
Abstract
Background:
Assisted dying, also commonly known as euthanasia and physician-assisted suicide, is legal in many countries. Interest in assisted dying is growing due to evolving societal understandings of a good death and a desire for choice. Ethico-legal perspectives are well-known, but as societies become more heterogenous, a greater understanding of the perspectives of people from diverse racial, ethnic, and cultural backgrounds is needed.
Aim:
To explore perspectives of people from diverse racial, ethnic and cultural backgrounds about assisted dying.
Design:
Scoping review with narrative synthesis. The protocol was registered with Open Science Framework.
Data sources:
Medline, CINAHL Complete, PsycINFO and ProQuest Dissertations & Theses Global were searched from inception to May 2023. Citations were independently assessed against inclusion and exclusion criteria.
Results:
Of the 17 included studies, perspectives of assisted dying were presented according to religion, religiosity, spirituality, race, ethnicity and ancestry. Perspectives were diverse, presenting more as a spectrum, with multiple intersections and interconnections. Support and/or opposition for assisted dying differed according to cultural attributes, but even amongst those with similar cultural attributes, perspectives differed according to life experiences and notions of suffering.
Conclusion:
Perspectives on assisted dying are dynamic and evolving. Even where assisted dying is legalised, individual’s cultural attributes contribute to unique perspectives of assisted dying as an end-of-life option. Thus, understanding a person’s culture, beliefs, expectations and choices in illness, treatment goals and care is fundamental, extending beyond what may be already considered as part of clinician-patient care relationships and routine advance care planning.
Keywords
Assisted dying, also known as euthanasia, physician-assisted suicide and Medical Assistance in Dying is legal in many countries around the world.
Given the purpose of palliative care is to improve the quality of life of patients with life-threatening illnesses and their families, and to prevent and relieve physical, psychosocial and spiritual suffering, but not to hasten death, assisted dying remains a hotly contested topic.
Growing public interest in assisted dying is linked to evolving understandings of the meaning of a good death, and an emphasis on choice at the end of life, but religious, moral and ethical concerns, a desire to protect the vulnerable, and concern over the medicalisation of death have been raised.
Religiosity, religious beliefs and spirituality had a clear influence on perceptions of assisted dying; enabling individuals’ clear and unequivocal stance on assisted dying.
Cultural attributes are many and complex, resulting in a spectrum of perspectives on assisted dying, and not all people assumed to have the same cultural attribute will hold the same perspective.
In addition to perspectives of assisted dying linked to cultural attributes, concern for vulnerable or marginalised people, those who lack resources to enable autonomy, and those who fear being a burden were also shared.
Promoting an awareness of, and openness to understanding the relationship between racial, ethnic and cultural attributes and the care provided to people with life-limiting illness, their family and carers across practice settings including palliative care is essential to supporting choice at the end of life.
Whilst we reported findings using the original terminology used to describe racial, ethnic and cultural attributes, a more nuanced approach to reporting in future research is needed because terminology changes over time, and must represent current societal preferences.
Considering the rapid evolution of assisted dying laws worldwide, more contemporary research is required to better understand current perspectives that would inform relevant policy and practice.
Introduction
Legal processes exist in many countries including Australia, Austria, Belgium, Canada, Colombia, Germany, Luxembourg, New Zealand, Spain, Switzerland, The Netherlands, and the United States of America, for individuals to voluntarily end their life. 1 Known as Assisted Dying, Euthanasia, Physician-Assisted Suicide, and Medical Assistance in Dying, 1 eligibility, processes and legalities differ widely between jurisdictions. Over twenty years ago, there was recognition that momentum for assisted dying would force a societal re-examination of assisted dying as a means to dignified death, 2 , 3 resulting in a paradigm shift in many countries. 2 Yet, assisted dying remains a hotly contested topic. 4 Given the purpose of palliative care is to improve the quality of life of patients with life-threatening illnesses and their families, and to prevent and relieve physical, psychosocial and spiritual suffering, 5 but not to hasten death, 6 the European Association for Palliative Care has taken a position that assisted dying (referred to as euthanasia and physician-assisted suicide) should not be included in palliative care practice. 6 Nonetheless, where palliative care begins and ends, 6 and how palliative care may intersect with assisted dying remains a major social issue for the wider community, with broader policy implications for governments 7 the health system 8 and all health care professionals who may care for people with life-limiting illness.9,10
There are diverse views on assisted dying. 9 Growing momentum and interest in assisted dying is linked to evolving understandings of the meaning of a good death, and an emphasis on choice at the end of life. 11 The emphasis on choice is linked with the principle of autonomy that underpins Western liberal traditions 12 and reflected in laws that authorise assisted dying. As societies become more heterogeneous, the primacy of autonomous decision-making, particularly at the end of life, may be questioned. 13 Consequently, different perspectives on life and death, 11 religious, 14 moral and ethical concerns and a desire to protect the vulnerable, 6 have emerged. In addition, strong moral convictions 3 and differing philosophies 11 contribute to concern over the medicalisation of death, and challenge beliefs about medicine. 8 There is also evidence that religious beliefs and anti-euthanasia sentiment influence societal tolerance and acceptance of assisted dying. 15
Cultural diversity is a broad term used to identify and acknowledge people or groups according to country of birth, language, Indigenous status, cultural background and ethnicity, 16 religion, ancestry, nationality and cuisine. 17 Cultural diversity may be most obvious when people or communities have alternate cultural characteristics from the broader society within which they live, such as is implied by the terms ‘ethnic minority’ 18 and ‘minority’. 19 For example, a person born in Australia, whose parents were also born in Australia, who identifies as Australian, and speaks English, may still identify as culturally diverse if they follow Buddhism, which is not one of the most common religions in Australia. Using this example, most of the person’s cultural attributes may be similar to broader society, but they may still be considered culturally diverse.
