
Abstract
Background:
Spirituality refers to the dynamic dimension of human life that relates to the way that persons experience meaning, purpose, and transcendence. The complex task of parenting a child with a life-limiting condition may raise existential questions, which are easily overlooked by healthcare professionals.
Aim:
We explored how the spiritual dimension becomes manifest in parents of children in pediatric palliative care.
Design:
A mixed-methods systematic review was conducted, registered in Prospero (2021 CRD42021285318).
Data sources:
PubMed, CINAHL, Embase, PsycInfo, and Cochrane were searched for articles published between January 1, 2015 and January 1, 2023. We included original empirical studies that reported on spirituality of parents of seriously ill children, from parents’ perspectives.
Results:
Sixty-three studies were included: 22 North-American, 19 Asian, 13 European, 9 other. Studies varied in defining spirituality. We identified five different aspects of spirituality: religion, hope, parental identity, personal development, and feeling connected with others. All aspects could function as source of spirituality or cause of spiritual concern. Sources of spirituality helped parents to give meaning to their experiences and made them feel supported. However, parents also reported struggling with spiritual concerns. Several parents highlighted their need for professional support.
Conclusions:
Although studies vary in defining spirituality, reports on spirituality focus on how parents connect to their faith, others, and themselves as parents. Healthcare professionals can support parents by paying attention to the spiritual process parents are going through. More research is needed into how healthcare professionals can support parents of seriously ill children in this process.
Spirituality is recognized as an essential component of high-quality palliative care.
While spirituality in pediatric palliative has gradually gained some interest over the last few years, spiritual assessment and spiritual care do not seem to be a standard practice in care for families of children with life-limiting conditions.
An in-depth understanding of the spiritual dimension of parenting a child with a life-limiting or life-threatening condition may result in spiritual care needs of parents being better recognized and met by healthcare professionals.
With regard to spirituality, for parents caring for a child with a life-limiting or life-threatening condition, five aspects are important: how they connect to their religious beliefs; how they deal with hope; their parental identity; their personal development; and how connected they feel to others.
All five aspects can function either as source of spirituality or cause of spiritual concern. However, there is a gap between the theory about spirituality, referring to spirituality as a process that is always there, and included studies referring to spirituality in terms of sources that give parents strength and causes of spiritual concern that bring confusion or frustration.
Parents have needs for spiritual support, but their needs are often not explicitly stated.
All healthcare professionals should be sensitive to the spiritual dimension in caring for parents with children with life-limiting conditions and support these parents more adequately and systematically in their spiritual process.
In future research, a clear definition of the concept of spirituality underlying a study would be helpful in bringing theory on spirituality and healthcare practice closer together.
Introduction
Dealing with a life-limiting illness can present patients and their families with considerable challenges. The same is true for children, adolescents, young adults, and their families, when diagnosed with a life-limiting illness. The often unpredictable and sometimes erratic course of the disease, and the confrontation with how transient life is, give rise to spiritual questions and challenges.1–4 Spiritual well-being is very important to patients with an advanced illness. 1 It can offer some protection against despair for adults at the end of their lives 5 as well as for pediatric patients 6 with an advanced illness, and the parents of ill children. 7 Since the 1990s, a large and growing body of literature on palliative care in general has addressed the importance of spirituality as one of its four dimensions. Besides the physical, psychological and social dimension, the spritual dimension is also recognized as an indispensable component of high-quality palliative care.8–11
Although spiritual care is acknowledged as an essential component of palliative care,12,13 it remains a somewhat indistinct concept.14–17 Whereas spirituality used to refer predominantly to faith and religion,15,18 the concept has gradually become broader, signifying the universal process of searching for meaning in connection with the world around us.12,14,19 With the aim of reaching an international consensus, the EAPC Reference Group on Spiritual Care proposed an overarching definition of spirituality in palliative care that can be found under the heading ‘Definition of spirituality in palliative care’ in the methods section. 12 We have chosen for this definition as guidance for this systematic review, because this broad definition suits well the current use of the concept of spirituality in palliative care and does not differ significantly from other important international consensus definitions.16,20The EAPC definition suggests that spirituality has not only religious and, or transcendental connotations, but also refers to the universal process of searching for meaning in everyday human experience.19,21,22
While spirituality in palliative care has gradually gained some interest over the last few years, the majority of the literature focuses on spiritual care for adult patients and their caregivers.9,16 Fewer studies have investigated the ways in which spirituality in daily life is perceived by parents of children in palliative care, although experiencing the life-limiting illness and death of one’s own child is known to be extremely challenging for parents.3,4 Spiritual assessment and spiritual care, meanwhile, do not seem to be a standard practice in care for families of children with life-limiting conditions. 23 An in-depth understanding of the spiritual dimension of parents’ experiences of taking care of a child with a life-limiting or life-threatening condition is still lacking 24 and may result in spiritual care needs remaining unmet. 25
Therefore the main research question for this review was:
How does the spiritual dimension, as defined by the EAPC Reference Group on Spiritual Care, becomes manifest in parents of children with life-limiting or life-threatening conditions?
