
Abstract
Background:
Spiritual care is increasingly recognised as an essential component of care in palliative settings. Given this growing body of literature on spiritual interventions, there is a need to systematically evaluate and synthesis findings from previous systematic reviews
Aim:
To systematically synthesise the available evidence from systematic reviews concerning (a) the efficacy of spiritual care interventions and (b) the extent and nature of spiritual care interventions used in specialist palliative care settings.
Methods:
An umbrella review of systematic reviews was conducted in accordance with PROSPERO (CRD42024455147) and followed the Joanna Briggs Institute methodology for umbrella reviews.
Data sources:
Electronic databases (Ovid Medline, Embase, APA PsycINFO, Cochrane Database of Systematic Reviews, CINAHL and Web of Science) and references of accepted systematic reviews were searched for systematic reviews from inception to 2024. The AMSTAR-2 criteria was used to assess risk of bias within systematic reviews.
Results:
A toal of 27 reviews met the eligibility criteria and reported the effects of 14 different spiritual care interventions across 431 studies including 55,759 participants. Findings show that spiritual care interventions especially dignity therapy and life-review may be effective for improving outcomes including spiritual wellbeing, emotional symptoms, quality-of-life and physical symptoms in people receiving specialist palliative care. Under half of included reviews report follow-up data where only emotional symptoms and quality-of-life are reported at more than one time-point.
Conclusion:
Overall, spiritual care interventions have positive effects on spiritual wellbeing, quality of life and mood, compared to control conditions. Increased methodological rigour is needed to capture effect and duration of effect with spiritual care interventions at different phases of palliative care.
Spiritual care interventions are effective for increasing spiritual well-being, emotional symptoms and quality of life.
Despite a growing body of therapeutic evidence, patients receiving specialist palliative care still report a vital need for spiritual support.
The findings additionally report that spiritual care interventions have positive impacts on the fostering of hope, life, meaning and purpose and physical symptoms including pain.
The findings highlight uncertainty concerning the long-term effectiveness of spiritual care interventions in specialist palliative care settings.
Tailored implementation strategies are needed to enable trained palliative care multidisciplinary teams to routinely deliver spiritual care interventions.
Researchers are encouraged to investigate optimal dosing and frequency of spiritual care for people in different phases of palliative care.
Acceptability and tolerability of spiritual care interventions should be explored, especially for people in the last days or weeks of life.
Introduction
Terminal illness requiring specialist palliative care can be distressing for patients and their families experiences associated with terminal illness are felt physically with symptoms including pain, nausea and dyspnoea but also emotionally with negative feelings such as depression, social isolation and spiritual suffering. Although clinical assessment and support for physical, emotional and social suffering are common, attention to spiritual distress and suffering is still an overlooked component of palliative care.1,2 For these patients, spiritual distress increases anxiety, a sense of futility and represents a significant challenge to their personal beliefs and values. 3 Specialist palliative care services provide spiritual care interventions delivered by clinicians and other healthcare workers as part of a multidisciplinary team. The team has specialist training to deal with complex physical, psychosocial and spiritual symptoms and whom therefore have a higher level of expertise compared to general palliative care. 4
Spiritual wellbeing is now considered one of the most important influences on quality of life in people receiving specialist palliative care. 2 Over the past decade, the importance of addressing spiritual needs has been strengthened with clinical studies 5 and systematic reviews2,6,7 that show positive effects of spiritual care interventions in finding meaning, purpose and value in life, a sense of belonging and inner peace.2,6 The need for spiritual care has been recognised by several bodies including the World Health Organisation, 8 Palliative Care Australia 9 and the European Association for Palliative care (EAPC). 10 Although confusion remains surrounding concepts of spirituality, recent studies cite the EAPC’s working definition of spirituality given here.
Spirituality is the dynamic dimension of human life that relates to the way persons (individual and community) experience, express and/or seek meaning, purpose and transcendence, and the way they connect to the moment, to self, to others, to nature, to the significant and/or sacred.
10
The aim of this umbrella review is to systematically synthesise available evidence from systematic reviews concerning a) the efficacy of spiritual care interventions and b) the extent and nature of spiritual care interventions used in specialist palliative care settings. Recognising the efficacy of these interventions is crucial for health and pastoral care providers, as it can guide the integration of spiritual care into standard palliative practices, enhancing the quality of care delivered to people receiving specialist palliative care.
Methods
Design
The methodology of this review was informed by the Joanna Briggs Institute’s methodological guidance for conducting umbrella reviews 11 and was reported according to the Preferred Reporting Items for Overviews of reviews (PRIOR) statement. 12 Given the number of reviews previously exploring the effects of spiritual care interventions in specialist palliative care settings, an umbrella review was chosen as the most appropriate methodology to synthesise this area of knowledge. No meta-analysis were conducted due to the heterogeneity of both interventions and outcome measures used in included studies. This umbrella review was prospectively registered in PROSPERO (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=455147) to identify, screen and describe the protocols of this review.
