
Abstract
Background:
People of African and Caribbean descent experienced disproportionately high mortality from COVID-19 and have poor access to palliative care.
Aim:
To explore palliative care experiences of people of African and Caribbean descent during and immediately prior to the pandemic.
Design:
Qualitative interview study with thematic analysis. Refinement of themes/recommendations in consultation with an expert patient and public advisory group.
Setting/participants:
Twenty-six bereaved relatives and 13 health/social care professionals (cared for people of African and Caribbean descent) from throughout England, recruited using social media, community networks and direct advertising to over 150 organisations.
Results:
Three themes were identified: Representation: Participants did not see themselves reflected in the palliative care services and did not expect their needs to be understood. Mistrust of the healthcare system and perceptions of racism were common and led to anticipation of inequitable care. Personalisation: Relatives and professionals reported a lack of cultural and religious sensitivity in healthcare. Assumptions were made based on ethnicity, and services not offered to all. Awareness and education: Professionals felt they lacked the knowledge to provide care to diverse communities, but were reluctant to ask, due to fear of making mistakes. Inequitable access to services was exacerbated by, but not unique to, the pandemic. Participants recommended raising awareness of palliative services, building professional competence in culturally-sensitive care, and greater ethnic diversity within services.
Conclusions:
Person-centred, culturally-competent palliative care is not the norm for people of African and Caribbean descent. Expectations of inequitable care are widespread. Sustained action on multiple fronts is needed.
Keywords
COVID-19 had a disproportionate impact on people of African and Caribbean descent, with high levels of illness and death.
People from these ethnic minority backgrounds experience some of the highest levels of material disadvantage internationally, and historically have had worse access to palliative care services, compared to the majority White community.
During the pandemic, people of African and Caribbean descent experienced poor palliative care. This was exacerbated by an anticipation of inequity. Help was not offered and, in turn, was not asked for, as it was not expected to be received.
Bereaved relatives and health and social care professionals would like to see better representation of people of African and Caribbean descent in palliative care services; more culturally sensitive training for healthcare professionals; and investment in resources for service users.
Racism and discrimination in palliative care provision should be acknowledged and addressed. This should include better representation of African and Caribbean communities within services, better community engagement and more representative public-facing material
Services should be adapted to ensure they are culturally and religiously competent, recognising diversity in cultural and religious beliefs and practices and challenging racial and cultural stereotypes
Services should be better integrated into communities by working with faith/community leaders to raise awareness and build confidence and competence
Background
It is well established that ethnic minority populations experience health and social care inequity.1–3 Structural racism in care provision, housing, employment and the criminal justice system has a negative impact on the physical and mental health of individuals, whilst discouraging access. 4 Literature demonstrates that health seeking behaviour is delayed or avoided due to fear of racist treatment, specifically; negative interactions, stereotyping, disrespect, discrimination and cultural insensitivity. 4 Some communities, including people of African and Caribbean descent, have particularly poor access, experiences and outcomes. Anti-Black racism is a specific form of racism with a particular impact on health.5,6 Disparities in medical conditions and risk factors are not explained by biological differences.5,6 This was highlighted during the pandemic.7–9 People of African and Caribbean descent experienced the highest levels of intra-pandemic morbidity and mortality.7,10–19
