
Abstract
Background:
Palliative care and supportive care provided in the home for people with heart failure can improve quality of life, caregiver wellbeing and reduce healthcare costs. Identifying components of home-based palliative and supportive care in heart failure is useful to inform tailored care to people with heart failure.
Aim:
To identify and describe components of home-based palliative and supportive care in adults with heart failure.
Design:
A scoping review was undertaken in accordance with Joanna Briggs Institute guidelines. The protocol was registered prospectively with the Open Science Framework (https://doi.org/10.17605/OSF.IO/GHCME).
Data sources:
Embase, PubMed, CINAHL and Cochrane databases were searched from inception in May 2023 and re-run in January 2024. Original research focussed on palliative and supportive care in the home setting that included adults diagnosed with heart failure who have not undergone nor awaiting a heart transplant was included.
Results:
Results were extracted from 13 papers based on eight studies. The findings highlight that nurses supported by a multidisciplinary team, providing symptom management, patient and carer education and discussion of goals of care and advance care planning, facilitates home-based palliative and supportive care for people with heart failure.
Conclusion:
Ensuring patient and caregiver-centred care supported by a multidisciplinary team is essential to delivering home-based palliative and supportive care for people with heart failure. Further research focussed on the role of digital interventions in home-based palliative and supportive care, the composition of the multidisciplinary team and research which includes individuals across all stages of heart failure is needed.
Providing palliative and supportive care in the home setting for people with heart failure is advantageous because care can be provided in accordance with an individual’s way of life.
Home-based palliative and supportive care for people with heart failure has the potential to improve person and caregiver outcomes and reduce healthcare costs.
The components of home-based palliative and supportive care are symptom management; expert communication; multidisciplinary team involvement; continuity of care; education; end-of-life discussions; and caregiver support.
While initiation of care, the services provided in the home-setting and health care approaches provided differed across the reported studies, in all included studies, nursing staff were strategically placed to provide a wide range of services in the home-setting.
Continuous and early liaison between cardiology, palliative care and primary care providers is needed to provide continuous, non-fragmented care.
The detailed findings of this review which highlight the components of home-based palliative and supportive care can provide guidance to enable health care providers to tailor care for this population.
Future research into the perspectives of people with heart failure on each of the identified components and their implementation will assist service providers to gain a better understanding of how to enable home-based palliative and supportive care for persons with heart failure.
Background
Heart failure affects over 26 million people worldwide with the affected numbers rising due to the increasing and ageing population and improved survival due to advancement of therapies.1,2 Despite improvements in diagnosis and therapeutics, people with heart failure often experience high symptom burden, poor quality of life and frequent re-hospitalisation.1,3 Increasing multimorbidity and healthcare expenditure highlight the need for broader, multifaceted approaches to the clinical management of heart failure. 4
Palliative care is an approach which aims to improve the quality of life for individuals and their families experiencing concerns associated with life-limiting illnesses. 2 Early identification, correct assessment and treatment of physical, psychosocial or spiritual problems are core to palliative care and is most effective when considered early in the illness. 2 Early access and utilisation of palliative care is recommended for persons with heart failure5 –10 to alleviate symptom burden and improve overall quality of life. A systematic review by Hui et al., 11 identified that palliative care is often incorporated at advanced stages of illness, despite evidence to support the reported benefits of early utilisation of palliative care, including improved quality of life of the person and their family members. One of the reasons that palliative care is often incorporated in practice at the advanced stages of illness despite the evidence, is due to palliative care being viewed as end-of-life care for people with heart failure, despite definitions of palliative care shifting away from care provided to individuals imminently dying. 12 The term supportive care has a similar definition to palliative care as it focusses on alleviating symptoms and improving overall quality of life of the patient through the illness trajectory and alongside heart failure management and refers to the provision of a wide range of services from early onset to advanced disease, but is associated with less stigma than palliative care.11,13 –16 The term supportive care has the potential to be more acceptable for people with heart failure and clinicians, enabling earlier access and uptake to interventions aimed at improving quality of life. Acknowledging the overlap of the terms supportive and palliative care, this current review uses both palliative and supportive care to indicate care from early onset of disease to advance stages and beyond.
While palliative and supportive care is delivered across care settings,8,17 most people with heart failure spend a considerable time in the community. 18 Therefore, the delivery of palliative and supportive care in the home setting is of particular importance if we are to improve the outcomes for people with heart failure and reduce costs associated with potentially preventable hospitalisations.19 –21 A growing number of studies report that home-based care when provided in a timely, integrated manner, with a person-centred focus, can improve health-related quality of life and reduce health care costs.22 –24 However, little is known about the components of home-based palliative and supportive care in heart failure. Current literature has described essential components of home-based long term care with a focus on activities of daily living, 25 components of palliative care in the home-setting 20 and components of heart failure management in the home-setting. 26 While this literature provides information about the essential health and non-health components required for care provision in these contexts, the components of this care model for people with heart failure who experience an unpredictable disease trajectory and require care in the home which reflects the principles of palliative and supportive care have not been well described. The aim of this scoping review is to identify and describe components of palliative and supportive care in the home setting for persons with heart failure.
Methods
Review question
What are the components of home-based palliative and supportive care for persons with heart failure?
