
Abstract
Background:
Almost half the world’s population lives in rural areas. How best to provide palliative care to rural populations is unclear. Privileging rural patient and family voices about their experiences of receiving care delivered via rural palliative care models is necessary.
Aim:
To identify the key palliative care elements that rural patients with palliative care needs and their families perceive to be critical to receiving the care and support they need to live well.
Design and Data Sources:
A systematic review and meta-synthesis registered with Prospero (CRD42020154273). Three databases were searched in June 2024. Raw qualitative data were extracted and analysed using Thomas and Harden’s three-stage thematic synthesis methodology. Findings reported according to the PRISMA statement.
Results:
Of the 10,834 identified papers, 11 met the inclusion criteria. Meta-synthesis of extracted, raw quotes (n = 209) revealed three major themes: (1) Honouring the patient’s existing relationship with their General Practitioner (GP); (2) strategically timed access to specialist services, clinicians and equipment is critical; and (3) a need to feel safe, prepared and supported.
Conclusion:
The strategic inclusion of specialists alongside primary care providers is integral to optimising rural palliative care models. General Practioners are central to these models, through being embedded in their communities and as the conduit to specialist palliative care services. Rural palliative care patients and families value responsive care, trajectory signposting, effective communication, 24/7 support and recognise the value of virtual health. Globally, positive public policy and funding is critical to ensuring access to GP-led, specialist-supported, rural palliative care models.
Keywords
Despite improvements in rural healthcare processes, challenges persist in the delivery of high-quality palliative care for people living in rural and remote areas.
There is limited qualitative evidence representing rural patient and family voices on how best to deliver palliative care.
This systematic review and meta-synthesis has revealed several key elements that rural patients with palliative care needs and their families deem most important, including honouring the central role of general practitioners; strategically timed access to specialist services, clinicians and necessary equipment; and the presence of various processes and people who contribute to feeling safe, prepared, and supported across the illness trajectory.
This systematic review and meta-synthesis affirms the importance of a population-based approach to rural palliative care delivery, advising the need for strategically timed specialist palliative care input to better support the care provided by primary care clinicians, especially general practitioners, using appropriate tools such as comprehensive care planning, care coordination, and early signposting of clinical changes.
It identifies that rural patients and families will have a sense of safety, security and preparedness if they have access to: 24/7 after-hours palliative care support, competent clinicians, care planning and receive clear instruction on what to expect as the patient’s condition changes.
It calls for commitment from all levels of government to develop positive public policy underpinned by adequate funding to ensure the development of and access to GP-led, specialist supported, integrated rural models of palliative care.
Background
Despite global attempts to improve rural healthcare1 –4 and calls for end of life care reform,5 –8 people in rural areas with palliative care needs remain underserved.9 –12 Resource constraints, geography, sparse population distribution, and a limited workforce impact specialist palliative care access and delivery. 12 Older people are disproportionately represented in rural populations and experience a higher burden of disease, other comorbidities and greater levels of disability.2,13,14 Collectively, these factors increase the need for rural palliative care.2,13,14
Palliative care aims to improve the quality of life of patients and their families facing problems associated with a life-threatening illness, by preventing and relieving suffering through identification, assessment and treatment of physical, psychosocial and/or spiritual complaints. 15 Most patients with palliative care needs express a desire to maximise their time spent in a location of their choice.10,16 For many, the preferred location is their home or within their own community (i.e. a local hospital). 16 Achieving this depends upon the patient’s access to 24-hour, 7-day-per-week community-based palliative care services. 17 In rural settings, this can be impacted by the aforementioned barriers, as well as fragmented service delivery; difficulty recruiting and retaining staff; unclear referral processes to specialist services; and dual personal and professional relationships among rural care providers creating potential emotional and ethical challenges.10 –12,18,19 While most patients with straightforward palliative care needs living in rural communities can access primary palliative care, 6 it is more challenging to access specialist palliative care services to address complex and persistent palliative care needs.6,12,20 How best to situate specialist palliative care services to complement existing rural services remains unclear.
Increased demand for seamless, well-coordinated care in the last year of life has led to the development of different primary and specialist palliative care models. 21 A model of care is defined as ‘. . .an overarching design for the provision of a particular type of healthcare service shaped by a theoretical basis, evidence-based practice and defined by standards. It consists of defined core elements and principles and has a framework that provides the structure for the implementation and subsequent evaluation of care’ 21 (p. 49). Key elements able to optimise rural palliative care models include: (1) a multidisciplinary team approach integrated across local healthcare settings;22 –35 (2) information systems that allow care planning and information sharing amongst the team,22 –35 including virtual care;25,26,34,35 (3) care coordination, overseen or led by specialist palliative care clinicians;25,27 –29,34 and (4) the provision of palliative and end of life care information (i.e. what to expect along the illness trajectory, and ways of navigating this time) for patients and families.22 –24,36 While this service utilisation data sheds light on rural palliative care access, delivery, and key components of service design which positively influence care quality, more information is required to understand the experiences of rural palliative care consumers in receipt of such care.9,16,19,20,36,37
Healthcare consumers, namely patients and their families, have a crucial role in service appraisal and in identifying healthcare priorities. 38 Exploring and understanding the perspectives and experiences of rural patients and their families receiving care through rural palliative care models deepens our understanding of their needs and what care elements matter most for this population.
Methods
Aim
To identify the key palliative care elements that rural patients with palliative care needs and their families perceive to be critical to receiving the care and support they need to live well.
Design
While our earlier systematic review – narrative synthesis 36 evaluated rural palliative care models from a quantitative perspective, the search process revealed many qualitative studies reporting on patient and family perspectives about their experiences of receiving care through such models. This prompted a meta-synthesis of raw qualitative data to better understand this populations’ reported perceptions and experiences. The raw data were extracted, analysed and synthesised across the included studies using Thomas and Harden 39 three-stage thematic synthesis methodology. This meta-synthesis was prospectively registered with PROSPERO (CRD42020154273) as an extension to the registration for the first systematic review, 36 completed and published in 2023. The Preferred Reporting Items for Systematic Reviews and Meta-analyses reporting guidelines 40 guided study reporting.
Research question
What are the key elements within palliative care models that support rural patients with palliative care needs and their families to receive the care and support they need to remain in their community?