The situation is complex; available data suggests layering of contributory factors, including; socio-economic deprivation, environmental, physiological and health-related behaviours exacerbates inequity. 20 Whilst the evidence demonstrating inequity is convincing, comprehensive understanding of its extent and causation is limited.1,2,7 Good-quality data is essential to enable policy-makers and health services to identify the specific needs of different ethnic groups, respond with tailored strategies for addressing inequity, together with associated evaluation of effect.1,2
Whilst inequity is seen across a wide range of services, certain providers, including specialist and generalist palliative care services are particularly culpable. 20 Palliative care has recently been identified as a basic human right. 21 Despite this, at least one in four families miss out on crucial support. 22 This is particularly true of those from ethnic minority communities,23–27 specifically, people of African and Caribbean descent who face enduring barriers to effective provision.10,15,16,28–30 Experiences during the coronavirus pandemic have highlighted this.31,32
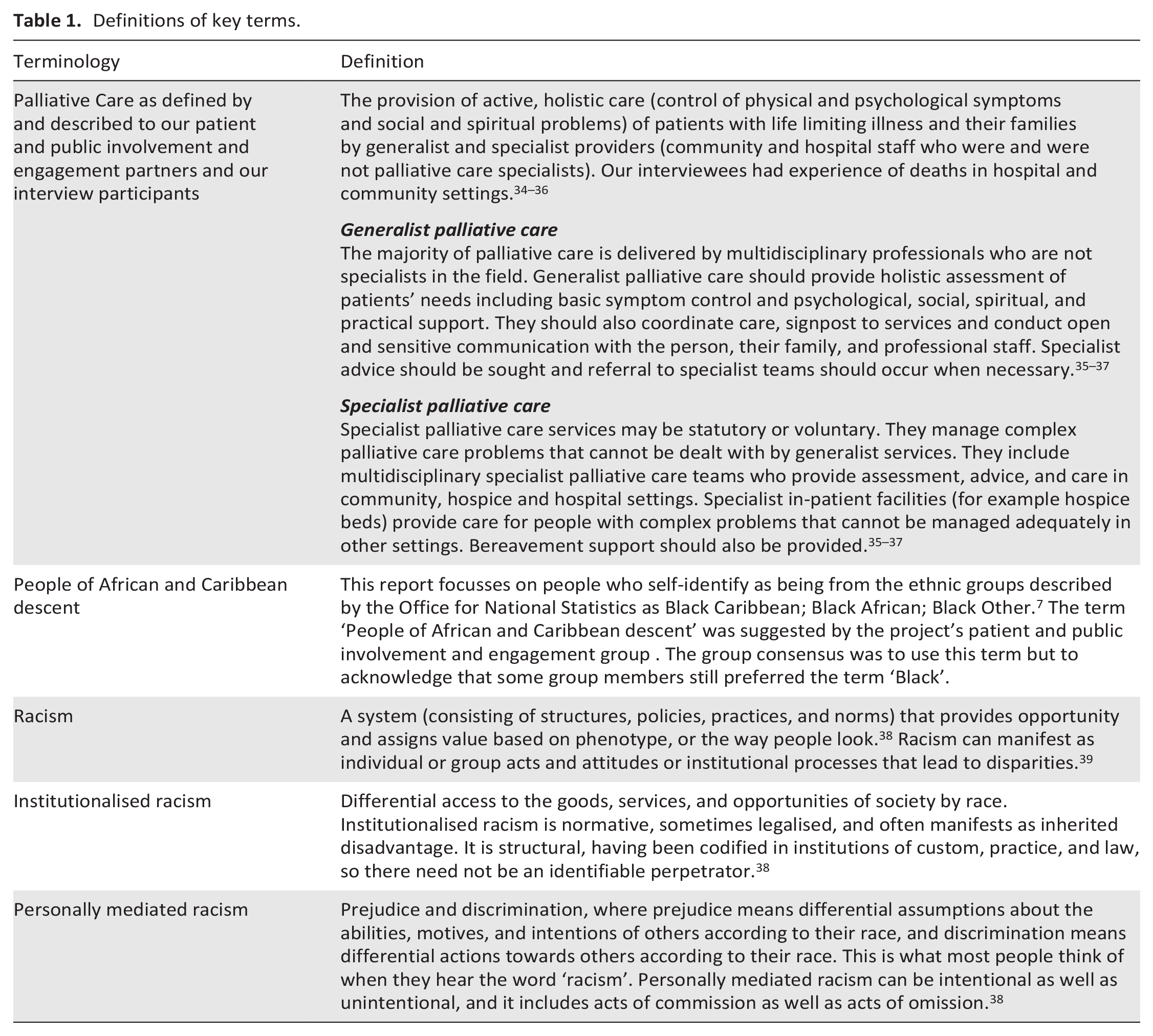
Palliative care services must be sensitive to diversity in religious practices, cultures and languages. 15 Yet, most research into how to provide culturally competent palliative care for ethnic minority groups is out-dated, out with the UK, or from London, where ethnic minority groups comprise over 40% of the population.10,15,16,28–30 This study begins to address this gap. We aimed to explore the palliative care experiences of people of African and Caribbean descent in England during and immediately prior to the COVID-19 pandemic. Importantly, we sought to foreground their recommendations for service improvement. The views and experiences of patients (by proxy), families, community workers, and health and social care professionals were explored. Given the majority of palliative care provided is by multi-professional teams who have not undertaken specialist palliative care training, generalist care was the main focus of evaluation. However, where people of African and Caribbean descent require high levels of support, and would benefit from care from multi-professional palliative care specialists, they rarely receive it, specialist palliative care was therefore also considered.10,28,33 Key terms/definitions are detailed in Table 1.
Definitions of key terms.
Methods
Design
The design was informed by existing research, which foregrounds structural racism as a key driver in ethnic inequalities. We used Critical Race Theory (CRT) to inform our theoretical approach.40,41 A core tenet of CRT is that structural racism and the resultant differential outcomes for minoritised ethnicities is due to subtle and ingrained institutional dynamics, rather than the explicit prejudices of individuals. CRT shaped our research question, with a focus on the voice and experiences of the minoritised and service improvement. We approached this qualitative interview study as applied researchers, therefore, the design was underpinned by pragmatic epistemology and critical constructionism. 42 Reflexive thematic analysis was performed with refinement of themes/recommendations in consultation with an expert patient and public advisory group. 43
Setting
Participants were recruited from throughout England.
Sampling
A combination of purposive and snowball sampling was used. 44 Over 150 regional and national health, social care, voluntary, charitable and educational organisations from throughout the UK were approached. The study was also advertised via social media (Twitter/Facebook) and radio. ‘Word of mouth’ recruitment utilised existing networks (identified by, or known to the study team) and used face-to-face, text message, email, telephone and WhatsApp contacts. Participants were offered a £25 voucher, on the recommendation of the patient and public involvement and engagement partners.
Population
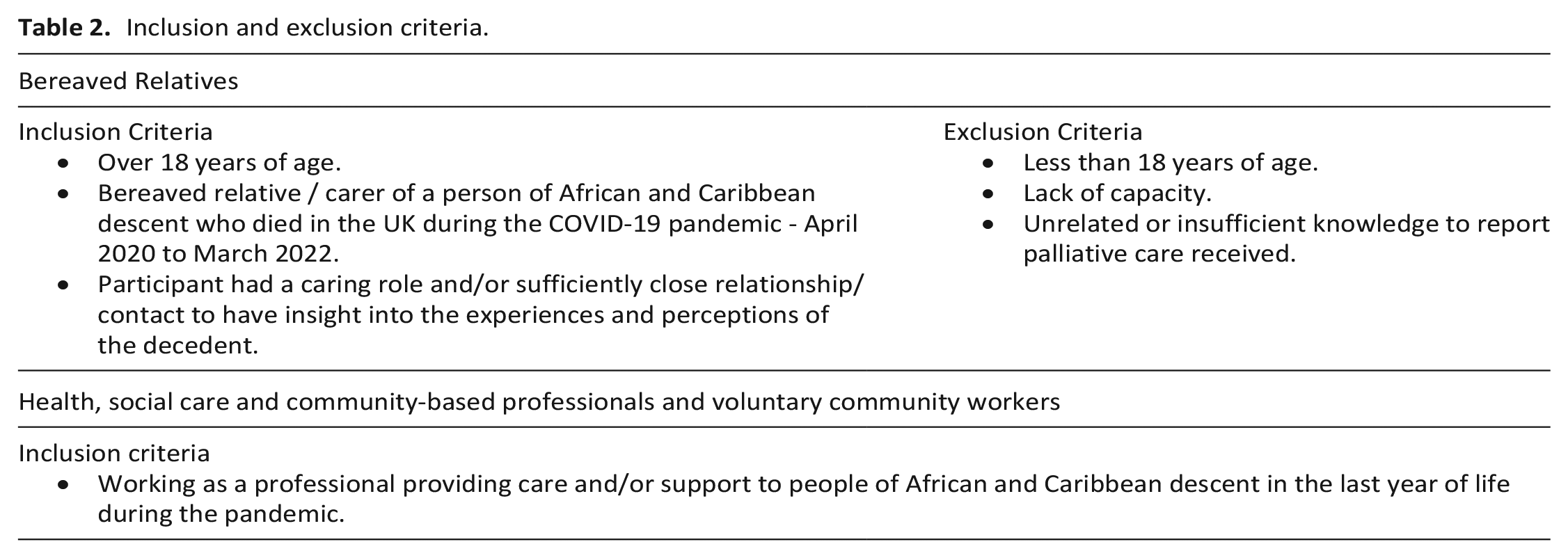
Bereaved relatives and health/social care professionals (related to/cared for people of African and Caribbean descent) were recruited between June and December 2021 (Table 2).