Methods
Design
We conducted a mixed-methods systematic literature review with a convergent integrated approach to the synthesis and integration of findings. 26 This review is reported according to the updated Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement for reviews. 27 The protocol was registered in Prospero (2021 CRD42021285318).
Definition of spirituality in palliative care
Definition of spirituality adopted by the EAPC Reference Group on Spiritual Care
Spirituality is the dynamic dimension of human life that relates to the way persons (individual and community) experience, express and/or seek meaning, purpose, and transcendence and the way they connect to the moment, to self, to others, to nature, to the significant and/or the sacred.
The spiritual field is multidimensional, containing:
Existential questions (concerning, e.g. identity, meaning, suffering and death, guilt and shame, reconciliation and forgiveness, freedom and responsibility, hope and despair, love and joy)
Value based considerations and attitudes (i.e. the thing most important to each person, such as relationships to oneself, family, friends, work, nature, art and culture, ethics and morals, and life itself)
Religious considerations and foundations (faith, beliefs and practices, the relationship with God or the ultimate).
The definition of the EAPC Reference Group on Spiritual Care was chosen as an overarching definition because it presents a broad view on spirituality. 12
Search strategy and databases
The search strategy was based on the “Palliative cAre Literature rEview iTeraTive mEthod” (PALETTE). This is an iterative method for the development of search strategies in palliative care literature for complex concepts such as spiritual care. 28 An exploratory search was conducted in PubMed. The provisional search was adjusted several times following PALETTE methodology. 28 The final search string was developed further in PubMed, optimized, and manually adjusted for use in other databases. On the 13th of October 2021, the original search was carried out in five online databases: PubMed, CINAHL, Embase, PsycINFO, and Cochrane (see Supplemental File 1 for search terms). The search was updated from October 2021 to January 1, 2023 on April 30, 2023.
Inclusion and exclusion criteria
We included full-text English original empirical papers if they met the following criteria: they concerned pediatric palliative care; they concerned spirituality as experienced by parents; their findings fitted the EAPC definition of spirituality; they reported data from the parents’ perspective; and they were published between 1 January 2015 and 13th October 2021. The year 2015 was chosen as a starting point because the attention given to spirituality from the perspectives of children, their parents/families and healthcare professionals in pediatric palliative care, building on important international consensus definitions,12,16,20 is only been evident in recent years. The same is true of the development of guidelines.29,30
Duplicates were removed from the EndNote library using a method for de-duplication of database search results for systematic reviews in EndNote. 31 The title and abstract screening and the follow-up screening based on the full articles were performed by two researchers (ME, NJ) and four researchers (ME, NJ, MB, MK) respectively. They used the screening capabilities within EndNote X9. 32 Differences in the selection of articles which were potentially included were resolved in mutual consultation. When in doubt, an article was judged on its full text or in consultation with the research team.
Data extraction and analysis
We developed a data extraction table that included the author, year, country, aim setting, design, sample, number of participants, data collection, and quality appraisal.
To analyze the findings from studies with qualitative, quantitative and mixed-methods research designs, we took a convergent integrated approach to the synthesis and integration of these findings. 26 For the purpose of the synthesis, a conceptual overview of the results with regard to spirituality was made of each article and in this overview, statistical findings from included studies were transformed into descriptive summaries. This was performed by ME, MB, and NJ. An initial thematic structure was developed based on the overviews of the findings of articles published in 2020 and 2021 (found in the original search, n = 17) by ME and NJ with regular input from MB and MK for checking the themes found and their validation. Subsequently, all information from remaining articles, including articles from the updated search, was also analyzed thematically and placed along this preliminary structure. If necessary or desirable, themes were added or existing themes were merged. This resulted in a final structure of themes and subthemes reflecting the aspects of the spiritual dimension. During the later stages of analysis, the wider research team (also including CL and SCCMT) regularly validated the findings.