Eligibility criteria
Inclusion criteria
Eligible studies were published in English in peer-reviewed journals since January 2000, presenting raw, qualitative data addressing the primary study aim, collected from patients with palliative care needs and/or their family, and met the following criteria:
Population: Eligible participants included paediatric and adult patients with palliative care and/or end of life care needs receiving care in a rural community. Studies were included if they defined the participants as being ‘terminal’ or ‘palliative’ or requiring ‘end of life care’ or ‘palliative care’; or if ⩾50% of the participants were: categorised as having New York Heart Association (NYHA) Level III or IV limitations; 41 or had a terminal illness that met the Supportive and Palliative Care Indicators Tool™ (SPICT) criteria. 42 Family members are specified by the relationship to the patient, including spouse, parent, sibling or child. The term ‘palliative care’ has been used throughout this manuscript to reflect the care received by this population.
Setting: As no global coding system exists for rurality, studies needed to explicitly mention that ⩾50% of participants lived in a rural community. Given known telecommunication gaps in some rural settings,43 –45 studies needed to have been undertaken in a high-income country as defined by the World Bank criteria. 46
Intervention: Rural palliative care models needed to include: two or more elements of care delivery (e.g. complex care planning, telehealth appointments/videoconferencing and/or care coordination) and meet the model of care framework definition. 21
Search strategy and information sources
The search strategy was designed in consultation with two University librarians. It used a combination of free texts (as keywords) and MeSH terms utilising Boolean Logic operators of ‘AND’ and ‘OR’. Limiters, including ‘peer reviewed’, ‘English’ and publication from January 1, 2000, were applied (Appendix 1). The database search was performed during June, 2024. We searched PubMed, Ovid MEDLINE and Cumulative Index to Nursing and Allied Health Literature (CINAHL). CareSearch – the Australian palliative care knowledge network PubMed search filters for ‘Rural Health’ ‘Models of Service Delivery’ and ‘Palliative Care’ were used to increase precision. 47 The included studies reference lists were hand-searched.
Selection process
Records returned from the searches were imported into Endnote X9 and then uploaded into Covidence 48 before duplicates were removed. CM categorised 100% of the remaining retrieved records against agreed a priori inclusion criteria. CV reviewed 20% of the returned records for accuracy, and any discrepancy was reviewed by the team for consensus. All authors reviewed and voted on the outcome of full-text reports under review and arrived at a consensus for any conflicts via collective discussion. The ‘PRISMA’ function included within Covidence 48 was used to generate the flow chart and to capture the full-text reasons for exclusion.
Data collection process
Study data were extracted independently into an electronic spreadsheet in Microsoft Excel® by CM. Items included: country, aim, participants, setting, study design, intervention, palliative care element/s, results, strengths and weaknesses. Quills and Abernethy’s 49 definitions were applied, with a ‘primary palliative care service’ considered a model where non-specialist palliative care clinicians provided most care versus a ‘specialty palliative care service’ being where specialist palliative care clinicians delivered most care. Unless otherwise specified, references to ‘nurses’ were interpreted as ‘registered nurses’ and medical staff were interpreted as non-specialists unless it was stated that they had specialist palliative care expertise.