Inclusion and exclusion criteria.
Data collection
Experienced (>10 years) qualitative researchers (MP/EM) conducted interviews via secure videoconferencing platforms. They lasted between 30 min and 2 h. Participants provided informed verbal consent. Interviews were directed using a topic guide which was informed by the literature and co-designed with patient and public involvement and engagement partners (Supplement 1). They explored which services were and which were not, used in the last year of life, and the reasons for this, views on the care received, and recommendations for change. Interviews were transcribed, anonymised and checked to ensure individuals could not be identified.
Analysis
Data were analysed thematically, allowing flexibility to interpret and situate our findings in a policy and practice context. 45 Three researchers (MP/EM/TPK) coded the data. Two separate coding frames (relatives (Supplement 2) and healthcare professionals (Supplement 3)) were devised with codes and subcodes. These were discussed and agreed with the wider team who each coded 10% of interviews. NVivo 12 Pro software was used to manage the data. 46 The interviewing and analysis process overlapped to allow us to establish when data sufficiency/adequacy had been reached. This was said to have occurred when no new themes or codes were emerging from the data. It is appreciated that this is a subjective process, as such attempts were made to improve the robustness of this decision making using triangulation from multiple coders with different backgrounds and involvement of public and patient involvement and engagement partners as suggested by the literature.47,48
Patient and public involvement and engagement expert advisory group
We worked with a dedicated group of patient and public involvement and engagement partners, comprised of eight people of African and Caribbean descent. They were diverse in self-reported ethnicity, gender, geographical location and occupation. Some had experience of bereavement, some were healthcare professionals who have provided palliative care, and others were from Voluntary, Community and Social Enterprise (VSCE) organisations who have supported people of African and Caribbean descent during the pandemic. Patient and public involvement and engagement influenced the research in a number of key areas including terminology, scope of the research question, ethical considerations, recruitment, interview topic guide development and data analysis. 49 The expert patient and public advisory group reviewed a selection of the transcripts (25%) and provided input to the coding frame. They were in agreement with the final themes.
Results
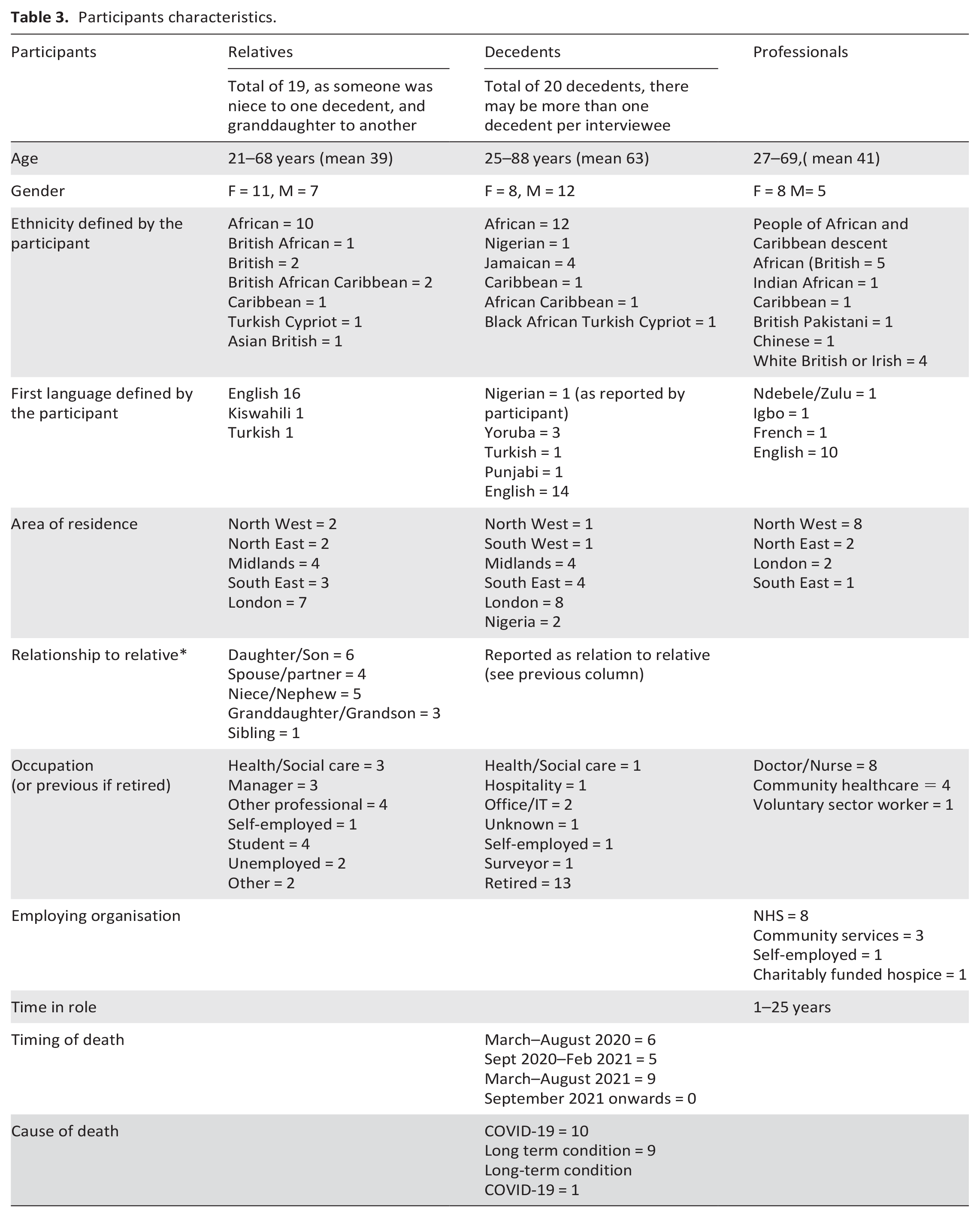
Thirty-nine interviews were undertaken, 26 of which were with bereaved relatives. Thirteen interviews were completed with health, social care and community-based professionals and voluntary community and social enterprise (VCSE) workers. No one declined to participate after initially volunteering to be interviewed. As interviews progressed, the researchers became concerned that some participants were not truly eligible. Eight of the bereaved relatives claimed to be living in the UK and have experience the death of a relative during the pandemic. However, these participants had supplied inaccurate demographic information and reported notably sparse detail in their accounts during interview. We suspect that participation was motivated by the payment offered. This judgement was based on experienced researchers and a whole team decision. None of the interview data judged to be inauthentic have been included in the analysis. As such, interviews of 18 bereaved relatives and 13 professionals were included and these participants’ characteristics are detailed in Table 3.
Participants characteristics.
The three generated themes were: representation, personalisation and awareness and education
Theme 1. Representation (in palliative care specifically and healthcare generally)
Participants reflected on low representation of people of African and Caribbean heritage in healthcare, specifically noting that people depicted in the COVID-19 response as frontline workers were predominantly White:
