
Abstract
Background:
Children with serious illness who receive hospice care often interface with nurses who lack training, experience and comfort in the provision of paediatric palliative and hospice care. Hospice nurse preferences for paediatric-specific training are not well known.
Aim:
To describe the types of paediatric-specific training received and educational content preferred by hospice nurses.
Design:
Population-level dissemination of a cross-sectional survey with qualitative analysis of open-ended survey items.
Setting/participants:
Nurses from 71 community-based hospice organizations across 3 states completed the survey.
Results:
An open-ended response was provided by 278/551 (50.5%) survey respondents. A total of 55 respondents provided 58 descriptions of prior paediatric-specific training, including a formal 2-day course (n = 36; 65.5%), on-the-job education (n = 13, 23.6%), online training (n = 5, 9.1%), nursing school (n = 2, 3.6%) and paediatric advanced life support courses (n = 2, 3.6%). A total of 67 respondents described 74 hospice-led educational efforts, largely comprised of a 2-day course (n = 39; 54.2%) or provision of written materials (n = 11; 15.3%). A total of 189 respondents described 258 preferences for paediatric-specific training, with nearly half (n = 93; 49.2%) requesting ‘any’ or ‘all’ types of education and the remainder requesting education around medication use (n = 48; 25.4%), symptom assessment/management (n = 32; 16.9%), pain assessment/management (n = 28; 14.8), communication (n = 29; 15.3%) and psychosocial assessment/management (n = 28; 14.8).
Conclusions:
Hospice nurses self-report inadequate exposure to educational resources and programs, in conjunction with a strong desire for increased paediatric-specific training. Identification of targetable gaps should inform the development of educational resources, policies and other supportive interventions to improve delivery of care to children and families in the community.
Keywords
Children with serious illness who access hospice resources and services often receive care from nurses who lack training, experience and comfort in provision of paediatric palliative and hospice care.
No prior studies have investigated the specific types of paediatric palliative and hospice care training received by hospice nurses, nor the educational content desired by hospice nurses who provide care to children and families in the community.
These data demonstrate that community-based hospice nurses often receive little to no paediatric palliative and hospice care training.
Available training opportunities primarily consist of the 2-day End-of-Life Nursing Education Consortium seminar, on-the-job education or online training.
Nurses express a strong desire for increased paediatric palliative and hospice care training and support, with nearly half of respondents requesting ‘any’ or ‘all’ types of paediatric palliative and hospice care education and the remainder requesting education around symptom assessment/management and medication use.
Hospice nurses self-report inadequate exposure to paediatric palliative and hospice care educational resources and programs, in conjunction with a strong desire for increased specific training with a focus on symptom assessment and management.
Identification of these targetable gaps should inform the development and investigation of educational resources, standardized operating procedures, policies and other supportive interventions to improve delivery of paediatric palliative and hospice care in the community.
Introduction
Within the United States, approximately 500,000 children suffer from life-limiting illness annually, and 50,000 children die each year.1,2 Many of these children and families are eligible for provision of community-based paediatric palliative and hospice care, as endorsed by the World Health Organization, Institute of Medicine and the American Academy of Paediatrics.3–6 In the context of paediatric serious illness, hospice organizations facilitate the provision of medical, psychosocial and spiritual care for children and families, with community-based resources and services delivered in the home setting or in a separate hospice facility.7,8 When provided by staff specifically trained in paediatric palliative and hospice care, hospice services are known to improve symptom burden and quality of life for children with serious illness,9–11 mitigate parental burden and psychosocial stress 10 and improve the experiences of healthcare providers as well. 9
Although more than three-quarters of nationally accredited hospice organizations in the United States report serving paediatric patients, very few hospices offer formal paediatric programs. 12 Specifically, data from the National Summary of Hospice Care demonstrate that only 14% of hospice programs offer formal paediatric services with specialized trained staff. 12 A 2018 population-based survey of nurses employed by hospices that offer services to paediatric patients revealed that the vast majority of nurses have no formal training in paediatric palliative and hospice care, and half of these nurses have no experience caring for paediatric patients. 13 Uniform standards for educational requirements for hospice nurses who provide care to children and families do not exist. Unsurprisingly, the vast majority of hospice nurses in this population study reported feeling somewhat or very uncomfortable providing services to children during the illness trajectory and at the end of life. 13
Despite these established deficits, no prior studies have investigated the specific types of paediatric palliative and hospice care training received by hospice nurses, nor the educational content desired by hospice nurses who provide care to children and families in the community. To address this gap in the literature, we conducted a targeted sub-analysis of open-ended survey items within a large cross-sectional survey study of hospice nurses employed by all accredited hospice organizations that offer services to paediatric patients across a tri-state region, with the ultimate goal of identifying gaps in training to inform the development of educational resources, standardized operating procedures, policies and other supportive interventions to improve delivery of paediatric palliative and hospice care in the community.
Methods
The authors’ Institutional Review Board reviewed and approved this study. The methodology of this investigative protocol has been previously described in detail. 13 Briefly, a population-based, cross-sectional survey was developed by an expert panel of paediatric palliative and hospice care clinicians and researchers through an iterative, rigorous process. The survey was pilot-tested to enhance face and content validity, and a total of 36 survey items assessed hospice nurse experience and comfort across the domains of symptom management, end-of-life care, goals of care, family-centred care and bereavement. Three items involved open-ended questions that allowed participants to free-text responses with regard to specific type(s) of paediatric palliative and hospice care training previously received, type(s) of training provided by the respondent’s employer and type(s) of training desired by the respondent. This article presents the findings from qualitative analysis of responses to these open-ended questions.