Study risk of bias assessment
To ensure inclusion of the highest quality data, each included paper underwent rigorous assessment using The Walsh and Downe 50 ‘Appraising the quality of qualitative research’ tool. This tool was selected due to its ability to assess the integrity, transparency, and transferability of findings. The tool’s simple point scoring system required eligible studies to meet ⩾75% of the appraisal criteria (Yes = 1 point; No = 0 points) to be included. This appraisal process was performed by CM and overseen by CV and JLP.
Data analysis
Thomas and Harden’s 39 three-stage thematic synthesis methodology were applied to generate new interpretive constructs, hypotheses and/or explanations beyond the outcome of the identified primary studies. ‘Line-by-line’ text coding was performed on each item (quote) of extracted raw qualitative data. This was followed by grouping similar concepts to develop ‘descriptive themes’. From there, ‘third order interpretations’ (analytical themes) were generated by synthesising the collective meaning of the combined data, escalating our findings beyond the original outcomes of each individual study. 39 Privileging the raw patient and family data ensured it remained central to analytical theme generation, limiting bias due to secondary interpretation of pre-identified themes. Microsoft Excel® was used to manage the data at each stage of the analysis.
Results
Of the 10,834 records identified 3661 duplicates were removed, leaving 7173 abstracts for screening, with 214 undergoing a full review, of which 11 met the inclusion criteria (Figure 1).51 –61 Ten studies collected data using semi-structured interviewing,51,53 –61 with one drawing additional data from open-ended survey questions, and the final study using discovery interviewing methadology. 52 Six studies used a phenomenological;53,54,56,58 social constructionists; 57 or ethnographic approach; 60 one used a qualitative descriptive approach; 51 one used a retrospective descriptive approach; 52 while the three remainder captured qualitative data as part of a mixed methods study design.55,59,61 Most (n = 8) collected data from family members only;52 –56,58,60,61 two collected data from patients and family members;57,59 and one collected data from patients only. 51
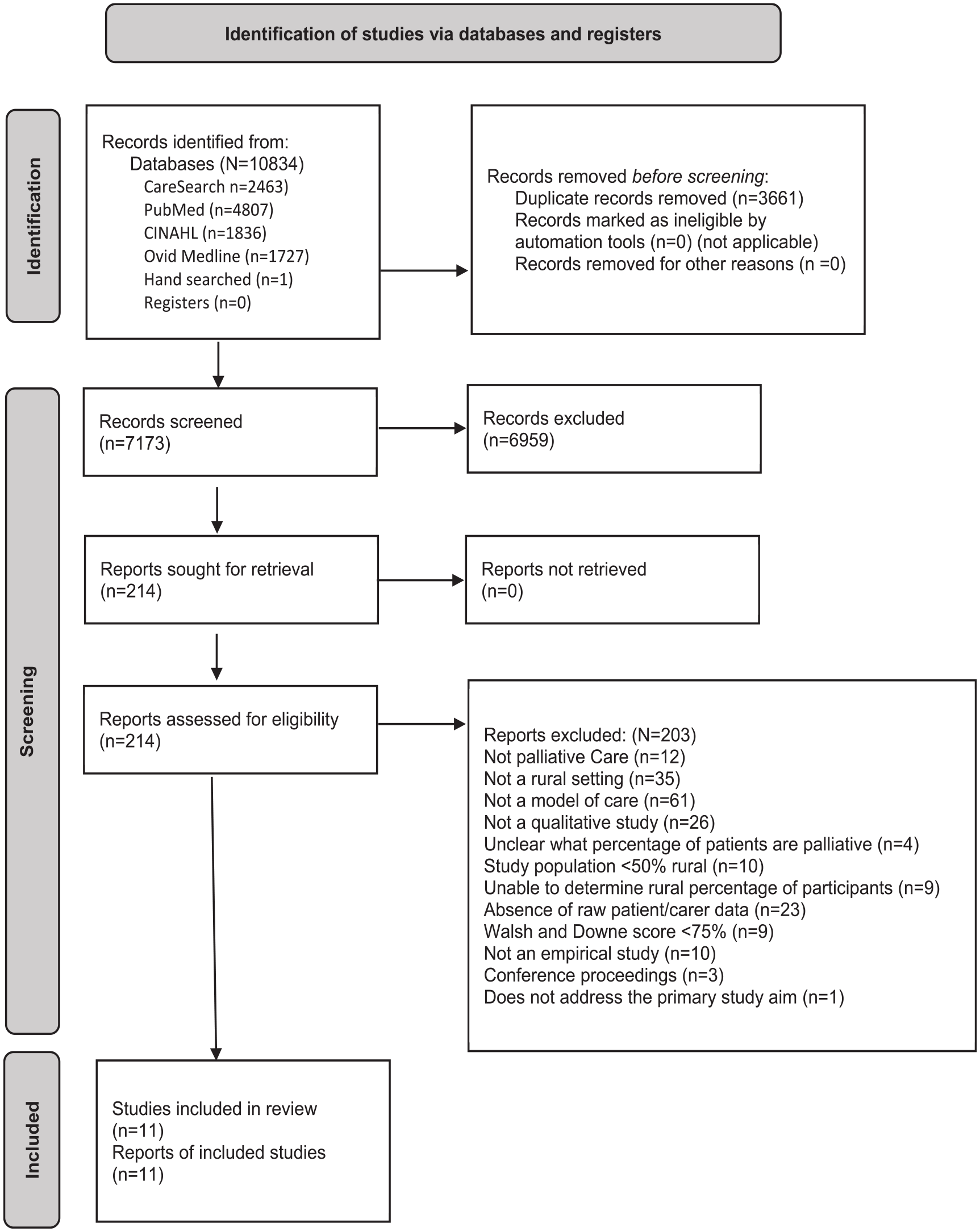
PRISMA Flow Diagram. 40
Study location and setting
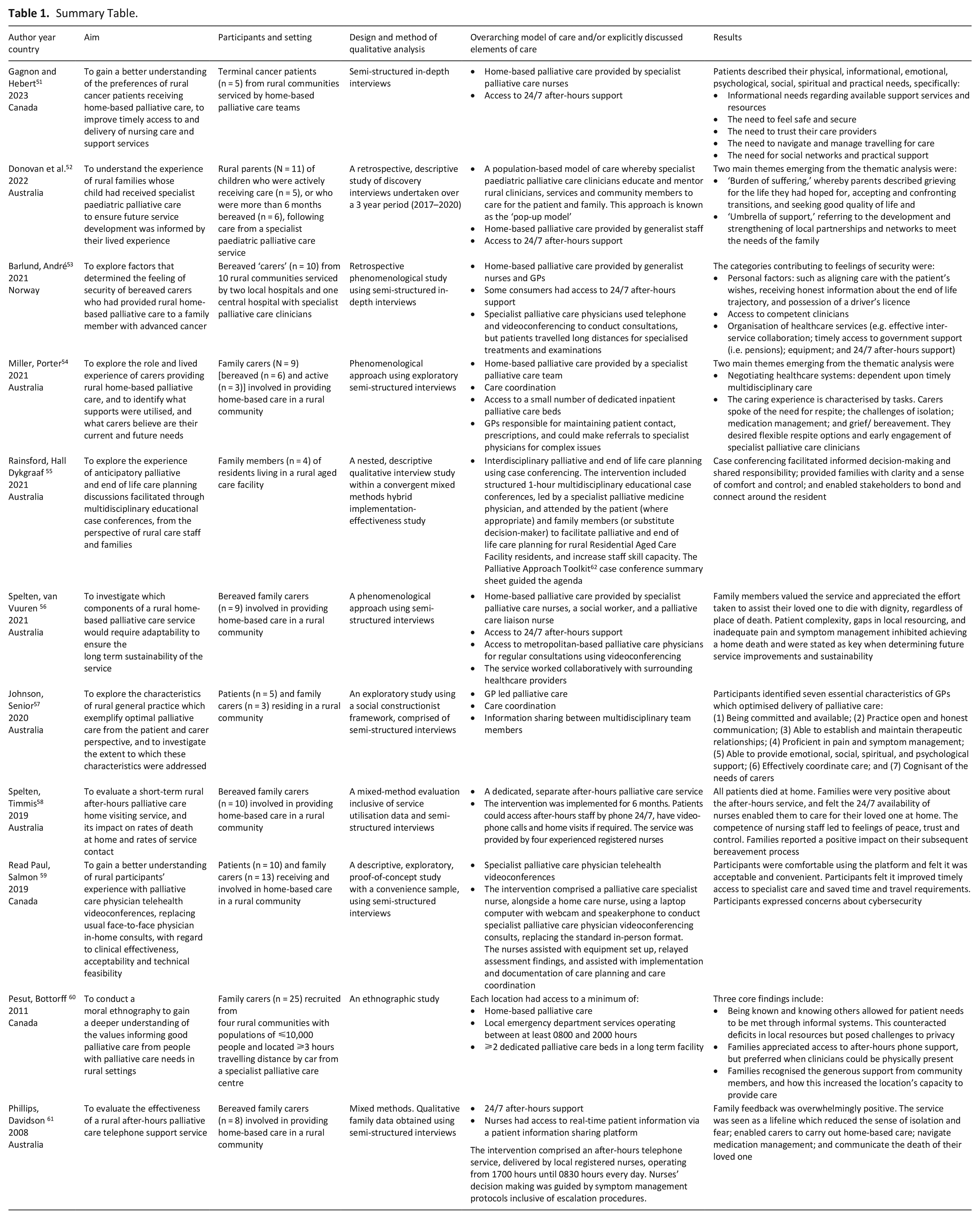
All studies were undertaken in high-income countries with universal healthcare. Seven were Australian,52,54,55 –58,61 with the remainder undertaken in Canada (n = 3)51,59,60 or Norway (n = 1) 53 (Table 1). Nine studies involved a specialist palliative care service;51 –56,59 –61 one study evaluated a generalist program that expanded to include specialist palliative care after-hours home-based care; 58 and another provided generalist level care only. 57 In most studies (n = 9), patients, at a minimum, had daytime access to home-based care.51 –54,56,58 –61 In six studies, consumers had access to 24/7 after-hours support,51 –53,56,58,61 and a seventh study described where rural clinicians offered this level of support despite it not being a paid or recognised component of their employment. 60
Summary Table.