‘If you’re trying to encourage the Black community to go to the hospital, well, then actually at the early stages there wasn’t any evidence that the media were speaking to Black nurses and doctors at that time . . . there are lots of people who have come over from the Caribbean who have worked in the National Health, and clapped for them, but on television, you didn’t see that . . . there was lots of missed opportunities to speak to, erm, niche communities in a way that was, that- and then the government said, “Oh, you know, but people are not taking up” well, why would people take it up, because, you’re not talking to us’. Relative 9
‘When they started doing all the clapping thing for the NHS, at first all the images that they would show, they would all be White staff . . . now, Black staff, as in Black doctors, Black female doctors started doing their own on TikTok, you know, er, you know, to show that, “Look, we’re here as well, what about us?”’ Professional 12, VCSE
Both relatives and professionals perceived this lack of visibility had negative consequences. Some professionals felt that it represented institutionalised racism and that it was important to have a diverse workforce that reflected the communities served. The provision of information in different languages and using images of staff of different ethnic backgrounds, was proposed as a way of enabling people to feel they belong.
‘So, when people do come to the hospice, do they feel represented? You know, if- if they feel like they don’t belong, erm, because they don’t see themselves in the workforce. . . in the staff and the volunteers, then they’re not- you know, they’re less likely to share their experience in a positive way, with others in their community’. Professional 6, Clinical
‘We just don’t see ourselves there. That’s why it’s happening. As soon as we start and, “We’re here to help you,” even if it’s your food, your language, something to, like, they really do care, they’re really listening, I think that. . . because if a White person just comes to talk to you about palliative care and you don’t see yourself, I’m like, “Well, it’s only them.”’ Relative 5
Racism and discrimination
Both relatives and professionals spoke about their perceptions and experiences of racism in healthcare. However, the groups differed in their readiness to explicitly label NHS care as racist. Relatives felt that racism was difficult to articulate and prove.
‘So, if you’re, if you’ve experienced racism within society, why would you then think in, in health that you’re, you know, that you’re going to be treated fairly? And it wouldn’t be obvious . . . but it would be about someone waiting for attention and being overpassed; it would be that subtle’’. Relative 9
They described concerns about being treated fairly and a feeling that they had received differential treatment on the grounds of race, and the impact this has on trust of healthcare providers:
‘You pick up a tone, you pick up a, a vibe. I can’t explain it. You see how somebody talks to White people . . . then you, you might ask something similar whatever, and you get a different response, and you might not notice it if you’re the White person. . . But as Black people we do. It’s very difficult, because . . . you can’t prove it always. Most of the time you can’t . . . you are made to feel that, you know, you’ve got a chip on your shoulder, you are imagining it, you know, it’s not, yeah. But it is. It’s very real. Yeah. Definitely. Like I said, I’ve got a lot of experience of this unfortunately’’. Relative 3
‘. . .in terms of my uncle’s case, the elder generation, I think have been through more in terms of systemic, erm, obstacles and systemic kind of biases, erm, so they are gonna be more reluctant to take up any form of intervention or care-erm because the trust just isn’t there’. Relative 7
Some commented that people of African and Caribbean descent may delay presenting to services when unwell, as they anticipate a different level of care. Around a third of relatives cited population health data about ethnic health inequalities in COVID-19 and childbirth deaths to support narratives of their experiences of discrimination, or fear of racism in healthcare.