Search strategy
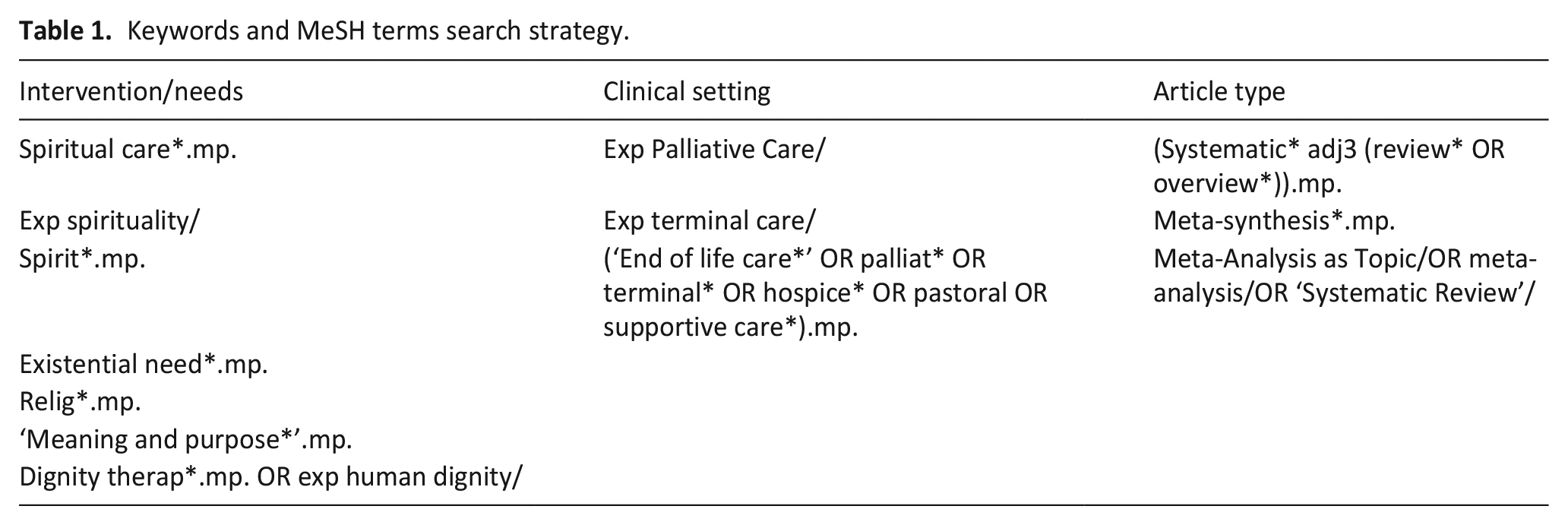
A search was conducted of relevant systematic reviews identified by the title and abstract in Ovid (Medline, Embase, APA PsycINFO, Cochrane Database of Systematic Reviews), CINAHL and Web of 13 Science from inception to March 2024. A summary of the keywords and MeSH terms are shown in Table 1, while individual database search strategies are shown in supplementary file 1. Only systematic reviews written in English were accepted. Due to the potential for variability in language and terminology related to spiritual care interventions, the OR Boolean operator was used to broaden search results and maximise the number of matches so none were excluded. 13 The AND Boolean operator was used to bring the three concepts together (supplementary file 1). Searches were also performed across all references list of accepted articles while searching for grey literature was done on Google and Google Scholar.
Keywords and MeSH terms search strategy.
Inclusion criteria
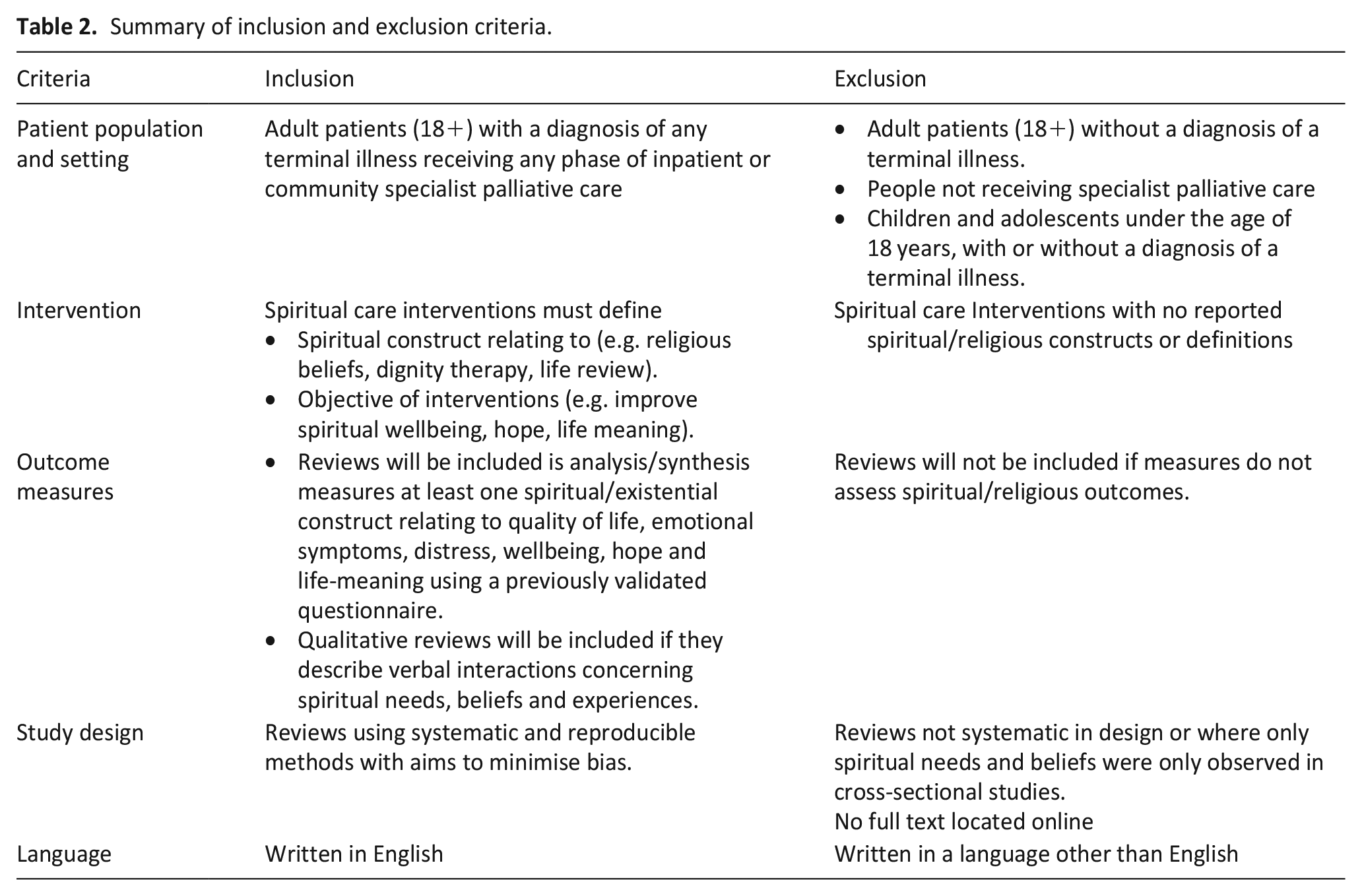
Following the exclusion of duplicates, titles and abstracts of all studies were assessed against inclusion and exclusion criteria (Table 2) by two independent reviewers (P.A. and W.L.). Characteristics of studies excluded at full text review are shown in supplementary file 2.