Quality assessment
The assessment of the quality of the articles included was performed independently by two researchers (ME, NJ). Observational studies were assessed using an adapted version of the Cochrane risk of bias instrument, which was based on the Cochrane Bias Tool for intervention studies 33 and was adapted for observational studies in cooperation with Cochrane Netherlands.34,35 For the quality assessment of qualitative articles, we used the CASP tool. 36 Articles with a slightly lower quality assessment were also included given the exploratory nature of this systematic review. 37
Results
Characteristics of the included studies
The final, updated search strategy resulted in 2527 unique articles covering the period from January 1, 2015, to January 1, 2023. Of these 63 were included meeting the criteria set out (see Figure 1).38–100
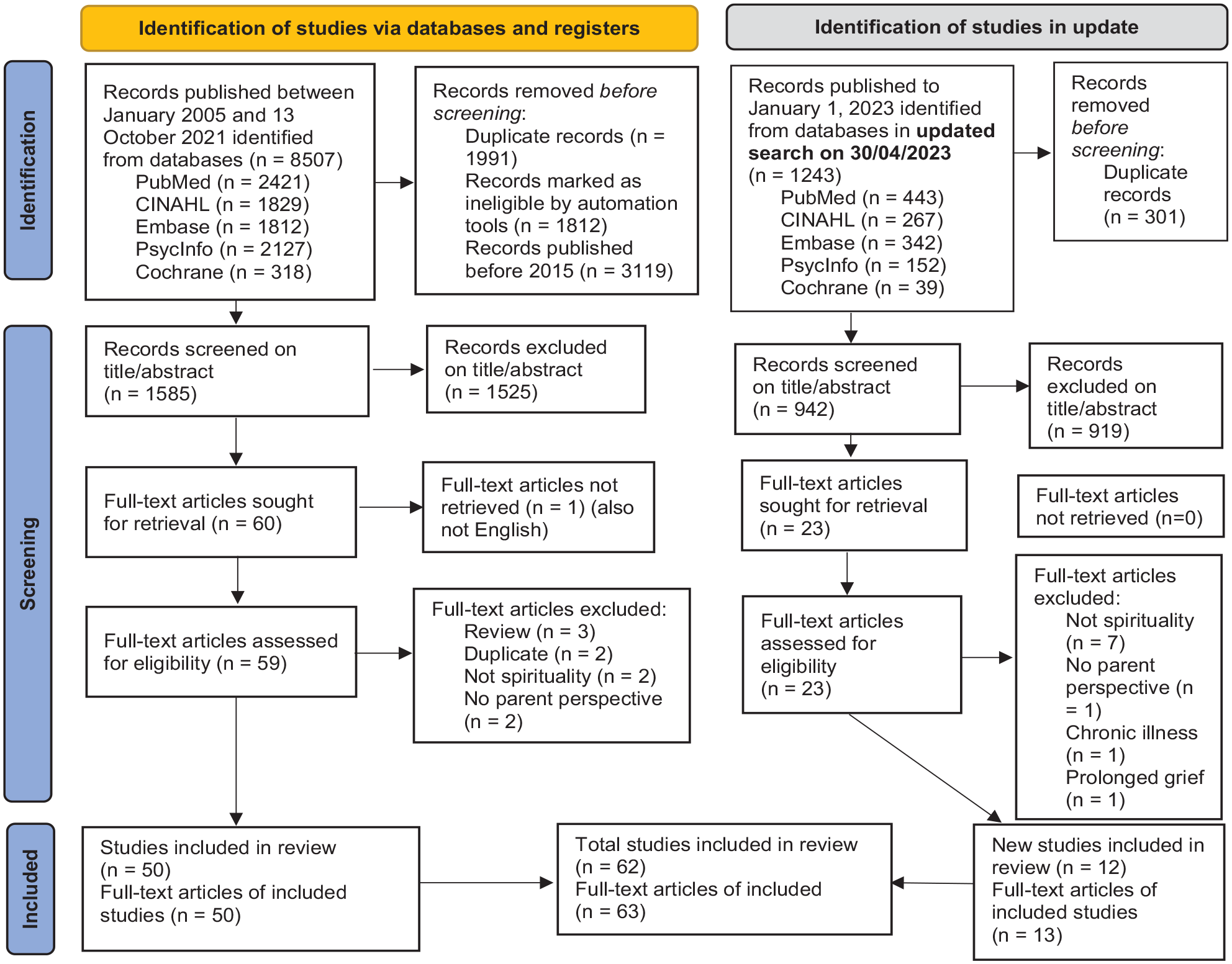
Flow diagram search strategy 27 (2021-10-13 and updated search to 2023-01-01).
