
Abstract
Background:
Every advanced cancer diagnosis brings enormous challenges to patients and their relatives on numerous levels: be it physical, practical, social challenges, or on a more personal level. While specific aspects have been researched before, an overarching approach is lacking.
Aim:
To understand the lived experiences of people with advanced cancer, to identify gaps along the cancer care continuum, to identify potential opportunities for meaningful interventions and to develop a theoretical framework for practitioners and researchers.
Design:
A qualitative study using in-depth interviews with patients, relatives, and care professionals. Interviews were transcribed verbatim and analysed using a conventional content analysis.
Setting/participants:
Fifty-four interviews with 17 patients from a university oncology department and palliative care service, 15 relatives and 22 care professionals from physicians to funeral directors. All interviewees were recruited by a German university hospital.
Results:
We developed a novel model describing the diagnosis with advanced cancer as a highly disruptive experience that threatens to challenge the integrity of personhood in cancer patients through four areas: communication, knowledge, relationships, and confidence. We were able to identify factors leading to disintegration in these areas and factors supporting a restoration of integrity of personhood.
Conclusions:
The developed model provides a more thorough understanding of patients lived experiences. It can help to develop new interventions along the cancer care continuum to support patients in the complex challenges they face. These interventions should focus on supporting the integrity of personhood.
Keywords
Key Statement
Being diagnosed with advanced cancer is a highly disruptive experience with an often underestimated psychosocial cost.
It brings enormous practical, social, financial, psychological, and existential challenges for patients and their caregivers.
The complex interactions and cumulated effects of these challenges on the patients self experience are not well understood.
We developed a model that focuses on the integrity of personhood as a cohesive experience of the self.
We identify four areas that threaten this integrity of personhood in patients living with advanced cancer: communication, knowledge, relationships, and confidence.
We show ways to help patients restore the integrity of their personhood, for example, by improved communication and knowledge transfer, by including relatives and by effective symptom control and psychosocial support.
Interventions should address the restoration of the integrity of personhood in cancer patients.
We need more creative, transdisciplinary, and innovative interventions to be found, implemented and evaluated.
These interventions should be searched for, implanted and evaluated along the whole cancer care continuum.
Introduction
Being diagnosed with cancer, especially if in an advanced stage, brings enormous challenges on numerous levels: next to the therapeutic decision-making process, hospitalisation and impairments, there are significant challenges on an emotional, psychological, social, and spiritual level.1 –3 Palliative care specialists try to address these with outpatient and inpatient care.
The psychosocial impact affects patients,4 –6 but also their relatives and caregivers.7 –11 An Italian study found that 19% of patients with terminal cancer suffered from dignity-related existential distress. 12 A grounded-theory study among lung cancer patients showed the importance of social aspects of dying and how patients tried to maintain integrity by acting as normal as possible. 13 Others have looked on the impact of the disease on the self-identity of patients14 –16 and on the traumatic effects of such a diagnosis.17,18 A systematic review identified four central unmet needs for people with advanced cancer: 19 information deficits, preoccupation with worries and uncertainties, fatigue and pain management, and loss of functioning.
A systematic review demonstrated how the navigation of continued loss and the acknowledgement of terminal illness shaped the self-identity. 20 This process was modulated by personalised knowledge and by negotiating personal and healthcare relationships. Other studies have described the impact of terminal illness on the patients identity14,21,22 and identified opportunities for psychotherapeutic interventions. 23
In the fields of anthropology, sociology and philosophy, various theories exist to understand the life-changing consequences of a terminal illness and the existential distress involved. A recent ethnography of palliative care services described the core challenge as aligning two repertoires of practice: 24 caring for human life and supporting personhood. Navigating this assemblage of the two repertoires and especially developing meaningful interventions remains a major challenge for palliative care today. Therefore, it is important to gain a deeper understanding of how these repertoires take effect in the lived experiences of patients, their relatives, and caretakers as well as professional healthcare workers and other disciplines involved in dealing with people with advanced cancer. This study uses a transdisciplinary, explorative approach, triangulating patient, relatives, and professional caregiver perspectives to gain a better understanding of the processes and challenges along the care continuum and to identify potential interventions. We aim to synthesise these findings in a way relevant to practitioners and researchers along the whole cancer care continuum.