‘With childbirth, I know the, the mortality rate is highest in Black, Black women. I know that as well, erm, and I do worry because of my race and because I’m a woman I’m always worried that I’m gonna receive, erm, poor quality of care, that’s my main worry as well’. Relative 4
The professionals interviewed were more direct, providing examples of what they perceived to be institutionalised or personally mediated racism, whilst acknowledging the difficulties of tackling interpersonal and institutional racism:
‘A lot of [NHS staff] are quite narrow in their outlook . . . they will have had pretty kind of closed, working-class upbringings where it’s fairly common to have, erm, views that I would certainly consider to be overtly racist. And they probably wouldn’t consider to be overtly racist . . . So there’s a lot of kind of work to be done to try and. . . I, I think it’s really difficult to have those conversations in the workplace without kind of making people feel like they’re being judged but they have to happen’. Professional 13, Clinical
Race-based assumptions about people of African and Caribbean descent were felt to cause differential decision-making about treatment, care and support.
‘I think that’s also [NHS staff’s] knowledge, that, “Oh well, that community of people, they like to look after their own, so just leave them to get on with it”.’ Professional 12, VCSE
Two professionals commented on the lack of ethnic diversity in senior NHS roles, specifically in managerial positions, as such they observed that only those who were ‘White’ had power and influence.
‘There are certainly in existence, my experience of the snowy white peaks of the NHS. Erm, you know, the higher you go up, the more white and male it becomes, and that is seen all of the time. I think that there is an intersection as well with class here’. Professional 11, Clinical
Theme 2: Personalisation of care
The importance of a person-centred approach to palliative care was a consistent thread across interviews. Both relatives and professionals focused on the particular cultural and religious norms and practices around palliative care for people of African and Caribbean descent. But in such a large, diverse population, generalisations about culture, religion and history are seldom helpful. Instead, they stressed the need to ask about people’s individual/personal priorities.
‘I don’t think we should have a blanket approach to everybody. And I think we do need to be mindful, and just be brave and ask people, you know, “Is there anything in your culture that is important to you, and that can help me deliver care better?”’ Professional 6, Clinical
‘I just think that there’s too many assumptions made, that we do kind of cope within our communities and, and that’s it’. Relative 7
Families with members that worked in healthcare commented that they needed information on care provision and accessing support. Other relatives talked about their sense of duty to fulfil caring roles for older members of the family. Both groups were wary of healthcare providers making assumptions about what they knew or needed.
Almost all the interviewees remarked on the role of culture and religion in decision-making. Relatives emphasised the importance of spiritual wellbeing, faith leaders and religious rituals. Professionals, suggested patients should be encouraged to share information on their needs and expectations and acknowledged that professional recognition of religious sensitivities was needed.
‘With the African and Caribbean . . . some people are Christians, some people are Muslims, some people believe in traditional ancestral beliefs, so you have to respect all those. So if you ask the relatives or ask the patient, if the patient can communicate with you, they should be the one giving you the lead and telling you what they expect and what they want you to do’. Professional 2, Clinical
Only a minority of relatives recalled being asked about their religious beliefs. Fewer still reported that appropriate provisions were made by care providers. The neglect of religious practices was a potent cause of distress. One relative reported that Muslim after-death rituals were not followed, leaving them feeling that ‘they just dumped him anywhere’. (Relative 13) Overall, our interviewees described wide ranging deficiencies in the way services addressed the needs for people of African and Caribbean descent.
‘The care service is not set up for . . . cultural differences, . . .. So whether it’s in terms of food, whether it’s in terms of the family . . . I remember we talked about food. But just having familiar things, . . . whether it’s familiar music’. Relative 3
Impact of COVID-19
The coronavirus pandemic and associated social restrictions had a significant impact on the provision of care. All participants reflected on how people of African and Caribbean descent were disproportionately affected, which heightened fear in the community.
‘the amount of people of African and Caribbean descent and Asian people that died in the pandemic- [. . .] is completely disproportionate to the number of White people who died. [. . .] And so they, I did see that fear, I definitely saw that fear in, in those patients and their relatives’. Professional 9, Clinical
Increased risk of infection, greater likelihood of poor health outcomes and disruption to social life and customs were all described. A sense of isolation was a particular concern in bereavement, when families were obliged to be self-reliant. The wife of relative 10 had died from COVID-19 and isolation was foregrounded through his narrative:
‘But I can tell you it was a very, very, hard situation. It was very hard to face the way that things went. Because you know, when someone passed away, if you have people around it’s different but I was alone, no one was there so. No one came to visit me because of COVID lockdown, many restrictions. You cannot meet people, you cannot do that. It was in the first, first lockdown so a very, very, difficult situation’. Relative 10
The significance of restrictions on visiting
Both relatives and professionals described the significant impact that visiting restrictions had on their experience of palliative care. Many relatives were unable to see their loved one before they died and spoke of the distress this caused. A number felt that they were not involved in decision-making and received insufficient information about their relatives’ status and care:
‘the one that I struggled with . . . the most really was just dealing with not knowing you know, like just waiting for that phone call and not knowing so it’s kind of like you wake up but your day does not really start until you get that phone call to say, ‘Th-This is where we’re at’ and even if you do but, it’s only for a short period of time but three hours later you can’t just then phone in and say, ‘Oh how is he now?’ Or you can’t – you know, so yeah, the communication is the one that I really struggled with the most. N- not getting the information and obviously not knowing’ Relative 1
Healthcare professionals understood the importance of facilitating visits but were also aware of the need for restrictions. They described difficulties in navigating the social restrictions at different points in the pandemic and the impact on patients and families. Beyond health services, the social restrictions meant that many bereaved families had limited support.
‘Yeah, I think as time went on, we were just realising that’s not humane and that nobody wants to die alone, so you know, allowing some people in with, you know, relative precautions, erm- [. . .] was important’. Professional 9, Clinical
The demand on the health service, and impact on care
The demands placed on the health service by COVID-19 were part of many narratives, but families and professionals had different interpretations of the impact. Staff described the challenges faced in providing care, with high workloads, complicated cases and staff illness. Relatives described care being delayed or failing to meet expectations.