Eligibility criteria and study selection
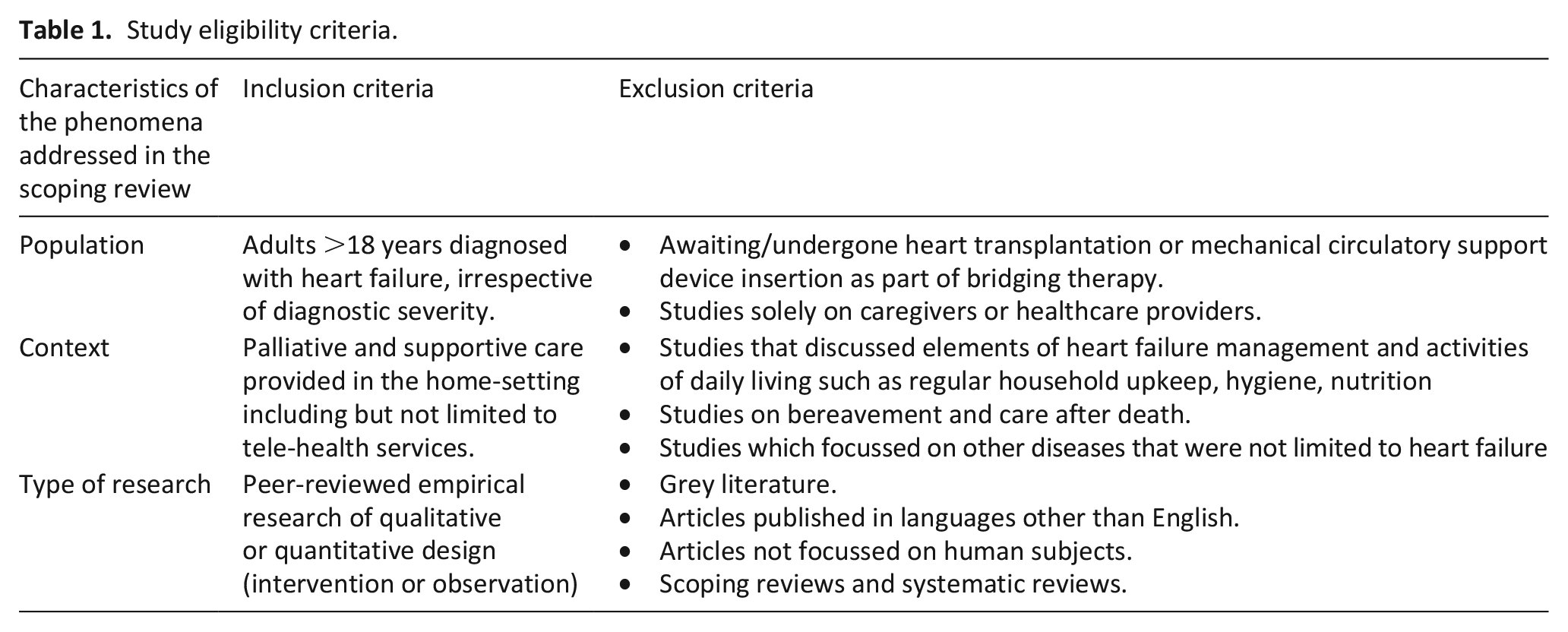
Studies with the following criteria were included: (1) peer-reviewed empirical research of qualitative or quantitative design (intervention or observation) focussed on palliative and supportive care at home (2) adults ⩾18 years diagnosed with heart failure; (3) who were not awaiting/nor undergone heart transplantation or mechanical circulatory support device insertion as part of bridging therapy. This cohort was excluded as home-based palliative and supportive care for these populations are likely to differ due to the specific issues and needs such as the risk of infection, perioperative complications and prolonged deterioration. 27 Articles that reported multiple populations (i.e. health care providers and caregivers) were included if the population with heart failure could be extracted separately. Multiple articles from the same study were included if each article provided different insights to answer the research question. The eligibility criteria for the articles are detailed in Table 1.
Study eligibility criteria.
Title, abstract and full-text review was conducted by two independent reviewers (MP and UH). Disagreements between reviewers on articles for full text inclusion were resolved by the members of the research team (GKS, WP) who are experts in palliative care and cardiology. Preferred Reporting Items for Systematic Reviews and Meta Analysis extension for Scoping Review (PRISMA-ScR) guided reporting. 28
Data sources and search strategy
In May 2023, the electronic databases: Embase, PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Cochrane were searched from inception and re-run in January 2024. Search results were not limited by year of publication. The references of the included papers were also searched for inclusion.
This review focusses on palliative and supportive care provided from early onset to advanced stages in the home setting and the following key search terms were used; (Home OR domicil*) AND (supportive care OR palliative care OR end-of-life-care OR hospice care OR terminal care OR patient centred care OR palliative therapy OR terminally ill patient OR advance care OR advanced care OR ‘palliat*’ OR ‘terminal*’) AND (heart failure OR cardiac failure OR left ventricular failure). The search strategy was refined in consultation with a librarian and the final search strategy for all databases is available in Supplemental Material A. The final protocol was registered prospectively with the Open Science Framework (https://doi.org/10.17605/OSF.IO/GHCME) and guided by the Joanna Briggs Institute methodology. 29
Data extraction
Data extraction was done using a data charting form developed in Microsoft Excel. The data charting form was piloted by two independent reviewers (MP and UH) using two articles and was revised in an iterative manner following discussions with the research team. The final data extraction sheet included author, year of publication, country of origin, type of article, aim of article, study method, sample size, New York Heart Association class of the study population, description of the home-based model and components of the home-based model/intervention (Supplemental Material B).
An a priori framework was used to organise the data. The a priori framework was informed by a conceptual framework of supportive care, 11 the components of heart failure management at home, 30 the Kidney Supportive Care Framework 31 and the components of palliative care at home.20,32 Collation of the frameworks to identify the broad categories used in this scoping review is presented in Supplemental Material C. The final categorisation of study findings is presented narratively and organised under the broad categories of symptom management, expert communication, multidisciplinary team involvement, continuity of care, education, end-of-life care and caregiver support.
Results
Study selection
The search yielded 4074 publications, from which 789 duplicates were removed. The remaining 3285 publications underwent title and abstract review, followed by full text review of 66 articles using cloud based open-source software as a service (SaS) ‘Rayyan’. The search was rerun in January 2024 and an additional article included. After excluding 53 articles, a total of 13 articles that matched the eligibility criteria were included in this scoping review (Figure 1).