Sample characteristics
Data were collected from a combined total of N = 122 participants. Most (84%) were family members (n = 102) while a smaller proportion were patients (16%, n = 20). Of the five studies reporting demographics, three reported patient (n = 20) mean age (69.1 years)51,57,59 and two reported family members age range (37–76)53,54 or mean age (60.5 years). 53 Of the six studies reporting participant gender, the majority (80%, n = 51) were female.52 –54,56 –58 Of the eight studies reporting the patient’s progressive illness, most (n = 5) involved patients with either malignant or non-malignant diseases,52,54,56,58,59 while three studies only included patients with cancer.51,53,57
Synthesis
Out of the 209 extracted patient (n = 53) and family (n = 156) quotes that explicitly addressed the research question, three analytical themes emerged as being central to rural palliative care, namely: (1) Honouring the patients existing relationship with their General Practitioner (GP); (2) Strategically timed access to specialist services, clinicians, and equipment is critical; and (3) Feeling safe, prepared and supported across the palliative illness journey is essential.
Honouring the patients existing relationship with their General Practitioner
When considering the role of the GP across the palliative journey, two sub-analytical themes arose. (1) Rural patients and their family members value GPs whom possess effective communication and interpersonal skills; and (2) rural patients and their family members often have long-standing and/or close relationships with their GP which strengthens the clinician-consumer relationship, especially as their palliative care needs increase.
Effective communication and interpersonal skills
Rural patients and their family members value GPs who possess effective communication and interpersonal skills.53,57 Rural patients expressed being comfortable discussing their terminal illness and associated needs and concerns with their GP, with the therapeutic relationship enhanced when the GP adopted an informal and friendly conversation communication style 57 ‘. . .more like going to visit a good friend rather than just a doctor’ (and equated their conversations with) ‘. . .having a good old chat’ (Patient, p. 2165). 57
Similarly, family members appreciated a GP’s ability to contextualise their observed deterioration and communicate these changes respectfully, gently, and honestly:
57
The [GP] provided a metaphor of a river and being in a boat and maybe just letting the stream flow rather than trying to steer it in any particular direction. . .maybe watching the stream. . .rather than anticipating where it’s going to end up. . .maybe dealing with it 1 day at a time. (Daughter of a patient with advanced cancer, p. 2164).
57
Both patients and family members preferred if information was tailored to their understanding of the situation53,57 “. . .sometimes I say to her [GP] ‘plain English please!. . .’ (patient with advanced cancer, p. 2164).
58
In relation to sharing information, patients expressed a preference for all clinicians, including their GP, to exchange information to ensure all team members were up to date and aware of the current plan, concerns or issues, to reduce unnecessary repeating of information:
57
They [the GP] [need] to keep up contact with my oncologist and my local community team. . . [I] have to keep repeating the things to them. . .it’s exhausting. . . (Patient with advanced cancer, p. 2164).
57
Rural patients and their family members can have long-standing and/or close relationships with their GP which strengthens the clinician-consumer relationship
Family members felt that an accessible and supportive GP could assist in problem solving and enable timely care, with comments to suggest this accessibility was enhanced by long standing and/or close relationships:
57
If I rang up and said ‘I need help today with [patient’s name],’ she [the receptionist] would just say ‘I’ve got an appointment in twenty minutes or so,’. . .In the last three weeks our GP even gave me his mobile number so that I could call him if I desperately needed him. . .He said to me ‘I don’t care what time of the day or night it is. . .’ (Spouse of patient with advanced cancer, p. 2164).
57
Rural family members suggested that their relationship with their GP stepped beyond the clinical realm, and considered them as a companion across the illness trajectory:
57
. . .[a] physician companion. . .present. . .not just a doctor that visits and prescribes pills and then goes. . . (Daughter of patient with advanced cancer, p. 2165).
57
Strategically timed access to specialist services, clinicians, and equipment is critical
This theme is comprised of two sub-analytical themes. (1) Timely access to specialist palliative care services and clinicians; and (2) timely access to equipment.
Timely access to specialist palliative care services and clinicians
Rural patients and families expressed a preference for earlier, timely involvement of specialist palliative care clinicians.52
–54,57 Rural patients and families often saw the value of specialist palliative care involvement in retrospect, recognising how specialist palliative care clinicians’ skills and expertise extended beyond that of their existing general team and/or non-palliative care specialists:51,52,54,56,57
How do people get into the palliative team in the first place? There are some people just not getting the right information at the right time. . .you will get some paediatricians who just don’t get it. . . (Parent of a child, p. 7).
52
Rural patients and their families suggested that their lack of understanding about the role of specialist palliative care services contributed to them not being linked to these services until later in their illness trajectory:52,54,58
. . .They probably stay away until someone really enters those final, final stages. . . (Family carer, p. 5).
54
In some cases, family members noted that late referrals to specialist palliative care involvement made it harder to connect with these services and wished it had been introduced much earlier:52,53,57
. . .It was a shame that they were present [in] the last few days of mom’s life . . . They should have been present earlier . . . They don’t meet us [i.e. the family] at our best, the last few days. . . (Female caregiver to a family member with advanced cancer, p. 6).
53
For these families, more timely access to specialist palliative care services enhanced their ability to proactively focus on optimising the patient’s quality of life, as opposed to being consumed by the technical aspects of managing the patients care needs:
52
And they [specialist paediatric palliative care service] were the ones that actually encouraged us to go and find memories and take photos and do all of those things to give us the confidence. So two weeks after being diagnosed with all of his new medicines and he had a nasal gastric tube, and we had all of these pumps and all of these instructions, and all of this stuff that we had to take with us but we got into a campervan . . . and we did it. . . (Parent [female], p. 10).