‘But I think the main thing is probably the volume. Like I said at the beginning, it’s like the sheer numbers of people and the fact that not a lot of people get better’ Professional 13, Clinical
‘Yeah, I think it was really difficult. I do get that the nurses, doctors were quite busy but I feel, erm, more attention should have been put on my uncle. And the appointments and the transplant should have been scheduled on time because as I said it was an ongoing condition, it was a year. And I feel like if he had that proper care, he would still be here today’ Relative 2
Theme 3: Awareness and access to palliative care
Professionals and relatives felt that the provision of holistic palliative care may not be offered to or understood by people of African and Caribbean descent. They identified the influence of culture on the social acceptability of talking about death, suffering, and grieving. Some described this in a historical context, referring to slavery:
‘There is a, erm, a belief, an understanding, a, a silent consensus that you don’t talk, you don’t talk about your hurts, you don’t talk about your upsets, you don’t talk about your, your fears or your concerns in that way . . . this also goes back to the event of enslavement, because there was a huge lack of distrust amongst ourselves, because we never knew who was going to go back and tell master and so that would equal a whipping or you could even lose your life’ Professional 5, Self-employed
‘In the Black community, there’s still that taboo of going for support and talking things out . . . especially with the older . . . that stigma and that taboo is still very much there . . . some of them are probably not aware that these services are available, but some of them are aware and just wouldn’t use them just because of the stigma’. Relative 26
‘I’ve known friends that died of cancer, my friends that didn’t want to tell anybody . . . I tried to signpost . . . to a support group. [but they said] “I don’t know what they do in support group. They just drink tea . . . all these White people’”. Relative 5
Professionals who were born, or had relatives, overseas described how the absence of healthcare systems in other countries may influence how people access care in the UK. This could lead people to self-manage or seek advice from religious leaders instead of accessing services. Professionals readily acknowledged that many healthcare providers lack awareness of the diversity of cultural needs.
‘if you ask the healthcare professionals . . . there is still a lack of understanding about different cultural beliefs. In Africa they think Africa is, er, or Afro-Caribbeans are just one community, they’re not. Africa is a continent. There so many diverse communities in Africa [. . .] They’re all different, they have all different practices, they have different communities, different cultures, different, you know, it might as well be Asia and Europe, you know, it can be as diverse as that’. Professional 4, VCSE
Participants highlighted a need to increase professional awareness of religion and cultures and public awareness about death, dying and the services available. Greater visibility within communities and stronger relationships between care providers and faith and community leaders were identified as potential strategies. One relative championed the potential contribution of older generations from diverse communities, as rich resources for learning about cultural diversity. There was a general feeling that responsibility to seek support opportunities should not lie with families who may be disadvantaged at a difficult time in their lives.
‘So I think on the whole, improving education amongst both the public and the healthcare professionals about what end-of-life care is available, er, what palliative- [. . .] care is available and what support, erm, is available’. Professional 7, Clinical
‘Yeah, so, I think- erm, I think reaching out to the community actually is- is really important. Linking with faith leaders, erm, and community groups’ Professional 6, Clinical
Improvements that would have wider benefits across the population were also identified by professionals and relatives. One professional commented that better training in palliative care amongst all healthcare professionals was required. Care homes and home care were specific settings highlighted by families as requiring better trained staff.
Communication and decision making
The COVID-19 pandemic had a profound effect on communication between professionals, relatives and patients, and within families. Remote modalities were often the only way to maintain contact, and some of these were new and unfamiliar to patients. Relatives described telephone calls from healthcare providers as infrequent, unclear or of poor quality. Video calls were seen on media coverage of the pandemic, but were not uniformly available to our interviewees. Provision was ad hoc and poorly resourced, sometimes relying on staff to share their own devices to facilitate contact between the patients and their families.
‘. . .We were able to FaceTime them, which was really lovely. The staff members, the carers, allowed us to call them on their private phones because there was no facilities . . . there were no, they didn’t have mobile phones for staff, erm, because I guess it wasn’t a thing that they were expecting would go on for, and then to try and get, you know, smartphones for every resident to have their own connection. So, we were really appreciative of the, the staff who allowed that to happen’. Relative 14
Changes in the mode of communication had a knock-on effect on the content of conversations. Open and honest communication was the aspiration for all interviewees. Relatives wanted information that was correct, timely, and sufficient to allow them to take part in decision-making and prepare for what was to come. They also felt that it was important for services to initiate contact with families, not vice versa. Healthcare professionals discussed the importance of building trust with families and devoting time to conversations, including advance care plans. They stressed that good relationships with families made it easier to understand what they were going through, and provide better support.
‘It feels really inadequate, me trying to support people over the phone when you’ve not even really met them before’ Professional 10, Clinical
In practice, changes associated with COVID-19 restricted the involvement of families in decision-making at end-of-life. Relatives stressed the importance of being able to see their relative and understand their decline, but this was often not possible or facilitated. Only one relative reported a positive experience of involvement in treatment decisions. Many felt that decisions were made without their knowledge or consent. Others were informed of treatment plans but felt unequipped to make informed decisions:
‘So I was going to ask them not to do it up ‘til Christmas. Maybe just give it two days so that you know, the kids at least can have. . .. . .Christmas . . . I don’t know whether that was an option or not because all they said is ‘This is what we’re going to do now’, . . . I didn’t know how bad it was the brain haemorrhage. I didn’t know if there was anything that can be done, like I don’t know anything about brain haemorrhages . . . I didn’t have any more information. All they said was like, ‘This is what’s gonna happen because he’s had a brain haemorrhage and we don’t think he’s gonna survive’. Relative 1
Professionals reported that their capacity to spend time building relationships with relatives was limited. Many described discomforts in, and the negative impact of conducting conversations about resuscitation and palliative care over the phone.
Access to support before and after death was hindered by service closures and reduced provision. Families felt that they were left to care for dying relatives without the necessary support, equipment or knowledge. Many described experiences that were overwhelming and incurring a lasting psychological cost. Support was more likely to be perceived as adequate if families were familiar with the healthcare system or able to advocate for their rights. Relatives who had access to specialist palliative care teams felt that this provided continuity of care for the family unit.