Methods
Methodology
Living with an advanced cancer diagnosis is a complex and highly subjective experience. We were interested in exactly this experience and the interaction with family members, healthcare professionals, and other care providers. To account for the assemblage of subjective perspectives, institutional frameworks, and challenges in day-to-day life, we opted for an explorative qualitative research design based on a post-positivist epistemology and a critical realist ontology. This reflects the transdisciplinary nature of the research team and our objective to develop insights into the social realities to inform interventions within the care continuum. Our methodology can be best summarized as a conventional approach to content analysis: 25 building on an inductive category development, we incorporated abductive elements at a later stage and a deductive re-evaluation after model development.
The research question and design were developed by a transdisciplinary research group consisting of experts from the field of oncology, palliative care, nursing, psychotherapy, psychology, public health, theology, and others. A study nurse and two research students with prior training in qualitative interview technique conducted the interviews. Psychologists, physicians, and a public health researcher conducted the analysis process.
Ethical approval was granted from the ethics committee for human research at Philipps-University Marburg (reference number 73/22).
Setting
This study was conducted by an interdisciplinary cooperation between departments of clinical psychology, medical ethics, and oncology at a university hospital in Germany. The oncology department provides an interdisciplinary ambulant chemotherapy unit, several inpatient wards, and a palliative care unit, treating patients with a wide spectrum of malignancies.
Population
Interviewees were recruited from patients and from accompanying caregivers of the oncology department during routine visits. Inclusion criteria were an advanced cancer diagnosis, age above 18 years, fluency in German and the mental and physical capability for an in-depth interview. We intentionally included patients with a diverse range of cancers. An advanced cancer diagnosis was defined as being diagnosed with a non-curative cancer and a negative surprise question. As the distinction between life-prolonging and symptom-controlling chemotherapy was not always clear, we did not follow the strict definition of advanced versus terminal cancer, 26 but extended the criteria by the surprise question answered by an experienced oncology consultant. 27 The oncology consultant preselected patients that met the inclusion criteria. All patients had been made aware of their advanced cancer diagnosis by their oncologist independent of and before inclusion. Relatives and caretakers were included independent of patients. Hence, they were not necessarily the care takers of patients included in our study. We did especially no dyadic sampling or analysis. Care professionals were recruited through announcement via mailing-lists of professional networks in Germany.
Sampling
We used a purposive sampling strategy with theoretical variation. 29 To triangulate participant perspectives, we recruited (1) people living with advanced cancer, (2) relatives and caretakers and (3) care professionals, that is physicians, nurses, occupational, and physiotherapists, but also counsellors, chaplains, and funeral directors. Within these groups, we aimed for a maximum contrast, according to predefined categories as developed by the transdisciplinary research group: age, gender, education, religious affiliation, ethnic background, and cancer diagnosis. Based on prior experience, existing research, and expert advice we expected to need 15–20 interviews per group to account for the diverse experiences of people living with advanced cancer. 28
Recruitment
Participants for the first two groups were recruited from the interdisciplinary ambulant chemotherapy unit and the palliative care unit of a German university hospital. They were approached face-to-face after clinical appointments or—if inpatients—on the ward by an oncologist.
Data collection
We developed a semi-structured interview-guide based on guidance from the expert group and an extensive literature research. We used a narrative start into the interview, asking participants to tell us about their experience with an advanced cancer diagnosis. We then followed up with clarifying questions and toward the end more specific questions on the information and support they had or thought they should have had. Interview guides were formulated for patients, relatives, and care professionals, respectively.
After explanation of the study goal and setting, participants gave their verbal and written consent. Care professionals were recruited through professional networks in Germany via e-mail. They gave their written consent in advance and verbal consent at the start of the interview. Most of the interviews were conducted in a counselling office at the university hospital. Some of the interviews with care professionals were conducted through an online video conference-tool. All interviews were audio-recorded and transcribed verbatim. All information allowing for identification was removed from the transcripts.
