
Abstract
Background:
Nurse-patient relationships are an integral component of person-centred palliative care. Greater understanding of how nurse-patient relationships are fostered and perceived by patients and nurses can be used to inform nursing practice.
Aim:
To systematically identify and synthesise how nurse-patient relationships are fostered in specialist inpatient palliative care settings, and how nurse-patient relationships were perceived by patients and nurses.
Design:
Integrative review with narrative synthesis. The review protocol was registered with PROSPERO (CRD42022336148, updated April, 2023).
Data Sources:
Five electronic databases (PubMed, CINAHL Complete, Medline, Web of Science and PsycINFO) were searched for articles published from their inception to December 2023. Studies were included if they (i) examined nurse and/or patient perspectives and experiences of nurse-patient relationships in specialist inpatient palliative care, (ii) were published in English in a (iii) peer-reviewed journal. The Mixed Methods Appraisal Tool was used to evaluate study quality. Data were synthesised using narrative synthesis.
Results:
Thirty-four papers from 31 studies were included in this review. Studies were mostly qualitative and were of high methodological quality. Four themes were identified: (a) creating connections; (b) fostering meaningful patient engagement; (c) negotiating choices and (d) building trust.
Conclusions:
Nurses and patients are invested in the nurse-patient relationship, benefitting when it is positive, therapeutic and both parties are valued partners in the care. Key elements of fostering the nurse-patient relationship in palliative care were revealed, however, the dominance of the nurses’ perspectives signifies that the nature and impact of these relationships may not be well understood.
The nurse-patient relationship is considered the foundation of palliative care nursing.
Nurse-patient relationships are founded on trust, empathy, authenticity, genuineness and intentionality.
Person-centred care requires palliative care nurses to form interpersonal relationships that elicit patients’ true wishes and recognise and respond to both their needs and emotional concerns.
The nurse-patient relationship is contingent on the patients’ trust of the nurses’ authenticity.
Nurses are not aware that their verbal and non-verbal communication do not always align creating apprehension in patients.
The need for further research from the patient perspective on the authentic behaviours that foster the nurse-patient relationship is warranted.
A greater emphasis on strategies or models to promote positive nurse-patient relationships in palliative care are needed.
Identification of the various components or phases of the nurse-patient interaction that develop positive relationships perceived by the patient are necessary for optimal, ethical and culturally respectful health outcomes.
Actions to aid in understanding each person’s unique needs are key to person-centred care.
Introduction
Nurse-patient relationships are a core feature of person-centred care in nursing. 1 Nurse-patient relationships have been conceptualised as a key element of holistic care, together with physical and psychosocial dimensions, intrinsically related to the discipline of nursing.2,3 Despite many attempts to define the nurse-patient relationship there is no one universally accepted and used definition. 4 Guiding principles include that the nurse-patient relationship influences care incorporating the person’s perspective; 5 it is holistic, compassionate, mutually beneficial to nurses, individuals and families;6,7 and understood to be safe and respectful. 8 The nurse-patient relationship has also been referred as relationship-centred care, 9 a caring relationship, 6 patient-centred care, 3 and person-centred care. 4
The philosophy of person-centred care is described as basic, human kindness and respectful behaviour, 4 where care is impacted by the very nature and quality of that relationship. 10 Critical to the success of the nurse-patient relationship is an awareness and sensitivity to the patient’s preferences, their responses and reactions, 11 ensuring respectful and tailored care,6,12 that is therapeutic.13,14 Patients from across all healthcare settings report valuing personalised treatment and positive interpersonal communication. 14 Patients report placing great significance on being treated with care, respect and dignity, and nurses connecting with each patient through simple acts of kindness. 15 Patients value being seen as a person, who is deserving of being treated respectfully with authentic compassion, 16 with equal merit, 17 and being included in decision-making.18,19 Several issues exist on how the nurse-patient relationship is measured stemming primarily from a lack of conceptual and theoretical clarity around what constitutes the nurse–patient relationship. 20 First and foremost is the context in which the nurse-patient relationship is developed or exists, which constitutes the context of care. The Fundamentals of Care Framework has been promoted as key to explaining and guiding person-centred care, emphasising the importance of developing trust with the patient, anticipating patient needs and knowing enough about the patient to respond appropriately. 3 The context of care as described in the framework is expressed in terms of policy and system level factors more readily applied to inpatient settings. 3 Whilst the lack of specificity around the context of care has been recognised as a limitation to the framework, 12 the framework does emphasise the importance of the nurse-patient relationship as part of person-centred care in inpatient settings.
It is posited that identifying the ways in which nurses can develop relationships with patients when they encounter a range of challenges might be more useful. 20 While there is significant rhetoric about the value of the nurse-patient relationship in person-centred care, 4 how nurses foster a positive and therapeutic relationship is less clear. 11 Rather, a person-centred approach to care that focuses on authentic shared decision-making and empowerment form the base on which the nurse-patient relationships develops.21,22 Evidence about nurse-patient relationships in palliative care from the patient’s perspective are comparatively limited. 3 A previous review which explicated researcher concerns that asking patients with a life-limiting illness to participate in research was too burdensome, or even unethical 23 may partially account for this. Thus, building a comprehensive understanding requires that patient and nurse perspectives are examined together. Therefore, the aim of this integrative review was to identify and synthesise the research evidence on how nurse-patient relationships (i) are fostered in inpatient specialist palliative and hospice care services and settings and (ii) perceived from the nurse and patient perspectives.
Methods
Design
This integrative review was undertaken to answer the research question, using an approach similar to the preliminary stages of (i) problem identification, (ii) literature search and (iii) data evaluation described by Whittemore and Knafl. 24 Reporting of this review was guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses: The PRISMA Statement. 25 The integrative review protocol was registered prospectively with Prospero #CRD42022336148, and updated in April 2023.
Search strategy
A comprehensive search of five electronic databases was initially conducted in June 2022 and updated in December 2023. Databases searched were CINAHL Complete, PsycINFO, MEDLINE (via OVID), PubMed and Web of Science, guided by the inclusion and exclusion criteria (Table 1).
Inclusion and exclusion criteria.