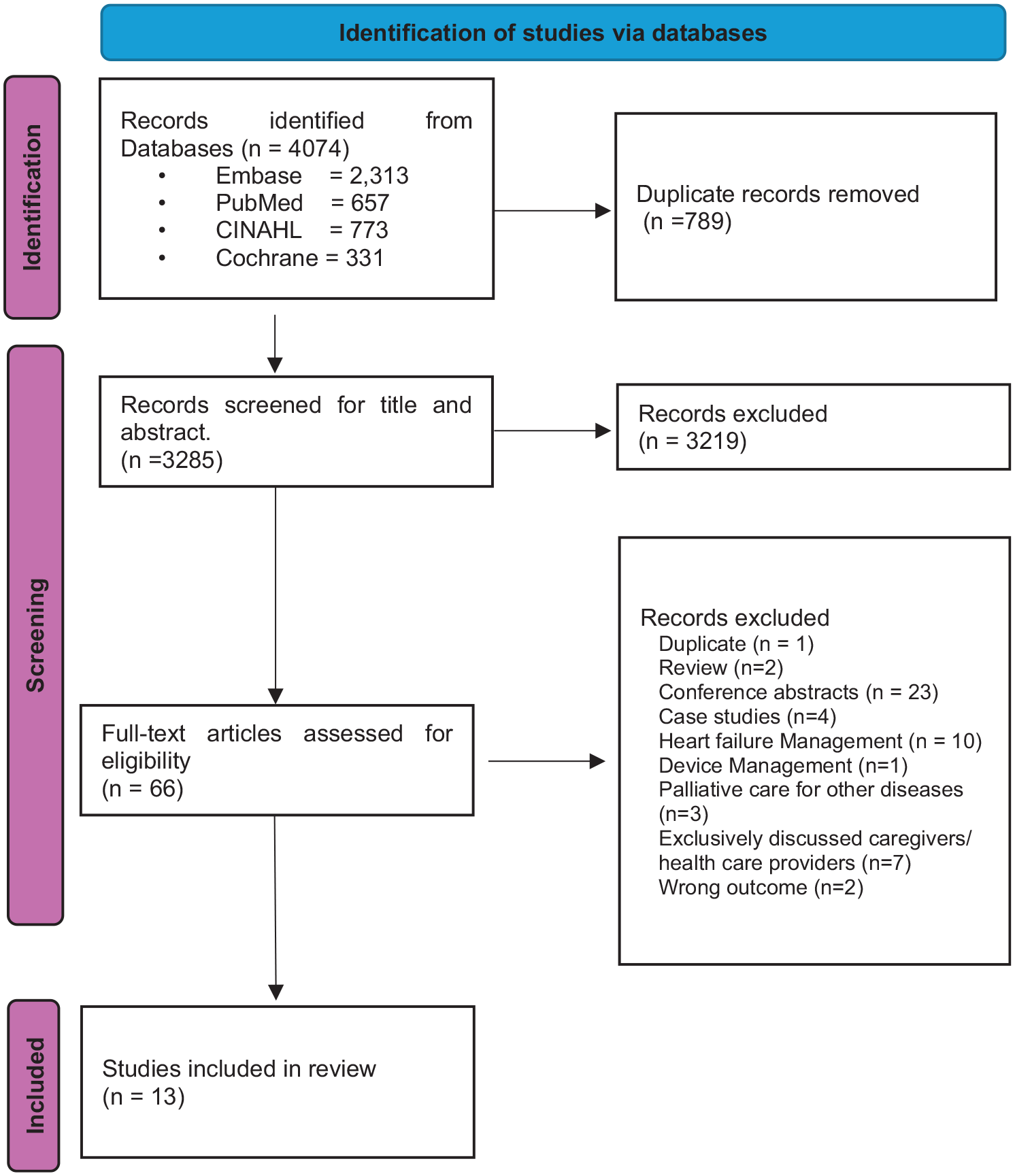
PRISMA flow diagram.
Study characteristics
The 13 papers included were from eight original research studies. Among the studies (N = 8), five described models of care, while two studies described administration of a drug for symptom relief in the home and one study on a quality improvement project based on education of the home health care team to provide home-based palliative care in heart failure. Detailed characteristics of the 13 published articles are presented below (Table 2). The highest number of studies originated in Europe (n = 3, 37.5%), followed by North America and Asia (n = 2, 25%). All studies in this review were published after 2010.
Summary of study characteristics.