Data analysis
The overall analysis process fits best under the category of conventional content analysis. 25 It encompasses elements of an inductive category development typical for a thematic content analysis as introduced by Mayring29,30 but also abductive elements in the model generation 31 and deductive workflows at a later stage of work applying our findings from the first two steps. Even though this analysis process shares some similarities with Grounded Theory methodology, 32 it does neither share the epistemological assumptions, nor does it follow its strictly iterative design. After collection, transcription and pseudonymisation of all interviews, a third of the interviews in every group were coded inductively and an initial category system was built by identifying overarching themes. Coding and analysis was conducted in MAXQDA. 33 During the coding process regular meetings were held to discuss findings, ambivalences and to check for traceability. This code system was then further refined and used for the remaining interviews, while being open to new codes and shifting categories during the coding process. Early results on a descriptive level were presented to the transdisciplinary research group and feedback, especially on traceability and comprehensiveness incorporated. These results were then further analysed and relationships between the themes identified. From there we developed initial models, contrasting the experiences of patients, relatives, and care professionals. Out of these models the final integrating model was postulated. This postulated model was then used to analyse the data again with a deductive approach to check for coherence with the data and to further refine the model categories. Throughout the analysis process, we utilised the transdisciplinary working group to bring together different perspectives and background knowledge to allow for a high level of reflexivity within the research team and to create a more transparent process for the model generation. Extensive memo writing during the coding and analysis process, regular team meetings and triangulation of data and researchers were deployed to enhance traceability and trustworthiness of the research results. 34
Results
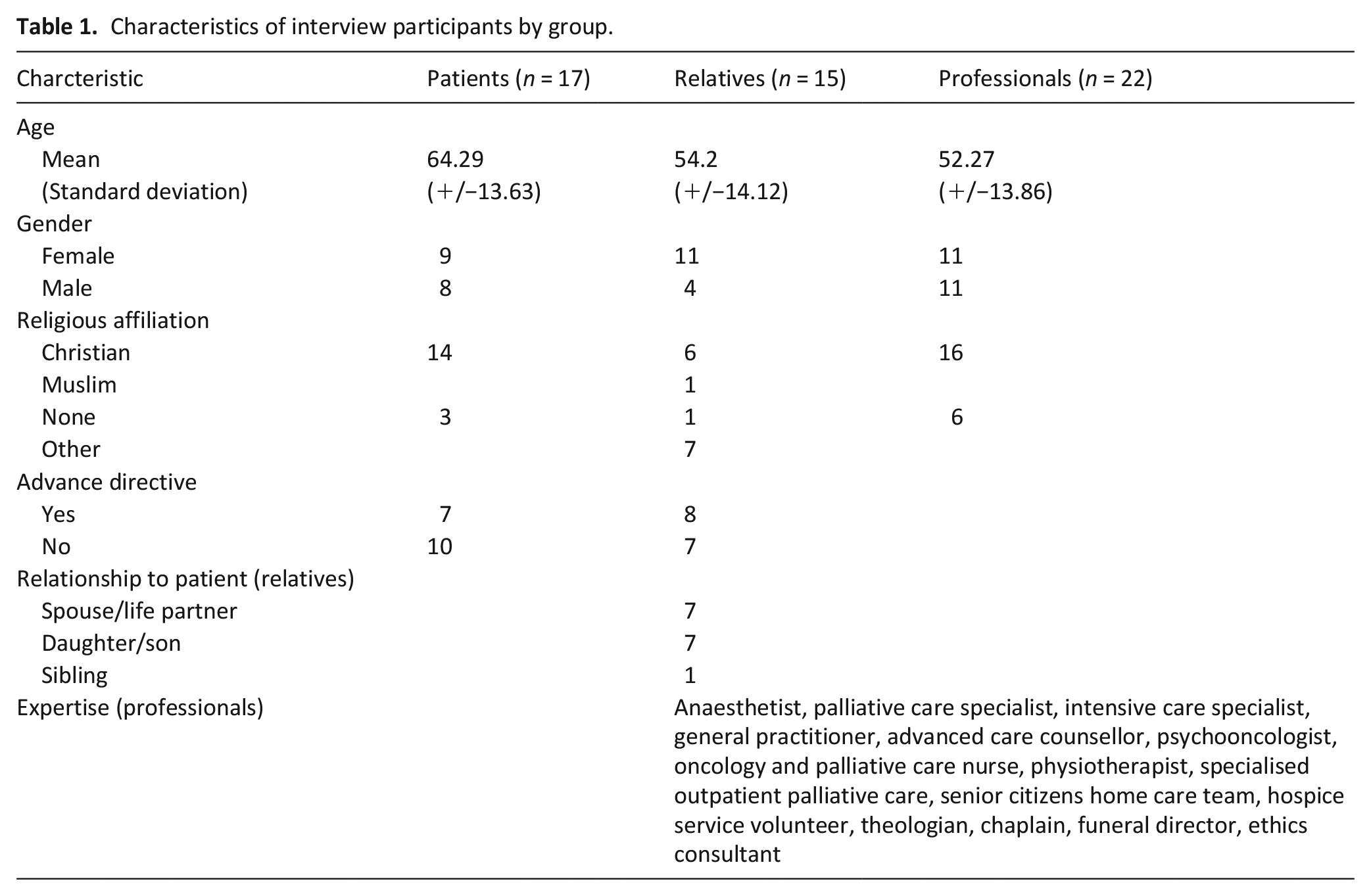
From September to November 2022 a total of 54 interviews with 16 patients, 15 relatives, and 23 care professionals were conducted. Interviews lasted between 15 and 75 min. Further characterisation of the participants can be found in Table 1.
