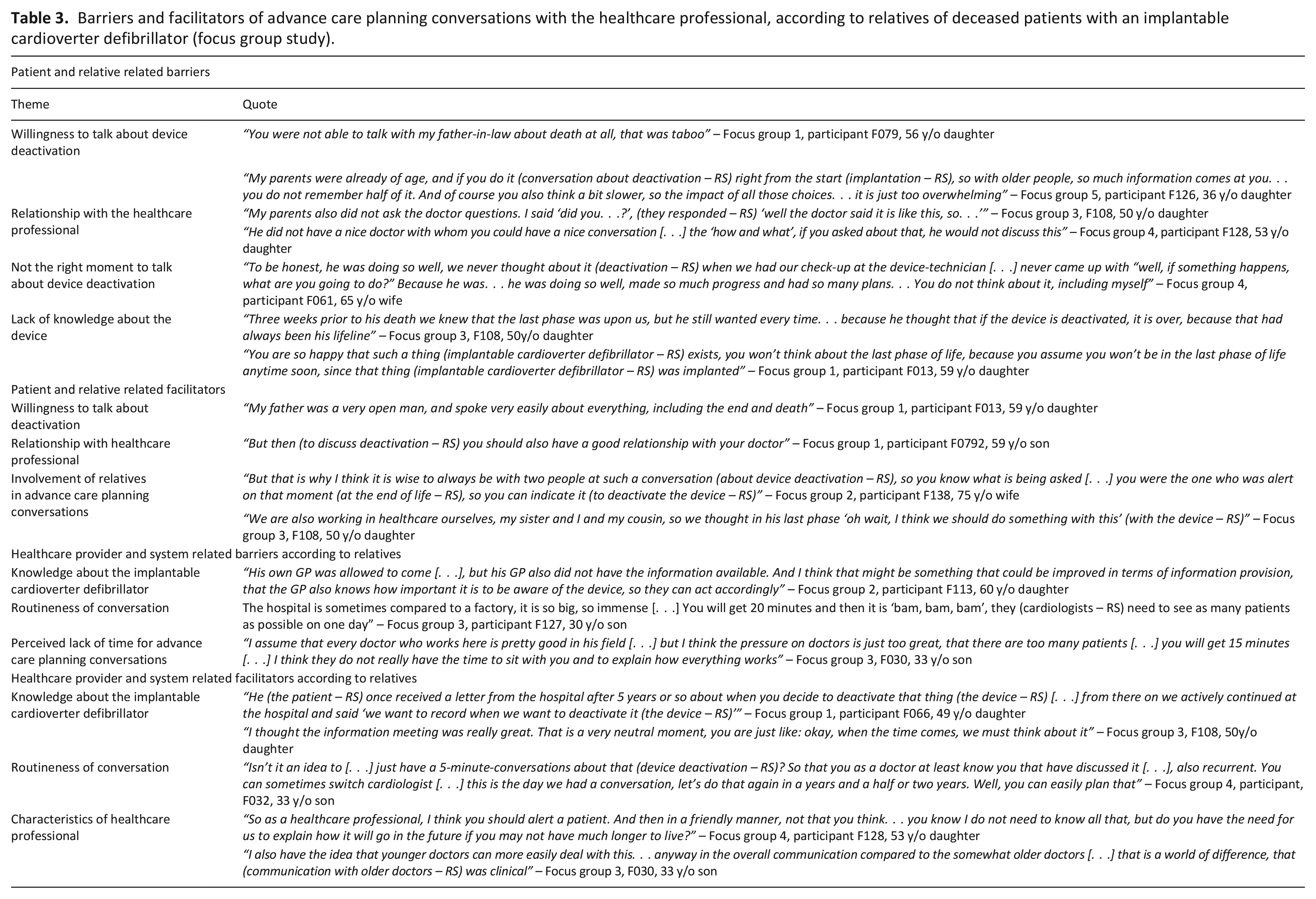
Some relatives mentioned they thought that healthcare professionals other than cardiologists (such as the GP) were not always knowledgeable about the functioning of the implantable cardioverter defibrillator and the possibility to deactivate. Also, some relatives perceived advance care planning conversations about device deactivation to be ‘routine practice’, which made some feel they were ‘one of many’, as one relative described: “Sometimes you get the feeling like you are walking into a factory, and you are just one of many. . . yes I do understand that the doctor may have this conversation 365 times a year, but well [. . .] for us it is only one time” – Focus group 3, participant F127, 30 y/o son
At the same time, routineness was valued by others, as this would normalize the topic and ensured its discussion. Another discussed barrier was the perceived lack of time of the healthcare professional, while some personal characteristics of the healthcare professional, such as a younger age, were sometimes perceived to be a facilitator.