The survey was disseminated electronically to all nurses employed by accredited hospice organizations that offer services to paediatric patients across the tri-state region of Tennessee, Arkansas and Mississippi. Both adult and paediatric hospices and nurses were eligible to participate, as either could be asked to provide care to a paediatric patient within the purview of their organization. No participating hospices in the tri-state area functioned exclusively as stand-alone paediatric agencies. Liaisons at each participating hospice organization assisted with survey distribution between June 2017 and May 2018. A written explanation of study risks and benefits was provided on the first page of the survey; by opting to complete the study, participants provided their informed consent.
Responses to open-ended survey items were analysed by E.C.K., J.A. and M.G. using semantic content analysis. 14 Text transcripts were reviewed in depth to discover similarities and trends within each question; this process informed the development of an a priori coding schemata, which was applied across all free-text responses. Reconciliation processes were used to achieve consensus among coders. Codes ultimately were collapsed into five categories per survey item, as described in Table 1. Of note, respondent comments that encompassed diverse content satisfying criteria for more than one coding category were included, such that reporting percentages in some cases exceed 100%.
Coding categories derived from responses to free-text survey items.
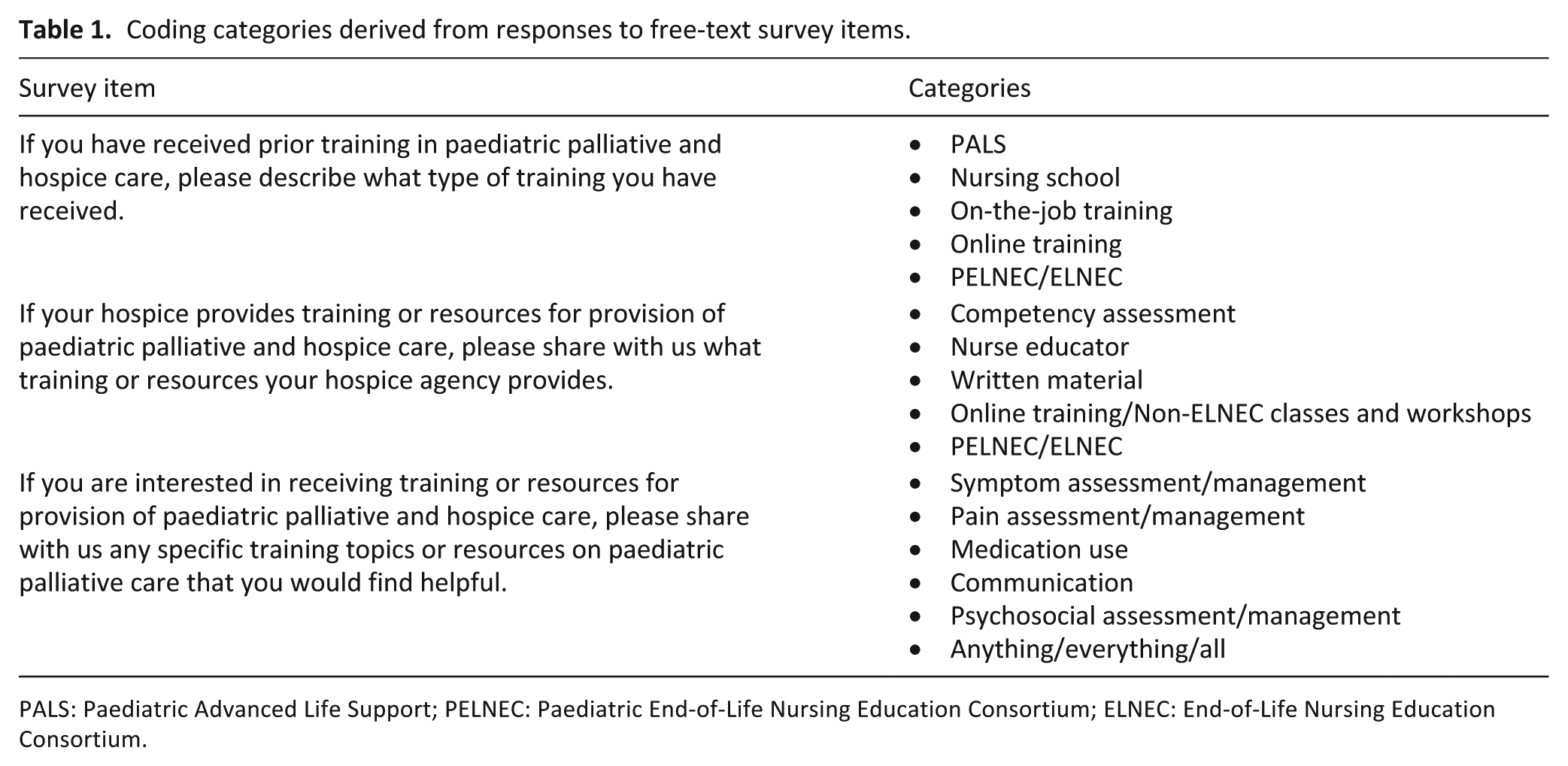
PALS: Paediatric Advanced Life Support; PELNEC: Paediatric End-of-Life Nursing Education Consortium; ELNEC: End-of-Life Nursing Education Consortium.
Results
A total of 91 accredited hospices were identified in Tennessee, Arkansas and Mississippi, which provide services to paediatric patients. Enrollment rates were high in hospices across all three states, with 91.7% (22/24) participation in Tennessee, 78.6% (22/28) in Arkansas and 69.2% (27/39) in Mississippi. Each hospice organization represented a ‘participating site’, through which care could be provided to paediatric patients in the home or (less frequently) in an inpatient facility. A total of 1366 nurses were eligible to receive the survey across 71 participating hospice sites, and a total of 551 surveys were completed for a response rate of 40.3%. Out of a total of 551 survey respondents, 278 participants completed at least one open-ended survey item (50.5%). Herein, we present the findings from a qualitative analysis of free-text responses to the open-ended questions.