Summary of inclusion and exclusion criteria.
Data extraction
To determine inclusion eligibility, titles and abstracts from results of the search were independently screened and data extracted by two authors (PA, WL) between 12th and 16th of March, 20204 using Covidence systematic review software. 14 All reviewers read and agreed on the included articles. At each stage disagreements were resolved through discussion between PA, WL and ML. After removing duplicates, two authors (PA, WL) independently assessed the eligibility of each abstract and title returned by the search strategy. Full texts of studies meeting the inclusion criteria were evaluated for inclusion. Conflicts of agreement were resolved by consensus with all authors (PA, WL, ML, RK). The process of data selection is shown in PRISMA Figure 1. Synthesis involved pooling the extracted data from the included systematic reviews. Here, all data relating to demographics, interventions, comparators, outcome measures, findings and appraisal of systematic reviews was tabulated into a Microsoft Excel spreadsheet. From this, a narrative review of findings was developed based on the overall strength of the evidence and consistency of observed effects.
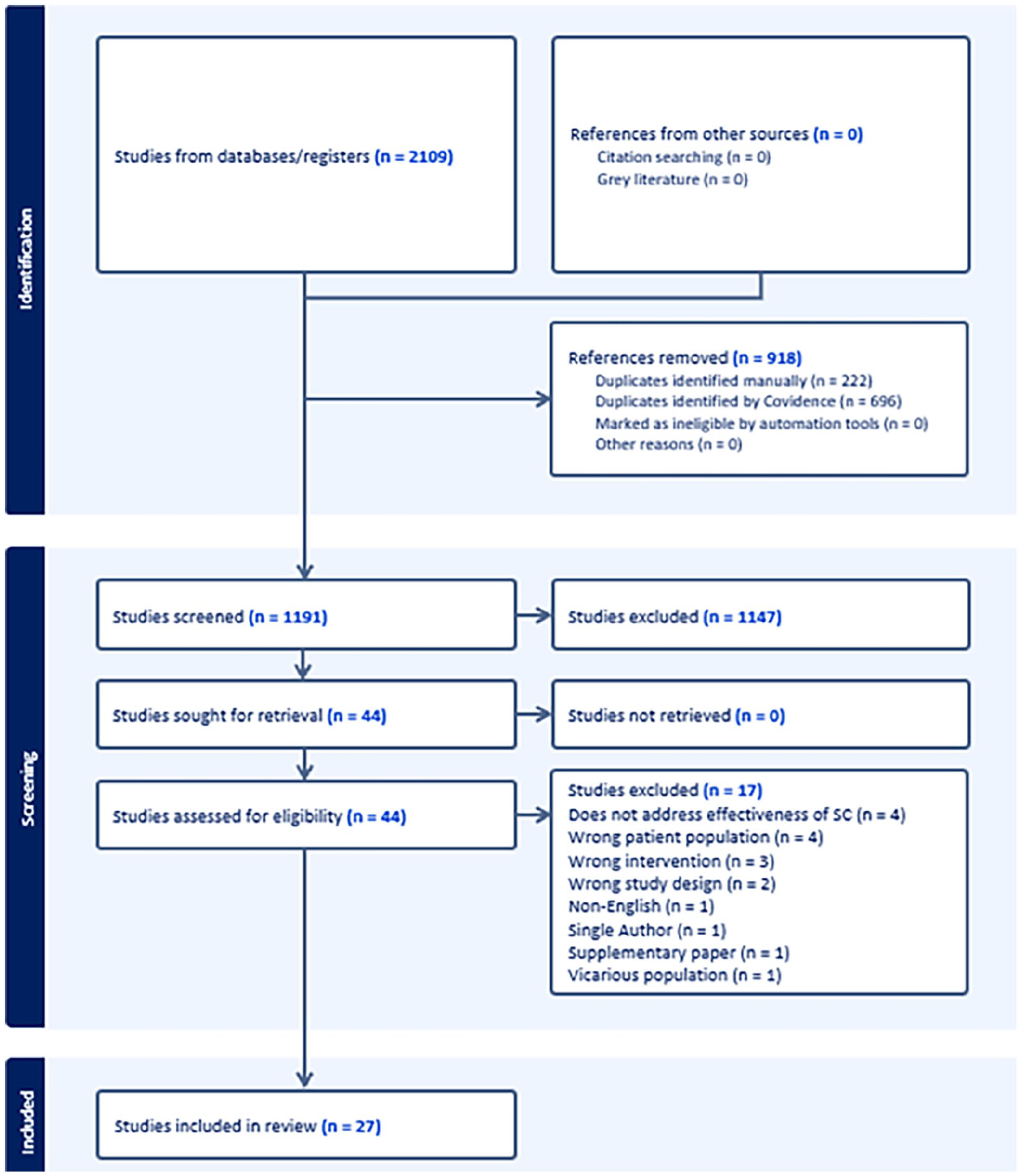
PRISMA flow diagram, preferred reporting items for systematic reviews and meta-analysis.