What is clear however, is that culturally diverse groups may have lower rates of health literacy impacting access and navigation of healthcare systems.20,21 Additionally, barriers such as low knowledge about assisted dying, 22 stigma, fear and embarrassment, 21 and alternate beliefs and emotions23,24 have been linked to polarising views. Nurses from culturally different backgrounds working in Australia have described how their views of assisted dying conflicted with their cultural and religious beliefs and practices. 25 Little is known, however, about the perspectives of members of the community from culturally diverse backgrounds; a perspective that is fundamentally important to all healthcare professionals who may provide care to people with life-limiting illness, irrespective of profession or specialty.
Methods
Aim
The aim of this scoping review was to explore the research evidence to answer the following question: What are the perspectives of people from culturally diverse backgrounds about assisted dying?
Design
Given the broad nature of the review aim, and potentially diverse and disparate forms of evidence, a scoping review 26 was undertaken using a five-stage review process including (a) identifying the research aim; (b) identifying relevant studies; (c) study selection; (d) presentation of the data; and (e) collation of the results. 26 A review protocol was prospectively registered with Open Science Framework https://osf.io/2dj69. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) statement was used to guide reporting of this review. 27
Inclusion and exclusion criteria
The focus of this review was people from culturally diverse backgrounds, however defined, and their perspectives of assisted dying. The concept and context guided the development of the inclusion and exclusion criteria (Table 1).
Inclusion and exclusion criteria.
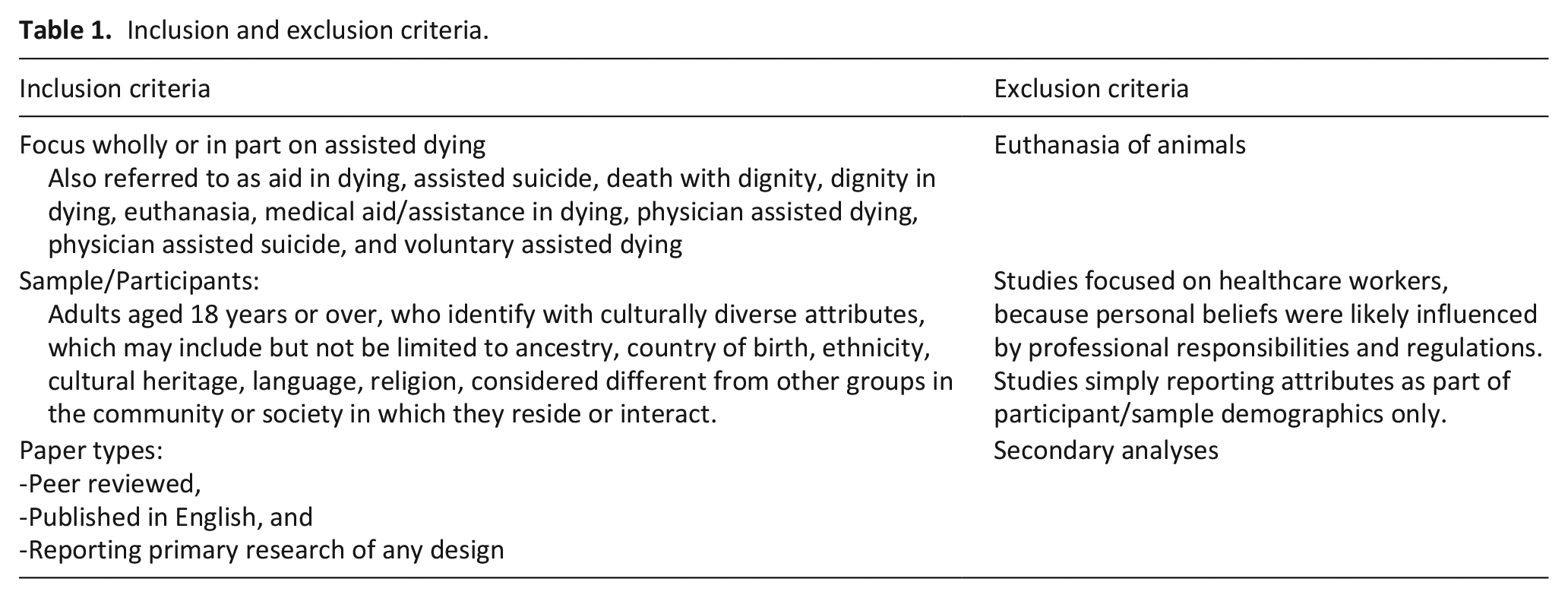
Similarly, studies with a less specific focus on death, with mixed samples that included children or healthcare workers were only considered if data were separated, enabling extraction from the findings.