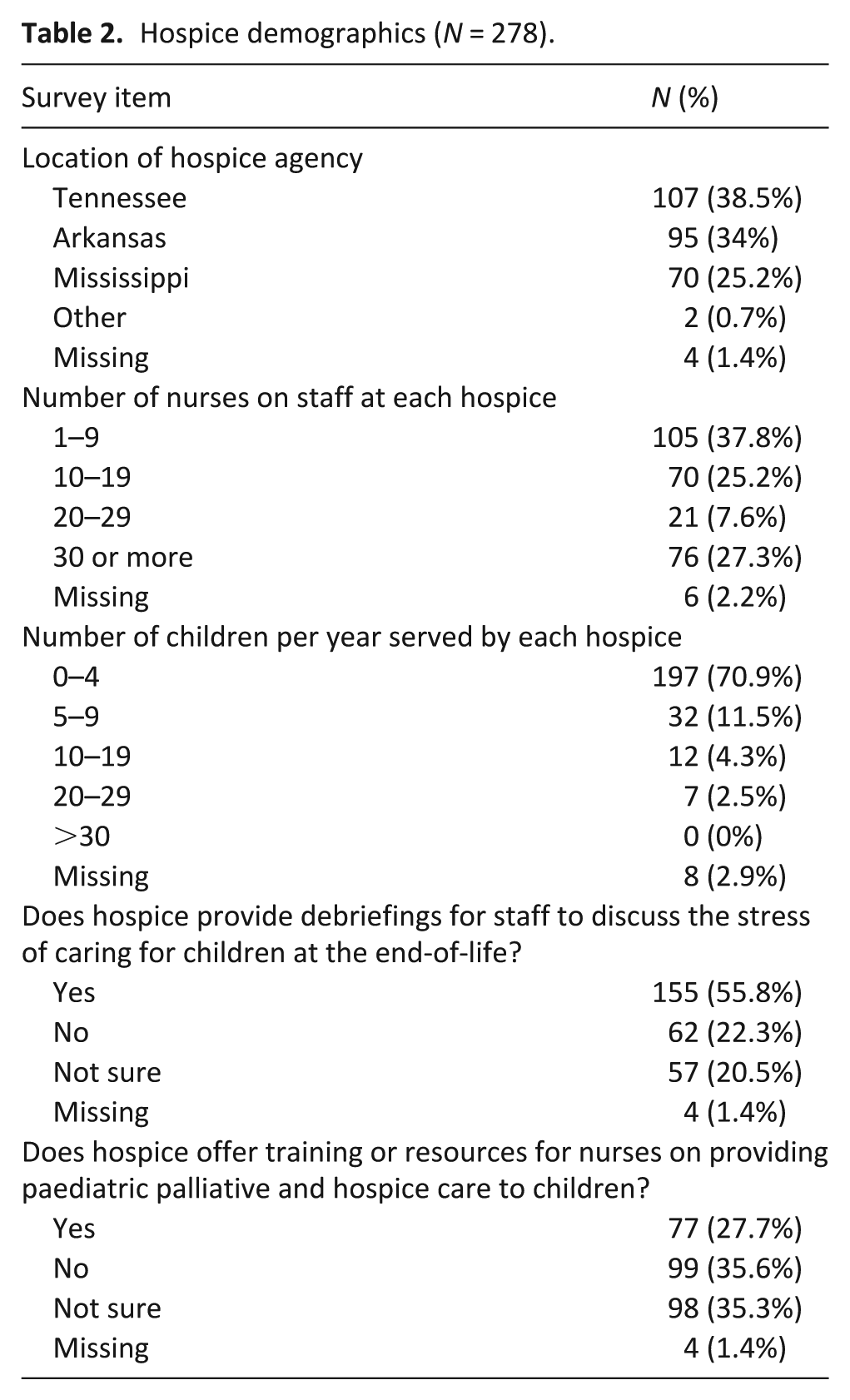
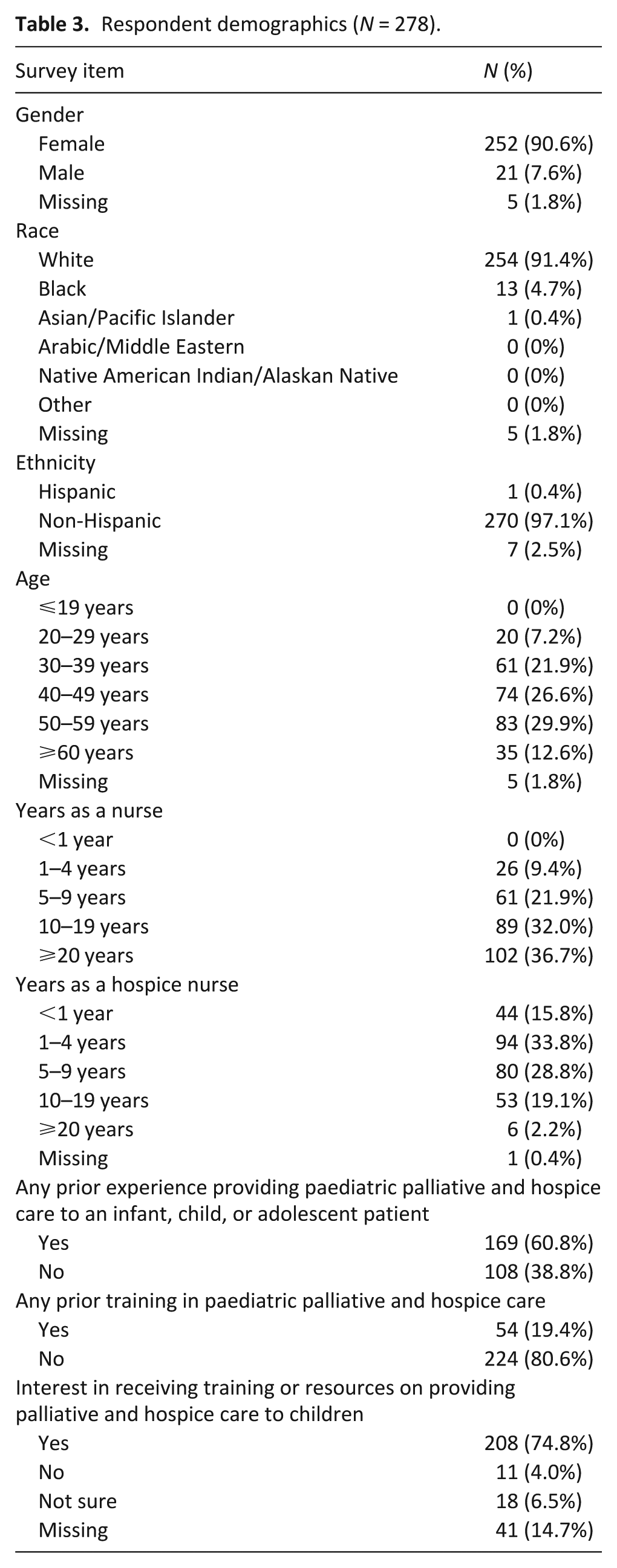
Hospice and participant demographics from the original cohort that completed the full quantitative survey have been previously published. 13 For the purposes of this targeted sub-analysis, hospice and individual respondent demographics from the sub-cohort that provided free-text responses are described in Tables 2 and 3. Nearly half of these 278 respondents (49.6%) had fewer than 5 years of experience working as a hospice nurse, and over one-third (38.8%) had no experience providing paediatric palliative and hospice care to an infant, child or adolescent patient. The majority reported that their agencies lacked formal training or resources on providing care to children (70.9%); those who reported a lack of training/resources available within their hospice organization also reported a desire for educational strategies to improve their comfort/competency in provision of care to children (74.8%).
Hospice demographics (N = 278).
Respondent demographics (N = 278).