Overlap of primary studies
Overlap of primary studies across included systematic reviews was quantified by calculating the Corrected Covered Area (CCA); the proportion of primary studies included across multiple systematic reviews. 15 A citation matrix was compiled (supplementary file 3) to document all primary studies and their corresponding systematic reviews after which the CCA was calculated as a percentage of publication overlap in this umbrella review as formulated by Kirvalidze and colleagues. 15 0%-5% is considered as ‘slight overlap’, 6%-10% is considered as ‘moderate overlap’, 11%-15% is considered a ‘high overlap’ and >15% is considered as ‘very high overlap’.
Systematic review appraisal
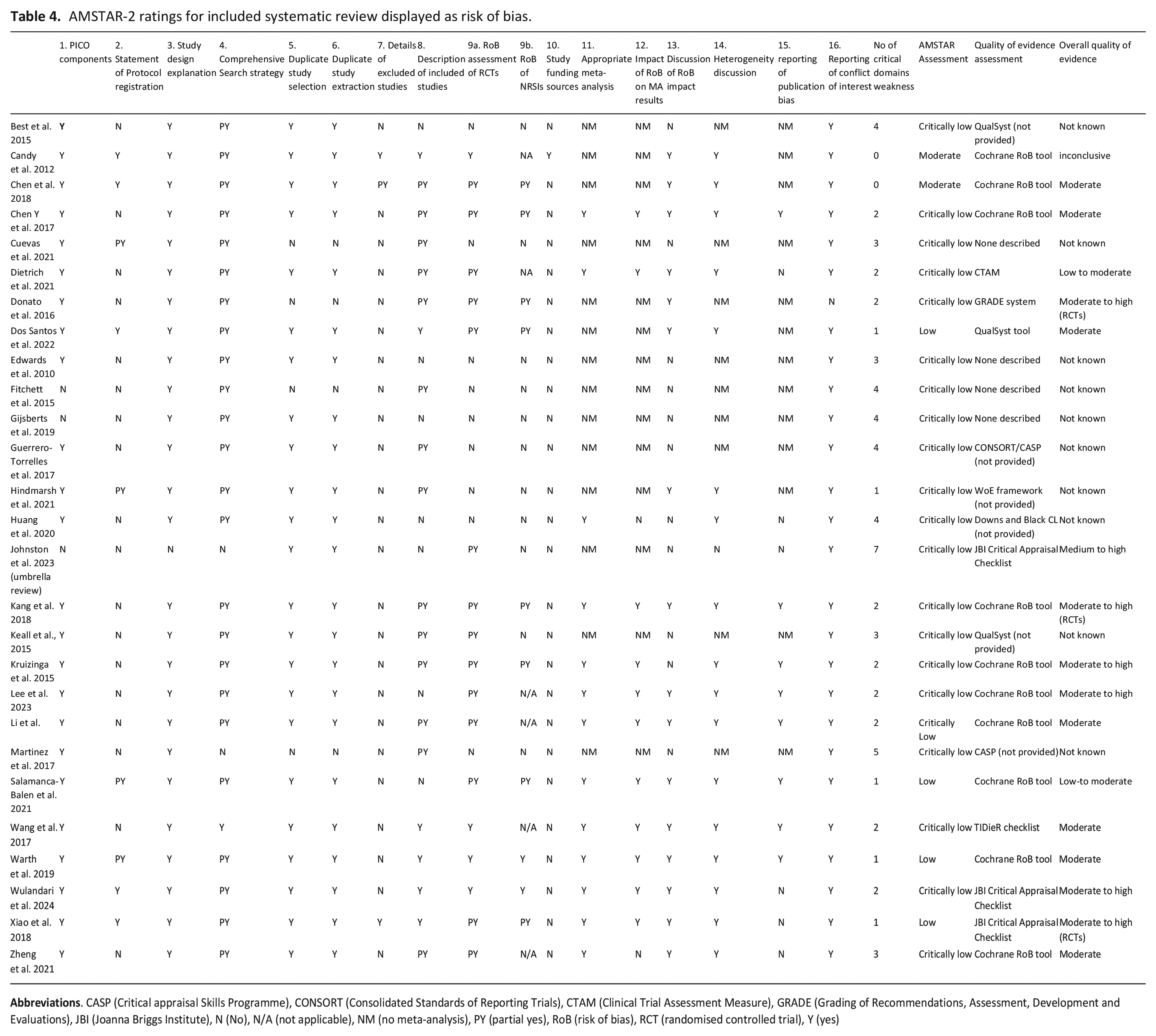
Risk of bias of included systematic reviews was assessed using the AMSTAR 2 (Assessment of Multiple Systematic Reviews) checklist. 16 AMSTAR 2 is a 16-item checklist that includes critical domains relating to (1) protocol registration prior to review commencement, (2) Adequacy of literature search, (3) justification for excluding individual studies, 4) risk of bias from individual studies included in review, (5) appropriateness of meta-analysis, (6) consideration of risk of bias when interpreting review results and (7) assessment of presence and likely impact of publication bias. 16 Two reviewers (PA and ML) independently rated review quality where differences in evaluation were noted and resolved by discussion. If disagreement was not reached a third reviewer (RK) resolved any discrepancies.