Search strategy
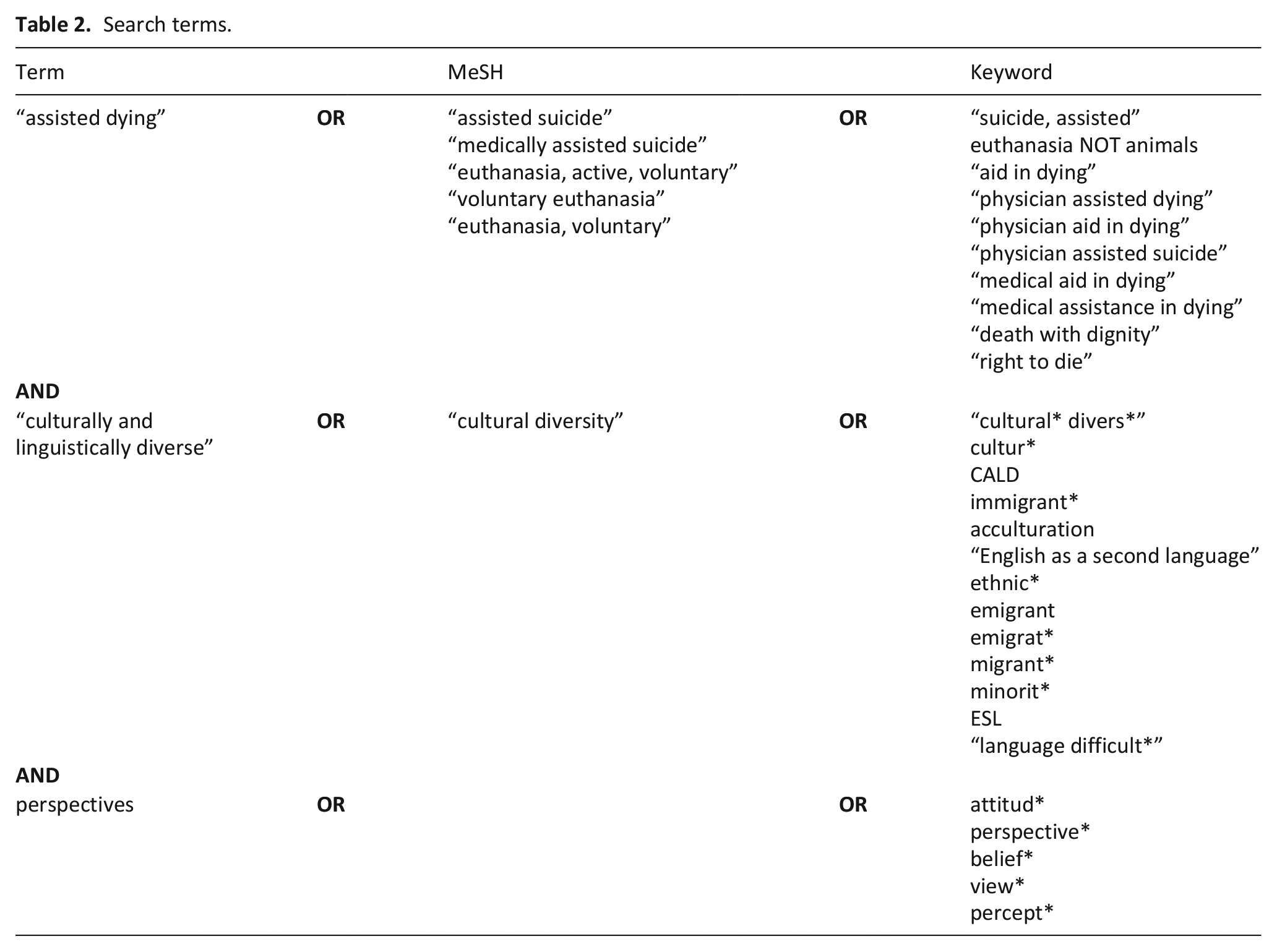
In collaboration with a university specialist librarian, an extensive literature search was conducted in May 2023, in these databases—Ovid Medline and Cumulative Index for Nursing and Allied Health (CINAHL) Complete, PsycINFO and ProQuest Dissertations & Theses Global. Searches for each term, the related MeSH headings and keywords were operationalised using OR, then combined using AND to identify studies. No publication date limits were applied to the searches (Table 2). The search was limited to English language only. A search is provided as an exemplar in Supplementary File 1.
Search terms.
Search outcome
Citations from all database searches were imported into Endnote, Version X9, 28 and de-duplicated. Citations were then exported into Covidence, 29 where additional duplicates were identified and removed. Screening of titles and abstracts against the inclusion and exclusion criteria was undertaken in Covidence 29 with each citation screened by two researchers. Full texts were retrieved for the remaining citations to enable independent full-text review by two researchers. As the meaning and assumptions about who may be ‘culturally diverse’, and how this was determined or understood, can differ according to context, the researchers worked on the assumption that not all people with the same cultural characteristics would have similar perspectives. Studies were included when and if the sample were described by the original authors as culturally diverse, or where cultural characteristics were reported that align with the study definition. Importantly, ‘culturally diverse’ does not necessarily infer minority. At both screening stages, conflicts were resolved through team discussion.
Data extraction
One researcher (LS) then independently extracted data from included studies, with a second researcher (MJB) confirming the accuracy of extraction across 40% of included studies. Data were extracted that contributed to describing the perspectives of people from culturally diverse backgrounds of assisted dying, necessary for synthesis. Where necessary, a third researcher (AB) was used to resolve disagreements. Data were extracted from each included study to denote year of publication, setting, aim, methodology and method, sample/participants and key findings.