Free-text item 1: If you have received prior training in paediatric palliative and hospice care, please describe what type of training you have received.
Out of the 54 participants in the original cohort who self-reported receipt of formal training in paediatric palliative and hospice care (9.8% of total respondents), 55 (all 54, plus 1 additional respondent) provided narrative responses when asked to describe the specific training they had received. Five categories were identified to describe these responses, with percentages of responses per category depicted in Figure 1. A total of 58 codes were applied due to participant provision of double responses (e.g. ‘I received PELNEC (Paediatric End-of-Life Nursing Education Consortium) training and we had training in my facility’.)
Free-text item 2: If your hospice provides training or resources for provision of paediatric palliative and hospice care, please share with us what training or resources your hospice agency provides.
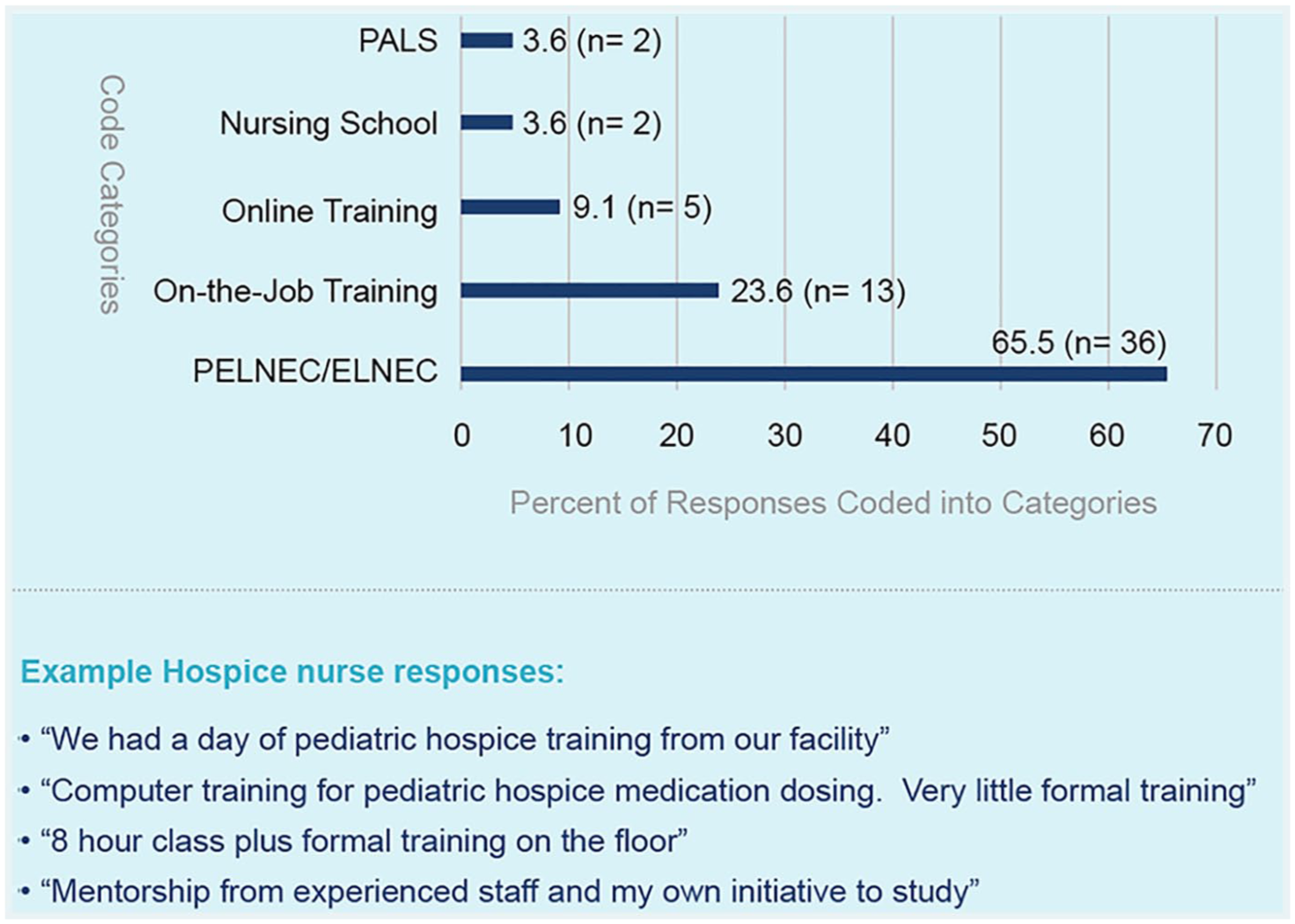
Hospice nurse self-report of prior training in paediatric palliative and hospice care.