52
In the event a patient required specialist home-based palliative care, rural families valued prompt commencement. Yet, sometimes the process for initiating services was overly complicated and burdensome for busy carers, which added to their distress and delayed the commencement of appropriate supports:52,54
It took me six weeks to fill those forms in and find all the documents. It was just so overwhelming, that when I finally did it, they told me I’d taken too long, and I had to start again. And it was like; I’m not going to do it. It was too hard. Lo and behold, along comes this social worker who just fixed it. . . (Family carer, p. 5).
54
As travelling for specialist care is exhausting and costly for rural palliative patients and their families, most expressed a desire for access to specialist care as near as possible to home:51,54,57
Usually, the appointments were quite early in the morning, so we’d stay in a hotel the night before just so it was only 10 min away. . . (Family carer, p. 7).
54
While face-to-face care is optimal, rural patients and families welcomed the availability of virtual health care, which helped address some of their timely access issues and reduced their need to travel:51,54,57,59
“It [web-based videoconferencing] could be done on short notice. . .” (Patient, p. 3326);
59
and “. . .it hastened his care too like it helped to facilitate his change of meds [medication] and the speed at which we were able to get them. . . (Family, p. 3326).
59
Virtual healthcare promoted stronger family input and collaboration between the entire healthcare team:
59
. . .I liked it that the family was able to be there to speak with the doctor as well as the home care folks. . . (Family, p. 3325).
59
However, it was acknowledged that some types of conversation and assessments could not be performed using virtual health,
59
and at times, the setup process and the number of people involved was overwhelming:
59
It was uh. . .well it was uh. . .quite. . .intimidating in that there were so many people around and I prefer talking on a one-to-one basis . . . but at the end of the conference it was really worthwhile. . . (Patient, p. 3325).
59
While largely accepted as a platform to expedite specialist palliative care, rural patients and families voiced fears for cybersecurity:
59
. . .You know? Because you do not just 100% trust the Internet. . . (Patient, p. 3326).
59
Timely access to equipment
Family members highlighted how timely access to necessary equipment and medications supported home-based care:51
–53
They were incredibly good at the hospital [i.e. Health Care Professionals]. We had an occupational therapist who submitted applications, facilitated the house and received the equipment we needed. They contacted the municipal physical- and occupational therapist who came home, and . . . We got what we needed. . . (Female caregiver to a family member with advanced cancer, p. 7).
53
Similarly, co-operation and information sharing between the local services and family supported timely access to necessary equipment:52,53
We had to have a specific ventilator . . . when it got shipped home, they made sure that they let us know that they’ve been to the hospital, locally trained in the equipment area so, if you ever had to get to the hospital for any reason . . . they could take care of us. . . (Parent of a child, p. 8).
52
Feeling safe, prepared and supported to provide palliative care is essential
Feeling safe
Responsive home-based palliative care made rural families feel secure, while a slower-than-anticipated response time added to families’ feelings of insecurity:
53
You couldn’t ring a bell and get help when you needed to, it’s not the same with home nursing care, right? They are on their rounds and there are large geographical areas and they can’t get there so fast, so you feel much more alone. So, the insecurity with how we would get help when we needed it was- when could they come, right? (Female caregiver to a family member with advanced cancer, p. 7).
53
Family members expressed a sense of honour and duty in caring for their dying loved one, with some suggesting it was safer for them to traverse this journey in their home environment:
53
It was important to me to be with him. . . to be there, all the time. And it wasn’t hard, it was natural to be there. It was safe for me to be there with him. . . (Female caregiver to a family member with advanced cancer, p. 43).
53
However; at times, the presence of home-based care providers and equipment disrupted the calm home environment and led to feelings of insecurity,53,54 especially if visiting clinicians lacked the capacity to engage with the patient and/or family,
53
or converse with them in their language:
53
If he said something, they answered “yes” no matter if they understood or not. So, both he [i.e. the patient] and I felt terribly insecure . . . No matter what you said, you never knew if they understood what you meant. . . (Female caregiver to a family member with advanced cancer, p. 6).
53
Feeling prepared
Feeling prepared was comprised of two descriptive themes. (1) Rural patients and families expressed a need for clinicians to guide open discussions; and (2) rural patients and families voiced a preference for timely, honest information about what to expect across the illness trajectory (trajectory sign-posting).
Rural patients and families expressed a need for clinicians to guide open discussions
When seeking information, rural patients and families perceived it was their responsibility to ask the correct questions to elicit the necessary information from clinicians.53,54,57 In some cases, they feared asking direct questions about death could be perceived incorrectly:
53
I tried to hint, but I was so scared that it would be misunderstood, that he would think I would get rid of him or something, or that he would understand something else than what I really meant. . . (Female caregiver to a family member with advanced cancer, p. 5).
53
A need for timely, honest information
To be adequately prepared to manage the patient’s palliative care needs, families expressed a need for timely and honest information about what to expect across the illness trajectory, including the realities of caring for a dying person at home.53
–55 Providing rural family members with clear signposting helped to clarify the journey ahead:53
–55
We had many conversations with the doctors and nurses at the hospital before we took him home [i.e. the patient] where we could ask any questions we wanted. I felt that we got very good information about the situation and of taking him home at the end of life. . . (Female caregiver to a family member with advanced cancer, p. 6).
53
Rural family members appreciated clear, documented instructions, finding that when a patient’s wishes were documented, it empowered them to advocate to ensure care aligned with the patient’s preferences and wishes:52,55,57
I was told everything, and I was really trained up on it; and I knew exactly what to do. . .it was all written down for me to follow. . .and also we talked about not giving [patient’s name] resuscitation, anything like that. . . (Spouse of patient with advanced cancer, p. 2164).
57
To support information sharing and decision making, rural family members valued the inclusion of the wider multidisciplinary team, using case-conferencing, when planning palliative care.
55
Case conferencing was appreciated for its ability to provide space for family members to voice their feelings and concerns, and provide scope to understand different care options:
55
I think it was really useful to have a mixture of people in the room, like the GP and pharmacist and carers, because there were some elements that I wasn’t as aware of around Mum and her, how she’s been living and coping, until all of those people were in the room. Equally, a number of staff after the case conference told me that they found it really useful because they were also exposed to information that they didn’t have before, and it helped them understand some things a bit better in terms of Mum’s care (Family member of Residential Aged Care Facility resident, p. 8).
55
Feeling supported
Four sub-analytical themes are critical to feeling supported in a rural community, namely access to: (1) 24/7 after-hours support; (2) competent clinicians; (3) emotional, practical, and financial support; and (4) spiritual support.