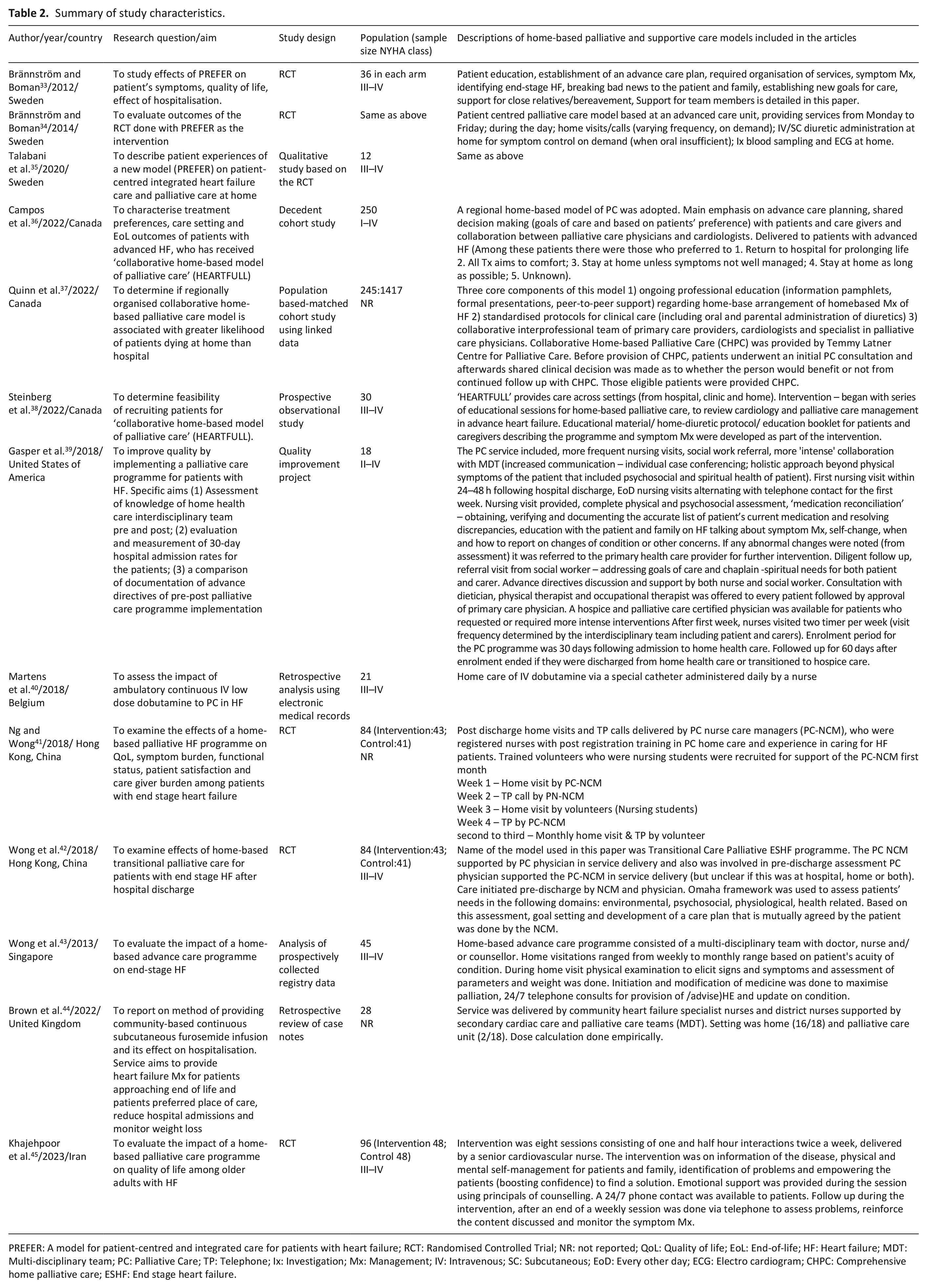
PREFER: A model for patient-centred and integrated care for patients with heart failure; RCT: Randomised Controlled Trial; NR: not reported; QoL: Quality of life; EoL: End-of-life; HF: Heart failure; MDT: Multi-disciplinary team; PC: Palliative Care; TP: Telephone; Ix: Investigation; Mx: Management; IV: Intravenous; SC: Subcutaneous; EoD: Every other day; ECG: Electro cardiogram; CHPC: Comprehensive home palliative care; ESHF: End stage heart failure.
From the eight studies, six (75%) included people with heart failure with New York Heart Association class III–IV (Supplemental Material D includes the classification of Heart Failure by New York Heart Association). One study 39 included people with heart failure New York Heart Association class II–IV and only one study 36 included people belonging to all four classes of New York Heart Association. The referral criteria included in these studies were based on prognosis with almost all having advanced heart failure (New York Heart Association III–IV) as a pre-requisite to receive any component of home-based palliative and supportive care.
Study participants
Characteristics of the study participants in the included studies are described in Table 3. Among the 8 reported studies, a total of 709 persons with heart failure received a range of services relating to home-based palliative and supportive care. All patients were >65 years of age. Among the studies that reported the mean ± standard deviation age of study participants, the age was between 69.46 ± 11.61 and 88.7 ± 7.9 years. One study did not report the sex of participants. 40 Of the remaining seven studies, male participation ranged from 39% 43 to 79% 44 with four studies having a predominant male participation.33,40,44,45
Characteristics of study participants the eight primary studies.
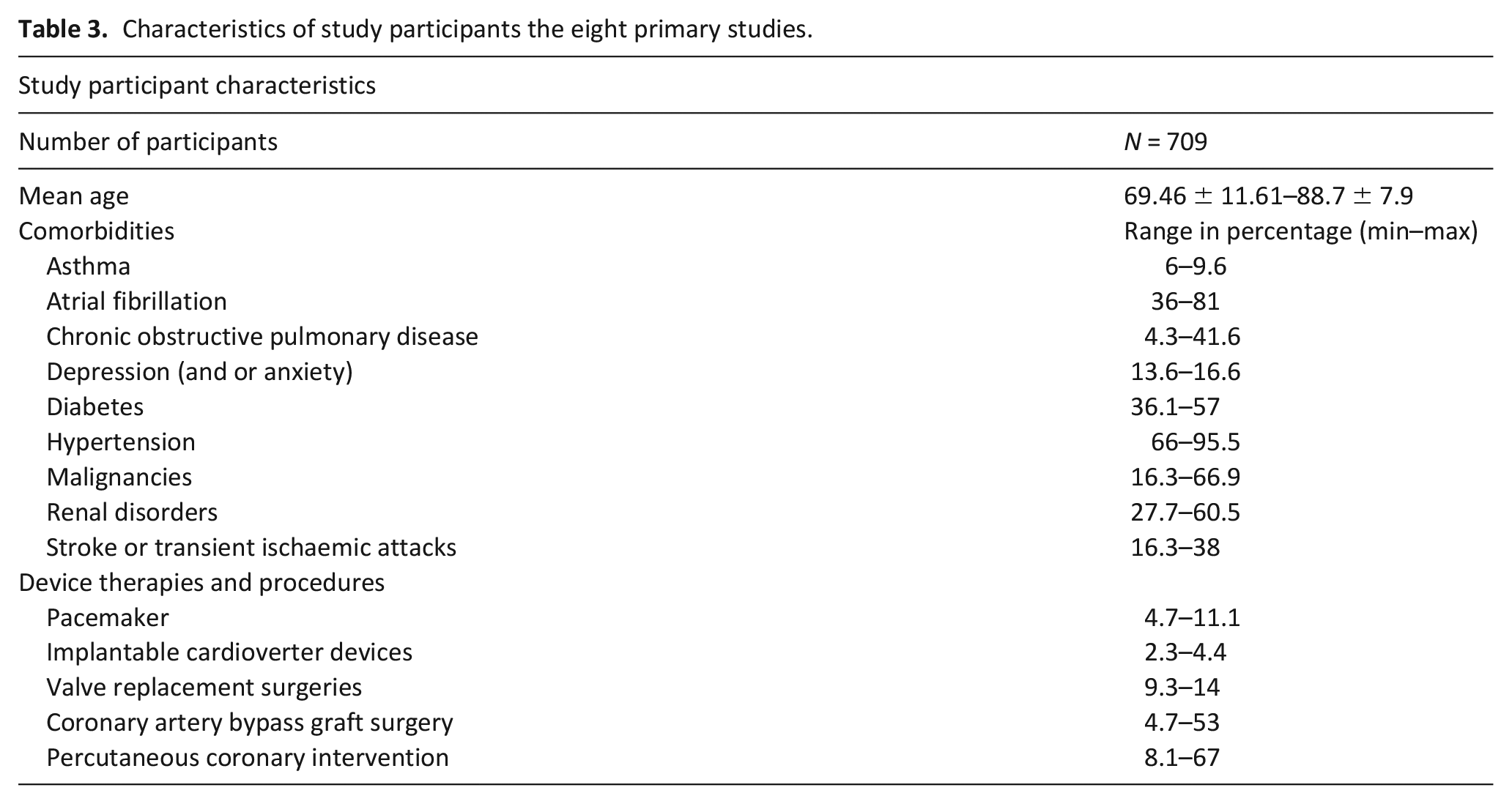
Six studies described the presence of comorbidities of study participants33,36,40,42,43,45 and among those, five described the types of comorbidities.34,35,40,42,43 Hypertension, atrial fibrillation, diabetes, renal disorders and stroke and or transient ischaemic attacks were among the commonly reported comorbidities with the reported frequency percentages varying across the studies. Table 3 depicts the minimum and maximum range of percentages reported across the studies. Additionally, one study reported on dementia 37 and cirrhosis. 36
The aetiology of heart failure was reported in five studies33,40,42 –44 and ischaemic heart disease was among the most commonly reported aetiology ranging from 69.8% to 81%. Hypertension was listed as a cause for heart failure in two studies33,42 along with cardiomyopathy, 42 heart valve disease 42 and severe left ventricular dysfunction. 44
Four studies reported device therapies and procedures33,37,40,42 undergone by the study participants while one study only reported the current medications of the persons with heart failure. 43 Participants with pacemakers ranged from 4.7% 42 to 11.1%. 33 Implantable cardioverter devices were present in 2.2% 42 to 4.4% 37 of participants. Coronary artery bypass graft (CABG) surgery and percutaneous coronary intervention (PCI) were among the most reported surgical procedures ranging from 4.7%-53% and 8.1%-67% of participants respectively and valve replacement surgery being reported in 9.3% to 14%.