‘Erm, the fear that was within us all was, are they safe? Are they being looked after? Is anybody speaking to them? What is their, who’s looking after them whilst they’re in the hospital? Are people just in beds and being walked by? And that is pretty much what was happening. So, they would do the medication, erm, as it got busier there was less interaction. . .So, in mum’s case, she was a bed number; we would call, “Oh, bed number 25” erm, ,“there’s a call for bed number 25, if somebody could-” And my sister said, “Can you please stop calling our mother as bed number 25. . .”’ Relative14
Interviewees highlighted that improvements in palliative care and bereavement support are needed across the board, not just for African and Caribbean communities.
Recommendations
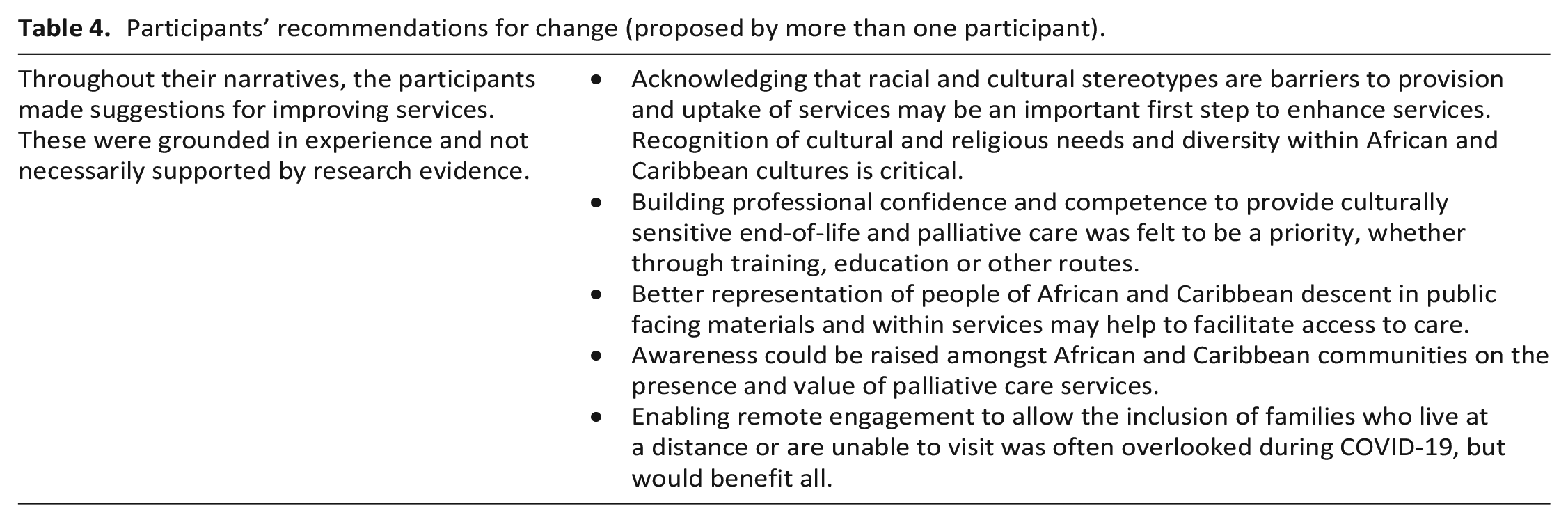
Participants made recommendations for change (Table 4).
Participants’ recommendations for change (proposed by more than one participant).
Discussion
Main findings
This research shows that the palliative care provided for people of African and Caribbean descent fell short during the pandemic on multiple fronts. Access to services was influenced by a mistrust of a healthcare system that does not represent minoritised groups. Assumptions were made about what was wanted and needed, based on ethnicity. Some participants, both relatives and professionals, believed racism to be entrenched in the NHS. Visiting restrictions and remote communication were areas of particular concern. Longstanding deficiencies in palliative care were evident during, and exacerbated by, the pandemic. Communication, shared decision-making and bereavement care were singled out. Priorities suggested by participants centred around refining services to better meet the needs of minoritised groups. This includes improving representation, challenging assumptions and building professional confidence and competence to provide culturally sensitive care. Working with African and Caribbean communities to raise awareness of palliative care services is needed.
Implications for practice
Research over recent decades has reinforced the need to improve end-of-life experiences and ensure equitable access to palliative care. 50 Certain populations miss out, but the underlying reasons and solutions for this have remained obscure.15,16,26,51,52 It has been suggested that the way palliative care is provided should be diversified. 30 Care should be personalised 53 and culturally sensitive. 13 Our study reiterates that requirement, whilst also providing suggestions from those with lived experience, to how this should be done.
Improving representation, including in advertisements and staffing, was proposed as a way of facilitating access and improving outcomes. Previous studies support the importance of representation to mitigate mistrust in healthcare systems. 54 Recent research has highlighted the presence of, and the need for, action against racism in palliative care provision.27,55 Our findings emphasised the importance of avoiding cultural assumptions and acknowledging our discrepancies as a catalyst for change. Participants proposed joint education initiatives between local communities and palliative care providers to improve access. Although we found no specific evidence of effectiveness to support this approach, this should be an area for future research.
Many of the deficiencies in care highlighted in this study may have arisen from the demands inflicted on services by COVID-19. This had impacts for all population groups.31,32,56,57 There is a growing body of evidence of the negative impact of hospital, hospice and care home visiting restrictions. 58 Communication and lack of access to appropriate technology exacerbated this issue, further isolating people from their social support networks. 59 There is speculation that a secondary bereavement pandemic will result. 60 Recent literature suggests that policies introduced to reduce the spread of COVID-19 disproportionately affected those from ethnic minority backgrounds. 27 Our study was not designed to evaluate the comparative impact of the pandemic on people of African or Caribbean descent. However, we did gain an in-depth understanding of the importance of community support rather than formal health and social care structures. The pandemic damaged these networks and left people isolated, and in many cases unable to appropriately mourn and attend religious ceremonies.