Access to 24/7 after-hours support
Rural patients and families valued access to 24/7 support either by phone or through after-hours access to home visiting services. Access to clinicians 24-hours-a-day provided relief and reassurance to rural family members, and supported them to sustain the care the patient needed at home, while alleviating feelings of fear and isolation:52,53,56
–58,60,61
. . .As long as that lifeline was there I felt I could do it (continue caring). . . (Carer, p. 18).
61
Access to competent clinicians
Rural families voiced the need for competent clinicians, noting such access can determine where the patient will be cared for (home vs inpatient setting):52,53,55,56,58
When she [i.e. the patient] came home [i.e. from the hospital], she had to have intravenous pain relief, but the home nursing care couldn’t come to our home and administer this, so she had to go to the nursing home every day. . . (Female caregiver to a family member with advanced cancer, p. 7).
53
Rural family members described developing strong bonds with the treating clinicians,54,55,58,60,61 especially with the home-based nursing team,52,58,61 which were often founded upon the competence of the visiting nurse and the impact of their care on their loved one and wider family:52,58,61
Oh, ten out of ten. . . they [nursing staff] were. . . you could not help but actually bond with them. . . (Carer, p. 339).
58
Emotional, practical, and financial support
Rural patients and family members found informal support – be that emotional or practical, from friends, family, or an online group helpful:51,52,54,58,60
My friends found out that it was getting very hard on me and they just took over and said, ‘One of us will be there for every meal to help feed him. Set him up, feed him, get him back into position afterwards.’ If it wasn’t for them. . . (Family member, p. 6).
60
Rural family members reported feeling exhausted, and noticed changes in their relationships within and outside of their homes, which could be exacerbated by insufficient support:51,52,54,57
Well, it really put my relationship with my daughter on the back burner as well . . . She felt she couldn’t come to me with anything, for anything, because I was so worn out looking after him, she didn’t want to put any more pressure on me. . . (Family carer, p. 6).
54
To alleviate this, rural family members desired more flexible, in-home respite, which would give them some much-needed time out to attend to other matters or rest:52,54
That was one of the things that really needs to be looked at for people that are caring for the partner in the home, that need in-home respite because . . . you just don’t know what’s going to happen and when it’s going to happen. . . (Family carer, p. 6).
54
Similarly, a need for flexible access to bereavement and mental health services, was noted to be important:52,54
I think [what] would have been really good is someone to talk to about your emotional and mental state and maybe some skills around looking after yourself. . . (Family carer, p. 6).
54
Providing long term home-based care to a loved one, particularly to children with palliative care needs, can lead to long term financial disadvantage.52,53 Rural families voiced a preference for prompt financial support from government agencies:
53
They [NAV – Norwegian social security system] said that they had to have a confirmation that my husband really was so sick . . . It wasn’t unfamiliar that he was sick, within the NAV– system, but this is the way it is. I haven’t heard from NAV since. They wait until they don’t have to pay. That’s what happens. . . (Female caregiver to a family member with advanced cancer, p. 7)
53
Spiritual support
Rural patients reported feeling supported through their spiritual beliefs:
51
. . .I think I’m a deeply spiritual person and that helps me get through those moments where I’m feeling down. . . (Advanced cancer patient, p. 50).
51
Discussion
Having privileged the patient and family voice, this meta-synthesis has revealed three key elements that rural patients with palliative care needs and their families consider to be critical to them receiving the support and care required. Their GPs input, encompassing both the physician-patient relationship and their role in care planning and care delivery; along with strategically timed access to specialist clinicians and necessary equipment; and the presence of various processes and people who ensure patients and families feel safe, prepared and supported across their illness trajectory, are all perceived as being critical to rural patients staying within their communities. While these preferences are similar to people with palliative or end of life care needs in other locations, the uniqueness of the rural environment is highlighted. Given that in many rural communities, the GP holds a central and critical community role, it is not surprising that their input is highly valued and essential to dying an expected death in a rural community, and their long-term relationship and involvement with the patients needs to be honoured and leveraged. Similarly, these rural patients want to be linked into timely care provided by specialist palliative care providers and have access to equipment to enable them to spend more days within their community. Finally, the concept of feeling safe is also not surprising, given that many rural patients and their carers are managing complex end of life symptoms and situations at home and so naturally want to feel safe.
Addressing the increasing demand for access to quality palliative care requires innovative change to meet this need commensurate with an ageing global rural population.2,13,14,63,64 Our findings reinforce the importance of GP-led multidisciplinary rural palliative care models, with strategically timed input from specialist palliative care clinicians, inclusive of complex care planning and trajectory signposting. Such an approach is synonymous with a population-based approach to care. 65 Research from predominantly urban areas has detailed how general practitioners are considered well placed to provide primary or generalist palliative care due to their: relationships with patients and families; ability to coordinate healthcare resources and service providers; breadth of clinical responsibility; and capacity to visit patients at home. 66 Similarly, qualitative interviewing with mostly urban GPs (n = 11) and specialist palliative care clinicians (n = 10) exploring the role of GPs in the planning and provision of palliative and end of life care, identified several key roles including: performing care planning; timely referral to palliative care services; and being the lead primary care clinician in charge of patient care. 67 Importantly, a GP-led multidisciplinary rural palliative care model can be augmented by virtual care (e.g., telehealth or videoconferencing), specifically for its capacity to connect GPs with specialist palliative care clinicians.25,26,29,34,35 Solutions to ensure GPs can successfully lead primary palliative care relies on commitment by local, state and federal levels of government 68 to address known gaps 69 such as strengthening care coordination and team-based planning practices; 69 time restraints and workload; 69 and the palliative care capabilities of generalist workforces. 69 Policy supporting integrated primary and specialist palliative care has been postulated since 1990 70 and more recently by the public health strategy for palliative care, 71 yet gaps applying a population-based approach to care continue to exist. Despite our findings demonstrating the need to strengthen palliative care service integration in rural settings, this must be balanced against rural GP workforce projections which outline current and future shortages related to a lower supply of GPs relative to community demand, and a lowering of average hours worked. 72 Finding solutions to increasing the availability of GPs in rural areas is a complex and ongoing issue. Any innovative primary care intervention, be that virtual or otherwise, must be flexible, responsive, tailored to local rural circumstances, consider the roles and capacities of the broader health workforce, and capture usable data to drive service development and policy. 73
Despite reduced access to specialist palliative care clinicians and services in rural communities, 12 this meta-synthesis has affirmed that rural people view specialist palliative care clinicians as integral to their care, but not necessarily on an ongoing basis. Identifying cost-effective methods of connecting rural clinicians and specialist services is critical to addressing these populations’ palliative care needs. Identifying the timing, indictors or frequency as to when to include specialist palliative care clinicians to assist with complex care planning and trajectory signposting for this specific population requires further exploration.