Components of home-based palliative and supportive care
Despite this review’s focus on palliative and supportive care provided from early onset of disease through to advanced disease, the findings below reflect a focus on persons with advanced stages of heart failure and there is less information on persons with heart failure who have mild symptoms and slight limitations during ordinary activity. The components of home-based palliative and supportive care for adult people with heart failure centred around broad categories of symptom management; expert communication; multidisciplinary team involvement; continuity of care; education; end-of-life care; and caregiver support (Figure 2). A detailed summary of the components is presented in Supplemental Material E.
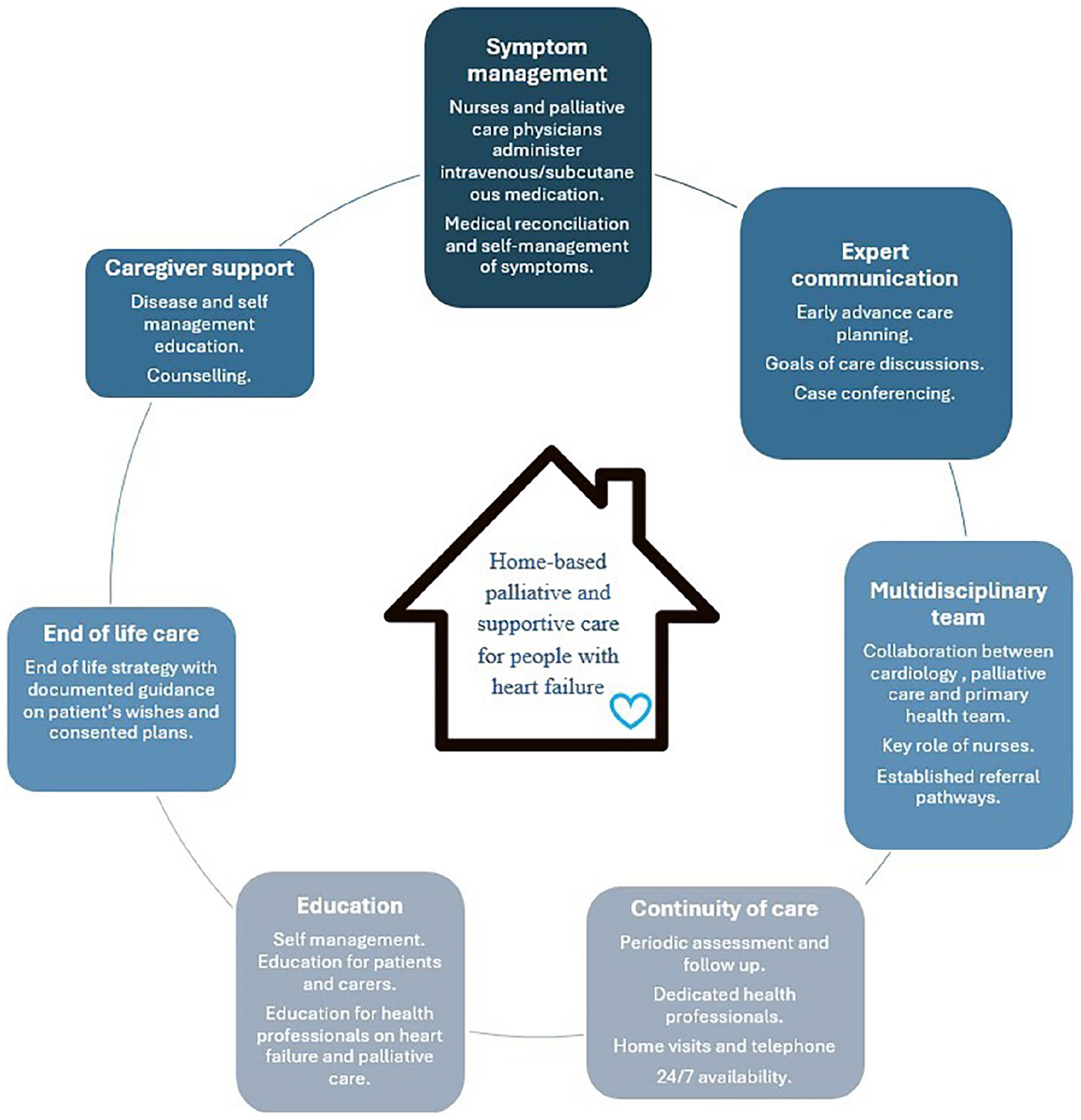
Components of home-based palliative and supportive care in heart failure.
Symptom management (Physical/ Psychological/ Spiritual/ Existential)
Symptom management was a component reported in all articles as it was pivotal to ensure health related quality of life among people with heart failure when providing palliative and supportive care in the home setting 46 and to address heart failure symptoms.33 –45 Identification and management of physical symptoms was noted among all included studies and was carried out by dedicated health care provider delivering the service/intervention. Managing both physical and psychosocial symptoms in the home setting was also mentioned in two studies37,38 with three other studies focussed on physical, psychosocial and spiritual symptoms.33,39,41
Heterogeneity was observed in medication administration route for symptom management in the home. Five articles based on three studies described intravenous administration of drugs for people with heart failure receiving a palliative and supportive care approach at home33 –35,40,44 for alleviation of physical symptoms of heart failure (mainly breathlessness and oedema). Dedicated nursing staff40,44 and palliative care physicians assisted by nursing staff 34 were involved in home administration of intravenous medication.
Medical reconciliation 39 – the process of obtaining, verifying and documenting an accurate list of medications the person is currently prescribed in order to identify and resolve discrepancies, – and optimising medication for palliation by reviewing the medication with adjusting and omitting of medication was reported in three studies in the home.33,39,41 Strategies for de-prescribing, including identification and timing of de-prescribing was not reported. Self-management of symptoms at home was reported in the majority of studies.33 –39,41 –43,45 None of the studies reported use of self-administered instruments by persons with heart failure in identifying and reporting of symptoms. One study mentioned an education booklet which contained information on symptom identification and self-management, including guidance on when to contact health care providers. 38