COVID-19 had an adverse impact on access to support before and after death and involvement of patients and families in decision-making.31,32,56,57 However, many of the findings are not specific to the pandemic. Research and evaluation of practice has consistently called for action to improve communication and decision-making at the end-of-life.36,61–64 Our participants’ accounts suggest that there is still work to be done. The few participants who had access to specialist palliative care services highlighted the benefits. Expansion of these services may contribute to a general improvement in end-of-life experiences.
Strengths and limitations
Proxy interviews can never capture the detail of lived experiences, but the views of relatives are important and have implications for bereavement. Proxy interviews also allow exploration of the entire end-of-life care period, including care just prior to death and in bereavement. A retrospective approach supports evaluation of care provided to people who deteriorated suddenly, or in whom the dying phase had not been recognised.
Recruitment to this study was challenging, despite use of the research team’s existing networks and contact with more than 150 diverse organisations. The decision was therefore taken to interview health and social care professionals. This added a range of complementary perspectives. We did not collect data on educational status, however we collected details on profession which demonstrates a range of backgrounds.
A small number of the relative interviews were judged by experienced researchers within the team to be inauthentic. We believe that these participants were motivated to take part solely to receive the voucher payment. We are aware that this may reflect complex and disadvantaged socio-economic situations.
Due to social restrictions, many family members who spoke to us were unable to be in close contact with their relatives or the service provider. Ordinarily, family members may have visited the person at end of life in their own home, care home or hospital – however this was not possible at the time. Therefore, this may have limited their specific knowledge about care and support.
Both researchers who collected the data were female and White British. However, other researchers key to recruitment and data analysis included individuals who identified as being Black British (TPK) and Black British/African (ED). All of the Patient Public Involvement and Engagement partners were of African or Caribbean descent. The research team, participants and the patients and public involvement and engagement group was not limited to a specific geographical location, with representation from North East, North West, South East, South West England and Greater London.
Conclusions
The delivery of culturally sensitive, personalised palliative care for people of African and Caribbean descent appears to be the exception, rather than the norm. This study was conducted during the pandemic, but the findings have implications for care beyond COVID-19. Participants proposed ways of addressing issues that would have implications for recruitment policies, workforce development and training and how services relate to local communities. Improvements in palliative care that would benefit all, could be focussed on communication, shared decision-making and bereavement care. Where palliative care provided to people of African and Caribbean descent was poor, this may not have been directly related to ethnicity. Applying a CRT lens to existing evidence on interventions to enhance equity and quality in end-of-life care may be a useful precursor to further empirical research. Comprehensive and accurate data on ethnicity are essential building blocks for evaluation and research. Promotion of their collection within routine and research datasets may also be helpful.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231188156 – Supplemental material for Unrepresented, unheard and discriminated against: A qualitative exploration of relatives’ and professionals’ views of palliative care experiences of people of African and Caribbean descent during the COVID-19 pandemic
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231188156 for Unrepresented, unheard and discriminated against: A qualitative exploration of relatives’ and professionals’ views of palliative care experiences of people of African and Caribbean descent during the COVID-19 pandemic by Felicity Dewhurst, Louise Tomkow, Marie Poole, Emma McLellan, Tafadzwa Patience Kunonga, Efioanwan Damisa, Melanie Stowell, Chris Todd and Barbara Hanratty in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163231188156 – Supplemental material for Unrepresented, unheard and discriminated against: A qualitative exploration of relatives’ and professionals’ views of palliative care experiences of people of African and Caribbean descent during the COVID-19 pandemic
Supplemental material, sj-pdf-2-pmj-10.1177_02692163231188156 for Unrepresented, unheard and discriminated against: A qualitative exploration of relatives’ and professionals’ views of palliative care experiences of people of African and Caribbean descent during the COVID-19 pandemic by Felicity Dewhurst, Louise Tomkow, Marie Poole, Emma McLellan, Tafadzwa Patience Kunonga, Efioanwan Damisa, Melanie Stowell, Chris Todd and Barbara Hanratty in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163231188156 – Supplemental material for Unrepresented, unheard and discriminated against: A qualitative exploration of relatives’ and professionals’ views of palliative care experiences of people of African and Caribbean descent during the COVID-19 pandemic
Supplemental material, sj-pdf-3-pmj-10.1177_02692163231188156 for Unrepresented, unheard and discriminated against: A qualitative exploration of relatives’ and professionals’ views of palliative care experiences of people of African and Caribbean descent during the COVID-19 pandemic by Felicity Dewhurst, Louise Tomkow, Marie Poole, Emma McLellan, Tafadzwa Patience Kunonga, Efioanwan Damisa, Melanie Stowell, Chris Todd and Barbara Hanratty in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to: Acknowledge the contribution of the participants, we are very grateful for the time they dedicated to the project and thank them for sharing their very personal experiences. Their insights are invaluable. Express our gratitude to our PPI contributors for their thoughtful feedback throughout the research process. Thank the Policy Research Unit for Older People and Frailty for hosting the study, specifically Jane McDermott, Anosua Mitra and Linda Welch for their support. Thank the many individuals and organisations who helped to publicise the project and assisted with recruitment. Finally the authors would like to thank St Oswald’s bereavement team for supporting our participants when they needed it.
Author contributions
All authors made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data. MP, EM, LT, FD, TPK, ED CT and BH drafted the original article. All authors approved the final version to be submitted. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Data management and sharing
Anonymised data is stored by Newcastle University and can be accessed on request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report presents independent research funded by the National Institute for Health and Care Research (NIHR) Policy Research Programme: Recovery, Renewal, Reset in collaboration with the NIHR Policy Research Unit for Older People and Frailty. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. Policy Research Programme Project Reference Number NIHR202685 and Policy Research Unit Programme Reference Number PR-PRU-1217-21502.
Research ethics and patient consent
This project was approved by Newcastle University Research Ethics Committee (2077/10053/2020 (including amendments 2077_1, 2077_2, 2077_3)).
Research was conducted according to the World Medical Association Declaration of Helsinki.
This manuscripts conform to the ICMJE Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.