Data analysis and synthesis
Given the heterogeneity of data across studies, a narrative synthesis approach, 30 was used in step (e) of the scoping review methodology. Analysis was initially undertaken independently by one researcher (MJB) using an iterative approach to enable identification of commonalities, differences and grouping of data according to common features and relationships in the data. 30 Preliminary findings were reviewed by a second researcher (LS) so that any differences or disagreements could be resolved, and to enable refinement of groupings. The synthesis was then reviewed by the remaining members of the research team (AB, JH, DM, LJ) so that final findings could be determined.
Findings
A PRISMA flowchart 31 documenting the results of the search and screening process is provided in Figure 1.
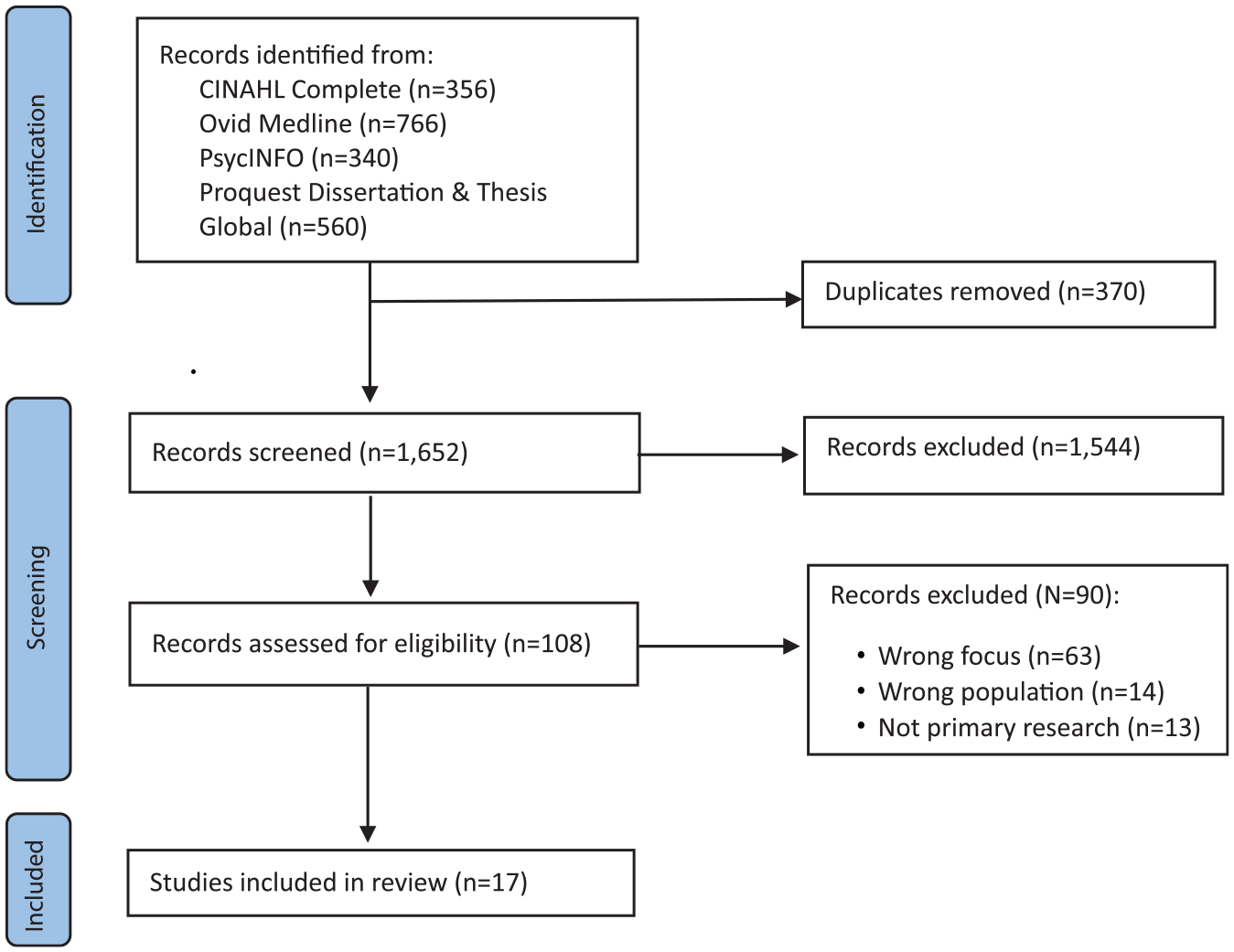
RISMA flow chart. 31
Characteristics of included studies
Ten studies, published between 1993 and 2022 provide data about the perspectives of people from culturally diverse backgrounds on assisted dying. Studies were conducted in the United States of America (USA),32 –41 three in Belgium,42 –44 and one each in Australia, 45 Austria, 46 Canada, 47 and Finland. 48 Nine studies used cross-sectional quantitative designs, and the remaining eight were qualitative, with data collected via interviews or focus groups. In total, more than 4450 participants were involved in the included studies (Table 3).
Characteristics of included studies.