Expert communication (shared decision making/advance care planning/re-visiting goals of care)
A key component of home-based palliative and supportive care for people with heart failure was expert communication and the specific care providers involved in communication varied among the reported studies. Communication between people with heart failure, caregivers and health care providers occurred in the form of shared care provision, and centred around advance care planning,33 –35 revisiting goals of care,33 –35,39,41,42 clarification of preferences, spiritual care, 39 counselling,35,41 –43 case conferencing39,40 and end-of-life discussions.34,41
Use of frameworks for advance care planning was reported in a Swedish study, which described the six S model, underpinning principles of patient centred care led by nurses. 34 The Six S model included the following key aspects in delivering home-based palliative and supportive care: self-image, self-determination, social relationships, symptom control, synthesis and surrender. 34 Only one study highlighted the health professionals who had a key role in advance care planning with specific support for documentation of advance care directives offered by nursing staff and social workers in a quality improvement programme in United States. 39 In addition, the social worker engaged in a conversation on goals of care throughout the disease trajectory, linking the person and caregiver to the community resources. 39 Identification of a substitute decision maker36 –38 was also included to strengthen a persons’ wishes especially during end-of-life. Initiation of expert communication was either by the person with heart failure or the care provider, usually at the first consultation in the home and continuing through the length of the interventions.
Multidisciplinary team involvement
Provision of home-based palliative and supportive care was carried out in collaboration with varying disciplines across settings. Either multidisciplinary (knowledge is drawn from different disciplines while maintaining boundaries of the disciplines) and interdisciplinary (linking of different disciplines in a synthesised manner) involvement was observed in all studies33 –44 except for a self-management intervention carried out in Iran. 45
Nurses were involved in care provision in all studies. The role of coordinating patient care with the multidisciplinary team was undertaken by palliative care physicians36,37,39 or home palliative care nurses33,40 –43 and heart failure nurses. 44 Involvement of primary care physicians, cardiology and palliative care teams was common among the studies.33 –38,44 Inclusion of a chaplain, 39 and counsellor 43 was noted less frequently. Occupational therapists and physiotherapists were included in some studies based on patient needs,33 –35,39 and dieticians and social workers 39 were other disciplines that sometimes formed the multidisciplinary team.