The vast majority of articles are based on qualitative research (n = 47).38,39,41,42,44,46–52,54–59,61–63,65,66,68–70,72,74–78,80,82–84,86,88,90–97,99 Eleven articles report a quantitative observational study.40,43,45,53,67,71,73,85,87,89,98 Five articles present a mixed-methods design.60,64,79,81,100 Most stud-ies (n = 22) were conducted in North America.39,40,42–45,63,64,67,70–72,77–79,81,83,88,89,91,97,98 Nineteen studies were from Asia.38,41,46–49,58–60,69,73,74,76,82,86,87,94,96,99 Thirteen were from Europe.50,52,53,55,61,66,68,75,85,92,93,95,100 Six studies were from South America,54,57,62,80,84,90, three from Australia.51,56,65 In total, the studies report on the perspectives of 2355 parents. An overview of the characteristics of the included studies is presented in Table 1.
Characteristics of the included studies.

For this study, we focused on the perspectives of parents.
Quality appraisal
For qualitative studies (n = 47), and for qualitative components of mixed-methods studies (n = 5), the median quality score of the report was 8.5 out of 10 (range 4.5–10). For observational studies (n = 11), and the quantitative parts of mixed-methods studies (n = 5), the median quality score was 3.0 out of 7 (range 1–4). A detailed presentation of the quality assessments by the researchers is presented in Supplemental File 2, Tables A.2.1 to A.2.4.
The spiritual dimension of parents’ experiences in pediatric palliative care
Description of spirituality
There was a wide variation in the definitions of spirituality. In 49 articles spirituality was not specified. In the other 14 articles a wide variation in the definition or description of spirituality was found. In 10 articles two or more different aspects of the EAPC definition were given. In four articles spirituality was only described as religion. An overview of the characteristics of the descriptions of spirituality is presented in Supplemental File 3.
Aspects and how they manifest themselves in parents
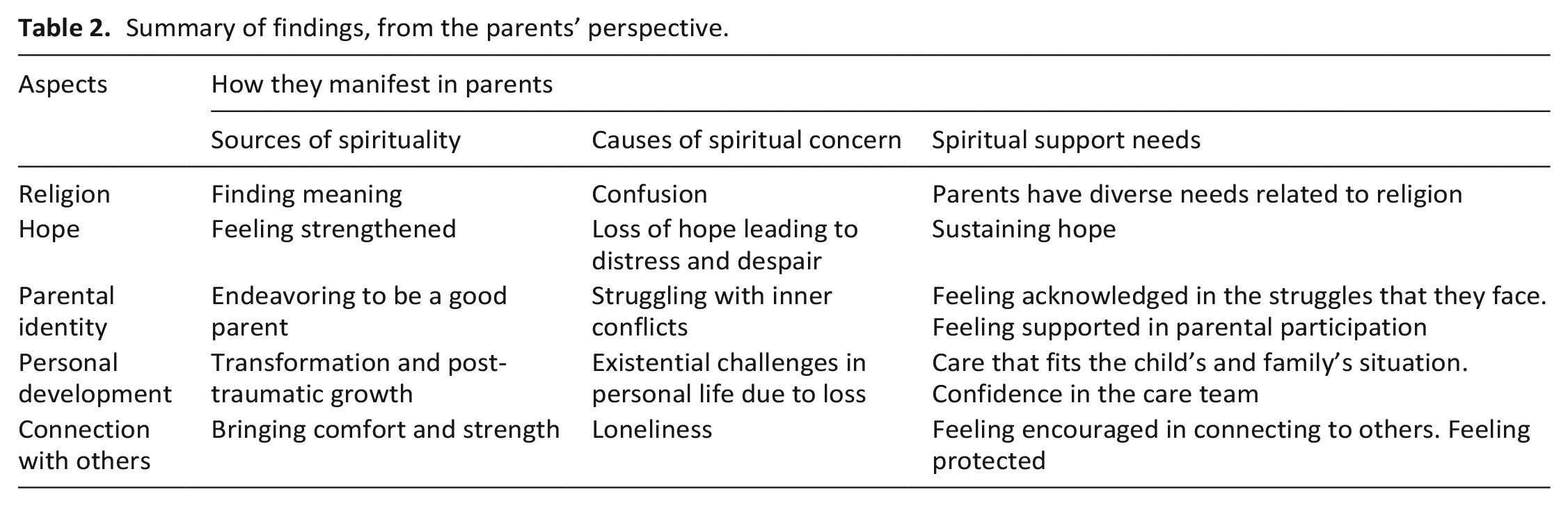
We identified, through thematic analysis, five aspects that are important to parents with regard to spirituality. These were: how they connect to their religious beliefs; how they deal with hope; their parental identity; their personal development; and how connected they feel to others. Sometimes parents mentioned these aspects as source of spirituality. It strengthened them in various ways, for example by helping them to find meaning in their difficult situation, to retain some hope and control, function as a cause of spiritual concern bringing confusion, inner conflicts, and, or frustration to parents. This could lead to feelings of senselessness, despair, and loneliness. Thematic analysis also revealed that parents often did not explicitly express their need for spiritual support or maybe researchers reported little about these needs. A summary of findings is presented in Table 2.