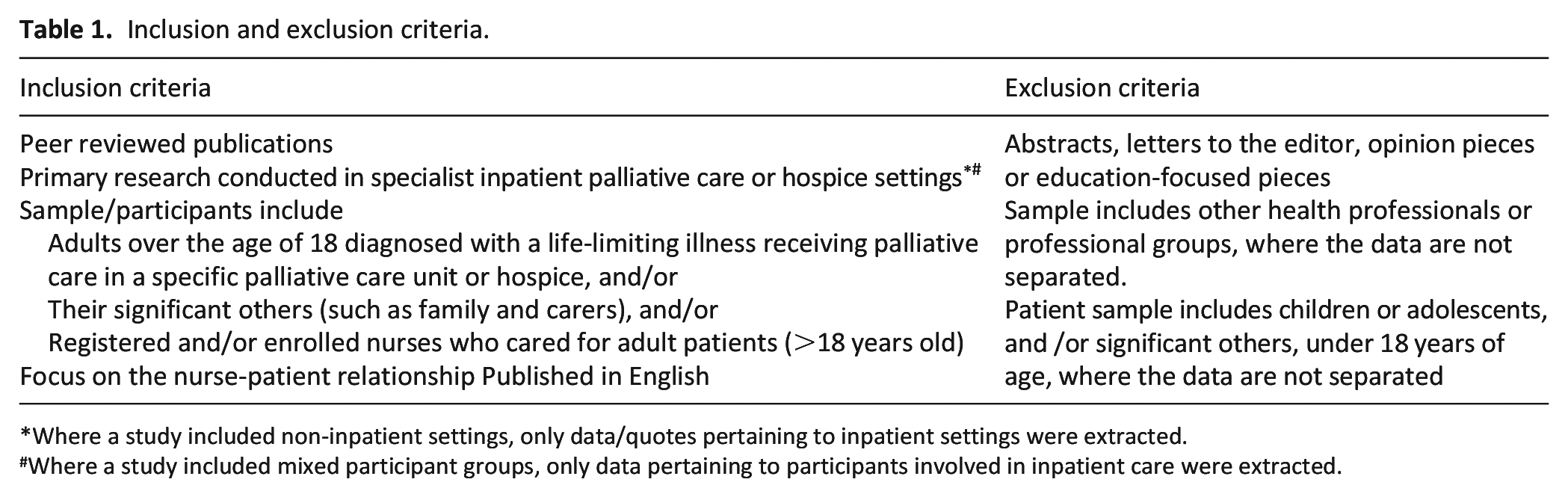
Where a study included non-inpatient settings, only data/quotes pertaining to inpatient settings were extracted.
Where a study included mixed participant groups, only data pertaining to participants involved in inpatient care were extracted.
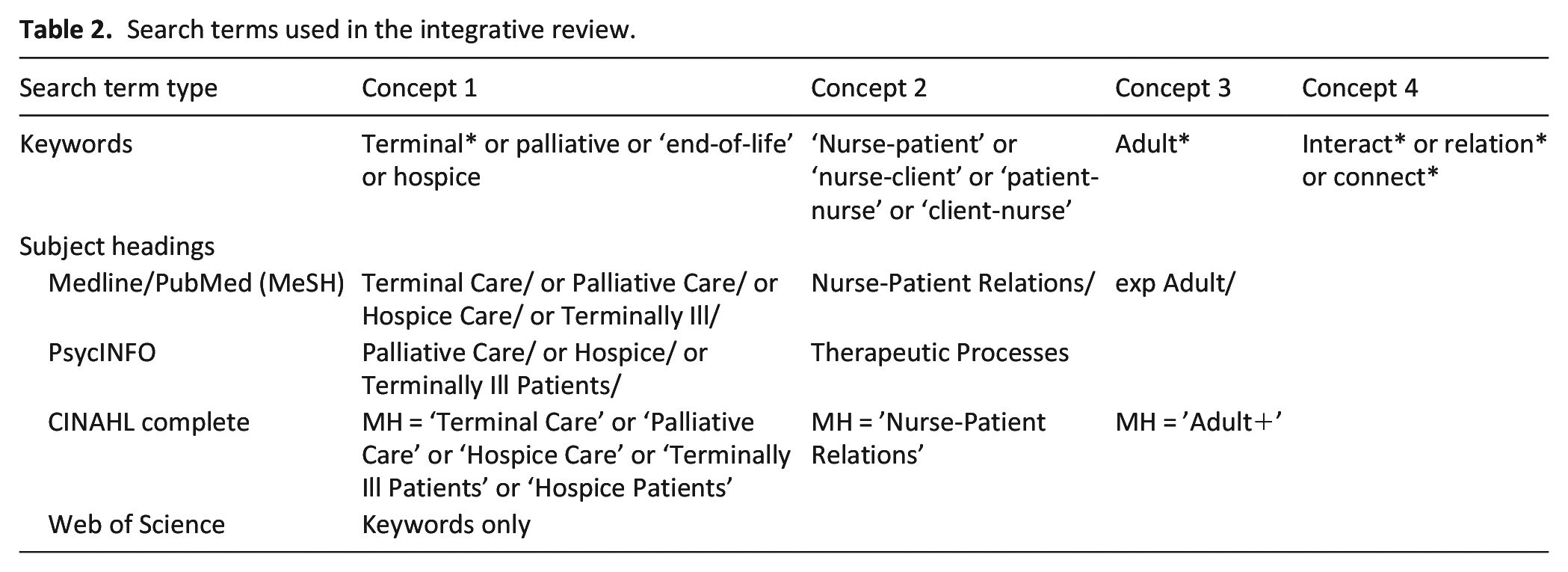
A search strategy was developed with a health-sciences librarian and used MeSH terms for the concepts: ‘nurse’, ‘nurse-patient’, ‘patient’ and ‘relationship’ with combinations of terminal* OR palliative OR ‘end of life’ OR ‘hospice care’ AND ‘nurse-patient’ OR ‘nurse-client’ AND interact* OR relation*. The phenomenon of interest was nurse-patient relationships in specialist palliative care or hospice care inpatient settings. Results were limited to English language, with no time limit applied (Table 2).
Search terms used in the integrative review.
The search yielded 1763 citations, which were imported into EndNote v.20. 26 Duplicate citations were removed in EndNote and the remaining citations were exported to Covidence, 27 where additional duplicate citations were automatically identified and removed. Citations were independently screened first by title and abstract, then full text, by two members of the research team. Conflicts were resolved by team consensus.