Implantable cardioverter defibrillator management in the last phase of life
Survey study
Relatives reported that 113 (73%) patients were admitted to a hospital at least once in the last three months of life (Table 4). For 125 (74%) relatives and 108 (71%) patients, it had been clear that the patient was going to die within several days. In 84 (55%) patients, the implantable cardioverter defibrillator was deactivated, 35% in the last week and 32% on the last day of life, in most cases by the implantable cardioverter defibrillator technician (49%) in the hospital (74%). Relatives reported that 37 (24%) patients experienced one or more shocks in the last month of life, 25 (16%) in the last week and 16 (10%) on the last day of life. Relatives reported that 74% of patients were distressed by these shocks, and 73% of relatives reported to be distressed themselves.
The last phase of life of patients with an implantable cardioverter defibrillator (N = 154) (survey study).

All 170 relatives were included in calculating this variable.
One response missing.
Only the 39 relatives of patients who had a shock in the last month of life were included.
Only the 37 patients who had a shock in the last month of life were included.
Only the 84 patients who had their device deactivated were included.
Satisfaction with treatment and care in the last phase of life
Survey study
Of the 170 relatives, 104 (61%) agreed with the statement that healthcare professionals had sufficiently informed them and the patient about the patient’s prognosis. Seventy-one (42%) relatives agreed with the statement that issues related to the implantable cardioverter defibrillator in the last phase of life were sufficiently discussed by the healthcare professional. Ninety-two (54%) relatives felt that the healthcare professional respected the wishes of the patient, and 88 (52%) felt that they received good emotional support from the healthcare professional. For the 59 patients who had a device deactivation conversation with the healthcare professional and the 47 relatives who were present during this conversation, respectively 42 (71%) and 38 (81%) were satisfied with this conversation. Relatives rated the quality of death of the patient with a mean score of 6.4 (SD 2.5). Relatives of patients who had their device deactivated reported a significantly higher quality of death (6.74) as compared to relatives of patients who did not have their device deactivated (5.67) (p = 0.012). The occurrence of shocks (reported quality of death with shocks 5.89 and without 6.60) and the occurrence of advance care planning conversations (reported quality of death with advance care planning conversations 6.72 and without 5.97) was not significantly associated with quality of death (p = 0.163 and p = 0.077 respectively).
Focus group study
Satisfaction with treatment and care in the last phase of life of the patient varied (Table 5). Three themes emerged in the focus groups concerning the satisfaction with treatment and care in the last phase of life. First, the relationship between the patient and relative and the healthcare professional was considered important by many relatives. They greatly appreciated emotionally involved healthcare professionals, respect, honesty and kindness, while others described missing these features.
“Honesty is also important, what the doctor had always been, he was always clear and honest, what they (patient and the doctor – RS) really valued in each other” – Focus group 5, participant F126, 36 y/o daughter
Satisfaction with treatment and care in the last phase of life according to relatives of deceased patients with an implantable cardioverter defibrillator (focus group study).

Second, communication between the patient and relative and the healthcare professional was often mentioned. Some relatives described that healthcare professionals were always available for questions and took the time to answer all questions, which was appreciated. However, others described that healthcare professionals never educated the patient about the implantable cardioverter defibrillator and the last phase of life, and communication was lacking.
“We have never heard anything about the last phase of life [. . .] I feel it (communication about the implantable cardioverter defibrillator in the last phase of life – RS) went so wrong with us and I still feel bad about that” – Focus group 1, participant F079, 56 y/o daughter
Third, communication between healthcare professionals was often mentioned in the focus groups. Some described that this communication lacked, especially when healthcare professionals worked in different institutions, which made relatives feel responsible for the patient’s medical care. Some relatives described missing a ‘coordinator’, who could act as a contact person and take the lead in organizing end-of-life care, including implantable cardioverter defibrillator management.