Out of the 77 participants in the original cohort who self-reported that their hospice organization offered formal training or resources in paediatric palliative and hospice care (14.0% of total respondents), 67 participants (87.0%) provided narrative responses when asked to describe the specific training or resources offered. Five categories were identified to describe these responses, with percentages of responses per category depicted in Figure 2. A total of 74 codes were applied due to participant provision of double responses (e.g. ‘My facility provides PELNEC (Paediatric End-of-Life Nursing Education Consortium) training and written materials.’)
Free-text item 3: If you are interested in receiving training or resources for provision of paediatric palliative and hospice care, please share with us any specific training topics or resources on paediatric palliative and hospice care that you would find helpful.
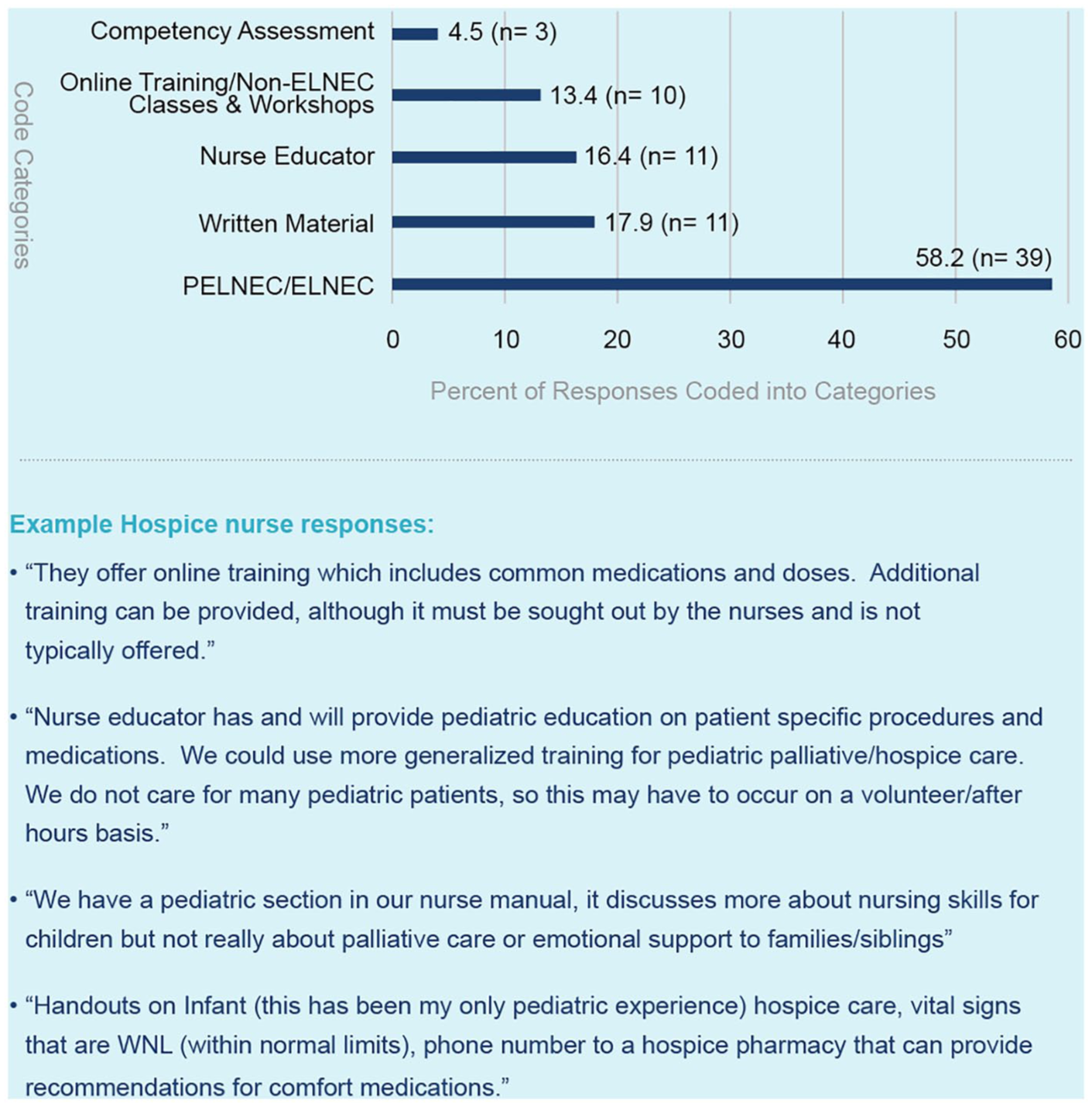
Hospice nurse self-report of training and resources related to paediatric palliative and hospice care offered by their hospice organization.
Out of the 276 participants in the original cohort who self-reported an interest in receiving formal paediatric palliative and hospice care training or resources (64.9% of total respondents), 189 (68.5%) provided narrative responses when asked to describe the specific training or resources they would prefer to receive. Six categories were identified to describe these responses, with percentages of responses per category depicted in Figure 3. A total of 258 codes were applied due to participant provision of double responses (e.g. ‘I would like training in communicating with patients and with dosing medications’.)