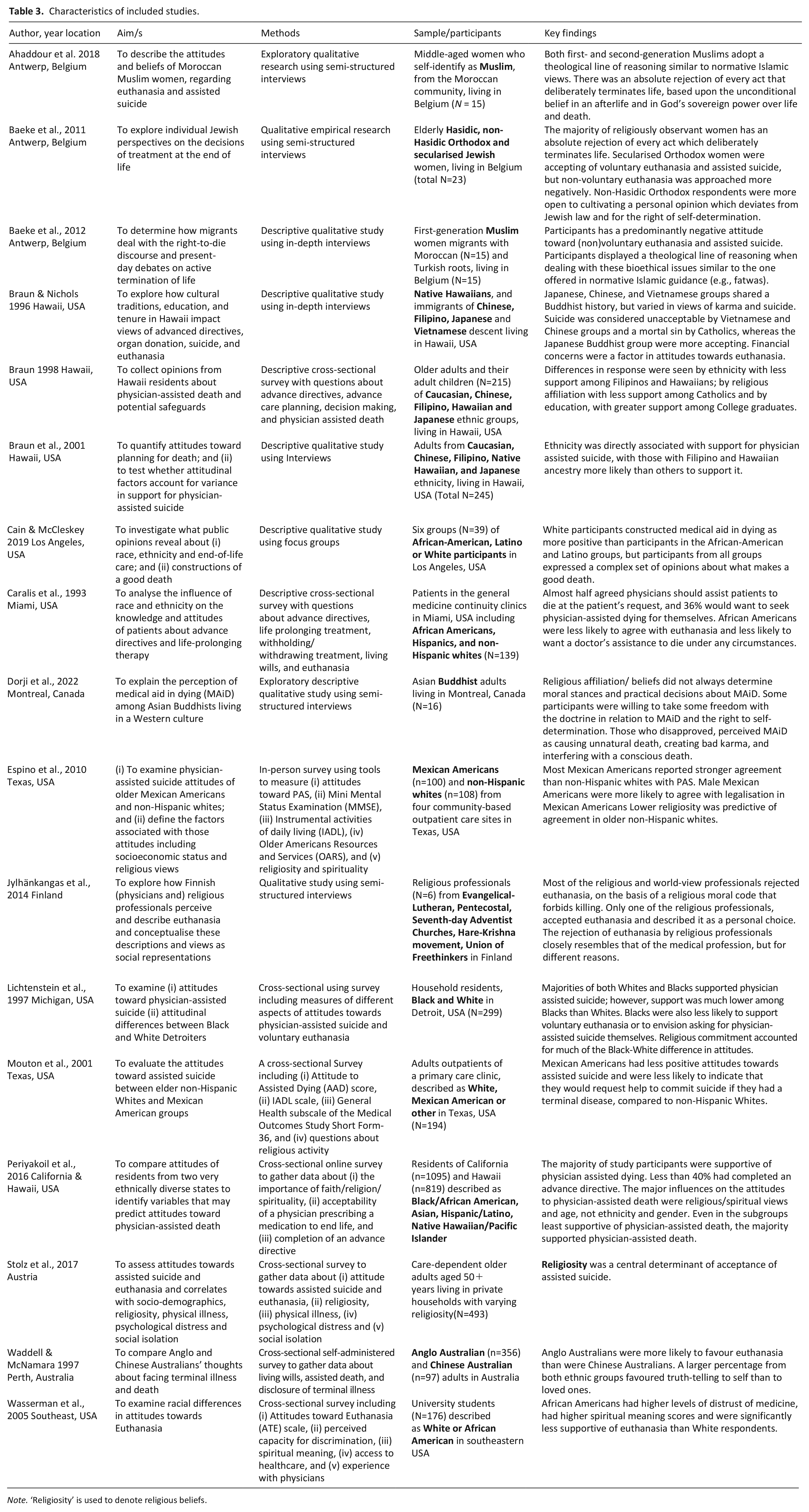
Note. ‘Religiosity’ is used to denote religious beliefs.
Findings are presented according to two major themes: (a) Religious and spiritual perspectives, and (b) Race, ethnicity and ancestry. For the purposes of this review, original descriptors used to denote religion, race, ethnicity and/or ancestry are used for reporting.
Religious and spiritual perspectives
Five studies provided perspectives on assisted dying according to various religious perspectives including Muslim,42, 44 Jewish, 43 Buddhist, 47 Evangelical-Lutheran, Pentecostal and Seventh Day Adventist churches, Hare-Krishna and those from the Union of Freethinkers. 48 Another five focused on religiosity37, 38 , 46 or spirituality.40, 41
My beliefs forbid it
The influence of religiosity, religious beliefs, and spirituality was identified across multiple studies, with the majority demonstrating a negative perception of assisted dying. Higher religiosity was predictive of disagreement with assisted dying in studies conducted in Austria, 46 and the USA.37 –39 Two other studies conducted in the USA reported on spirituality (not further defined) in which one reported a majority of participants supported assisted dying irrespective of spirituality 40 and the other reporting spirituality was negatively correlated with attitude toward assisted dying. 41
Perceptions of, and/or support for assisted dying was also examined according to specific religions. In three studies, the perspectives of Muslim women from Morocco42,43 and Turkey
44
living in Belgium indicated assisted dying was considered unlawful, in conflict and irreconcilable with Muslim faith.42,
44
Participants shared that a human being does not have the right to end their life, such as:
“According to our faith, it’s forbidden” (Turkish Muslim migrant, living in Belgium, p. 38).
44
“No no, that’s not good, that’s jahl [ignorance]. That’s shirk [blasphemy]. You may not end your life” (Moroccan Muslim migrant, living in Belgium, p. 5).