Established referral pathways for people requiring further intervention (e.g. following abnormal investigations) were noted in the home care setting.33,37 –39,42,43 Home care providers referred people with heart failure to treating physicians, primary care providers or in certain instances to hospice certified palliative care physicians (for additional intensive therapies).33,37 –39,42,43
Continuity of palliative and supportive care
Continuity of palliative and supportive care in a holistic manner can improve quality of life, minimising care fragmentation.7,8 Strategies to initiate and continue palliative and supportive care for people with heart failure at home included multidisciplinary team of care providers and physical examination and assessment of the patient in a holistic manner, including assessment of comorbidities.33 –35 Following initial consultation and assessment of the patient, most studies included periodic assessment and follow-up was conducted and tailored to the individual patient.
A Swedish study33 –35 reported continuity of patient care coordinated by a dedicated palliative care physician, with continuous communication with the patient’s treating cardiologist and primary care provider to provide seamless care. Cardiologists were reported as remaining involved in the care until death in three studies, facilitating the continuum of care across disciplines.33 –35
Variation was observed between studies, when contacting people with heart failure through home visits and/or telephone for provision of continued care. While in some cases, the frequency was determined by the person, some programmes had the treating physician deciding based on the acuity of the person’s illness. 40 Frequency of home visitation reported in studies varied from daily40,44 to weekly or monthly33,34,36,41,42 as did the telephone consultations.
Care provision after hours33 –35,45 and care provided 24/7 via telephone consultations36 –38,41,42,45 were reported. A palliative care transitional model used home visits and telephone consultations alternately for care provision, which was intensely carried out in the first month and later sustained monthly.41,42 No clear guidelines were reported to decide the frequency or intensity of home visits.
Education (people and health care providers)
Education of persons with heart failure and caregivers was reported among the included studies,33 –39,41 –43,45 in particular, for symptom management and self-management.39,41,43 Nurses were the health care providers who delivered education in the majority of reported studies. Two studies used printed educational material containing information on the natural history of heart failure, management of symptoms and on how to liaise with health care providers.38,45 The timing of initiation and frequency of education varied between the two studies. The Canadian study delivered education at the beginning of the study recruitment period at a single time point, 44 while the study in Iran, 34 primarily providing an intervention based on self-management, delivered education during the pre-planned sessions of the intervention, which occurred bi-weekly for a month. Another study provided education via a nurse at time of care initiation 39 but did not mention the mode of education (i.e. lectures and leaflet). In studies that mentioned providing education to persons with heart failure and caregivers, frequency of delivery was not reported in three studies.39,41,43 The place of providing education included home-visits 39 through to telephone conversations.
Education of health care providers was reported in four studies.34,38,39,44 Ongoing professional education on management of home-based heart failure and standardised protocols for clinical care (e.g. home diuretic administration) was delivered to palliative care physicians using pamphlets, lectures and peer-to-peer support. 37 Mentoring of palliative care physicians also occurred, which strengthened collaboration with cardiologists. 38 A palliative care education programme containing an overview of palliative care specific to people with heart failure was delivered to a wide range of health care providers at a hospice care agency 39 using lectures, question and answer sessions and slide presentations. Another study reported that as part of ongoing team support, ‘team-based educational activities’ were conducted. 34 However, details on the ‘team-based educational activities’ (i.e. topics covered and how the education was delivered) was not mentioned. 34
End of life care
Despite communication of end of life care and documentation of advance care directives described in many studies, end of life care was only reported in one study where an end-of-life strategy with documented guidance on patient’s wishes and consented plans regarding resuscitation were mentioned. 34 It was reported to be provided by a nursing staff member (Six S model of care) but the timing of initiation of the care plan was not documented.33,34
Caregiver support
Caregivers are instrumental in provision of home-based heart failure palliative and supportive care and caregiver support to minimise caregiver burden is pivotal. 47 The studies reported education of caregivers on heart failure and symptom management33 –39,45 spiritual guidance 39 and counselling for caregivers41,42 as mechanisms for supporting caregivers.
‘Support to close relatives’ was identified as a key component, in an integrated palliative care model developed for people with heart failure in Sweden at home.33 –35 Explaining disease progression to the caregiver and providing support as and when needed via a phone call (including after-hours care for caregivers) were mentioned as caregiver support and were delivered by nurses and a palliative care physician. None of the studies specifically reported on education of caregivers to administer medication via intravenous or subcutaneous routes at home.
Spiritual support was provided by a chaplain during the home visit to the caregiver, allowing the caregiver to discuss distress and spiritual issues. 39 Counselling for caregivers was provided on psychological symptom management by a specialist palliative care nurse case manager.41,42 One study reported provision of ‘adequate caregiver support’ but did not report how the caregiver was supported. 43
Discussion
Main findings of the study
The findings of our review were organised into key components informed by previous frameworks. The importance of symptom management including medical reconciliation and self-management is a key component of home-based palliative and supportive care. Expert communication on advance care planning and goals of care discussions with patient’s wishes documented are crucial. Collaboration between multidisciplinary teams can facilitate continuity of care, enabled by periodic assessment and follow-up through home-visits and telephone calls by a dedicated health care provider. Education of patients, caregivers and health care providers is a component of home-based palliative and supportive care. Despite recommendations for early initiation of palliative care in heart failure,8,9,48,49 the findings from this review are consistent with the reported underutilisation of this approach to care among people who are early in their heart failure illness trajectory and not experiencing advanced stages of heart failure.7,8,17,45,50 Most studies reported in this review included individuals with advanced heart failure and only one study 36 included people with heart failure across all four New York Heart Association classes.
What this paper adds?