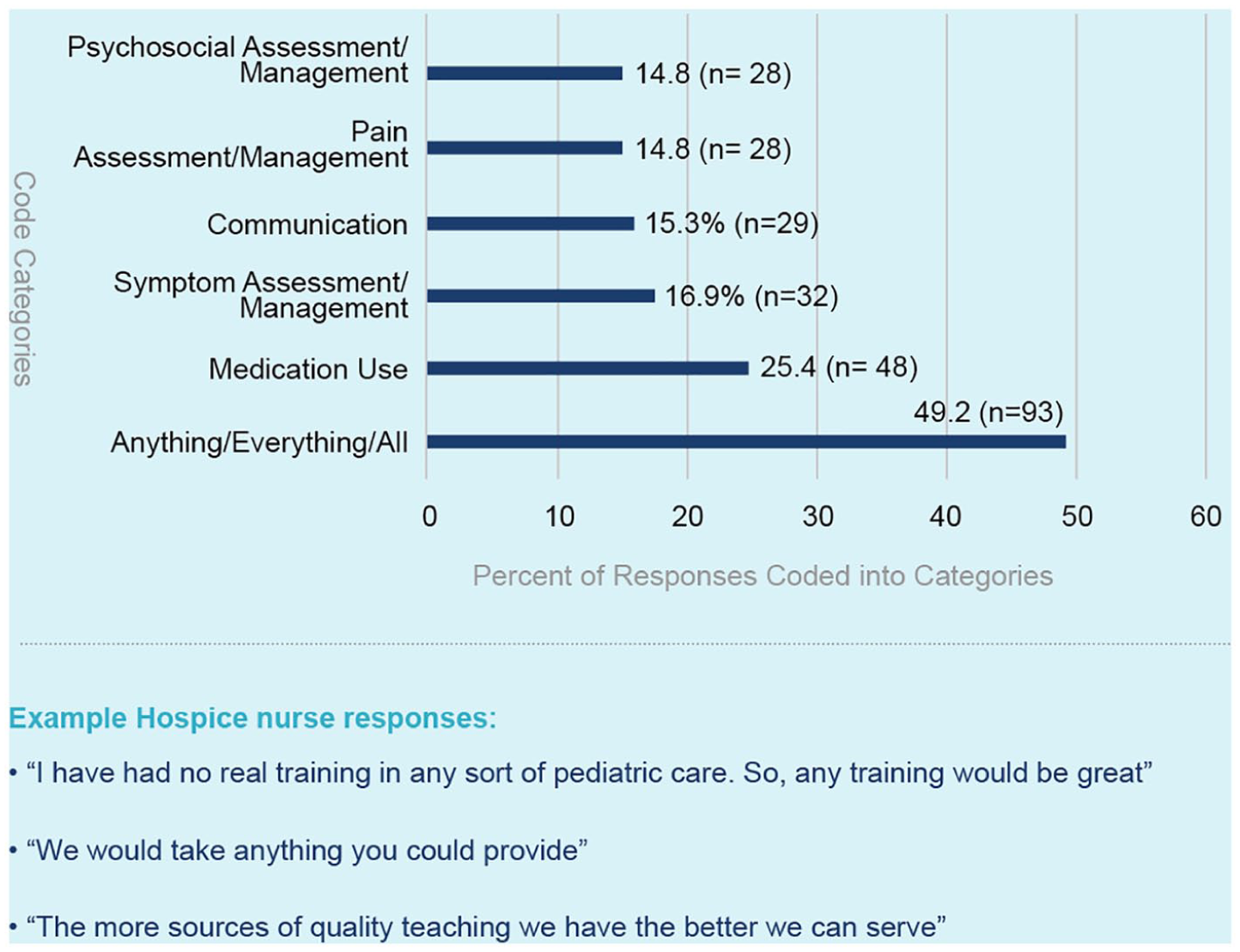
Hospice nurse preferences for training and resources related to paediatric palliative and hospice care.
To provide additional nuance and insight into the experiences and perspectives of hospice nurses who informed their responses, select quotes are presented beneath Figures 1–3 as examples to represent, clarify and enhance the meaning behind the coding categories.
Discussion
Main findings/results of the study
The findings from this qualitative analysis provide insights into hospice nurse experiences with and preferences for improvements in paediatric palliative and hospice care training. The vast majority of hospice nurse respondents from the original full study cohort reported no exposure to formal training in paediatric palliative and hospice care, 13 and approximately 10% who reported previous receipt of training described inadequate educational opportunities to support optimal provision of paediatric palliative and hospice care. Several respondents described the American Heart Association’s Paediatric Advanced Life Support (PALS) course as the primary source of their paediatric palliative and hospice care training; notably, this didactic course uses simulated paediatric emergencies to reinforce the application of a systematic approach to effective treatment algorithms to optimize resuscitation, 15 and it does not provide instruction or resources related to paediatric palliative and hospice care principles, concepts or evidence-based practice. Additional respondents described nursing school as their sole source of paediatric palliative and hospice care training. Per National Council of State Boards of Nursing, the majority of nursing schools do not include formal didactic or clinical exposure to paediatric palliative and hospice care in their training, 16 and nursing training programs that include paediatric palliative and hospice care in their curriculum typically offer a single didactic or brief clinical shadowing experience, which are likely insufficient to yield expertise or comfort with provision of paediatric palliative and hospice care to children and families in the community.