Overall ratings for each study considers flaws in each critical domain which may weaken confidence placed on results in each systematic review and are categorised as follows: High – where all critical domains and no more than one non-critical weakness is evident and provides an accurate and comprehensive summary of results; Moderate – more than one non-critical weakness, but no critical flaws, and may provide an accurate and comprehensive summary of results; Low – one critical flaw with or without non-critical weaknesses and may not provide an accurate and comprehensive summary of results; and Critically low – more than one critical flaw, with or without non-critical weaknesses and thus, should not be relied upon to provide an accurate and comprehensive summary of results. 16
Results
Study selection and characteristics of included studies
Our systematic search retrieved 2109 potential articles (Figure 1). After full text scrutiny, 27 systematic reviews with 431 studies and involving 55,759 participants were included for review. The 27 systematic reviews covered 269 non-overlapping studies. Overall, the CCA showed a slight degree of overlap (2.3%) between primary studies. (Supplemental Table 3). Only five primary studies were included in over 25% of systematic reviews,17 –20 however Chochinov and colleagues 2011 dignity therapy RCT was cited in nearly 60% of systematic reviews. 21
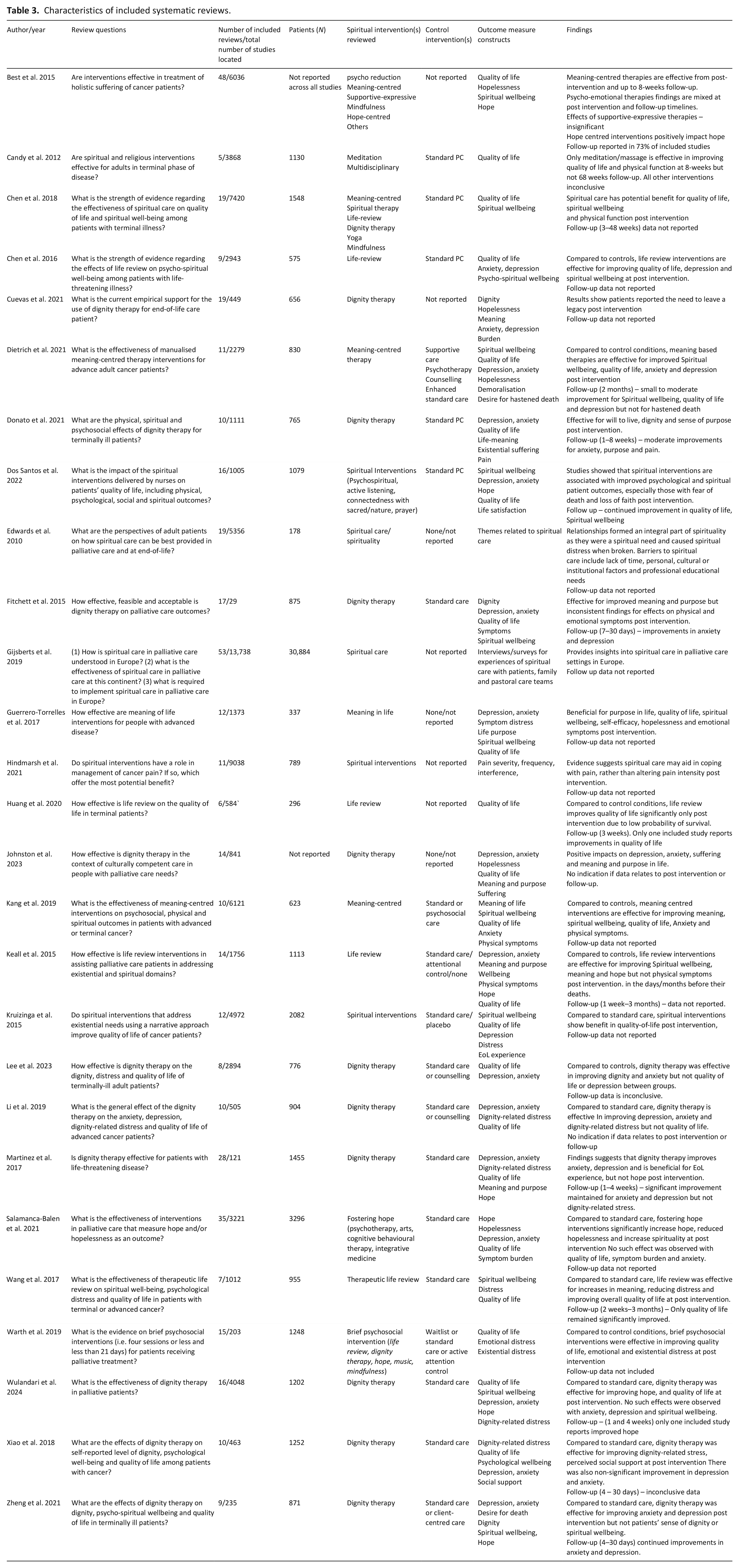
The characteristics of the included studies are shown in Table 2. Of the 27 systematic reviews (12 with meta-analysis22 –33), five included only randomised controlled trials (RCTs),26,27,29,31,34 12 included RCTs and quasi-experimental/non-randomised clinical trials,3,22,24,25,28,30,32,33,35,36,37,38 five included intervention trials regardless of design,23,39 –42 three included both quantitative and qualitative studies,1,43,44 one included only qualitative studies, 45 while one other included systematic reviews and meta-analyses. 46 Only 11 (42%) studies reported follow-up data that ranged between 4 days and 3 months.