Quality appraisal
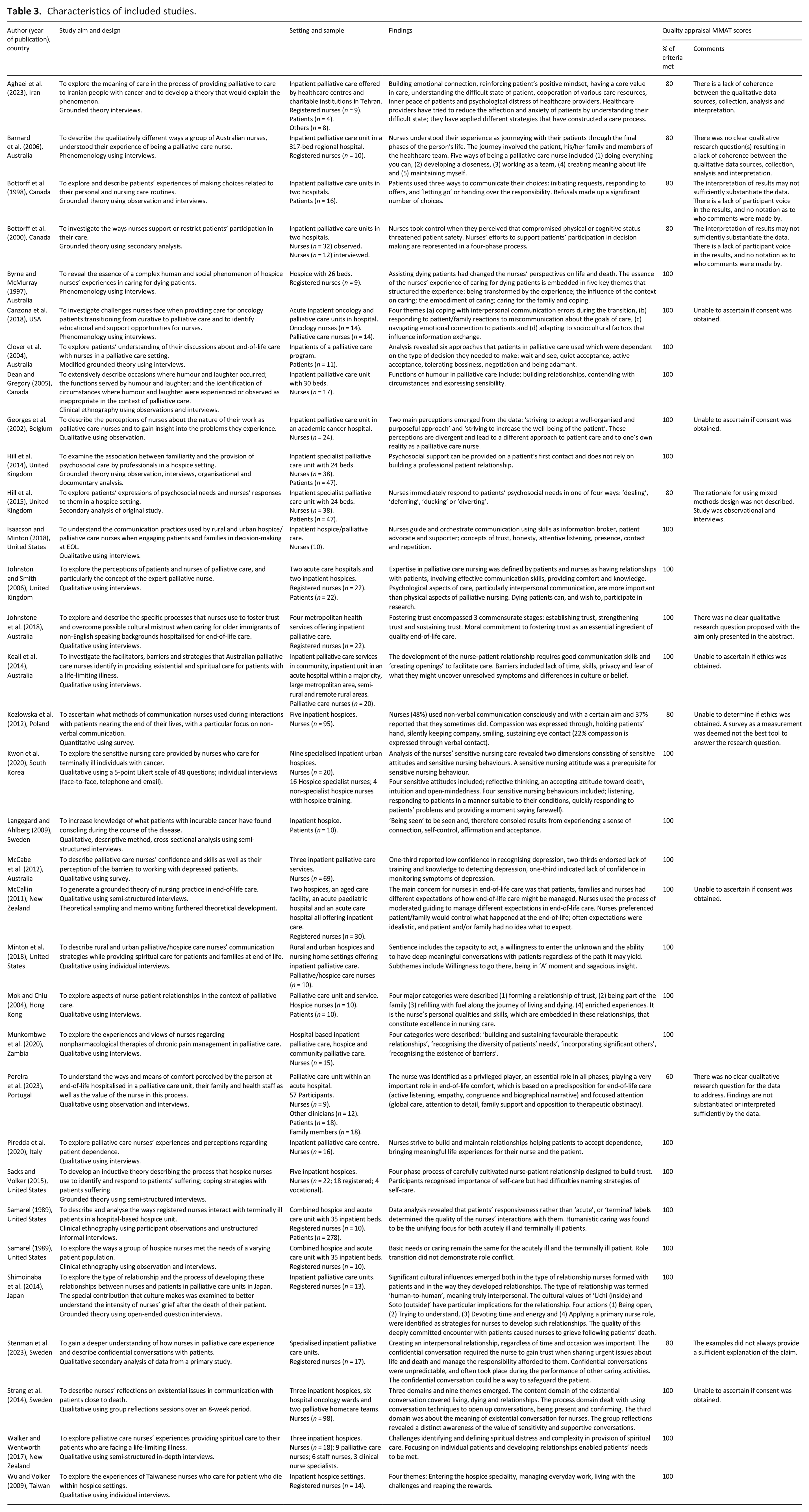
Quality appraisal was undertaken independently by three members of the research team to assess the quality, methodological rigour and risk of bias of each study included in the final review using the Mixed Methods Assessment Tool (MMAT). 28 Discrepancies were discussed by all members of the research team until final scores were agreed upon. Regardless of the MMAT scores, all articles meeting the inclusion criteria were included because it was considered they may include valuable data. Factors that contributed to lower scores are detailed in Table 3.
Characteristics of included studies.
Data extraction
Data about key features including authors, year of publication, country, purpose/aim, setting and context, sample, study design, data collection method/s and key findings were extracted into a spreadsheet (Table 3). Where a study included data from participant groups who did not meet the inclusion criteria, or from alternate settings, such as oncology wards, these data were not extracted. Guided by the Fundamentals of Care Framework, 3 which specifically describes context of care factors relating to inpatient settings, this review was limited to a focus on inpatient settings to help ensure findings were not influenced by differences in models of care, workload and time allocation, previously posited as confounders when examining nurse-patient relationships in cancer care 29 and nurses’ roles across inpatient and community palliative care contexts. 30
Data analysis and synthesis
For data analysis and synthesis, narrative synthesis as described by Popay et al. 31 was used. Narrative synthesis emphasises the use of words to explain and summarise findings, and to ‘tell the story’ of included studies. 31 Popay et al.’s 31 guidance does not represent definitive or prescriptive rules for approaching narrative synthesis, nor is a wholly linear approach suggested. Rather, this approach was used because of the emphasis on story-telling to guide organisation of data from included studies, and consideration of potential patterns or relationships in the data. 31 From a practical perspective, this approach allowed shared concepts and like ideas from both qualitative and quantitative research, to be grouped into themes, thereby forming the story. 31 Analysis was initially undertaken independently by the lead researcher using an iterative approach to enable identification of commonalities and differences, allowing for grouping of data according to similarities, common features and relationships. 31 A second reviewer then reviewed the preliminary findings so that any differences or disagreements could be resolved, and to enable refinement. The synthesis was then reviewed by the remaining members of the research team until the final findings could be determined.
Results
Search results
The decision trail for the search is presented in Figure 1.