Our findings highlight the role of virtual technology in connecting rural people with specialist palliative care clinicians for its ability to: improve the timeliness of care; reduce the need for travel; and at times, be performed in one’s own home, offering comfort and added convenience. While virtual technology augmented with face-to-face care shows promising results,74 –76 data on usability and acceptability in rural populations requires further evaluation. 77 Importantly, serious gaps exist in internet and telecommunication infrastructure in rural and remote areas, with many telecommunication ‘black spots’ 78 needing to be addressed to fully operationalise this model. 44 Ensuring dependable telecommunication infrastructure and devising strategies for an ageing rural population is imperative, but such advancements require significant government funding and supportive policy for this to be realised.
Importantly, this meta-synthesis contributes to the emerging field of safety and security in patients and families in receipt of rural palliative care.37,79 –81 Emerging evidence suggests that feeling safe impacts a patient and family’s decisions about their location of care and death.82,83 Aspects of care which support a sense of safety and security include: trust in the competence of clinicians;82,84 timely availability of home visiting clinicians to assist with care needs;37,82 impeccable symptom management; 82 being able to contact the team when required, inclusive of 24/7 support; 82 honouring patient agency and autonomy;37,79,82 and access to support and respite for family members when overwhelmed. 82 Our findings add to this evidence, revealing that a sense of safety and security is critical for rural palliative care patients and their families to remain at home for as long as possible.
Access to 24/7 support and advice outside of normal business hours aims to assist with the provision of high quality palliative care, and reduce the burden on caregivers and clinicians during stressful and unfamiliar situations. 85 Implementing wide-spread access to 24/7 support for rural patients and their families requires innovation, such as networked models and funding, to overcome known service-related, clinician-related, and patient-related challenges. 86 While some rural communities will have existing resources to develop an after-hours support service, others may need to collaborate with larger regional or metropolitan-based services to deliver this element. Regardless, prioritising government policy and funding support are essential to developing this capacity in rural communities.
Implications for future research
There is already strong support for GP-led rural palliative care models receiving oversight from specialist palliative care clinicians. An Australian quasi-experimental study 34 comparing usual care with a GP registrar-led model receiving specialist palliative care physician input, using patient assessment, case-conferencing and care planning improved care outcomes. In this study, the control group was twice as likely to be admitted to the hospital, twice as likely to have ⩾two hospital admissions, and less likely to die at home (preferred location) compared to the intervention group. 34 Similarly, a pre-test post-test case series evaluating the impact of a single case conference to plan palliative care for people with end-stage heart failure and lung disease involving GPs, chronic disease specialist nurses, and a specialist palliative care physician 29 reduced: emergency department (ED) admissions, ED admissions leading to discharge, hospital admissions, and length of stay, 29 and demonstrated average cost savings of AUD$41,023/person. 25 However, establishing a GP-led rural palliative care model depends upon universal health coverage; 87 access to specialist palliative care clinicians; access to virtual health technology; 24/7 after-hours support; and adequate drug availability. 71 Realising this model in any rural setting requires dedicated policy, targeted funding, and innovative solutions to address workforce challenges.
The evidence identified in this review supports the use of virtual health technology, to enable locally based rural palliative care to have the strategic input of the nearest specialist palliative care team. A recent Australian prospective mixed-method pilot study, 26 evaluated the inclusion of a metropolitan-based specialist palliative care physician telehealth appointment alongside a rural home care visiting nurse appointment, resulting in the intervention group having: less functional decline at 2 weeks and 3 months; fewer GP and community palliative-care nursing visits; and fewer hospital admissions 30 days before death compared to the control group in receipt of home care visiting nurse appointments without telehealth support. 26 Similarly, a longitudinal paediatric palliative care telehealth support pilot study, 35 where specialist palliative care clinicians provided support to local rural clinicians, noted a non-significant improvement in family functioning, with all children (n = 11) dying in their preferred location (home). 35 As these study designs were open to bias, confirming these preliminary findings in an adequately powered RCT design is important before being integrated into policy and translated into practice.
Finally, this study’s contributes to the emerging field of safety and security for patients and families receiving rural palliative care.37,79 –81 Key areas that may impact these feelings include complex care planning, trajectory signposting, and community support. Despite the emergence of community awareness programs88 –91 (e.g. compassionate communities), better understanding their impact on rural patients and their families’ perceptions of feeling safe, supported, and secure requires further research.
Strengths and limitations
This study’s completeness, accuracy and transparency was strengthened by adhering to the PRISMA guidelines. 40 Using rigorous consensus and author reflexivity increased trustworthiness. Similarly, the choice to only extract data from the highest quality studies, as determined by the Walsh and Downe 50 appraisal tool, increased rigour. Choosing raw published quotes as opposed to the full published results of included studies raises the likelihood our findings reflect the perceptions of rural palliative care consumers. However, an inability to consider the complete interview transcripts of each study raises subjectivity. Several included studies focused on specific elements of care, such as telehealth and case conferencing, which may skew the findings. This is balanced by data generated by other included studies which did not have such a specific focus. There is more available data from carers than patients. This speaks to the vulnerability of this population, and is a gap in the literature. This review sought and analysed data from studies published in English only, which might result in selection bias. All studies were performed in countries with universal healthcare coverage, and no studies exist from remote areas, altering the generalisability of our findings. The authors have performed a systematic review 36 examining the key elements of rural palliative care models from a quantitative perspective, providing scope for further analysis and representation of this underserved population.
Conclusion
Despite the gaps in access to and quality of rural palliative care, privileging patient and family voices to identify the best approach to care provides valuable insights. Our findings confirm current population-based models of palliative care, which advocate for the strategic inclusion of specialist palliative care clinicians alongside primary care providers to optimise care for rural patients with palliative care needs. Central to delivering quality rural palliative care is the GP, the conduit to specialist palliative care services and who plays a significant role in ensuring rural palliative care patients and their families feel safe and well cared for. Ensuring access to and viability of GP-led, specialist-supported, rural palliative care models, including telehealth access, complex care planning, and 24/7 after-hours support, requires commitment from all levels of government, positive public policy, adequate funding, innovative workforce strategies, and robust evaluation.