Concerning spiritual care interventions, 10 reviews included a range of spiritual interventions for spiritual distress.1,3,25,28,32,34,35,37,40,45 Ten reviews included studies only investigating dignity therapy,26,27,30,31,33,37,39,42,43,46 four included studies only investigating therapeutic life review,23,29,36,41 while three included only meaning-centred interventions.22,24,44 The main comparator was usual palliative care, placebo, waitlist or psychosocial care. In total, 431 studies were included in accepted systematic reviews. The most frequent evaluated outcomes were for spiritual wellbeing, quality of life, dignity, anxiety, depression, hopefulness and life meaning and purpose.
Quality of evidence
Using the AMSTAR 2 critical appraisal tool for systematic reviews, only two reviews were found that were judged as moderate quality,6,34 while four reviews were judged as low quality28,30,32,38 (Table 3). The remaining 21 reviews were missing at least two critical domains as detailed in the methods section above. Only three studies included details of excluded studies6,30,34 and eight reviews contained an explicit statement that review methods were established prior to the conduct of the review.6,28,30,32 –34,39,40 Thirteen studies performed meta-analysis, 12 of which reported satisfactory explanations for heterogeneity, while 10 provided risk of bias assessment in individual studies. Twenty-three studies reported PICO components. Twenty-two reviews conducted study selection and extraction with at least two reviewers.
Characteristics of included systematic reviews.
Twenty-three studies assessed quality of evidence of included reviews. However, six did not provide quality assessment results. Ten studies used the Cochrane risk of bias tool,6,24 –28,31,32,34,36 three used the Joanna Briggs Institute critical appraisal checklist,30,46 three used QualSyst35,38,41 and two used the Critical Appraisal Skills programme tool.42,44 Further reviews used the Template for Intervention Description and Replication checklist, 29 GRADE system 37 Clinical Trials Assessment Measure, 22 Weight of Evidence Framework 40 and finally, the Downs and Black checklist. 23 Five reviews describe overall evidence as moderate-to-high.24,30,33,37,46 Seven reviews report overall evidence as moderate,6,27,29,31,32,36,38 two reviews as low-to-moderate,23,29 one review as inconclusive, 34 while all remaining reviews do not report quality of evidence (Table 4).
AMSTAR-2 ratings for included systematic review displayed as risk of bias.
Efficacy of spiritual care interventions
Dignity therapy
The effects of dignity therapy was the most reviewed spiritual care intervention both specifically26,27,30,31,33,37,39,42,43,46 and as part of reviews examining spiritual care interventions in general.4,25,32,35,40,45 Dignity therapy is a psychological intervention that helps terminally ill patients reflect on their lives and create a meaningful legacy document. 21 Findings from studies only reviewing the effects of dignity therapy suggest that this therapy is most effective for reducing levels of existential distress27,30,33,35,37,46 and improving quality of life.33,21 However, findings are mixed between systematic reviews for the efficacy of dignity therapy for emotional symptoms where five studies reported improvements in anxiety and depression whereas three other systematic reviews showed dignity therapy to be of no benefit.30,37,43 Only one review examined the effects of dignity therapy on physical symptoms where efficacy was reported as inconsistent. 43 In one review exploring the effects of spiritual care on cancer pain, dignity therapy along with other spiritual care interventions were more shown to help people cope with cancer-related pain rather than reduce its severity. 40 Four of five located studies also showed dignity therapy to positively influence spiritual wellbeing and meaning and purpose in life.4,37,43,46 Interestingly, Best and colleagues in their review found that dignity therapy only showed significant therapeutic effects when baseline distress was high. 35 Cuevas and colleagues in their review of therapeutic effects of dignity therapy at end-of-life showed that participants need to leave a legacy as a means to relieve spiritual distress. 39 Lastly, high levels of satisfaction with dignity therapy were shown in all reviews reporting this finding.38,43 Six studies reported follow-up data where five reviews showed continued improvements in anxiety and depression31,37,42,43,46 while the remaining review reported inconclusive data.30,43 Findings should be interpreted with caution as nine/10 studies were assessed as critically low for methodological quality using the AMSTAR-2 criteria due to failure to report publication bias, excluded studies and pre-registered study protocols.
Life-review
The therapeutic value of life review interventions were also explored specifically23,29,41,44 and as part of wider spiritual care reviews.4,25,32,35 Life review is a therapeutic process where individuals reflect on their past experiences and significant life events to find meaning and resolve unfinished business. 47 All studies show positive therapeutic effects of life-review on spiritual wellbeing,4,29,35,36,41,44 quality of life23,29,36,41,44 and distress29,41,44 compared to control conditions. Only two reviews showed pooled decreases in anxiety and depression,41,44 while another showed reduced depression and not anxiety. 36 Although other reviews describe effects of life review on emotional symptoms, there were insufficient studies to pool data. One study reported the effects of life review on physical symptoms where no significant decreases were found. 41 Few studies located among selected reviews report levels of satisfaction towards life review. Only two reviews reported follow-up data, both reporting continued improvements in quality of life.23,29 All studies investigating life-review were assessed as critically low for methodological quality, especially concerning risk of bias assessments, details of excluded studies and failure to register study protocols and report details of excluded studies.