Characteristics of interview participants by group.
Descriptive analysis
The interviews with patients and their relatives touched on a vast array of topics—often triggered by the emotional burden of a cancer diagnosis. Experts talked primarily about what they deemed important for patients and relatives they interacted with, and what challenges they perceived. Overall, several recurring topic clusters could be identified: disease & therapy, structures of care, advance planning, psychological condition, dying, existential issues, and communication & relationships. To gain a better overview of the issues mentioned in the interviews, we sorted them by their significance for the different stakeholders within the cancer care continuum. 35 This overview shows how nearly every aspect is relevant for the patient, relatives, and the healthcare system and how all of them need to be aware of the issues and ought to address them (Figure 1).
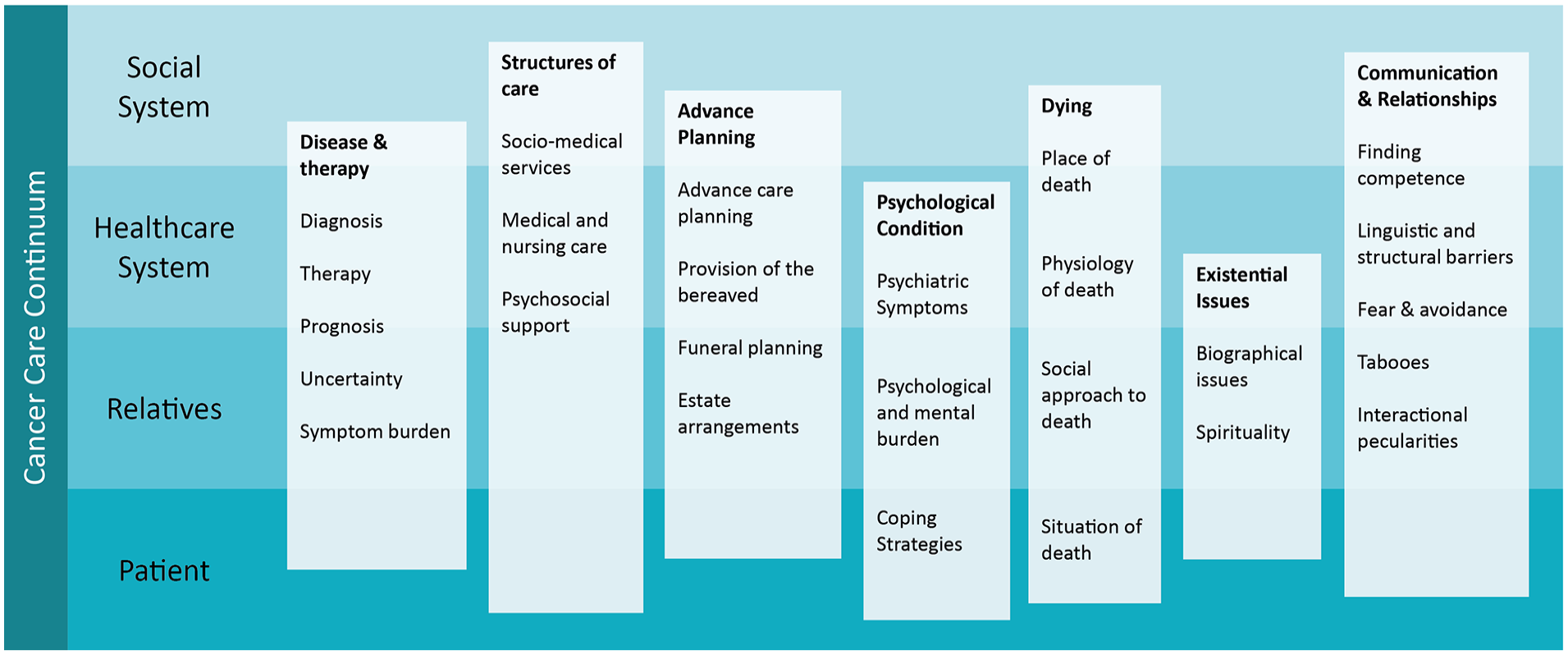
Topics within the interviews, categorised by relevance to cancer care continuum. Subitems have been listed but not specifically linked to one stakeholder within the continuum for better visual clarity. Cancer care continuum simplified from Taplin SH, Anhang Price R, Edwards HM, et al. Introduction: Understanding and influencing multilevel factors across the cancer care continuum. J Natl Cancer Inst Monogr. 2012;2012(44):2-10. doi:10.1093/jncimonographs/lgs008.