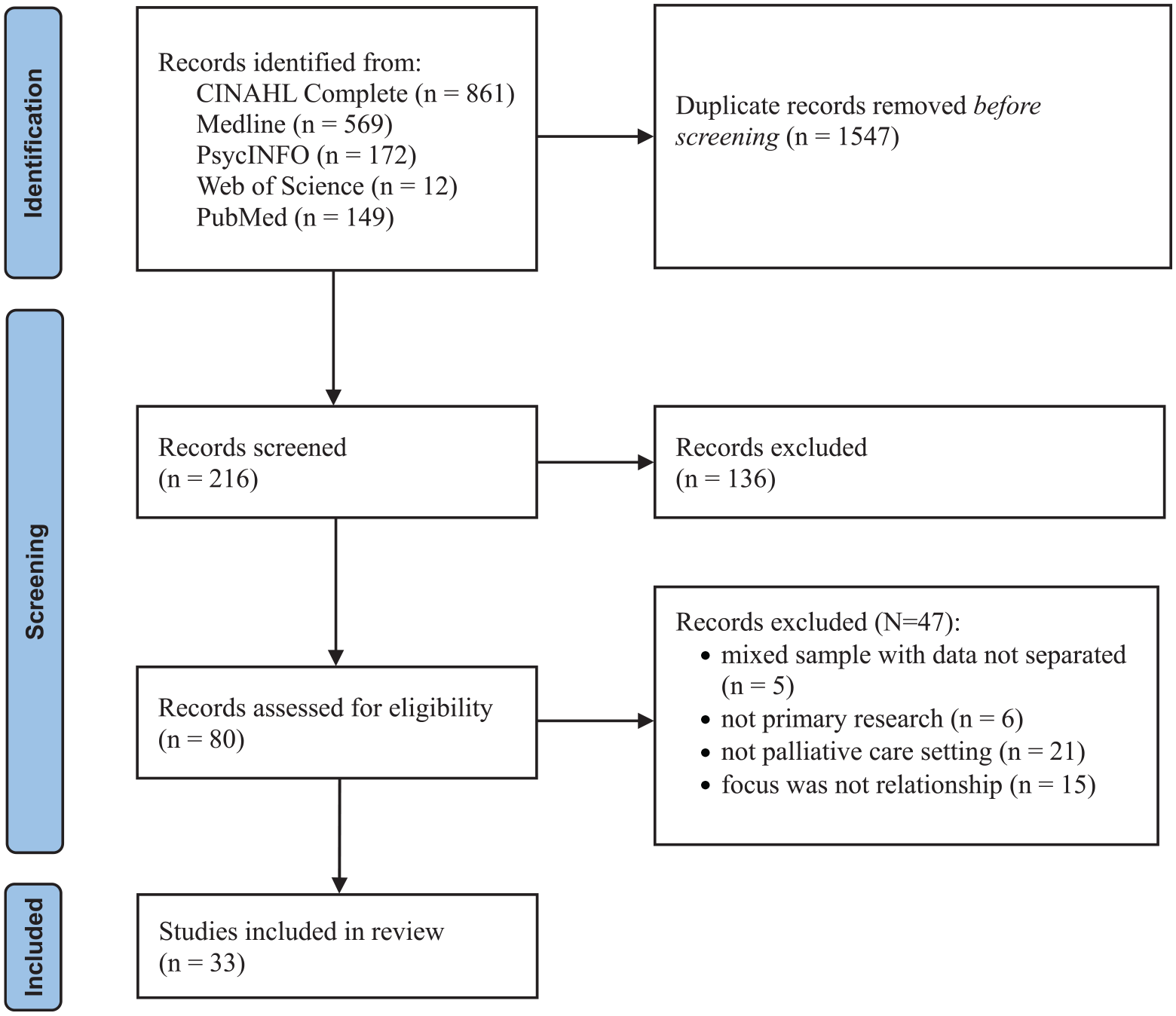
Decision trail of included studies (PRISMA flow chart). 25
In total, 33 papers from 31 studies published between 1989 and 2023, were included, with three papers reporting different components of the same study. Studies were conducted in the United States of America (n = 6),32 –37 Australia (n = 6),38 –43 Canada (n = 3),44 –46 Sweden (n = 3),47 –49 United Kingdom (n = 3),50 –52 New Zealand (n = 2),53,54 and one each in Belgium, 55 Hong Kong, 56 Iran, 57 Italy, 58 Japan, 59 Poland, 60 Portugal, 61 South Korea, 62 Taiwan, 63 and Zambia 64 (Table 3).
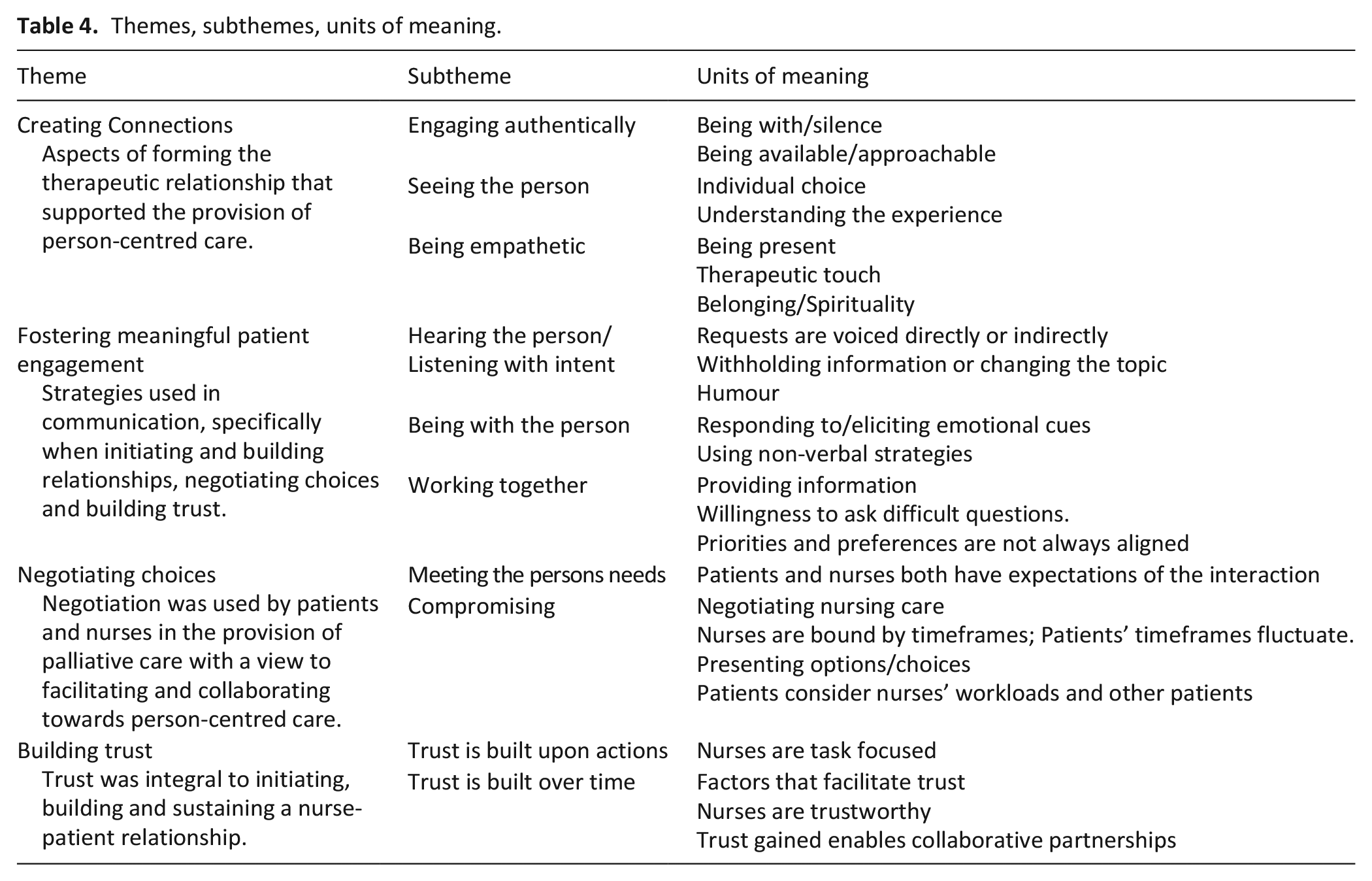
Study designs included qualitative (n = 29),32 –42,44 –49,52 –59,61 –64 survey (n = 2),43,60 and mixed methods designs (n = 2).50,51 In terms of quality, one study scored 60%, seven studies scored 80% out of a possible 100%, and the remaining studies (n = 26) scored 100% (Table 3). Studies were conducted in inpatient hospital palliative care units and inpatient community-based hospice care units, across metropolitan, rural and remote settings. Synthesis revealed four main themes (i) creating connections; (ii) fostering meaningful patient engagement, (iii) negotiating choices and (iv) building trust (Table 4).
