
Abstract
Background:
Perinatal palliative care can offer compassionate support to families following diagnosis of a life-limiting illness, to enable them to make valued choices and the most of the time that they have with their newborn. However, home birth is usually only offered in low-risk pregnancies.
Case:
A couple who received an antenatal diagnosis of hypoplastic left heart syndrome and who had made a plan to provide palliative care to their baby after birth requested the option of a home birth.
Possible courses of action:
Recommend birth at hospital or explore the possibility of a home birth with perinatal palliative care support.
Formulation of a plan:
Multidisciplinary discussion and collaboration enabled a plan for home birth to be made which anticipated potential complications.
Outcome:
The baby was born at home and died on day 5 of life receiving outreach nursing, paediatric and palliative care support and buccal and oral opioids for symptom management. We include reflections from the family on the importance of this experience.
Lessons:
We provide a list of potential criteria for considering home birth in the setting of perinatal palliative care.
View:
Facilitating a home birth in the setting of perinatal palliative care is an option that can be hugely valued by families, but this service may be practically difficult to deliver in many contexts. Further research is needed to understand the preferences of women and families receiving perinatal palliative care.
Keywords
Facilitating choices for families, such as place of birth and place of death, is an important element of perinatal palliative care
The diagnosis of a serious condition in a fetus would usually preclude birth taking place outside of a hospital setting
Facilitating a home birth in the context of perinatal palliative care is possible in selected cases
Experiencing a home birth when a baby is expected to die can be hugely valuable for some families
Delivering this type of care safely requires adequate resources to allow for forward planning and coordination of care in the community
Further research is needed to understand the birthing preferences of women and families receiving perinatal palliative care across different global settings
Healthcare organisations may benefit from multidisciplinary discussions to assess the safety, acceptability and feasibility of providing home births alongside palliative care in their context
Background
Perinatal palliative care offers holistic support to babies and families when a potentially life-limiting diagnosis is made before or shortly after birth. 1 There is increasing research evidence to support the benefits of palliative care support throughout pregnancy, birth and the neonatal period for babies with life-limiting conditions and their families 2 but such services are absent or patchy in many countries and perinatal palliative care remains poorly described in global resource-constrained settings. 3
A key component of perinatal palliative care is to provide support from the antenatal period onwards and to facilitate important choices for families, including place of birth and death. 4 In high-resource countries (HRCs), where midwifery services are well-integrated into the health system model of care, giving birth at home is typically a choice (with between 1% and 16% of childbearing people choosing to give birth at home 5 ) whereas in low- and middle-resource countries (LMRCs), birth at home occurs much more frequently and may be associated with high mortality, although the number of facility-based births is increasing. 6 In the UK where healthcare is provided by the publicly-funded National Health Service and is free at the point of use, guidelines from the National Institute for Health and Care Excellence (NICE) 7 recommend that pregnant people at low risk of complications during labour are given a choice of birth settings including the option of a home birth. However, the diagnosis of a significant fetal abnormality would ordinarily prompt a recommendation for birth to take place at an obstetric unit.
Whilst the choice to pursue a home birth is generally less well supported in the United States, 8 we found one conference abstract reporting a home birth supported by a home hospice team in Chicago, USA. 9 We found no other published reports in the international literature of home births in the setting of perinatal palliative care.
Case
Thomas and Rachel were told at their 20-week anomaly scan that their daughter Lily was affected by hypoplastic left heart syndrome (HLHS), a severe form of congenital heart disease. Parents are routinely offered three options: three-staged reconstructive surgical technique, termination of the pregnancy or compassionate supportive therapy only. 10 All surgical options are non-curative or ‘palliative’ and carry significant risks of mortality and long-term morbidity. 11 Thomas and Rachel elected to continue their pregnancy with a plan to provide palliative care to their baby after birth. From early on in the pregnancy, Rachel expressed a desire for a home birth. She had a history of two previous vaginal deliveries without complications.
Possible courses of action
Recommend birth at hospital (either on labour ward or a midwife-led birthing unit)
Explore the possibility of a home birth with perinatal palliative care support
Formulation of a plan
Through a series of multidisciplinary discussions, plans were made to facilitate birth at home with support from the community midwives, consultant neonatologist and children’s palliative care team. Rachel and Thomas were fortunate to have access to two community midwives who were able to provide continuity of care throughout their pregnancy and delivery and, in addition, they chose to employ a private birth doula who worked closely with the midwifery team. Interprofessional discussions explored the views of all involved and potential for concerns about providing care in an unfamiliar setting. Peer review of the case was sought at a national professional forum for perinatal palliative care. An anticipatory symptom management plan was written to ensure that medications were available in advance of the birth. One practical challenge was that prescription and preparation of medications was not possible prior to birth since a unique medical record number was unable to be assigned.