Our data and analysis do not allow for a quantitative triangularisation of patients, relatives and experts, but the data reveals large overlaps in the general topics mentioned, though with different focuses. Experts stressed the need for more patient information, while patients and relatives focussed on the style of communication, especially with healthcare professionals. Relatives were especially interested in practical advice and support. They were much more worried about the financial and care situation than patients, while patients stressed the need for trust and transparency. Overall, we found a surprisingly good agreement between the groups.
Advanced cancer as disruption
After this initial, mostly descriptive, overview we aimed for a better understanding of the patient’s experiences living with advanced cancer. Patients, relatives, and professionals all agreed on what a challenge advanced cancer poses and how many changes it brings. One of the patients described it like this: “Receiving the diagnosis is just a short moment. It takes some time to realise, but then it pulls out the rug from under you. And [pausing] it really makes your stomach turn.” (P9:39)
Another remembered: “It was quite confusing. It took a bit of time for the chaos to calm down and for things to be sorted. [. . .] I could not think ahead, could not plan my tomorrow. I had never experienced anything like that before.” (P3:33–35). A palliative care specialist talked about the “major disruption” (E9:11) patients experienced due to the advanced cancer diagnosis.
We therefore looked specifically for the ways this disruption became immanent in the lived experiences of people with advanced cancer. We identified four areas: communication, knowledge, relationships, and confidence (Figure 2).
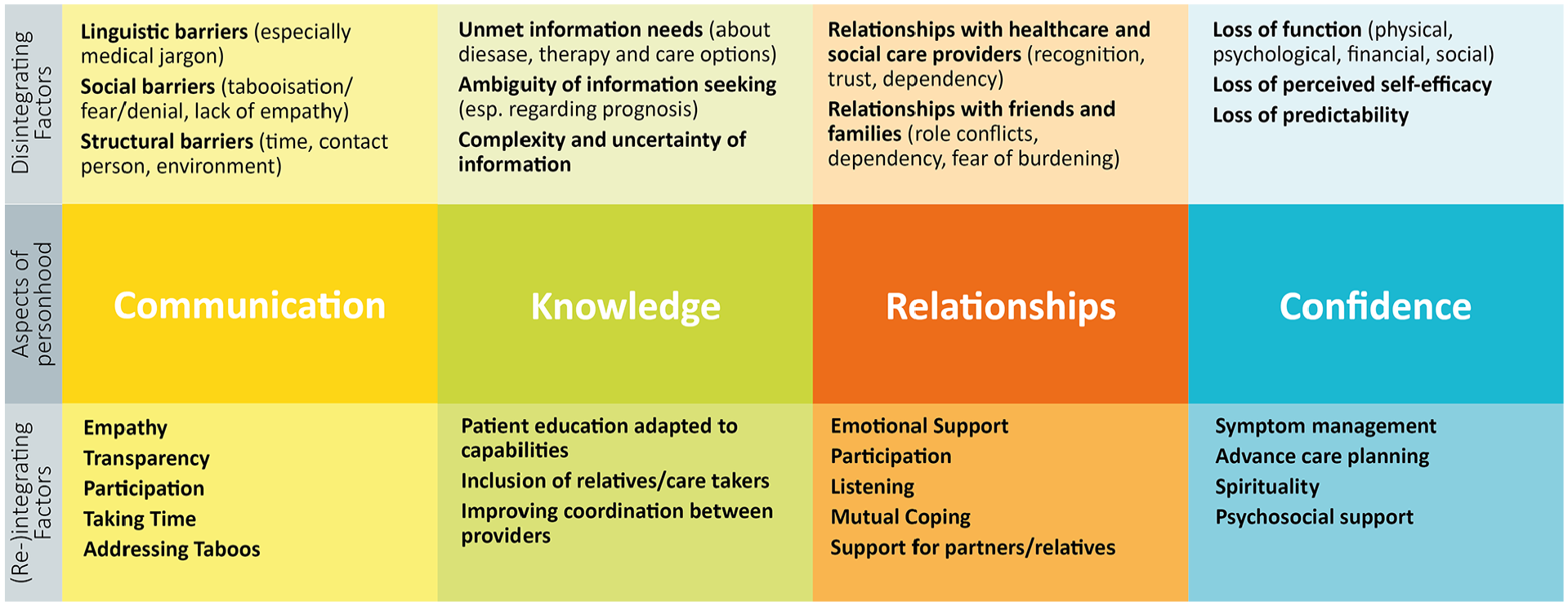
Areas that are disrupted by an advanced cancer diagnosis. The upper row displays barriers in these areas, while the lower row suggests possible interventions.