Themes, subthemes, units of meaning.
Creating connections
Thirty-one studies provided detail about creating connections between patients and nurses,32 –52,54 –63 resulting in three sub-themes about the importance of (1) engaging authentically, (2) seeing the person and (3) being empathetic.
Engaging authentically
Engaging authentically during the provision of care, and demonstrating compassion was identified as key to creating connections with patients.33,34,38,43,52,54,55 Of the studies that included patients, authenticity was prominent when it came to connecting with the nurse.36,40,43
–47,50,51,56 Authenticity and genuine interest included the ability of the nurse to see the person and anticipate their needs.43,47,54,57 Authenticity was expressed differently between individuals, but understood when behaviours were genuine.42,43,46,54 Nurses reported that in order to respond to patients needs authentically, familiarity was necessary to increase interpersonal connections, which in turn, improved their ability to anticipate and respond to patient’s needs.50,51,56,58 This familiarity was described by nurses as beyond superficial, being like family,
56
sharing something of themselves,38,41 and reciprocal self-giving.
58
Familiarity was also explained by a patient as:
Everybody gets to know you and they know your illness and they know how to treat you and take an interest in you personally. (p. 705)
52
But importantly, as this hospice patient stated, familiarity was not essential if the nurse demonstrated genuine interest:
It’s not necessary to know the person who listens well as long as he or she signals that there is time. (p. E104)
47
Connecting through authentic behaviours also permitted the use of humour to strengthen connections.43,46 Connections between the nurse and patient were also strengthened through presence.33,34,41,42,54,55,61 Presence was also acknowledged as life-giving, spiritual,
34
comforting,34,54 demonstrating compassion,
33
kindness,
54
and empathy,34,35,41,42,54,59 requiring the nurse to be witness to, and acknowledge the patient’s suffering.35,49,52,54,59,61 Being present with a patient at times of great distress and acknowledging their suffering was important to authenticity, in spite of the potential for personal emotional drain, as a nurse described:
. . . sitting with the pain . . . I spent a lot of the night with him; sitting next to him. It was horrible but I had to do it. (p. 22)
54
Importantly however, another nurse reflected on how presence was only useful if it was authentic, purposeful and meaningful:
Presence or just being, can be a way of providing spiritual care, but you have to establish a rapport first. Otherwise, it can be misinterpreted. Otherwise, it can be like, ‘What’s she doing here? She hasn’t got anything to offer’. (p. 22)
54
The importance of presence to engaging authentically was also described by a patient:
The conversations, the silences too. There was a night when I felt very anxious and afraid to fall asleep . . . The nurse spent the whole night here with me in the room. We talked and even when I fell asleep, she stayed there. Incredible professional and incredible human being. (p. 9)
61
Humour was used by nurses and patients to create connections,43,46,48,61 initially on a superficial level but then as a means of contending with the tension and emotional aspects of the relationship and setting.46,48 Nurses were rarely conscious or deliberate in the use of humour whilst more often patients used humour to convey critical aspects of their care and situation. 46
Seeing the person
The importance of viewing the entire person, not just a patient and a list of tasks,33,39,43,46,47,51,52,54,56,57,63 acknowledging and respecting each patient’s values and beliefs, address spiritual and existential needs, acknowledging a patient’s purpose and meaning were identified as key to building connections.34,35,37,39,42,47,49,52,54,57,59 As a nurse described, to connect and know the patient deeply is crucial:
. . . You have to know their lived experiences. (. . .) You have not only to listen to words but also to observe the nonverbal language, because he wants to tell you something different. (p. 334)
58
Viewing the person holistically required nurses to seek to know and understand each person, and their needs,35,39,57 such as:
. . . I observe suffering with my eyes and with my heart. I can see he wasn’t sleeping, so I talked with him a bit. He’s worried. He’s leaving a young family. I sense it. You can hear it in the tone of their voice, and you can see it . . . and they make little comments. (p. 494)
35
Another nurse reflected on seeing the loss of self-identity that occurs with a terminal diagnosis, connecting to validate the patient’s experience:
And when someone has been given a terminal diagnosis, there’s the pain of a loss that’s impending. And it’s the greatest loss any of us will ever suffer because it’s the loss of ourselves. (p. 492)
35
Engaging empathetically
Behaviours that demonstrated engaging empathetically were noted in 19 studies.32,34
–37,39,42,43,47,48,51,54,55,57,59,60,62,63 Empathic engagement was described as being an active listener,33,39,42,43,47,51,55,62 offering advice,
51
providing emotional and physical comfort.33,57,59,62 A patient shared a description of a nurse who listened and therefore consoled them:
One of my caregivers is on a very professional level . . . I receive a lot of consolation from her . . . I think about how she consoles me . . . When I leave her, I feel stronger, mostly. She listens and tries to make me put my feeling into words. (p. E104)
47
Empathy is an inherent quality of humanistic caring which was embodied by one nurse:
It’s subjective. You can’t be objective and care or you don’t have a heart . . . Commitment to their humanness; totally separate from what’s wrong with ‘em. (p. 321)
37
By touching,
54
hugging,
37
holding hands36,60 nurses believed they were providing tangible symbolic gestures of concern, acknowledgement and deep feeling towards the patients’ situation, such as :
And then I gave her a big hug. That’s important. That’s the most important thing. Everyone needs that. (p. 318)
37
Similarly, a nurse explained that connecting through purposeful therapeutic touch was:
. . . very strength giving, it’s life giving, it’s love giving, it can smooth hurt, and it can take away fears.(p. 22)
54
Touch was occasionally reciprocated, suggesting that they had made a special connection:
I didn’t know why I had a special connection with some patients’ families. After the patients died, their families hugged me and cried just like I was part of their family. (p. 580)
63
Other nurses knew they had created connections by the way patients and families let them know.