Parallel plans explored parental wishes in the event of complications of home birth, need for transfer to hospital, difficulties with symptom management, short or longer survival and the possibility of changing parental wishes after birth.
Outcome
After spontaneous onset of labour at 40 weeks’ gestation, Lily was born at home with two community midwives in attendance who already knew the family well. She was assessed shortly after birth by a consultant paediatrician and at subsequent daily home visits by the neonatal and paediatric palliative care teams and community nursing. She established breast feeding and was initially asymptomatic apart from intermittent grunting and mild cyanosis. On day 3/4, Lily had developed increased work of breathing, and received oral morphine and buccal diamorphine with apparent effect. She appeared comfortable, though fed less frequently and had episodes of colour change. On day 5 in the evening, she had a long apnoea followed by gasping respiration. She received intermittent buccal diamorphine and died in her parents’ arms 2 hours later. Box 1 contains Rachel’s personal account of what a home birth meant to her.
Rachel’s account of what a home birth meant to her.

Thomas and Rachel’s older children aged 3 and 5 were present throughout labour and delivery and took an active role in caring for their younger sibling. During pregnancy Thomas and Rachel had spoken to the children about what to expect when their sister was born and used drawings and art activities with the children as a way of facilitating these conversations (Figure 1).
Lily’s story. Pictures drawn by Thomas for Lily’s siblings.
Lessons
Planned home birth is an important option for a significant number of women. In low-risk pregnancies, it is associated with fewer interventions during labour and for multiparous women there is no impact on perinatal outcomes. 12 However, compared with ‘low risk’ women planning home birth, ‘higher risk’ women who plan a home birth have a significantly increased risk of an adverse perinatal outcome. 13 The ‘risk’ of a pregnancy might arise from factors in either the fetus, in the mother or both.
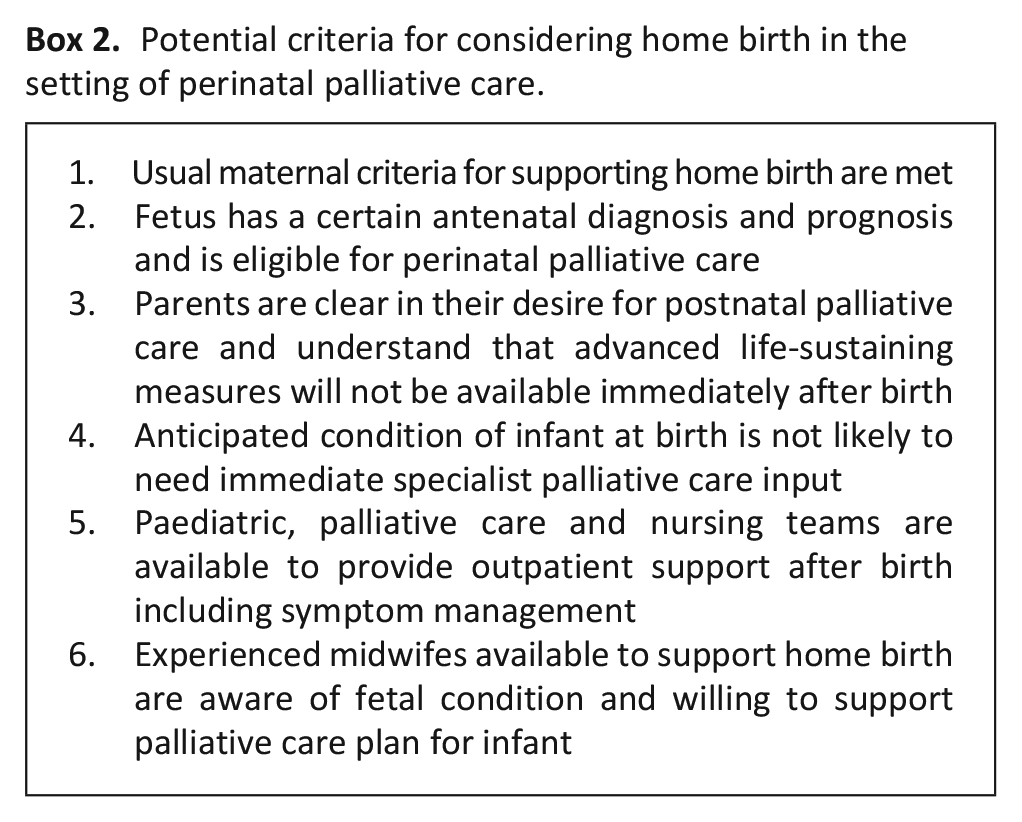
Home birth might be challenging in some cases of antenatally diagnosed severe fetal abnormalities – particularly where prognosis is uncertain, or where there is uncertainty about the appropriateness of palliative care.14,15 In a number of cases where perinatal palliative care is offered, parallel planning includes assessment of the infant’s condition at delivery and the option of some acute neonatal interventions. Delivery at home might make it difficult to provide these. In other cases, where an infant is anticipated to have early distressing symptoms (for example respiratory distress or pain), it may be challenging for midwives to support (since such neonatal symptom management is outside their usual scope of practice). In all cases where home birth is being considered, this is likely to require a significant amount of forward planning and access to the staff resources necessary to facilitate planning, coordination and delivery of this level of care. Good practice should include provision of a symptom management plan with the support of a specialist pharmacist with expertise in paediatric palliative care to facilitate both prescription and dispensing of medications at neonatal doses in the community setting. In Box 2, we list factors that would support the option of home birth. Additional facilitating factors in our case included the fact that parents had had a previous home birth, lived close to the hospital (and paediatric hospice) and the infant had a condition that is typically associated with normal (or near normal) neonatal condition initially after birth.