“There was no information transfer whatsoever, not from the hospital, not from the care facility, nobody. . . We were the only ones who had information, but only from what we had heard. We did not have the medical records.” – Focus group 2, participant F113, 60 y/o daughter
Discussion
In this study, relatives reported that 38% of patients had an advance care planning conversation with the healthcare provider, 55% had their implantable cardioverter defibrillator deactivated and 24% experienced shocks in the last month of life. These shocks were distressing for 74% of patients and 73% of relatives. About half of the relatives reported to be satisfied with different aspects of care and treatment in the last phase of life, such as the way in which relatives felt healthcare professionals respected the wishes of the patient. Relatives reported a rather low quality of death (mean score 6.40), that was somewhat higher when the device was deactivated (score 6.74).
A comparable American study conducted by Goldstein et al. 4 among relatives of deceased implantable cardioverter defibrillator patients in 2004, showed that 27% of patients had had a conversation about device deactivation. In our study, this was 38%. This is consistent with the trend of increasing rates of deactivation discussions. 5 It is remarkable that in our study only 11% of the relatives of patients who had not had a conversation about device deactivation thought the patient would have been interested in having had this conversation. Studies from the perspective of the patient had contradictory results, and indicate that most patients are interested in these conversations.8,15,16 However, other studies reported that patients are reluctant to discuss deactivation, partly due to inadequate knowledge of how the device works,15,17 which emphasizes the need to educate patients about the consequences of having an implantable cardioverter defibrillator. 3 These contradictory results also show that advance care planning is not a one-size-fits-all approach, and that the readiness and willingness of the patient to discuss device deactivation should be explored. 3 In our study, most relatives wanted to be involved in advance care planning conversations, although only 28% were present during these conversations. Previous research confirms this and shows that relatives often feel excluded. 18 Both patients and healthcare providers agree that relatives should be involved in advance care planning conversations.15,19 –21
We identified several barriers and facilitators towards conducting advance care planning conversations. Some relatives reported a lack of knowledge in both patients and relatives about the implantable cardioverter defibrillator, and patients often focused on the lifesaving capacity of the device.22,23 This might impair their willingness to engage in conversations about deactivation. In addition, relatives reported that the knowledge about the implantable cardioverter defibrillator of healthcare providers who work in specialties outside cardiology (e.g. general practitioners), seemed to be limited as well. Some personal characteristics of the healthcare professionals (e.g. honesty, younger age), and the perceived quality of the patient-doctor relationship acted as facilitators for having advance care planning conversations. 24 Some of these barriers and facilitators are comparable to barriers and facilitators towards ACP as mentioned by patients with cancer. 25 However, implantable cardioverter defibrillator patients are a unique population. Their disease trajectory is often unpredictable,26,27 and they have a potentially lifesaving device implanted in their body, which can be deactivated. 28 This adds to the complexity of decision-making at the end of life.
In our study, 55% of the patients had their device deactivated, compared to 21% in Goldstein’s et al. 4 study. The increase might be the result of enhanced awareness about this topic and the publication of guidelines.1,2 It is remarkable that the incidence of device deactivation in our study is higher than the occurrence of conversations about device deactivation between the patient and healthcare professional (38%). We assume this might be due to the possibility that the relative was not aware or had forgotten that the patient had a conversation about device deactivation with the healthcare professional. Relatives in our study reported that 24% of patients experienced shocks in the last month of life, and 10% on the last day of life, compared to respectively 27% and 8% of patients in Goldstein’s et al. 4 study, which is comparable. 6 Studies of medical records reported lower shock incidences, but these might have underestimated the shock incidence.5,6 Our study showed that 74% of patients and 73% of relatives were distressed by shocks in the last month of life. The high distress rate amongst patients and relatives, in addition to our finding that relatives reported a higher quality of dying for the patient when the device was deactivated, confirms the importance of conducting advance care planning conversations. Less than half of the relatives reported to be satisfied about the way in which they were informed about implantable cardioverter defibrillator deactivation in the last phase of life. This is comparable to previous studies,29,30 which showed that the information patients received about psychosocial consequences of living with the implantable cardioverter defibrillator and about the end of life was considered insufficient by the patient.