Meaning-centred interventions
Four reviews explored the effects of meaning-centred interventions, two specifically,22,24 and two as part of reviews exploring effects of spiritual care interventions.4,35 Meaning-centered interventions focus on helping people with terminal illnesses, find meaning and purpose in life despite their suffering. 48 Meaning-centered interventions in all four studies show improvements in quality of life, spiritual wellbeing, anxiety and depression. Kang and colleagues also showed that meaning-centered interventions was effective for reducing physical symptoms including pain. 24 Of the reviews specifically addressing meaning-based interventions, Dietrich and colleagues included only studies using Frankl’s conceptualisation of logotherapy, 22 while Kang and co-workers included all forms of individual or group interventions that included meaning of life therapy, meaning making interventions and logotherapy resilience and education programs. 24 Interestingly, Chen and colleagues categorised studies investigating dignity therapy and life review interventions as meaning-based in their review. 6 Best and colleagues provide additional evidence suggesting that positive effects can be gained even with short-term interventions regardless of whether therapies are delivered to individuals or groups. 35 One review of meaning-centered studies reported follow-up data showing small to moderate improvements in spiritual wellbeing, quality of life and depression, compared to control conditions. 22 Methodological quality was again assessed as critically low in three studies, however the work of Chen and colleagues fulfilled all AMSTAR critical domains of methodological quality. 6
Other spiritual interventions
Reviews exploring the effects and forms of spiritual and psychosocial care in palliative care settings found further spiritual interventions including fostering hope,28,35 meditation,6,36 mindfulness-based stress reduction6,32,35 and yoga. 6 Concerning fostering hope, findings from both studies suggest that these interventions can significantly impact hope.28,35 With pooled data from 35 studies, Salamanca-Balen and colleagues show that hope-centered interventions also increase spirituality and reduce depression but do not reduce hopelessness or quality of life. 28 The use of meditation as an intervention was examined by two reviews. Findings are mixed where Candy and colleagues show no significant difference between groups using meditation and usual care on quality of life and wellbeing. Later, Chen and co-workers found that people receiving meditation therapy show improvements in quality of life. However, Candy and colleagues reported that participants receiving meditation and massage report greater levels of quality of life compared to meditation alone. 34 Finally, Dos Santos and colleagues examined clinical trials using spiritual, existential, religious and mixed interventions. 38 Overall, these interventions these interventions have a beneficial effect on life satisfaction, spiritual wellbeing and mood. Concerning follow-up data for these interventions, only Candy and colleagues reported no significant differences from baseline to follow-up. 34
Discussion
Main findings
This umbrella review provides a comprehensive assessment and update of evidence on the effectiveness of a wide range of spiritual care interventions for people receiving specialist palliative care. However, high-quality of evidence for the efficacy of these interventions is limited. Results from 431 clinical trials including 55,759 participants show dignity therapy and life review have been the most thoroughly examined but all modes of care can be effective for improving a range of outcomes including spiritual wellbeing, emotional symptoms and quality-of-life. Positive impacts were also reported on the fostering of hope, physical symptoms including pain and life meaning and purpose. However, evidence relating to hopelessness and symptom burden was inconclusive. The methodological quality of existing systematic reviews investigating the effects of spiritual care in specialist palliative care settings is critically low when assessed using AMSTAR-2 evaluation criteria. Although the need for more rigourous methodology is obvious, spiritual interventions do elicit signals of relief for negative emotions and physical symptoms as well as improvements in wellbeing, quality of life and the ability to cope with their disease.
Our findings also highlight the uncertainty concerning the long-term effectiveness of spiritual care, which is uncertain in specialist palliative care settings, as less than half of included reviews report follow-up data where only emotional symptoms and quality of life are reported across up to four reviews. This finding is not surprising where due to the low probability of survival, increase in burden and distress, spiritual care interventions may be beneficial in the short-term. As such, more rigourous methodology should be implemented when defining study populations and follow-up timepoints. It is important to recruit participants from defined phases of palliative care as their needs, wellbeing and quality of life change over time and thus effect the success and duration of effect for a given spiritual intervention at given timepoints along the disease trajectory. Included studies in this review broadly defined their populations as ‘palliative care’, ‘advanced cancer’ or ‘terminal illness’. Considering these factors, it is worth considering the suitability of specific spiritual care interventions to people in different phases of palliative care. Importantly, early palliative care has recently been identified as a time where clinicians have a chance to establish connections with patients and their families. 49 This is defined as early integration of palliative care into standard care of solid tumours and haematological malignancies. 50 These connections not only broaden scope for symptom management, but also implementation of positive psychospiritual wellbeing that may incorporate outcomes including fostering of hope and spiritual wellbeing. Spiritual interventions initiated earlier in palliative care may assist people to cope earlier with the challenges of life-limiting disease more effectively by addressing their emotional, social and spiritual needs.49,51 Indeed, the inclusion of spiritual interventions earlier in a person’s illness course will allow for the evaluation of long-term treatment effects at follow-up periods along illness trajectories.
Although most located studies assessed the effectiveness of dignity therapy and life-review on spiritual wellbeing, mood, physical symptoms and quality-of-life, other interventions located in this review, namely those aiming to foster hope and promote a sense of meaning should be described. Commonly, spiritual interventions are often measured against other outcomes (e.g. spiritual wellbeing, quality-of-life and mood variables) where hope and/or hopelessness and meaning are assessed as secondary outcomes 17 and thus may not be included for assessment in systematic reviews. In the face of terminal illness or other vulnerable circumstances, hope appears to energise a person for future adaptation and finding meaning in life. 52 Psychospiritual interventions shown to foster hope and/or diminish hopelessness and increase meaning 53 in specialist palliative care settings support findings from systematic reviews included in this study. 28
Advantages of this study
Currently, this is the most thorough umbrella review investigating the efficacy of spiritual care interventions in specialist settings. Only one previous umbrella review evaluated the effect of dignity therapy and included 14 systematic reviews from five databases. 48 Our umbrella review identified 27 systematic reviews from six databases and associated reference lists for critical evaluation and synthesis. This review reports the therapeutic effects from a wide range of spiritual interventions in different palliative care settings across 12 countries. Furthermore, the quality of each systematic review included in this review was critically appraised using the AMSTAR-2 checklist.