Potential criteria for considering home birth in the setting of perinatal palliative care.
View
Whilst an antenatal diagnosis of a life-limiting fetal condition brings immense pain, it also offers a unique opportunity to plan care in advance and to shape a baby’s arrival into the world in line with parental wishes and values. With staff shortages across maternity and neonatal care 16 there may be challenges in providing this level of care and appropriately supporting this option may not always be possible for other families in the same situation. Nonetheless, our experience and that of Lily’s parents, indicates that home birth with perinatal palliative care is possible and can be hugely valued by families. Given the growing role of children’s hospices in perinatal palliative care 17 future work could explore whether hospices themselves might be an alternative birth location for some families. Further research is warranted to understand the individualised birthing and postpartum preferences of women and families receiving perinatal palliative care and how these may vary between different countries. Social, cultural and resource considerations may mean that perinatal palliative care as it is currently conceptualised in HRCs may not be applicable to the needs of LMRCs 3 and so further research is needed to delineate the role of perinatal palliative care in contexts where home birth is either more or less common. Further research to explore the safety, acceptability and feasibility of providing palliative care in the setting of home birth is needed. Consideration should also be given as to what additional support may be required for the healthcare professionals who care for families in such circumstances. Finally, there is a need to evaluate the long-term impact on families of having a home birth with perinatal palliative care support.
Learning points for practice/research
Further research is needed to explore the birthing and postpartum preferences of women and families receiving perinatal palliative care and how these may differ in different global contexts
Individual healthcare organisations may benefit from multidisciplinary discussions involving obstetric, midwifery, neonatal, palliative care and hospice teams to assess whether home birth in the setting of perinatal palliative care is feasible in their context
Further research is warranted to evaluate the impact on healthcare staff of facilitating home births alongside perinatal palliative care
Footnotes
Author contributions
SB and DW were responsible for the concept and design of the work. SB and RK drafted the article. TK, EH, AC and DW revised it critically for important intellectual content. All authors approved the final version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in whole, or in part, by the Wellcome Trust (Grant numbers 224744/Z/21/Z, 203132/Z/16/Z); Arts and Humanities Research Council (AH/W005077/1). The funders had no role in the preparation of this manuscript or the decision to submit for publication. For the purpose of open access, the authors have applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission. All research at Great Ormond Street Hospital NHS Foundation Trust and UCL Great Ormond Street Institute of Child Health is made possible by the NIHR Great Ormond Street Hospital Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Ethical approval and consent to participate
Our institution does not require ethical approval for reporting individual cases or case series. Both parents are included as authors on this submission and have given written informed consent for publication.