Strengths and limitations
This study is the first mixed-methods study about advance care planning in implantable cardioverter defibrillator patients from the perspective of relatives. It provides useful additional information to studies using data from medical records, since patients often die outside of the hospital. 6 In addition, by combining both quantitative and qualitative data, we did not only supply the numbers, but also provide a deeper understanding on how advance care planning conversations are experienced. Some limitations have to be considered. Selection bias may have played a role. It is possible that only relatives participated with either strong positive or negative experiences. This is partly accounted for by identifying relatives via medical records and the reasonable response. However, it was unknown to what extent relatives actively participated in the patient’s care. Furthermore, the relatives in our study were mostly female. However, no significant differences were found between the answers of female and male relatives. Also, recall bias should be considered, as we selected relatives of patients who had died between 2012 and 2017. However, past experiences that are significant to respondents, such as the death of a loved one or a device shock, are usually less prone to recall bias. 31 Lastly, it should be noted that 15 patients had more than one relative’s response analyzed in the questions on treatment and care. This could bias the results towards the experience of these 15 patients as compared to the whole.
Implications
Advance care planning conversations are aimed at eliciting preferences of implantable cardioverter defibrillator patients towards device deactivation. However, patients and relatives experience barriers towards having these conversations. Healthcare professionals should be attentive of these barriers and take the initiative to start the conversation. Since patients’ willingness towards having these conversations vary, and healthcare professionals themselves might experience barriers to conduct advance care planning conversations, educational programmes for healthcare professionals should be developed and implemented. 32 Healthcare professionals have to be aware that patients and relatives may struggle with the idea of deactivation. However, they should also be aware that implantable cardioverter defibrillator deactivation may result in a higher quality of death, and advance care planning conversations are vital in making this decision. Advance care planning conversations with patients and relatives should therefore be carefully tailored to their willingness to engage in these, but should provide them with the information needed to formulate their future wishes.
Conclusion
Implantable cardioverter defibrillator deactivation was discussed with a minority of patients, based on the relatives’ recollection. Half of the patients had their devices deactivated, and up to a quarter received shocks in the last month of life, which were reported to be distressing for both patients and relatives. Patients with a deactivated device had a higher reported quality of death compared to patients with an active device. Advance care planning conversations, tailored to the need of the patient, may help to make a timely and well-informed decision to deactivate the implantable cardioverter defibrillator, and to improve the quality of dying for these patients.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163211001288 – Supplemental material for Advance care planning and end-of-life care in patients with an implantable cardioverter defibrillator: The perspective of relatives
Supplemental material, sj-docx-1-pmj-10.1177_02692163211001288 for Advance care planning and end-of-life care in patients with an implantable cardioverter defibrillator: The perspective of relatives by Rik Stoevelaar, Arianne Stoppelenburg, Rozemarijn L van Bruchem-Visser, Anne Geert van Driel, Dominic AMJ Theuns, Martine E Lokker, Rohit E Bhagwandien, Agnes van der Heide and Judith AC Rietjens in Palliative Medicine
Footnotes
Acknowledgements
We would like to thank B.M. Vlottes for helping with the data-collection in the survey study. We would like to thank H.J. van Esch (HE), for assisting in the focus group study. We would like to thank M. Verheul for transcribing the focus groups.
Author contributions
AD, AH, DT, REB, RLB and JR designed the study. AS, JR and RS recruited participants. AS, AH, JR and RS collected the data. AS, JR and RS analyzed and interpreted the data. RS wrote the first draft of the manuscript. All authors made a substantial contribution to the concept or design of the work, revised it critically for important intellectual content and take public responsibility for appropriate portions of the content. All authors approved the final version of the manuscript to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by The Netherlands Organization for Health Research and Development (grant number 80-84400-98-076).
Research ethics and patient consent
Before conducting this study, approval of the ethics committee of the Erasmus MC, Erasmus University Medical Center Rotterdam, was obtained (METC-2017-357). Participants were given both verbal and written information on the study and all provided written consent.
Data management and sharing
Data and materials collected in the study are property of the Erasmus MC, Erasmus University Medical Center Rotterdam, The Netherlands, and are archived according to international and national regulations at the Department of Public Health of the previously mentioned institution. Due to the confidentiality of the data, data is not publicly available. The survey used in this study has been added as a supplementary file.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.