Summary of findings, from the parents’ perspective.
Religion
Religion as a source of spirituality
A large number of studies reported on religion as a source of spirituality. Parents mentioned ways in which their belief in God, or the ultimate helped them to deal with existential challenges and find meaning in their difficult situation. It helped them to make sense of the incomprehensible69,74,88and to believe that whatever happens, God knows what is best for them 62 or it offered comfort through the meaning of being part of a larger purpose.83,88 Religious belief could also help parents give meaning to their experiences and made them feel supported when coping with the reality of their child’s illness.41,44,46,61–63,69,74,76,78,82–86,88,89,93–96,99 Parents found meaning in their religion because they felt a sense of connection with God or the ultimate,38,41,44,46,61–63,69,74,76,78,82,83,85,86,88,89,93,95,96,99 felt suppor-ted,38,41,46,62,76,78,82,83,85,89,96,99 experienced guidance,69,74,88 or hope.44,46,62,63,69,74,82,83,86,93 The studies also included a variety of religions.38,40,41,45,49,58,61–63,71,73,74,78,83,94,96,99 In addition some parents with no previous religious belief reported still finding solace in religion and prayer in times of difficulty. 46
Religion could also help reconcile parents to their inability to protect their child from the serious prognosis. It helped them to accept their lack of control, 83 and to transform their grief over the prospect of losing their child to living life to the fullest with their child. 99
Finally, religion helped parents to give meaning to the death of their child.46,62,93 The belief in an afterlife or being reunited after death brought comfort.63,78,93,95 This was true even if the parents did not believe in an afterlife. 61 Some parents also believed that the illness of their child was a test of their faith. This helped them to remain strong.63,88
A cause of spiritual concern – confusion
Religion could also bring confusion, inner conflicts and, or frustration to parents.41,44,46,73,74,78,83 Some parents reported feeling a sense of divine, or spiritual, abandonment.48,83 They felt punished through the illness 78 and blamed God or the ultimate for the illness of their child. 78 Others reported inner conflicts between the information that they had been given by professionals and what they believed was the will of their God or the ultimate. 74 Uncertainty about the afterlife could cause great confusion and grief to parents. 46 Other parents wondered if they were being punished by their God or through the disease of their child.44,73,74 The psychological stress caused, for example, by not understanding why God created this problem for them, sometimes threatened parents’ connection with their religion41,46,78 or prophets or saints. 38 Some parents lost their faith as a result. 41 Finally, some parents reported that spiritual practices were too demanding during this time. 83
The need for spiritual support related to religion
Relatively few articles reported on the need for support with regard to religious beliefs despite being a major theme in the spiritual experience of parents.38,40,41,43,58,74,78,79,87,94 A North-American survey study among parents whose children had been admitted for more than 48 h to PICU at a tertiary academic medical center 40 showed that parents’ (n = 162, 82% Christian, 10% religious without category, 6% nonreligious and 2% other) wishes were mixed about whether their child’s physician should ask about their spiritual or religious beliefs. Parents views were divided equally between agreeing, disagreeing, and being unsure. A few recent studies reported on the needs of parents for facilities for spiritual practices including contact with a professional. Some parents indicated that during hospital admission of their child they need a prayer room, 87 the availability of a spiritual/religious person,43,79,87 or more time for praying. 94
Hope
Hope as a source of spirituality
Hope, derived from seeing the good, that is having good days or living longer than expected, strengthened parents. 75 It helped them to focus on the care of their child, and thus, to provide them the best quality of life. 80 Hope also helped parents maintain a combative spirit, 55 perceiving the illness of their child, against all knowledge, as temporary.55,61,75,91 Kamihara et al. 70 found that parents were able to balance hope with realistic and more distressing expectations regarding the prognosis and progression of the illness.