A cancer diagnosis challenges a patients day-to-day
This is closely related to the second area,
The third area deals with the challenges within
The fourth area deals with the challenged
A threat to the integrity of personhood
While analysing the interviews, it became evident that the areas presented above are highly interdependent and can ultimately result in a feeling for the patients to “not be themselves anymore.” One of the experts said: “When people go home with their cancer diagnosis [. . .]they need to find their orientation toward themselves again.” (E20:92–93) Communication, knowledge, relationships, and confidence affect the whole person and threaten her integrity of personhood (Figure 3): A definition of the entity “personhood” would go beyond this paper and would not be covered by our data. But we can describe the ramifications of advanced cancer on the integrity of this personhood. “Integrity of personhood” describes the cohesive experience of the complex compound personhood most probably signifies: components like self-perception, social roles, personal value systems and orientations, identity—in short that which makes a human being a human being. Even though cancer might not challenge the whole personhood, it challenges the integrity or cohesiveness of its various components. This reintegration becomes one of the key tasks for patients and consequently, their caregivers to support them in this process.
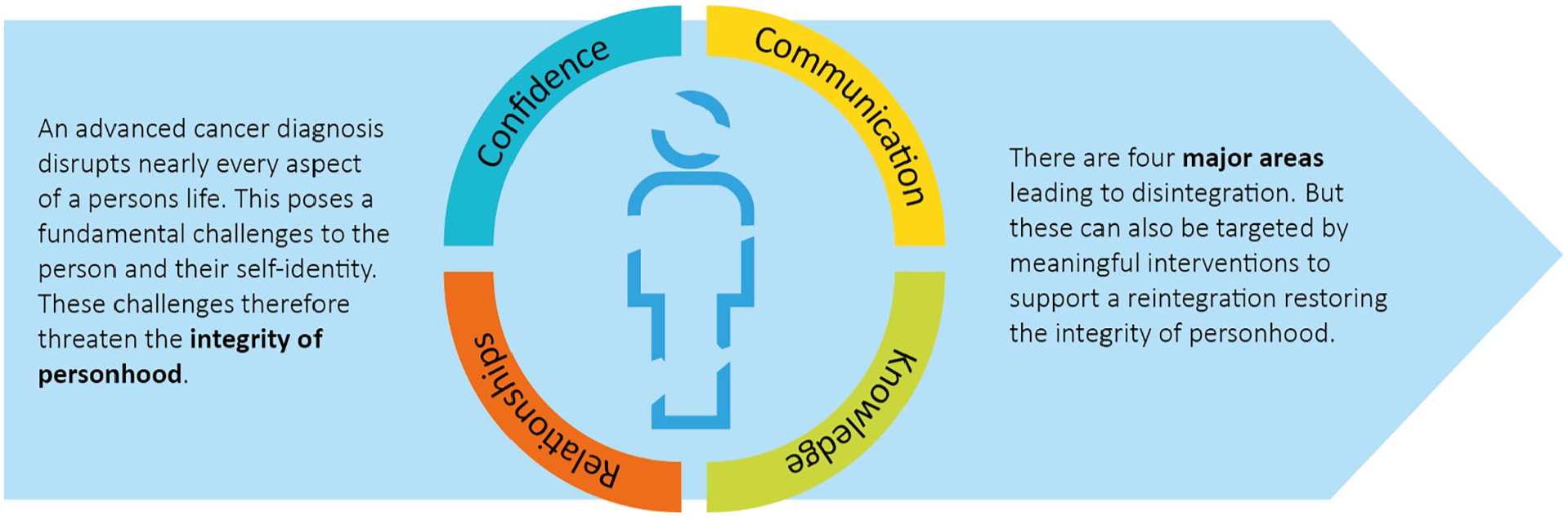
Advanced cancer as a threat to the integrity of personhood. Challenges in the area of communication, knowledge, relationships, and confidence lead to a less cohesive experience of the self.