This review highlights that home visits and tele-health consultations are both used to manage heart failure symptoms.18,34,43,45 Identification of symptoms and promoting self-management is central to palliative and supportive care in the home setting, supported by a multidisciplinary team and underpinned by effective educational interventions for the person with heart failure and their caregivers. Expert communication and continuity of care were also identified as elements that could provide peace of mind to the person with heart failure and their caregivers while they navigate an unpredictable disease trajectory. 33
Digital health, described as the use of information and communication technology in health care, 51 can also be used to provide a wide range of services, irrespective of geographical boundaries.18,51 In this review, telephone communication was the only technology reported for care provided in the home, despite evidence to suggest the value of other digital health technologies in palliative care. 52
Expert communication was another key element of palliative and supportive care in heart failure, encompassing continuous ongoing conversations on shared care, advance care planning, setting of goals of care, end-of-life discussions and identification of care preferences. Early initiation of expert communication enables the person’s voice to be heard early and enable the person’s wishes to be respected across the illness trajectory. The Six S model, 33 integrating patient centred care was the only detailed communication framework mentioned. Despite challenges to initiation of expert communication reported in literature, 53 the home setting potentially provides a more conducive environment for discussion around goals of care, advance care planning and end-of-life discussions, as both the person and caregivers can be more at ease in their own environment. 54
Multidisciplinary team involvement in provision of home-based palliative and supportive care in heart failure, coordinated by a dedicated health care provider, appears critical to address the comprehensive and complex care needs of the patient.8,48 Nursing staff are strategically placed for provision of care across many care settings attending to the many and varied care needs of the person in a holistic manner33,38 –41,43 –45 This review identified that services provided by nursing staff extended to include assessment of care needs as well as comprehensive provision of care (whether it be intravenous or subcutaneous drug administration or individual and caregiver education or counselling or follow up etc.). This review also supports the case for continuous and early liaison with the palliative care team, cardiology and primary care provider to address the multitude of ever-changing requirements of the person and their disease.33,38,39,43
Strengths and limitations
A strength of our review was the inclusion of articles which included individuals with less severe heart failure (New York Heart Association Class I and II), in accordance with recommendations for early utilisation of palliative and supportive care5 –10 No time restrictions were imposed upon searching, allowing to capture a wide breadth of evidence. Various frameworks were inspected to identify the most suitable framework to organise the findings of this scoping review, building upon existing knowledge.
This scoping review did not examine unpublished grey literature and studies published in languages other than English. The studies reported in this review were all from high income countries. The lack of studies from lower and middle-income countries may have resulted from the English language restrictions set for this review and so global nuances were not captured. The selection of studies primarily focussed on people with heart failure even though caregivers are an integral component of home-based palliative and supportive care. A more complete understanding of palliative and supportive care that predominantly focusses on the caregiver is warranted.
Conclusion
There was heterogeneity in the services provided in the home-setting and health care approaches provided. The studies included in this review highlight that nurses, supported by a multidisciplinary team of other experts in cardiology, palliative care and primary care, are well placed to provide home-based palliative and supportive care. Continuity of palliative and supportive care with home visits and telephone consultation was an important part of the model in some studies, although more research on the role of digital health interventions in provision of home-based palliative and supportive care for people with heart failure is recommended. Expert communication on goals of care, the person’s preferences, advance care planning, end-of-life discussions and shared care are key to home-based palliative and supportive care with the potential to lead to better outcomes for people with heart failure, their caregivers and health care systems. Ongoing education for people with heart failure, caregivers and health care providers is crucial to enhance symptom management and sustain continuity of care. Empowering persons with heart failure and their caregivers to taken on an active role in symptom identification and management could be beneficial in the home setting.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241290350 – Supplemental material for Components of home-based palliative and supportive care for adults with heart failure: A scoping review
Supplemental material, sj-docx-1-pmj-10.1177_02692163241290350 for Components of home-based palliative and supportive care for adults with heart failure: A scoping review by Madhurangi Perera, Ureni Halahakone, Sameera Senanayake, Sanjeewa Kularatna, William Parsonage, Patsy Yates and Gursharan K. Singh in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241290350 – Supplemental material for Components of home-based palliative and supportive care for adults with heart failure: A scoping review
Supplemental material, sj-docx-2-pmj-10.1177_02692163241290350 for Components of home-based palliative and supportive care for adults with heart failure: A scoping review by Madhurangi Perera, Ureni Halahakone, Sameera Senanayake, Sanjeewa Kularatna, William Parsonage, Patsy Yates and Gursharan K. Singh in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_02692163241290350 – Supplemental material for Components of home-based palliative and supportive care for adults with heart failure: A scoping review
Supplemental material, sj-docx-3-pmj-10.1177_02692163241290350 for Components of home-based palliative and supportive care for adults with heart failure: A scoping review by Madhurangi Perera, Ureni Halahakone, Sameera Senanayake, Sanjeewa Kularatna, William Parsonage, Patsy Yates and Gursharan K. Singh in Palliative Medicine
Supplemental Material
sj-docx-4-pmj-10.1177_02692163241290350 – Supplemental material for Components of home-based palliative and supportive care for adults with heart failure: A scoping review
Supplemental material, sj-docx-4-pmj-10.1177_02692163241290350 for Components of home-based palliative and supportive care for adults with heart failure: A scoping review by Madhurangi Perera, Ureni Halahakone, Sameera Senanayake, Sanjeewa Kularatna, William Parsonage, Patsy Yates and Gursharan K. Singh in Palliative Medicine
Supplemental Material
sj-xlsx-5-pmj-10.1177_02692163241290350 – Supplemental material for Components of home-based palliative and supportive care for adults with heart failure: A scoping review
Supplemental material, sj-xlsx-5-pmj-10.1177_02692163241290350 for Components of home-based palliative and supportive care for adults with heart failure: A scoping review by Madhurangi Perera, Ureni Halahakone, Sameera Senanayake, Sanjeewa Kularatna, William Parsonage, Patsy Yates and Gursharan K. Singh in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge liaison librarians Marvin Van Prooijen and Cameron Rutter for their advice on developing and reviewing the search strategy.
Author contributions
MP, GS, SS, SK and WP contributed in conceptualisation and design of this scoping review. Manuscript was drafted by MP and critically revised by GS. SK, SS, WP and PY provided input to the manuscript. All authors have approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Madhurangi Perera is funded by a Queensland University of Technology Higher Degree Research Scholarship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.