A cause of spiritual concern – loss of hope
Losing hope was a common feeling for some parents.44,91,93,99 It could lead to strong feelings of senselessness, anguish, sadness, fear, anger, and despair.54,65,80,88 Many parents indicated that accepting the child’s illness, while at the same time staying hopeful, could also be challenging.44,54,65,80,88,91,93,99 Some parents reported losing all feelings of hope after the diagnosis. They questioned why this was happening to their loved one.44,54
The need for spiritual support related to hope
Several parents highlighted their need for professionals to strengthen them by sustaining hope, 94 focusing on positive thoughts,75,91 taking things day by day, hoping for the best each day, and demonstrating positivity. 91
Parental identity
Endeavoring to be a good parent as a source of spirituality
Endeavoring to be a good parent was another source of spirituality that might strengthen parents and help them to find meaning in their experience. It presented parents with a destiny that is to care for their child.63,76,78,84,93,95,97,99 The endeavor to be a good parent manifested itself in several ways. Parents went to great lengths to provide the best care for their child. If cure was no longer an option, then they endeavored to grant their child a good and dignified death.73,75,76 Being acknowledged in this role, for example by being involved in decision-making processes, helped parents cope and gave them a sense of control.75,100
Being a good parent was also manifested in their efforts to strive for what they considered a good death for their child. Being able to let their child go helped parents to achieve this. 49 Taking care of their child’s legacy was another way for parents to find meaning.77,88 Parents also indicated that farewell-activities drew them, their child and others involved, closer together and helped them experience a good death.49,75,81,96,99
A cause of spiritual concern – struggling with inner conflicts
Most parents preferred to fully embrace their parental role by caring for the child themselves, 95 and when they experienced difficulties in doing so52,68 it caused feelings of distress and despair.52,54,69,72,86,88,90,93,96,98,99 With regard to treatment, parents reported inner conflicts between doing “too little” and doing “too much”,49,67,75,95 and frustration in case their expertise was questioned during hospital admission of the child 72 or their child was not addressed respectfully. 100 Lacking control made parents feel unprepared, scared, 46 and vulnerable. 68 Caring for their child may have reduced emotional and spiritual distress but parents often experienced it as a difficult and exhausting task. 95
Finally, parents reported inner conflicts related to what they considered important for their child. Providing care at home meant they had to navigate a lack of family privacy and control.49,50 Parents felt torn between wanting to stay physically close to their child and their other commitments, such as jobs or the interests of siblings and peers.49,50,72,97
The need for spiritual support related to parental identity
Parents expressed a wish for professionals to support them in their parental role. This could be achieved by acknowledging the struggles they face, 44 by emphasizing that they can still do a lot for their children and be good parents, 75 by providing meaningful information, acting as an advocate for their participation,39,50 and by sensitively introducing the possibility of legacy-building.43,77 Parents indicated that this helped them to feel more in control, to make the best decisions for their child,66,75,91 and not to feel disconnected from their child. 91
Personal development
Personal development as a source of spirituality
Several articles mentioned personal development as a source of spirituality.49,52,53,55,62,68,85,89 The illness was initially seen as a period of fear, chaos, and loneliness. 55 However, this phase could sometimes function as a welcomed liminal haven. 55 Parents mentioned elements of “restitution” in other words restoring things to their normal life, considering the illness, against better judgment, as temporary, 55 and an opportunity for personal growth.62,72 Several parents even experienced positive life changes as a result of post-traumatic growth.53,84,89 For some parents, their experiences led to a fundamental shift in their personal values, their approach to life, and their relationships with others62,68 or themselves. 62 Other parents coped with illness by framing the situation in a more positive way. 85 Being able to let their child go for some parents signified a turning point in the disease trajectory where they moved from doing everything possible to doing everything “right” in order to ultimately reduce suffering. 49 Parents also described achieving some meaning to their situation by giving something back, for example by doing voluntary work. 52
A cause of spiritual concern – existential challenges in personal life
Parents experienced an increasingly pronounced dislocation between two worlds from the moment they received their child’s diagnosis. There was the new world which revolved around the caring and other requirements of their child and their old world that did not.56,66,68,100 This brought existential challenges in their personal life. Parents put personal needs second, experiencing limited opportunities to continue their own life because of their child’s needs. 95 They had to constantly adapt to fulfill their parental duties.54,55,89,95 This meant they experienced losses in several ways51,52,56,80 such as the loss of normality.52,99 They also described feeling torn, guilty, and heartbroken, because they might not have lived up to the expectations they had set for themselves and their families.56,68,76,81,92,95