Importantly, nearly two-thirds of nurses who reported prior paediatric palliative and hospice care training in the quantitative survey and subsequently provided free-text responses to describe this training identified the End-of-Life Nursing Education Consortium seminar as the primary basis of their paediatric palliative and hospice care training. The Paediatric End-of-Life Nursing Education Consortium seminar is a standardized 2-day educational curriculum designed to enhance nursing comfort and experience with paediatric palliative and hospice care, which is widely utilized nationally and internationally. 17 Although 2 days of primarily didactic instruction are likely insufficient to ensure comprehensive training and ongoing support for hospice nurses, the Paediatric End-of-Life Nursing Education Consortium seminar offers a promising foundation upon which to build further paediatric palliative and hospice care education. In addition to participation in the Paediatric End-of-Life Nursing Education Consortium seminar, approximately one-quarter of respondents described exposure to additional online coursework (‘online self-training’ or ‘Computer training for paediatric hospice medication dosing. Very little formal training’). Approximately 10% of respondents described the receipt of on-the-job hospice training, although statements were typically vague: ‘We had a day of paediatric hospice training from our facility’. In general, these offerings suggest inadequate preparatory support to sustain high-quality provision of community-based paediatric palliative and hospice care.
Notably, less than one-quarter of participants from the original cohort affirmed that their hospice agency provided training or resources related to paediatric palliative and hospice care. 13 Within this subgroup, more than half of respondents described the End-of-Life Nursing Education Consortium seminar as the source of their hospice-directed education in paediatric palliative and hospice care. The next most frequent component of hospice-led training included access to written materials, such as books, booklets, policies and procedures. One participant wrote, ‘Handouts on Infant (this has been my only paediatric experience) hospice care, vital signs that are WNL [normal], phone number to a hospice pharmacy that can provide recommendations for comfort medications’. Many free-text responses included a caveat that materials were available for staff who sought them out but were not part of mandatory training and often lacked paediatric palliative and hospice care-specific content. One nurse wrote, ‘We have a paediatric section in our nurse manual, it discusses more about nursing skills for children but not really about palliative care or emotional support to families/siblings’. Opportunities for online training and coursework not related to the End-of-Life Nursing Education Consortium seminar were also described, including ‘On line training materials and meetings’ and ‘Class offered by a 3rd party’. However, responses often highlighted the fact that accessibility of paediatric-specific resources alone did not comprise adequate paediatric palliative and hospice care training.
Nurses also identified nursing competency assessments and education from a hospice nurse educator or peer as sources of hospice-led training in paediatric palliative and hospice care. Regarding the former, nursing competency assessments typically involve observed practice to ensure maintenance clinical skills (‘Annual competency includes paediatric assessment tools, med administration education’); however, the responses did not clarify how competencies were used to provide paediatric palliative and hospice care support and educational opportunities. Regarding the latter, respondents described receiving guidance from ‘Peer to peer interactions’, ‘A nurse practitioner available for resource’ or ‘A nurse who specializes in children and has trained a few other nurses to do the same’. ‘Nurse educators’ were also identified as resources to provide paediatric palliative and hospice care education for specific medication administration or procedures. These learning opportunities reflected a type of apprenticeship model, without mention of formal training modalities or educational infrastructure.
When asked about their interest in receiving paediatric palliative and hospice care training or resources, the vast majority of nurses who completed the quantitative survey were receptive to further education. 13 Nearly half of the 189 nurses who provided free-text responses stated that they would be interested in receiving ‘anything’, ‘everything’ or ‘all’ types of training or resources related to paediatric palliative and hospice care. Example responses included the following: ‘I have had no real training in any sort of paediatric care. So, any training would be great’ and ‘We would take anything you could provide’. This finding highlights the deficit in available training and resources as well as the robust desire and openness expressed by many hospice nurses for increased exposure to paediatric palliative and hospice care educational opportunities.
The remainder of requests for paediatric palliative and hospice care–specific content involved training to increase knowledge across 5 distinct categories: medication use, symptom assessment/management, pain assessment/management, communication and psychosocial assessment/management. The emphasis on pharmacotherapy in conjunction with pain and non-pain symptom assessment and management is unsurprising, particularly given recent findings demonstrating that three-quarters or more of hospice nurses within this tri-state region have little to no experience with assessing pain or non-pain symptoms or administering medications for management of pain or non-pain symptoms in the context of paediatric patients. 13 Likewise, prior analyses have revealed that significant numbers of hospice nurses in this region lack experience and comfort with navigating communication and providing psychosocial support to children with serious illness and their families. 13 These findings are not necessarily region-specific; hospice agencies in other parts of the country have described similar desire for education and support with a focus on similar topics in the context of providing care for paediatric patients and families. 18
Strengths and weaknesses/limitations of the study
Reports from the Institute of Medicine and National Hospice and Palliative Care Organization demonstrate that children with serious illness who access hospice resources and services often receive care from nurses who lack training, experience and comfort in provision of paediatric palliative and hospice care,12,13,19 and several recent studies, reviews and perspective pieces corroborate these concerns.13,18,20 This is the first study to directly ask community-based hospice nurses about their prior and ongoing access to paediatric palliative and hospice care training and their preferences regarding future educational opportunities. The cross-sectional survey design captured the voices of hundreds of community-based hospice nurses across a large region, with open-ended questions geared towards identifying gaps in training to inform the development of educational resources, standardized operating procedures, policies and other supportive interventions to improve delivery of paediatric palliative and hospice care in the community.
This study has several limitations. First, it represents the experience of a specific region and is not inherently generalizable across all areas of the country or worldwide. However, we believe that these data present a compelling argument for the need for further investigation of hospice nurse experiences and preferences for paediatric-specific training across the nation and globally. Second, although high levels of hospice participation were achieved, we cannot know the impact of missing data from non-participating sites. Third, the overall nurse-specific response rate was just above 40%, with more than 50% of participants providing text responses for the purposes of this sub-analysis; it is possible that the experiences of non-responders might have yielded different (or richer) findings. However, substantial efforts were made to achieve this level of community-based nurse participation across three states, and we believe that higher response rates would be challenging to obtain within this targeted population. Despite these limitations, we believe that a survey representing the perspectives and preferences of hundreds of hospice nurses offers a valuable addition to the literature.