Footnotes
Appendix
Database Search Terms.
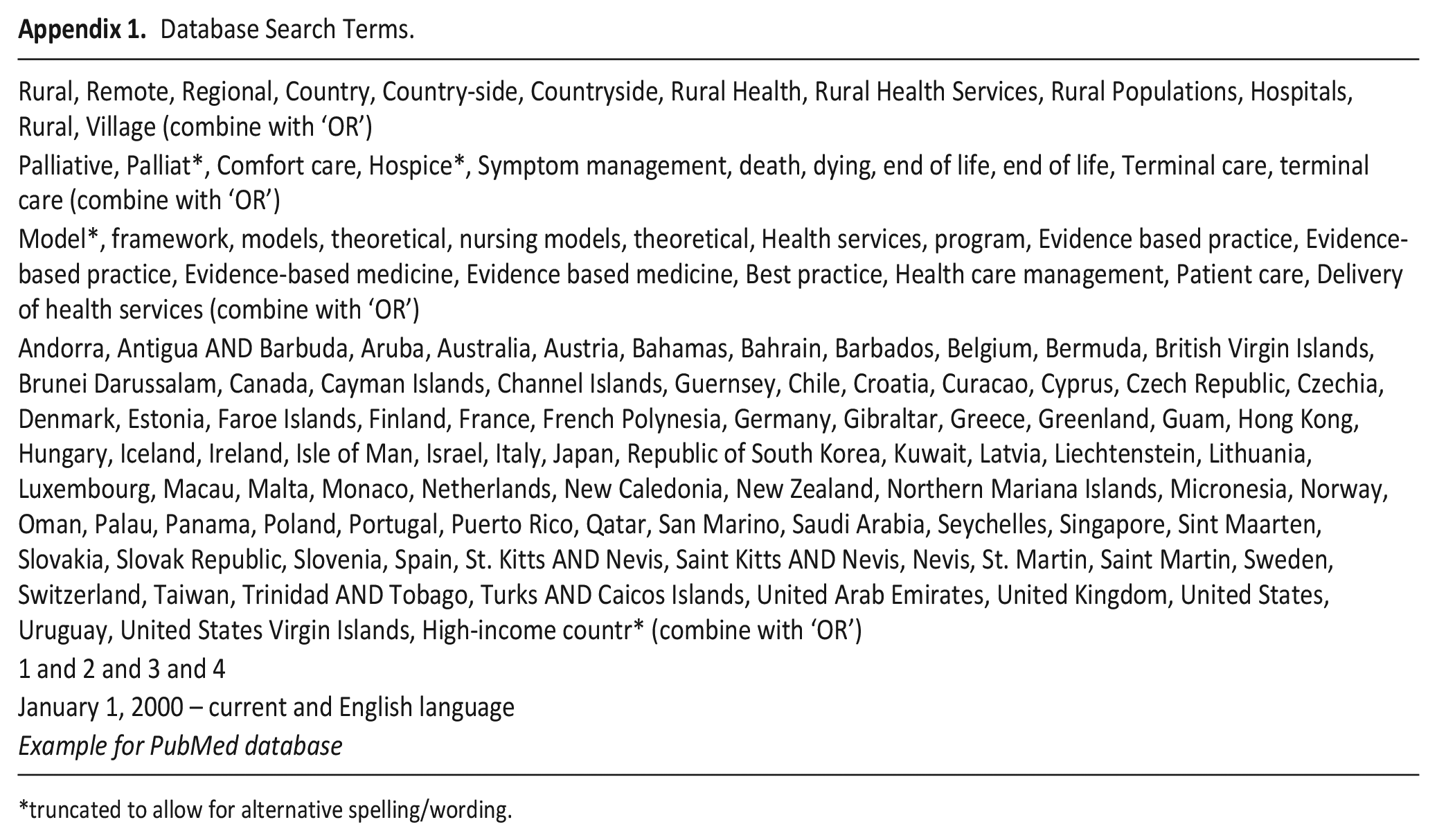
| Rural, Remote, Regional, Country, Country-side, Countryside, Rural Health, Rural Health Services, Rural Populations, Hospitals, Rural, Village (combine with ‘OR’) |
| Palliative, Palliat*, Comfort care, Hospice*, Symptom management, death, dying, end of life, end of life, Terminal care, terminal care (combine with ‘OR’) |
| Model*, framework, models, theoretical, nursing models, theoretical, Health services, program, Evidence based practice, Evidence-based practice, Evidence-based medicine, Evidence based medicine, Best practice, Health care management, Patient care, Delivery of health services (combine with ‘OR’) |
| Andorra, Antigua AND Barbuda, Aruba, Australia, Austria, Bahamas, Bahrain, Barbados, Belgium, Bermuda, British Virgin Islands, Brunei Darussalam, Canada, Cayman Islands, Channel Islands, Guernsey, Chile, Croatia, Curacao, Cyprus, Czech Republic, Czechia, Denmark, Estonia, Faroe Islands, Finland, France, French Polynesia, Germany, Gibraltar, Greece, Greenland, Guam, Hong Kong, Hungary, Iceland, Ireland, Isle of Man, Israel, Italy, Japan, Republic of South Korea, Kuwait, Latvia, Liechtenstein, Lithuania, Luxembourg, Macau, Malta, Monaco, Netherlands, New Caledonia, New Zealand, Northern Mariana Islands, Micronesia, Norway, Oman, Palau, Panama, Poland, Portugal, Puerto Rico, Qatar, San Marino, Saudi Arabia, Seychelles, Singapore, Sint Maarten, Slovakia, Slovak Republic, Slovenia, Spain, St. Kitts AND Nevis, Saint Kitts AND Nevis, Nevis, St. Martin, Saint Martin, Sweden, Switzerland, Taiwan, Trinidad AND Tobago, Turks AND Caicos Islands, United Arab Emirates, United Kingdom, United States, Uruguay, United States Virgin Islands, High-income countr* (combine with ‘OR’) |
| 1 and 2 and 3 and 4 |
| January 1, 2000 – current and English language |
| Example for PubMed database |
truncated to allow for alternative spelling/wording.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CM is a scholarship supported PhD. student.