42
Assisted dying was not accepted by members of the Seventh-Day Adventist Church,
48
and for Hasidic Jews, assisted dying was forbidden because human beings do not own their own bodies, with no distinction between personal opinion and the viewpoint of Jewish law:
Life is not so easy. But, when we come with a purpose. And we know that we are not the boss and the body is not mine. I have a, I will face the consequences up there. (Hasidic Orthodox Jew, p. 265).
43
Assisted dying was also considered contrary to Buddhist teachings, known as the dharma, disturbing the departing consciousness:
If something disturbs the departing consciousness, it will lead to have bad things in next life. . . Dying mindfully is very important. . . it needs peace and calm, mindful and conscious.” (Canadian Buddhist, p.590).
47
Suicide and killing
In eight studies, participants held the perspective that assisted dying was akin to suicide or killing.33,35,38,42
–44,47,48 For Catholic Filipinos, assisted dying was against the Fifth Commandment,
33
and for Buddhist Vietnamese participants, equating assisted dying with suicide meant that a person “must go to Suicide Land and are very unhappy since they have not paid back their karma and it will follow them” (p. 263).
33
For those with Evangelical Lutheran faith, assisted dying goes against the Christian moral code that forbids killing.
48
Assisted dying was considered by Muslims as a grave sin,
44
indicative of turning away from God.
42
The person who does this “is a heretic, he does not have faith in Allah. (Moroccan Muslim, living in Belgium)
44
, and “. . . that person is very weak” (Moroccan Muslim migrant, living in Belgium, p.39).
44
Similarly for Hasidic Jews,
43
seeking assisted dying was considered a great sin and “out of the question. . . You do not decide when you come into the world. You do not decide when you die” (p. 267).
43
In a study conducted in the USA, assisted dying was considered “. . .absolute suicide for Christians” resulting in the person going “to the ninth circle of hell for it” (Christian, African American, p. 1185).
35
These sentiments were not dissimilar to the beliefs expressed by a Priest of the Hare-Krishna movement who likened assisted dying to suicide and murder:
We don’t accept that a person is killed with a poisonous injection or any other similar way just because suffering is unbearable . . . According to our view, suicide is not accepted. A person’s life should not be ended even if he wishes to die. Murder is never accepted. (Priest, Hare-Krishna Movement, p.360).
48
Assisted dying was also likened to killing in relation to beliefs about doctors’ involvement: “If the doctor does this, he commits a sin. Because that’s killing someone” (Turkish Muslim migrant living in Belgium, p. 39).
44
This perspective was also shared by Buddhists, such as:
“As a Buddhist, I don’t agree with it. Whether somebody infuses me the lethal substance or I do it by myself, it is anyway leading a person to die which is not natural. As a Mahayana Buddhist practitioner, killing is condemned and is a heinous crime. That is from a Buddhist view. Even if we look from another view, if you kill yourself, you are not accepting what is happening to you: the death, the suffering.” (Buddhist, p. 588).
47
In the hands of God or self
For many, the predominant view was that ‘life is in the hands of God’ (Pastor, Pentecostal Church, p. 360).
48
Similarly, other studies reported a Muslim belief that only God has the right to determine the time of death,42,43 with illness viewed as “God’s test. . . You have to endure it” (Turkish Muslim migrant, living in Belgium, p. 39).
44
Thus, any attempt to end life was forbidden, and explained as:
“God has given you a life and He is the only One who may take it away. It’s just that Islamic concept of ‘God has given you a life, God created you.’ You cannot decide when you will be born. You cannot decide when you’ll die” (Moroccan Muslim migrant, living in Belgium, p.7).
42
Jewish perspectives were similar, such as “no, it is shortening of life. He is no more in position to judge what is good for him” (non-Hasidic Jew, p. 267). 43
Even when assisted dying was forbidden by faith, some from Jewish,
43
Muslim,
42
and Buddhist faiths,
47
and the Union of Freethinkers
38
acknowledged the importance for each person to determine for themselves their course of action, such as:
“And if that, on that moment, is really your decision, why not? Why can you make decisions during your whole life, for sixty, seventy years, 24/24, and then you should not take the most important decision in life? . . . You only have one life, and I think, you can have a say in it” (secularised Orthodox Jew, p. 263).
43
“If the person is suffering, intensely hard for the family to see, I feel the person has to full right to say if he or she does not want to life anymore” (Buddhist, p. 592).
47
Maybe for unbearable suffering
Some who held fast to their religious doctrine were able to acknowledge that others may want to avoid suffering. 35 For many others, unbearable suffering was considered the decisive factor for which assisted dying may be more acceptable, for others even if not for themselves. There was acknowledgement that it was “not easy for the patient, to suffer so much pain (Turkish Muslim migrant, living in Belgium, p. 40); 44 and that “I think he or she should be given the chance to go peacefully, rather than. . . going through all kinds of pain and sufferings” (Buddhist, p. 590). 47
Data from the included studies also demonstrates divergent views even amongst those of the same faith, as demonstrated by these two Jewish perspectives, one of a non-Hasidic Orthodox Jew, and the other a Hasidic Orthodox Jew:
“According to me, yes. But it is not allowed according to the religion. . . if he suffers unbearable pain. And he does not want to live any more. For me, yes. I do know that it’s against the religion” (non-Hasidic Orthodox Jew, p. 264).