What this study adds
Over the past several decades, data suggest that increasing numbers of children who die from complex chronic illness are returning home for the end of life,21,22 yet fewer than 20% of hospice programs offer formal paediatric palliative and hospice care services with specialized and trained staff, 12 and nearly one-third of existing hospices in the surveyed region have policies in place prohibiting provision of care to paediatric patients. 13 In 2003, the Institute of Medicine report ‘When Children Die’ noted that children who die at home frequently rely on professionals and providers with limited paediatric experience, resulting in suboptimal quality of care. 19 More than a decade later, the National Hospice and Palliative Care Organization’s report revealed negligible advancements, demonstrating that children referred to home-based paediatric palliative and hospice care continue to receive care from adult hospice programs with little to no experience with provision of care to paediatric patients. 12
Recent population-level survey data suggest that the majority of nurses employed by hospices that offer services to paediatric patients in the mid-South have fewer than 5 years of hospice experience, have never received formal training in paediatric palliative and hospice care, have no personal experience providing paediatric palliative and hospice care to children or families and feel somewhat or very uncomfortable providing paediatric palliative and hospice care to children. 13 Although the literature on this topic remains limited, several papers corroborate the need for improvement in paediatric palliative and hospice care educational and supportive resources for community-based hospice nurses.18,20
The findings from this study provide concrete, targetable content-based goals for the delivery of educational services to hospice nurses in the community. We advocate for the development of regional infrastructure and educational programs to support community-based hospice agencies in the provision of care to paediatric patients. Both the National Hospice and Palliative Care Organization and the Center to Advance Palliative Care have investigated strategies to facilitate such programs, with subsequent endorsement of collaborations between hospitals and community-based hospices to promote mutually beneficial interdisciplinary partnerships.18,23
One such collaboration, the Partners in Paediatric Palliative Care program, focuses on promoting relationship-building and teamwork between a hospital-based paediatric palliative care team and a network of community-based hospice/home care agencies across 5 states. 18 The Partners in Paediatric Palliative Care program enables real-time medical support, provision of paediatric-specific educational and networking opportunities, and bidirectional information sharing and feedback on ways to improve the parternship. 18 Through the Partners in Paediatric Palliative Care model, community-based hospice programs that previously enrolled adult patients exclusively have expanded their services to paediatric patients, with lack of experience and/or comfort levels mitigated by access to paediatric-specific resources and experts available 24/7 to provide anticipatory guidance and respond to hospice staff questions and concerns. 18
In addition to encouraging the creation of hospital–hospice collaborative networks, we also advocate for the development of a central repository of educational materials, curricula, standard operating procedures and quality improvement metrics specifically designed to support community-based interdisciplinary paediatric palliative and hospice care clinicians. This repository could provide the requisite building blocks to encourage hospital-based programs to develop collaborative partnerships with networks of local hospice agencies in their surrounding communities, as well as empower local hospices with the tools needed to connect with paediatric palliative care experts via telemedicine to provide additional support. Educational curricula targeting hospice nurses’ self-described gaps in experience/comfort could be freely available for hospital-based and hospice programs to modify and use according to their specific needs. Resources also could be provided to assist hospital–hospice partnership programs with development of advocacy and policy programming to address the most salient and/or topical paediatric palliative care issues specific to each region. We advocate for further studies to investigate the feasibility, acceptability and impact of models that promote collaborative partnerships between hospitals and community-based hospices.
Conclusion
Children with serious illness enrolled on hospice often receive care from nurses who lack training, experience and comfort in provision of paediatric palliative and hospice care. 13 Hospice nurses self-report inadequate exposure to educational resources and programs in conjunction with a profound desire for increased paediatric palliative and hospice care–specific training with a focus on symptom assessment and management. The identification of targetable gaps in hospice nurse training should inform the development and investigation of educational resources, standardized operating procedures, policies and other supportive interventions to improve provision of paediatric palliative and hospice care by nurses within the community.
Footnotes
Acknowledgements
The authors wish to acknowledge the St. Jude Biomedical Communications team for their assistance with editing the figures. The authors also wish to share our deep appreciation to the families who inspired us to pursue this study during the ‘Comprehensive Cancer Care for Children and Their Families’ conference hosted by the Institute of Medicine and the American Cancer Society in March 2015.
Author contributions
Erica C Kaye contributed to conceptualization, methodology, data curation, formal analysis, investigation, project administration, supervision, validation, visualization, writing – original draft and writing – review and editing. Jacob Applegarth contributed to methodology, data curation, formal analysis, investigation, writing – original draft and writing – review and editing. Melanie Gattas contributed to data curation, investigation, project administration, supervision and writing – review and editing. Ashley Kiefer contributed to methodology, investigation and writing – review and editing. Jason Reynolds contributed to methodology, investigation and writing – review and editing. Kristina Zalud contributed to methodology, investigation and writing – review and editing. Justin Baker contributed to conceptualization, funding acquisition, methodology, project administration, resources, supervision and writing – review and editing. All authors affirm that they (1) made a substantial contribution to the concept or design of the work or acquisition, analysis, or interpretation of data; (2) drafted the article or revised it critically for important intellectual content; (3) approved the version to be published; and (4) have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Data management and sharing
Please contact Erica C. Kaye for access to original, de-identified data files.
Erica C. Kaye, MD, MPH St. Jude Children’s Research Hospital
262 Danny Thomas Place
Mail Stop 260
Memphis, TN 38105
Email:
Phone: 901-595-8188.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was sponsored in part by ALSAC, as well as by the Paediatric Oncology Education (POE) program at St. Jude Children’s Research Hospital under the auspices of a R25 CA023944 grant. There are no other funding sources relevant to this article.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Research ethics and patient consent
The authors’ Institutional Review Board reviewed and approved this study (XMP17-111 (Pro00007699), approved 6/6/2017).