The need for spiritual support in relation to existential challenges
Several articles reported a need for structures that provided stability when facing existential challenges.39,49,50,66,78,85,95 Parents, for example, do not want to be left alone by the care team after receiving their child’s diagnosis. 66 They need confidence that the care team, whether specialized in palliative care39,44,80 or not,50,85 takes responsibility for supporting them in what they consider important.39,44,49,50,66,78,80,85 Parents, therefore, need adequate care that fits their child and family situation and they actively guide healthcare professionals to provide such care.49,95
Being connected to others
Being connected to others as a source of spirituality
Feeling connected to others was mentioned as a great source of spirituality. Parents were strengthened, especially, through the bond with their child.61,100 The connection that parents felt with their child, even in the absence of verbal communication, 61 helped parents to know that their child was still fighting, 61 or when the child decided “it was time to go”.61,95 After the death of their child, ordinary events could have a transcendent meaning for parents, signifying the ongoing feeling of connection with their child. 61 For example, through seeing a symbolic representation in birds or butterflies, or music from toys that spontaneously started playing without prompting it. 61
Support from family, friends, their faith community, and other parents with similar experiences, also brought parents comfort and strength.41,44,48,58,61,72,76,80,83,86,94 Parents spoke of stronger relationships, and a greater appreciation of people in their network, to the detriment of material values. 62
Parents’ connection with healthcare professionals enabled them to feel that the medical team was with them.76,85,100 This helped parents to feel tranquil and supported.57–59,76 Adequate communication by healthcare professionals was not simply a matter of professional responsibility, but was integral to the parents’ sense of themselves as effective in a world in which they had often lost previous competencies. 68
A cause of spiritual concern – loneliness
Despite the meaningful connections parents described, many parents also described feeling disconnected or lonely from the world around them. They felt that people around them did not understand the complexities of their lives.51,52,54,56,76,80,92 Parents missed activities that would allow them to connect with other families.51,52 In the period after the loss of their child, they struggled to redefine themselves in relation to the outside world. 60 Parents also described a certain distance from their child, because they felt their expertise was not sufficiently recognized by the healthcare professionals and their role as a caregiver was unclear. 91 Some parents reported that their marital relationships had become markedly strained72,92,94 because of a lack of social time together, or because they did not share the goals they had for their child.52,54,76,81,86
The suffering and loneliness experienced by parents challenged permanent bonds with the healthcare professionals as parents often changed their previous evaluations of these relationships. 55 Parents could feel abandoned by the professionals after their child died as professional support stopped and there was no further regular contact.57,60,92
The need for spiritual support in relation to connections with others
Many parents expressed the need to be encouraged to connect with others.42–44,46,52,68,72,80,90 Supportive relationships provided security and protective factors for parents’ bereavement.57,68 Connecting to other parents who went through similar struggles could be helpful for parents.44,47,81,94 Being connected to others also involved parents’ relationships with the care team. Parents expressed a need for a supportive, compassionate relationship with the care team, whether or not they were specialized in palliative care.39,47,56,66,94,98 They wanted to feel “held” and protected by care providers, even when these relationships were not clarified through verbal communication. One mother described how she felt nurses’ non-physical presence. The knowledge that they were around, even though the nurses respected her privacy by leaving her alone at times, helped her to feel secure. 57
Discussion
Main findings
This systematic review explored how the spiritual dimension, in articles that included findings that fit to the EAPC definition, becomes manifest in parents of children with life-limiting or life-threatening conditions. We found five aspects that are important to parents with regard to spirituality: religion, hope, parental identity, personal development, and the connection with others. All can both function as a source of spirituality and as cause of spiritual concern. Sources of spirituality, such as hope and endeavoring to be a good parent, help give parents strength and meaning to their experiences. The causes of spiritual concerns, such as loneliness and feeling disconnected, bring confusion, inner conflicts and, or frustration to parents. Several parents highlighted their need for professional spiritual support, for example, by helping them maintain hope or by encouraging them to connect with others.