41
Creating connections was sometimes unexpected, as this nurse described:
Sometimes the patient will do something, and it’s like my heart opens up. It’s like a feeling of warmth or something. I had 1 patient; he was a real bear. I couldn’t find anything good about him. . . . He touched my cheek, and I thought he was going to hit me. But no, all he did was touch my cheek and look at me. And I thought ‘Wow’. He was not a nice patient, but from then on, we got along. (p. 495)
35
When a connection was established, patients felt safe with the nurse, sharing some of their deepest concerns:
When I was caught in the toughest emotional struggle, I chose to disclose my deepest pain to my nurse, although it was not easy for me to tell someone else, I needed help . . . It was a tough situation and the strong trust in her drove me to ease this pain through dialogue with her. (p. 480)
56
In contrast, some nurses recognised that not all patients may be prepared or ready to invest in building the nurse-patient relationship,56,65 still, nurses remained hopeful, acknowledging that it was the patient’s choice.42,55,56 Making connections through caring behaviours was highly valued by both the nurses and patients but was heavily reliant on the nurse’s commitment to the process. 52 Equally, patients were motivated by authentic behaviours such as paying attention, guiding instead of directing and displaying excellent listening skills. 47
Fostering meaningful patient engagement
Nineteen studies provided data about how nurses approached patients for the purpose of creating the relationship and getting to know the person, establishing a partnership and accomplishing the goals of both the nurse and the patient during daily interactions.33,35,37,39,41 –43,47,50,52,54 –59,61 –63 The importance of fostering meaningful patient engagement was evidenced by (1) hearing the person; listening with intent, (2) being with the person and (3) working together. Nurses described being present,41,47,55,57 sitting in silence,42,54,56 listening with intent,35,39,41,42,47,54 –56,59,62 responding to and eliciting emotional cues,47,50,54,56,57,59,63 respecting patients choices50,55,58 and the provision of information35,37 as ways to foster mutual respect and engagement. Patients reported interpersonal skills and the value of the nurse-patient relationship was the most important aspect palliative nursing.35,37,52
Hearing the person; listening with intent
Listening with intent was identified by nurses as being an important aspect of connecting with patients while patients indicated that it demonstrated nurses were interested in them as individuals.39,47,52,57,61 This nurse tells how by simply listening to the patient provided a safe environment for patients to explore their feelings:
. . . Its important to stop and listen. To talk if need be. But sometimes it’s just important to just be with the patient. You’re not there to do things to a patient. You are here to listen. You are to let them say things to you which they need to get off their chest. (p. 22)
54
Actively listening for expressed psychosocial needs gave the nurses opportunity to explore the patient’s anxieties fostering meaningful engagement, as this nurse describes:
If a patient says to me, ‘Am I dying?’ we’re listening to them and talking to them. ‘Do you feel like things are catching up with you?’ ‘Yes, I feel like I’m dying’. And that opens the door. (p. 23)
54
Nurses sought to understand the patient in order to foster meaningful relationships,39,41,54 waiting to be invited in
59
dependent on the patients’ willingness to engage.
56
Occasionally nurses felt they were shut out of a relationship recognising they may need to amend their approach.
58
Others acknowledged that the patient might not be ready to disclose their vulnerability:
When patients only talked to you in a superficial way and did not express their emotions, this indicated they did not want to disclose their intimate feelings. It did not mean they rejected the nurse. They were not ready to disclose their feelings and sufferings. (p. 479)
56
Being with the person
Being with the person was focusing on being present-centred, maintaining or improving the person’s quality of life at that time.35,39,43,56,61 The nurses’ ability to provide person-centred, individualised palliative care whilst interacting with patients was dependent on whether the nurses were busy,37,43,50,52,55 their comfort and skill level,51,52 or if the person was imminently terminal. 37
Nurses acknowledged that confidence and experience were necessary to enable them to connect through use of presence and listening.39,42,52,59
I just listened to the patient. I am with him, with his heart. I may cry with him. What can I say . . . I do not provide anything; I just listen to his heart. I feel it is great if I can support the patient who suffered emotionally and if he is relieved because I listen to. (p. 459)
59
Silence was also recognised as an invaluable aspect of being with the person,42,54,55,61 such as:
Allowing people to talk or allowing silences. One of my mentors told me that you should sit on your hands or if you feel like you should leave don’t – stay a bit longer. (p. 3200)
42
Being with the patient occasionally was an intrusion into the nurse’s workload,43,55 while other nurses understood that it was sometimes the required action:
Sometimes I tell the patient that I do not know. I also try to stay with him, at the patient’s side. You don’t always have to talk; sitting at his side is sometimes enough, the patient may find some peace or someway to cope with his own emptions and thoughts. (p. 790)
55
Patients reported nurses’ ability to convey a sense of security and calm,43,47,52,61 while nurses described the use of presence as a way of providing spiritual care, such as:
. . . Whenever he was in fear and sorrow, I took the initiative to be with him, listened to his feelings, or was just there, and encouraged him, and I found he was changed. (p. 480)
56
Other times, nurses made considerable effort to find time to spend with the patient:
I’m going to go and have another chat with Vera and try to persuade her to stay in a bit longer. But I want to make sure we have plenty of time. (p. 8)
50
Working together
Working together was a culmination of those connecting behaviours of listening with intent and being with the person.
52
It required the nurse to demonstrate expert skills in communication43,66 and a commitment to tackle the difficult questions allowing the nurse and patient to come together in a moment of shared openness:
If a patient says to me, ‘Am I dying?’ we’re listening to them and talking to them. ‘Do you feel like things are catching up with you?’ ‘Yes, I feel like I’m dying’. And that opens the door. (p. 23)
54
Connecting and working together sometimes required nurses to utilise the family,
33
but ultimately it was focusing on what was important to the patient:
If we are directing the conversations instead of letting them direct the conversation, it is two different conversations. So, to really ask questions trying to pull out what’s important to them and then having the discernment and the wisdom to see what you can pull out that’s really important out of that conversation. It takes listening. (p. 10)
33
Negotiating choices
Twenty studies provide data on approaches used by nurses and patients in negotiating choices in meeting the needs of the person;32 –34,37,40,41,44 –46,48,50 –53,55,56,58,59,62,64 presented according to two subthemes: (1) meeting the needs of the person and (2) compromising.