Limitations of this study
Findings from this review should be interpreted alongside some methodological limitations. First, it must be acknowledged that terminology relating to palliative is wide-ranging and although common search terms were used, related literature may have been missed. Second, although efforts to avoid methodological and publication bias were made, most included reviews lacked methodological quality where only 2 of 27 included studies were assessed as moderate quality using AMSTAR-2 assessment criteria. Third, it was found that high quality evidence of spiritual care is lacking where nine reviews did not provide quality of evidence assessments and across the remaining reviews, quality of evidence was rated as moderate.
Implications for clinicians and health policy makers
Given the benefits of spiritual care interventions on spiritual wellbeing and psychological outcomes, healthcare professionals should consider providing spiritual care as an integral part of usual healthcare planning in specialist palliative care. The myriad of spiritual care interventions identified allow healthcare professionals to select individually tailored spiritual care interventions for people depending on their spiritual needs and cultural background to improve outcomes. A significant proportion of people experience psychoexistential distress towards the end-of-life. 54 Thus, given the short duration of effect of many spiritual care interventions, strategies that enable regular delivery of spiritual interventions should be established as part of standard of care to ensure the continuation of benefit from spiritual care. Strategies should include the involvement of trained palliative care multidisciplinary members (nurse, pastoral care and social worker) to routinely deliver such care. 55 Building collaborations between the local palliative care services with the existing psychology and psychiatry services, trained in delivering spiritual care and relevant interventions is strongly recommended to allow timely access of spiritual interventions should there be escalating psychoexistential distresses. 56 If resourcing is an issue, training and utilising community volunteers to deliver such may also be useful.57,58
Implications for research
Although our findings suggest that spiritual care interventions are beneficial for people receiving specialist palliative care, it is unclear which interventions are most effective for what outcomes at each phase of palliative care. However, despite this heterogeneity, our synthesis of findings do provide a basis for researchers to focus their investigations towards both the efficacy and duration of effect from interventions on outcomes at different phases of palliative care. For example, certain interventions may show positive long-term effects for increasing mood and quality-of-life in early phases of palliative care but are ineffective or are only briefly beneficial for people who are distressed receiving end-of-life care. This being the case, future studies should also consider investigating the optimal frequency and dosing of various spiritual care interventions (e.g. twice weekly dignity therapy at short duration of 30 min sessions rather than weekly 1-h session) for patients in different phases of disease trajectory. 59 Furthermore, the acceptability, safety and tolerability for these interventions will also need to be explored, particularly for people in the last days to weeks of life where most trials excluded this population. It is further suggested that future research must consider increased homogeneity within participant groups, not only palliative care phase but also disease type, cultural background and if relevant, age and gender. The effect of spiritual interventions on various psychological outcomes such as depression and anxiety should also be explored more in-depth.
Future systematic reviews must increase their methodological rigour by reporting that (a) protocols are established prior to the conduct of reviews, (b) accurate reporting of risk-of-bias assessments and (c) if applicable, conduction appropriate meta-analysis with subsequent reporting of heterogeneity and publication bias. These methodological considerations would help researchers develop clinical trials to generate more accurate data concerning the optimal therapeutic duration of an intervention, appropriate follow-up timelines to illicit duration of treatment effects and provision of spiritual care interventions most suitable for a person’s cultural and religious beliefs.
Conclusion
Current systematic review data suggests that spiritual care interventions have positive effects on spiritual wellbeing, quality of life, mood and the ability of a person to cope with their disease, compared to control conditions. However, future studies would benefit from more rigourous inclusion criteria that would more accurately capture effects of spiritual care interventions at different phases of palliative care, especially at end-of-life.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241287650 – Supplemental material for Efficacy of spiritual interventions in palliative care: An umbrella review of systematic reviews
Supplemental material, sj-docx-1-pmj-10.1177_02692163241287650 for Efficacy of spiritual interventions in palliative care: An umbrella review of systematic reviews by Philip D Austin, Wei Lee, Robyn Keall and Melanie R Lovell in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241287650 – Supplemental material for Efficacy of spiritual interventions in palliative care: An umbrella review of systematic reviews
Supplemental material, sj-docx-2-pmj-10.1177_02692163241287650 for Efficacy of spiritual interventions in palliative care: An umbrella review of systematic reviews by Philip D Austin, Wei Lee, Robyn Keall and Melanie R Lovell in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_02692163241287650 – Supplemental material for Efficacy of spiritual interventions in palliative care: An umbrella review of systematic reviews
Supplemental material, sj-docx-3-pmj-10.1177_02692163241287650 for Efficacy of spiritual interventions in palliative care: An umbrella review of systematic reviews by Philip D Austin, Wei Lee, Robyn Keall and Melanie R Lovell in Palliative Medicine
Footnotes
Acknowledgements
We would like to thank The David and Judith Taylor Foundation for their financial support in grant funding PA over the course of this study.
Author contributions
PA, ML, WL and RK conceived and designed the study. PA completed all the searches and conducted the initial screen. Full manuscript reviews were conducted by PA, WL and ML. PA and WL interpreted the data. PA and WL drafted the manuscript and all authors have approved the submitted version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the David and Judith Taylor Foundation (Australia).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.