Supporting the restoration of the integrity of personhood
From the interview data, it was not just possible to elucidate the challenges and disintegrating factors, but also to identify pathways to support patients to restore the integrity of their personhood. A relative mentioned: “Well, where to get help—be it spiritual or psychological—but also financial support or with administration issues.” (R21:111). A patient reported how he had wished, physicians had included his relatives in conversations: “For me it would have been much easier, if someone had talked to [my family members] or if someone would do that and explain to them what is happening. [. . .] That would really help me.” (P4:218–220). These suggestions were checked against existing clinical evidence and supplemented where needed. We sorted these factors by the four areas as before (see Figure 2). Targeted effective support from the whole cancer care continuum can help patients navigate the challenges of their advanced cancer diagnosis and help them to restore the integrity of their personhood. This is exemplified in Figure 4 showing meaningful interventions to address the four areas that threaten the integrity of personhood and to help patients restoring their integrity of personhood.

Meaningful interventions in the areas of communication, knowledge, relationships, and confidence can help in restoring the integrity of personhood for patients living with advanced cancer.
Discussion
Main findings
This qualitative study conducted 54 interviews with patients, relatives, and care professionals to gain a better understanding of living with advanced cancer and to identify support potential. The diagnosis of an advanced cancer disease was described as a life-changing, disrupting experience. We identified four areas, which were seen as especially challenging: communication, knowledge, relationships, and confidence. We showed how these areas are interdependent and how they threaten the integrity of personhood. We then, deductively, demonstrated interventions along the cancer care continuum to support patients in restoring the integrity of their personhood.
Explorative analysis of advanced cancer experience
Over the past decade a number of studies have explored the perspectives of patients living with cancer and their subjective needs6,7,13,36 –39 To our knowledge this is the first study using a triangulated approach including relatives and care professionals from a variety of backgrounds to get a better understanding of patients living with advanced cancer. The variety and diversity of interviewees and research team have helped to widen our perspective and to see the issues along the whole care continuum, but also the diversity of issues patients face.
Advanced cancer as disruption
Our findings do align with previous research on the disrupting effect of a cancer diagnosis. Though not framed through the lens of the integrity of personhood, elsewhere the psychosocial burden of cancer has been clustered around four domains: the physical, the psychological, the social and the spiritual domain. 40 A recent Grounded Theory study analysing value statements in medical records framed the cancer experience as disruption to the individual, interpersonal and social identity, threatening a meaningful and fulfilled life. 41 Especially in the fields of sociology and anthropology there is a long history describing the impact of chronic and also terminal illness on the identity.42 –44 This research comes from various disciplines and epistemological stances, for example, positivism 45 , narrative and phenomenological approaches14,46,47 constructionist 43 , and constructivist48 –50 approaches. While they agree on the impact cancer has on the patients, it becomes clear that concepts like person, self and identity are far from being indisputable. It also becomes clear, that the concept of personhood cannot be understood from just one perspective or a single discipline and is rather a highly complex compound of psychological, social, moral, metaphysical, and bodily aspects. To avoid some of the dilemmas arising from a too narrow definition of personhood, we proposed to focus on the integrity of personhood. Morse wrote about chronic illness as threat to the integrity of the self. 46 Eric Cassell is probably the most prominent researcher pointing to the relationship of suffering and personhood.51,52 He shed light on two important aspects: the diverse character of suffering and the wholistic understanding of being a person with a soul and a body and how that should impact clinical care. So far, our research is in broad agreement with his findings. However, there are two important distinctions: In our data patients did not use the term “suffering” to subsume the numerous effects of their illness, but rather “challenge” or “shock.” By focusing on the disruption instead of suffering we also avoid some of the philosophical challenges of defining suffering without precluding that suffering is not a central phenomenon within or due to the disintegration. 53 We use the term personhood—similar to Cassell—to express, that the disruption does not just happen on a personal (i.e. psychological) level, but includes social and medical aspects as well. But we do describe the disruption as a threat to the integrity of personhood and not as a threat to the person itself. This has primarily ontological reasons, emphasising the persistent existence of the person even in the face of an illness that threatens the integrity of personhood. Cohn et al distinguished between “human being” and “personhood” in their ethnography of palliative care services to describe the medical and non-medical aspects, but also clarified that it is actually an assemblage of both in most situations. 24 In our paper, we subsume the medical aspects (human being) under personhood believing them to be indeed inseparable: biomedical interventions like symptom management are categorised under “confidence,” being the area most closely linked to traditional aspects of identity and the self. Focussing on the integrity of personhood emphasises the interaction of the different aspects of personhood, the intrinsic coping mechanisms, and the patient as a whole individual.