What this study adds
A wide variation in the description of spirituality was found in the articles. These ranged from no description at all, to several definitions of the concept of spirituality. In all the descriptions of spirituality given, we identified one or more dimensions that are also found in the EAPC definition: existential questions, value based considerations and/or religious considerations and foundations. In several articles, one or more dimensions of spirituality were found in the description of the coping strategies of parents or in the psychological, emotional, or social aspects of care. This conceptual ambiguity has already been addressed both in several studies on adult care12,14,15 and in a few studies on parents’ experiences in pediatric palliative care.4,101,102 The broad view on spirituality contained in the overarching definition used by the EAPC Reference Group on Spiritual Care touches on many important aspects and refers to a continuous spiritual process in persons. 12 However, in our review, parents’ language in included studies often refers to specific elements of meaning-making that would give them strength or be a cause of spiritual concern as if spirituality is not a process that is always there. Haufe et al., 5 for example, mention religion as a source of spirituality that leads to the process of meaning-making. Spirituality in itself is not only positive, but also a process of struggle and often found in everyday things.5,19 We found, obviously driven by the research topics of the studies in question and the underlying views on the concept “spirituality”, that parents talk about the spiritual process in terms of sources that give them strength and causes of spiritual concern that bring confusion or frustration. Parents’ use of language can lead healthcare professionals to think causally about spirituality rather than about spirituality as a process. In future research, a clear definition of the concept of spirituality underlying a study would be helpful in bringing theory on spirituality and healthcare practice closer together.
We also found that parents’ needs for spiritual support were often not explicitly stated. It is, therefore, not surprising that healthcare professionals do not recognize these needs and, thus, may not respond to them. Our findings show that further elaboration of the way in which parents experience spirituality, in both less or more visible forms, and the way healthcare professionals can recognize and respond to the process parents are going through, will be helpful in being sensitive to the spiritual dimension and supporting parents more adequately and systematically in their spiritual process.
We have the impression that most parents were aware that, together with their child and relatives, they had to walk this road themselves. In the spiritual dimension, they asked, mainly, that healthcare professionals care, and show they care, about their child and family. This finding is in line with a literature review of parents’ experiences of palliative care in which it was found that, in their communication with healthcare professionals, parents wish to be respected as experts in the care of their child but also have the support they need recognized. 4 The need for good communication between parents and healthcare professionals is true for all four dimensions of pediatric palliative care, but certainly for the spiritual dimension. We hope the findings of our research will contribute to a deeper understanding of parents’ needs for spiritual support and the ways in which healthcare professionals can better recognize these needs and communicate properly with parents about them.
Strength and limitations of the study
A strength of our study is that we included articles from five continents finding commonalities and cultural differences between spiritual beliefs and practices. However, caution is advised regarding generalizability of our findings to other parts of the world than the Netherlands and Europe because of differences in views on spirituality. Some other limitations of this systematic review should be taken into account. The terminology used in this systematic review refers to the EAPC definition and thus to a broad approach to spirituality, but was not labeled as such in part of the included studies. In addition, the concept of spirituality in a young discipline like pediatric palliative care is often not sharply defined. 28 As a result, there is a gray area in the selection. We are not sure how to interpret this, because our selection approximates practice, where spirituality often is found in everyday life and everyday language. 5 However, it could also serve as a disadvantage to leave the inclusion of findings to the interpretation of the research team, even when was sought for agreement among the team members as was the case in this study.
Conclusions
Although studies vary in their definition of spirituality, the spiritual dimension in parents of children with life-limiting or life-threatening conditions becomes manifest in how parents connect to their faith, others, and themselves as parents. Healthcare professionals can support parents by being sensitive to the spiritual process parents are going through. The way in which healthcare professionals can provide spiritual care to the parents of a seriously ill child requires more research in the natural setting of clinical practice. Quantitative and qualitative research methods are needed to explore further the spiritual process of parents, how professionals can respond to this spiritual process in daily practice, in which situations expertise from healthcare professionals specialized in palliative care or spiritual and grief counselors is needed and in what way spiritual care in pediatric palliative care can best be organized in diverse care settings.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163231186173 – Supplemental material for The spiritual dimension of parenting a child with a life-limiting or life-threatening condition: A mixed-methods systematic review
Supplemental material, sj-docx-1-pmj-10.1177_02692163231186173 for The spiritual dimension of parenting a child with a life-limiting or life-threatening condition: A mixed-methods systematic review by Marijanne Engel, Marije A Brouwer, Nienke Jansen, Carlo Leget, Saskia CCM Teunissen and Marijke C Kars in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank Marie-Louise S. Goudeau, PhD, Information Specialist at Utrecht University Library, Utrecht, The Netherlands, for her assistance in the development of the search strategy.
Authorship
M.E. has contributed to the design of the work, collected the data, analyzed and interpreted the data, and drafted the manuscript. M.A.B., N.J. and M.C.K. contributed to the design of the work, analyzed and interpreted the data, and critically reviewed and revised the manuscript. C.L. and S.C.C.M.T. were involved in the study design and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Registration
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Netherlands Organization for Health Research and Development (ZonMw) (project number 10050011910008)
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.