Meeting the needs of the person
Nurses acknowledged that meeting the needs of the patient as a person was essential to fostering nurse-patient relationships,45,59 such as:
It’s a real part of the caregiving to recognize when patients need to make choices and when they need to make as few choices as possible. (p. 9)
45
Meeting the needs of the patient required nurses to identify and act upon the expressed needs,50,52 claiming that familiarity of the patient was necessary to respond to the request.
51
Nurses initially sought patient knowledge and understanding of their needs and perceived capacity to ascertain what choices might be able to be offered,32
–34,41,48,53,56,59,64 while others relied upon their intuition of the patients’ needs.
46
But it was not always realistic to give the patient a choice, as this nurse claimed:
People are autonomous beings. It’s about who has the power or control. . . Working with patients, ultimately, I would like them to have total control, but it has to be moderated according to what is possible, what they are ready for and what they can do at this moment. (p. 2327)
53
Whilst the evidence demonstrated that patients and nurses sought to resolve any issues in a manner acceptable to all, their approaches were diverse. In four studies50,53,55,62 nurses cited recognising the importance of creating a trusting environment and were committed to enabling patient choices for activities related to hygiene,44,58 medications,37,44,58 and general day-to-day activities.37,44,45,58 Patients also negotiated choices either directly or indirectly voicing their needs, by initiating requests, responding either favourably or indifferently to offers and suggestions, and occasionally allowing the nurse to make the final decision:
Even if you end up saying (to the nurse), ‘Well, I don’t care. You decide’. Even if that is the outcome, I think it’s very important that the conversation at least be broached, be started. (p. 11)
44
Compromising
Negotiating choices was about compromise, as in compromising about the goal or objective and the timeframe. When nurses felt that strongly enough about a goal or the task at hand, sometimes opportunities for compromise or negotiation were not provided, particularly when nurses felt it was not realistic, feasible or safe.
53
Rather, nurses described offering pseudo-choices while actually completing the task before the patient could respond,
45
or dissuading the patient altogether.
40
Patients’ expectations of negotiation and compromise also changed over time, such as when the independence lessened,
44
when they trusted the nurse as an expert:
I rather do accept what they freely give me . . . I suppose I have to trust them. What other choice do I have? They are the experts; they have the knowledge and training. (p. 337)
40
Patients did not want to appear demanding when negotiating their choices, with some describing alluding to nurses’ workloads before expressing a request.
44
When requests were not adequately considered or they had not been provided with an adequate rationale, patients’ became persistent,40,44,45 and others resorted to withholding vital information, throwing away offered medications or enlisting families to advocate on their behalf when they felt manipulated.
44
When given too many options at once, or little time to consider them, some patients viewed choice as burdensome, irrelevant or even tokenistic.
45
Patients described feeling coerced, bullied or manipulated,
40
with nurses driving the agenda:
It was just that the nurse had an agenda, a time agenda, and had formed an opinion about what they thought I needed and when I needed it . . . The outcome was rather a nasty confrontation. . . I just got fed up and said that I wanted to be alone and go away. (p. 10)
44
When offered choices, patients considered whether they felt physically or psychologically ready to perform the offered activity of care, sometimes asking the nurse to delay or postpone the cares while they considered all options or until they felt able to.40,44 In contrast, nurses offered choices that fit their timeline, citing time limits,
45
doctors’ orders,
44
senior nurse managers,
40
hospital routines and work constraints
45
as the reason. A nurse shared:
It’s sometimes easy to phrase things so that you get what you want . . . I’ll do that when I know what my day is like and the things that I should get done, how much time that I have, and when my breaks are, and when they might have an appointment or something. Then I’ll phrase questions like that, so it fits into my schedule of the day. (p. 9)
45
Whilst this approach was intended to make the patient feel as though they had choice, both options were about meeting nurses’ timeframes.
45
Conversely, another nurse described how it was important for them to put aside their own agenda, timeframe and focus on the patients need:
‘. . . doing what the patients needed even if they were busy . . .’ and that ‘caring for hospice patients involves not doing what I need, but helping patients when they need’. (p. 4)
62
Building trust
Sixteen studies provided data on how trust is sought, established, sustained and occasionally lost, all requiring constant actions by the nurse, and attentive energy by the patient.33,35,40 –42,45,47,48,52,54,56,58,59,61,63,64 Trust was integral to the relationship,33,35,41,42,56 enabling the patient to feel secure, 41 valued, 52 consoled with a sense of belonging.47,61 There were two themes related to this category: (1) trust is built upon actions and (2) trust is built over time.
Trust is built upon actions
Trust was completely reliant on the actions41,52 and attitudes45,56,61 of the nurse. Trust fostered deeper conversations between the nurse and patient,33,35,42,48,56,59,61 and the utilisation of meaningful presence.
54
Eight studies highlighted that trust was built when nurses listened to the patient, acknowledging their story and being authentically empathetic.33,45,47,56,58,59 Occasionally trust afforded a special connection that nurses likened to being a friend or family.56,63 Early establishment of trust paved the way for nurses to provide person-centred care,35,56 patient advocacy,33,56 forming favourable therapeutic relationships.48,64 Trust supported nurses to console,
47
provide existential care whether the nurse was spiritual or not,42,48 and explore alternative options in the provision of care.
64
Nurses were aware that trust was achieved by getting it right from the start and being seen to be doing the right thing, supporting the patient, as described by this nurse:
. . . the patients know that you are supporting them and are on their side; that you are never going to ‘turn up your nose’ and do what you want to do. (p. 765)
41
Nurses sought to be trusted,48,58 monitored trust as an indicator of the strength of their relationship,
35
and were aware that trust was tenable and could be lost
41
if actions were not congruent to patients wishes.
40
Trust was integral to enabling a therapeutic relationship between the nurse and patient, with both participants watching and waiting for the behaviours that instilled trust.