43
“I can understand when one suffers unbearable pains and if one cannot, if one cannot do anything about it, one cannot alleviate it or whatever, then I understand that that person asks this. But. . . that is not my answer” (Hasidic Orthodox Jew, p. 265).
43
Similarly, an atheist Freethinker presented a perspective of open-mindedness towards assisted dying, as a solution to the problems of suffering, because “according to our life stance. people should have the right to decide about their own issues. . . nobody owns us” (Chair, Union of Freethinkers, p. 360). 48
Race, ethnicity and ancestry
Ten studies provided data about individuals from various racial, ethnic and/or ancestral backgrounds. These studies used a range of descriptors including African American and Black;35,36,38,40,41 Asian, which includes Chinese, Chinese Australian, Filipino and Japanese;32,34,40,45 Caucasian including Anglo Australian, Non-Hispanic White, and White Californian;32,34 -41,45 Hispanic including Latino and Mexican American;35 –37,39,40,43 and native Hawaiian.32,34
In six studies conducted in the USA, support for assisted dying was compared amongst racial and ethnic-diverse groups. In one study, African Americans expressed both strong support and strong opposition to assisted dying, 35 while other studies reported that African Americans were significantly less supportive compared to White Americans (mean score 22.71 vs 24.82, p < 0.05), 41 and significantly less supportive of its legalisation (56% for Blacks vs 76% for Whites, p < 0.01). 38 In a comparison between three other race/ethnic groups in the USA, African Americans were least likely to support assisted dying. 40 Opposition to assisted dying was attributed to feelings of vulnerability in a characteristically White institution 41 and lack of autonomy, with those without economic resources less likely to have healthcare choices in a society that wants the easy way out. 35
Hispanic, Latino and Mexican Americans’ support for assisted dying was also reported in four studies. Whilst findings from one study indicated the majority of Latino participants were not supportive of assisted dying, 35 in another comparing Mexican Americans with non-Hispanic Whites, Mexican Americans reported stronger agreement with assisted dying (52.7% vs. 33.7%, p = 0.008). 37 The third study indicated Hispanics were less supportive than non-Hispanic Whites and Asians, but more than African Americans 71.6% versus 75.6%, 74.3% and 59.6% respectively. 40 Another measured attitudes towards assisted dying and found that Mexican Americans had less positive attitudes than non-Hispanic Whites (Assisted Suicide score 14.4 vs. 16.1, p = 0.03). 39
Two studies conducted in the USA also compared resident Asian groups with each other, those with Hawaiian ancestry and other American racial groups. In one of these studies, native Hawaiians were most favourable towards assisted dying (mean 88%), followed by Chinese Americans (mean 84%), Whites (mean 77%), Japanese Americans (mean 76%), Filipino Americans (mean 72%), Hispanic (mean 68%) and Black/African American (mean 61%). 40 In contrast, in another study there were significant differences in support for assisted dying between Japanese respondents (90% supportive), followed by Chinese (77%), Caucasians (74%), native Hawaiians (51%) and Filipinos (33%; p < 0.001). 34
Irrespective of measures indicating support and attitudes towards assisted dying, several studies demonstrated diverse perspectives on seeking assistance in dying. For example, African-Americans emphasised the importance of independence and not losing one’s self to serious illness. 35 Others were possibly willing to seek assisted dying in the context of suffering, with evidence non-Hispanic Whites were more likely to seek assisted dying compared African Americans and Hispanics in the context of terminal illness (p < 0.05). 36 Another similarly reported acceptance of assisted dying for terminal illness and those in pain across the majority of the Caucasian, Chinese and Japanese respondents, but not for native Hawaiians or those of Filipino descent. 32 Conversely, even in the context of unacceptable irreversible life threatening illness, Chinese Australians were significantly less likely to accept assisted dying compared to Anglo Australians (18.4% vs. 28.9%, p = 0.05). 45
Discussion
This scoping review aimed to explore the perspectives of people from culturally diverse backgrounds about assisted dying. Acknowledging that consensus on assisted dying might never be achievable, 6 the intent of this review was not to take a position on assisted dying, but rather to build understanding about the multiple perspectives of assisted dying that may be attributed to cultural diversity, including but not limited to religion and religiosity, spirituality, race, ethnicity and ancestry. Importantly, perspectives are not the product of a single cultural attribute. 49 Rather, these findings demonstrate that cultural attributes are many and complex, resulting in a spectrum of perspectives. Not all people assumed to have the same cultural attribute will hold the same perspective, and the reverse also seems to occur in that those with divergent cultural attributes may hold similar views. Thus, rather than considering cultural attributes in isolation, cultural attributes should be considered as an intersection 49 within each person’s broader worldview, 50 where previous exposure to, or contemplation of dying and death overlap and interconnect.