Implications for the cancer care continuum
Our research shows the manifold challenges for patients with advanced cancer and the need for a transdisciplinary solution to support them in this situation. It confirms the need to look beyond the individual to understand the complex relational network from relatives to healthcare professionals. While there are effective interventions to address individual issues,54 –59 and also interventions along the care continuum,60 –64 more interventions are needed that empower and enable patients to navigate the care continuum and that focus on the integrity of personhood of people living with advanced cancer. Our model can serve as a framework for practitioners, explaining underlying mechanisms, improving awareness for wholistic needs, and showing concrete ways to better support terminally ill patients. This framework highlights the practical implications while presenting the complex psychological or philosophical theories underneath in a relevant and applicable manner to practitioners from all professions.
Implications for research
Our study brings together findings from the social sciences, psychology, and medical and palliative care. We suggest two directions for further research: on the one hand, foundational research to better understand the underlying mechanisms and relationships between the disintegrating factors of personhood. On the other hand, we need more research, how interventions in the field of oncology and psychooncology as well as palliative care could promote integrity of personhood. This could be substantiated by developing instruments to measure the integrity of personhood. Ultimately, this research can help to create more wholistic and patient-centred interventions for patients living with advanced cancer.
Limitations and strengths
Even though this study aimed for a diverse group of interviewees, it is still limited as it recruited only patients from a single oncology centre and does not properly reflect the true diversity of patients living with advanced cancer. Further studies might look into larger populations and especially more diverse cultural settings. This study remains on an explorative, hypothesis-generating level. Follow-Up studies will need to confirm and refine the models generated in this study. For a qualitative study it is difficult to measure validity or reliability, 65 but we have undertaken every effort, to ensure the rigour, robustness and trustworthiness of the data and presented models, by including a transdisciplinary research team with regular meetings, a high level of reflexivity, and triangulation of the researchers for the analysis and of interviewees. Through these methodological approaches we hope to offer a significant contribution to the further improvement of care for people living with advanced cancer.
Conclusion
This study offers insights into the lived experiences of people with advanced cancer. It shows how it affects them, proposes the central aspect of the integrity of personhood as key to understanding the situation and suffering of that population and hence helps to lay the foundation to develop new interventions along the cancer care continuum to support people toward a more meaningful and integrated living with advanced cancer.
Footnotes
Acknowledgements
The authors are deeply indebted to all participants who were willing to share their experiences as painful as they are with us helping us to gain a better understanding of their experience. We have to thank our transdisciplinary research group on health service research for people living with advanced cancer and the group’s feedback, encouragement and intellectual input. We are very grateful for the support of our study nurse and two research students conducting the interviews. We also have to thank the teams of the palliative care unit, the department of haematology, oncology and immunology and the interdisciplinary chemotherapy outpatient clinic (IAC) at the university hospital of Marburg for helping with the recruitment of participants.
Author contributions
AS and MH share first authorship. PvB and CS share last authorship. CS, PvB designed the study, AP trained and supervised the interviewers, AP, AS and MH analysed and interpreted the data. CS and PvB contributed to the model development. AS and MH drafted the article. All authors approved the current version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by German Cancer Aid (Deutsche Krebshilfe), Ref-No 70114360, PI: Carola Seifart.
Research ethics and patient consent
Ethical approval was granted from the ethics committee for human research at Philipps-University Marburg (reference number 73/22). Participants gave written and verbal consent before participation in this study.
Data management and sharing
The datasets generated and analysed in this study are not publicly available to guarantee anonymity of the participants. The corresponding author can share further findings and secondary data products on reasonable request.
Additional information and requirements
Author Checklist
Reporting guideline