47
Though it appears patients remained vigilant while some nurses may not have been so vigilant in their actions:
Consolation to me is when I can trust people when someone says, ‘Goodbye then, I’ll soon be back’, . . . and then she really is coming back. If she isn’t, I can’t trust her. But if she is, it’s a great solace. (p. E104)
47
Trust and the relationship can be lost very simply,
52
as one nurse explained:
‘. . . if you don’t have trust, you have no relationship . . .’ and ‘You can lose trust by just not even being able to answer a buzzer or something’. (p. 767)
41
Acknowledging that marginalised people may have an inherent mistrust in the health system, nurses described having to traverse additional hurdles such as language and cultural beliefs in building trust:
That trust and rapport is very different to what other staff have . . . I think it’s because I’m Turkish [and the family thinks] ‘Okay, she speaks our language, she’s of our religion’. (p. 765)
41
Trust was also tenuous,
40
and founded on action, as this patient explains:
They [the nurses] come in smiling – they are always smiling – and present tablets. I ask what are they for and the nurse looks at me blankly and says, ‘They are new, the doctor’s ordered them’. I feel like saying, ‘Well, I don’t care what the doctor’s ordered. Tell me what they are and any side effects and maybe I’ll take them’. (p. 337)
40
Trust is built over time
Some nurses were sensitive to the time it could take for patients to build sufficient trust to express their concerns or preferences.
45
To expedite the process, nurses disclosed personal attributes of themselves to build trust:
When they come to us, we need to get it right at the start. We need to give a bit of ourselves first and give a bit about what we really are here for and how we want to try and support them . . . Maybe then they would feel more comfortable disclosing those kinds of things to us and more comfortable at the start, feeling ‘It’s okay’. (p. 765)
41
The building of trust in the nurse-patient relationship was also described by nurses and patients alike. A nurse suggested trust was an ongoing process:
Trust – I guess you’ve got to feed it. . . to let it grow. And the more that it grows, the better [as] it will make it easier for us and them to be able to do things better. (p. 766)
41
From the patient perspective, trust could be built through advocacy and sharing:
With a trusting relationship, as patient I could tell her everything I need. She would bring my issues to the meeting at the hospital, so my concerns would be heard. It wouldn’t be that way if our relationship were a distant one. The nurse was not only a healthcare professional she was also a good friend, part of the family. (p. 480)
56
Discussion
Main findings
This review had two aims. The first was to identify and synthesise data on how nurse-patient relationships are fostered in specialist palliative care settings, and second, to examine how nurse-patient relationships were perceived from the nurse and patient perspective. These findings have demonstrated that nurses and patients alike are invested in the nurse-patient relationship, with both parties appreciating connections that are fostered, meaningful engagement, opportunities to negotiate choice and build trust.
Whilst this review highlights the complexity and richness of what happens when nurses and patients interact positively, the findings also explicate the consequences when the patient’s perspective is overlooked. Patients and nurses described both opposing and supportive relationships, while some nurses were willing to put the patient first, they cited workloads and daily tasks as activities that may be more favourably considered than engaging meaningfully with patients. Patients, nevertheless, disclosed the richness of the relationship52,56 while others have had to expend energy into creating and maintaining a sense of safety and succour.40,44 Spiritual, existential distress and psychological issues for patients and families have been promoted as areas of important nursing research. 67 Other research has reported that nurses have lost the sensitivity to deliver respectful, compassionate, person-centred care,68 –70 with the provision of palliative care being reduced to a series of checks and tasks within care pathways replacing good clinical practice encompassing empathy, humanity and communication. 71
What this review adds
The nurse-patient relationship is at the core of this review. These findings demonstrate that nurse-patient relationships are fostered using diverse actions, gestures and approaches. Nurse presence, authenticity, familiarity, empathy and ensuring patients were seen, were highly valued by patients, bringing comfort, 54 and a sense of support. 51 Similar to previous research which has demonstrated the perpetual importance of communication in palliative care,72,73 these findings further demonstrate how communication was key to working in partnership with patients in their care. The nurse’s ability to establish rapport, be trusted and be fully present, as part of the nurse-patient relationship was influenced by several factors highlighted in this review. Even when justified according to competing demands in nurses’ workload, resisting patient requests is demonstrative of the power imbalance that exists in the nurse-patient relationship.40,44 For nurse-patient relationships to be therapeutic and/or beneficial for patients, power imbalances must be avoided.
Although the nurse-patient relationship is known to be vital to ensuring safe and effective care, 74 knowing what is important to patients in palliative care and how their experience of care affects them enables health care organisations and nurses to align themselves with the principles of person-centred care. However, these findings suggest it is important not to simply assume that nurses can form positive and/or therapeutic relationships with patients, 75 particularly given that this may not always desired by the patient.56,58 or personal and behavioural barriers exist between the nurse and patient. 13 Nonetheless, given that, by-comparison, the majority of data came from nurses, these findings provide a clear argument for ensuring patients’ voice and experience is more equally considered, if the nurse-patient relationships is to be understood comprehensively and holistically.
Strengths and limitations
One of the strengths of this integrative review was the methodological rigour of the process, which contributes to the trustworthiness of the findings. The inclusion of evidence from multiple countries and heterogenous nature of the evidence also help contribute to the transferability of the findings; in essence because despite the differences, the synergies in nurse and patient experiences were clear. One of the challenges faced in attempting to answer the research question was that there is no universally accepted definition for or meaning of nurse-patient relationship. Compared to the amount of evidence presented from the perspective of the nurse, the paucity of evidence from the patient perspective is a limitation. As it was not possible to include research published in languages other than English, it is possible some research literature may have been missed. Finally, as the search was limited to peer-reviewed published research literature, it is possible that some unpublished research evidence and non-research literature may have been missed.
Conclusion
This review explicates an important perspective on the nurse-patient relationship in palliative care, building understanding on the importance of seeking to understand each person as an individual, including their unique needs, preferences and wishes for care. The evidence demonstrates that nurses’ commitment to being authentic, listening intently and building trust are core to fostering therapeutic relationships in palliative care. Yet, equally, trust cannot be assumed, and relies on nurses’ use of verbal and nonverbal indicators and earning patient trust. These findings emphasise the importance of nurses reflecting upon their approach to person-centred care in clinical practice, their actions and communication style and how these may affect the patient experience and nurse-patient relationship.
Footnotes
Acknowledgements
The authors acknowledge the assistance of Ms. Vanessa Varis, Faculty Librarian, Curtin University, for her support with the search strategy.
Author contributions
All authors meet the criteria for authorship as stated by the ICMJE or Australian Code for the Responsible Conduct of Research authorship guidelines. SB was responsible for the planning, design and conduct of the research, including database searching and data extraction. All authors contributed to citation screening. SB and MJB were responsible for data synthesis and led the manuscript development. MJB, EC and GKBH contributed to guiding the review design and conduct and editing of the manuscript. All authors have given final approval of the manuscript to be submitted for publication.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) declare no financial support for the research, authorship and/or publication of this article.
Ethics and consent
The author(s) declare ethics and consent was not deemed necessary for this study or publication of this article.
Data management and sharing
All relevant data are within the manuscript. Any other data are available upon request from the corresponding author.