Perspectives on assisted dying are inextricably linked to dying and death more broadly. Dying is a social process, 50 evolving alongside, and influenced by socio-cultural understandings about what it means to live, and to die a good death. 3 For some, hope alleviates concerns about dying, 51 but for others, the ‘threat of disintegration’ does not go away. 52 Contemplating or confronting dying and death emphasises the finitude and irreversibility of human existence, challenging long held beliefs about life, 50 and for some, their beliefs about God’s control. Whilst not measured, firmly held religious beliefs seemed to enable individuals’ clear and unequivocal stance on assisted dying. These findings confirm the importance of routine exploration of Faith and spirituality to build understanding of intrinsic mediators influencing perspective and choice in people receiving palliative care. 51
These findings also expose concerns underpinned by power, vulnerability, and fear. In addition to Faith-based fears of going to Hell or being punished by God,33,35,42 –44 concern for vulnerable or marginalised people, 41 and those who lack the resources to enable autonomy 35 were identified in this review. In addition, fears of being a burden to family, dying alone, dying a prolonged death 51 and suffering52,53 that robs meaning from the last stages of life 54 are also well cited in the literature. An important finding in this review was that even for those who were opposed to assisted dying, contemplation of intolerable suffering could ameliorate this stance. If still not a choice they would make for themselves, there was understanding why others may seek assisted dying, a finding similarly confirmed amongst patients receiving palliative care. 55
A key message to come from this review is that culture and cultural attributes, however defined, are not static entities. Rather culture is dynamic and evolving, 49 and people assumed to have the same cultural attributes are not homogenous. 49 Thus, increasing awareness and openness to understanding the meaning of culture and cultural diversity as it pertains to care, is key. 56 Whilst debate continues about the ‘rightness’ of assisted dying, where it fits within society and healthcare, within or alongside palliative care, or as an entirely separate process and practice,10,11,57 what is common to both assisted dying and palliative care is a commitment to respecting choice, reducing suffering and facilitating good dying. 11 Thus, the stance that good palliative care can make suffering bearable and that foreclosing a natural dying process undermines valuable life experiences, 11 must be balanced by respect for each person’s right to autonomy and self-determination in life and death. 15
These findings, therefore, have clear relevance to palliative care, and any other discipline or team, such as those providing specialist cardiac, respiratory or renal care to people with a life-limiting illness. The demonstrated relevance relies on clinicians being appropriately ready and able to respond meaningfully. There is extensive literature promoting cultural awareness, cultural competence and cultural humility;58 –60 all of which encourage an openness to care that meets the needs of people with diverse cultural characteristics, but not necessarily action. Instead, aspiring for culturally responsive care, 61 which emphasises action, not just openness, is key. Achieving this however, relies on clinicians’ educational,49,62 emotional and social preparedness, 62 knowing how to communicate with cultural sensitivity,56,63 and in ways that are respectful of difference.
Strengths and limitations
This scoping review has several strengths. First, it brings together heterogenous data representing multiple racial, ethnic and cultural attributes, examined over almost 30 years, to exemplify how cultural attributes contribute to perspectives on assisted dying. Whilst the focus was specific to assisted dying, these findings may also have broader relevance to other contexts and settings in which care is provided to those receiving palliative care, and those facing life-limiting or life-threatening illness.
Importantly, our intent was not to make assumptions about the terminology or descriptors used to describe cultural attributes, hence, the terminology used in the original studies was replicated here. That said, it is important to recognise that terminology changes over time, as might societal attitudes towards assisted dying, and thus, these findings may not represent current societal preferences. This review did not include LGBTIQ+, because LGBTIQ+ did not fit with our operational definition of racial, ethnic and cultural diversity. If the perspectives of those who identify as LGBTIQ+ were included, it is possible that additional or alternate perspectives may have been identified. Whilst all included studies contribute to building understanding of the perspectives of people from diverse racial, ethnic and cultural backgrounds about assisted dying, it is important to note that not all studies were conducted in jurisdictions or at a time when assisted dying was a legal end-of-life option. The lack of identification of any studies from Asian, African or South American contexts, and the exclusion of studies published in a language other than English, are limitations of this review.
Conclusion and recommendations
This review demonstrates that perspectives on assisted dying are dynamic and evolving. Whilst the focus of this review was not to examine or add to debate about the ‘rightness’ of assisted dying, these findings clearly demonstrate that even in jurisdictions where assisted dying is legalised, each person’s cultural attributes likely contribute to their perspective. Using assisted dying as the exemplar or prompt, these findings also emphasise the importance of promoting an awareness of, and openness to understanding the relationship between culture and each individual’s cultural attributes and the care preferences of people with life-limiting illness, their family and carers across all practice settings, including palliative care. As such, seeking to understand a person’s culture and how this may mediate their beliefs, expectations and choices in health and illness, healthcare, treatment goals and intensity, is fundamental. Further research to evaluate and drive awareness of cultural diversity and enable a tailored response, in addition to what may already be considered as part of clinician-patient care relationships and routine advance care planning, is key.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241268449 – Supplemental material for Maybe for unbearable suffering: Diverse racial, ethnic and cultural perspectives of assisted dying. A scoping review
Supplemental material, sj-docx-1-pmj-10.1177_02692163241268449 for Maybe for unbearable suffering: Diverse racial, ethnic and cultural perspectives of assisted dying. A scoping review by Melissa J Bloomer, Laurie Saffer, Jayne Hewitt, Lise Johns, Donna McAuliffe and Ann Bonner in Palliative Medicine
Footnotes
Author Contributions
MJB: Conceptualisation, design, database search strategy, review and selection of studies, Data extraction and synthesis, lead manuscript preparation. LS: Database searches, review and selection of studies, data extraction and synthesis, manuscript review, project administration. JH, LS, DM & AB: Conceptualisation, design, database search strategy, review and selection of studies, manuscript writing and review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the corresponding author, [MJB], upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.