
Abstract
Background:
Family caregivers of people with high-grade glioma often report high rates of psychological distress, which has been attributed to the unique aspects of the disease and onerous care demands. Clinical practice guidelines advocate for caregiver support from diagnosis through to end-of-life and bereavement. Yet, research has identified that caregivers’ support needs are often overlooked.
Aim:
To explore caregivers’ experiences of psychological support and perceptions of what constitutes optimal psychological support for caregivers in the context of high-grade glioma.
Design:
Qualitative study involving semi-structured interviews with data analysed using reflexive thematic analysis.
Setting/participants:
Eighteen current (n = 11) and bereaved (n = 7) family caregivers (73% female, aged 33–69 years) of adults with high-grade glioma participated. Interviews explored caregivers’ perceptions of psychological support.
Results:
Two major themes were generated. The first theme, ‘It was never about me’, reflected caregivers prioritise for people with high-grade glioma to be well supported despite experiencing their own unmet psychological support needs. The second theme, ‘Continuous, coordinated and personalised support’, highlighted the importance of timely and tailored interventions addressing caregivers’ practical, educational and emotional support needs throughout the illness journey.
Conclusions:
Caregivers commonly prioritise the support needs of people with high-grade gliomas; yet, have their own distinct needs that vary throughout the illness. Primary care providers have a potential role in facilitating timely access to palliative care, practical support and brain tumour-specific psychological support to meet caregivers’ diverse needs across the care continuum in the context of high-grade glioma.
What is already known about the topic?
Evidence suggests that caregivers of people with high-grade glioma often report high rates of psychological distress across the illness trajectory.
Research shows that caregivers report various unmet support needs related to information, practical and emotional support.
What this paper adds?
Our study contributes to the evidence base that caregivers prioritise the support needs of the person with high-grade glioma, while having complex unmet needs themselves.
Caregivers are rarely offered psychological support for themselves, and bereavement support is almost non-existent.
Caregivers want timely access to care coordination and palliative care services, practical supports and brain tumour-specific psychological support.
Implications for practice, theory or policy
Better integration between oncology, palliative care and primary care services is needed to enhance caregivers’ knowledge, skills and confidence to provide care.
Primary care providers have a potential role in monitoring caregivers’ well-being and support needs and providing timely support and referrals (e.g. palliative care and psychology) throughout the illness.
Improved access to psychological support from diagnosis through to bereavement would be beneficial for caregivers of people with high-grade glioma.
Introduction
High-grade glioma is a life-limiting condition that encompasses effects of both cancer and brain injury.1,2 Classified as grade 3 and 4 according to the World Health Organisation, 3 malignant brain tumours have a high likelihood of recurrence and median survival time of 1–3 years. 1 Glioblastoma (grade 4) is associated with the poorest prognosis and a 5-year relative survival rate of 6.8%. 1
Resulting from the tumour and associated treatments (i.e. surgery, radiotherapy and/or chemotherapy), individuals with high-grade glioma typically experience progressive functional impairments, including sensorimotor, cognitive and behavioural changes and fatigue.2,4 Stressors related to poor prognosis, disease symptomology, ongoing treatment and surveillance and eventual functional decline contribute to high rates of psychological distress in people with high-grade glioma and their caregivers.5 –8 Due to short hospital stays and emphasis placed on outpatient care, family caregivers typically have a primary role in supporting individuals with high-grade glioma.9,10
Distress levels and care burden have been found to be higher for caregivers of people with high-grade glioma than other caregiver populations.11,12 In comparison to metastatic brain cancer and other palliative conditions, individuals with high-grade glioma had poorer functional status and greater need for support with daily activities, cognitive impairment and socialisation, resulting in higher family burden. 12 Caregivers of individuals with high-grade glioma have diverse support needs, including timely access to information, communication about prognosis and illness progression, involvement in clinical decisions and psychological support.13,14 Yet, studies have identified a major gap in provision of psychological support to caregivers.14 –19 This is despite psychosocial care guidelines for cancer and palliative care standards advocating for caregiver support to extend from the time of diagnosis to end-of-life and bereavement.20,21 Notably, most psychological interventions have focussed solely on people with high-grade glioma, with only one-third of intervention studies including caregivers. 22
An existing psychological intervention that involves caregivers is the Telehealth Making Sense of Brain Tumour (Tele-MAST Program), a 10-session intervention delivered via videoconferencing that supports individuals with brain tumour and family caregivers to understand the illness, develop coping strategies and find meaning in their life situation.23,24 In a randomised control trial, Tele-MAST was found to improve mental health and quality of life for individuals with brain tumour. 24 However, psychological benefits for caregivers were not evident and their participation was low (i.e. typically involved in only two to three sessions), potentially due to the main focus on the therapy goals of the person with brain tumour. In contrast to Tele-MAST, CARE-IS is a nurse-led intervention providing informational and emotional support specific to caregivers through a telephone assessment of their unmet needs, tailored resource folder, home visit and monthly telephone support for 12 months. 25 In a large randomised control trial (n = 188), CARE-IS was found to improve caregivers’ preparedness to care, however, levels of distress and quality of life did not differ from controls. 26
A potential reason for the gap in caregiver-specific interventions is a lack of understanding of caregivers’ psychological support needs and preferences. Despite some shared support needs (e.g. access to information), caregivers’ support needs differ from those of individuals with high-grade glioma and extend beyond the illness to include bereavement support. 10 Caregivers want support to manage the impact of caring on their own life, discuss sensitive issues (e.g. behavioural and personality changes), address practical issues and make life decisions in the context of uncertainty.10,16 Therefore, caregivers’ perceptions of their own needs and preferences for support are essential to inform the optimal timing and format of caregiver-specific psychological support interventions.
Aims
This qualitative study aimed to explore current and bereaved caregivers’ perceptions of previous psychological support and identify what they consider as optimal at different illness phases. We sought to address three research questions:
RQ1: How do caregivers perceive the psychological support available to them across different illness phases?
RQ2: What type/s of psychological support would caregivers have wanted or preferred that was not available to them at the time?
RQ3: What do caregivers consider optimal psychological support at different illness phases?
Methods
Design
Qualitative methodology using semi-structured interviews (Supplemental Material 1) and reflexive thematic analysis was employed.27,28 The focus on caregivers’ perceptions of psychological support aligned well with reflexive thematic analysis which follows an interpretivist-constructivist paradigm27 –29 concerned with understanding subjective meaning of experiences in particular social contexts. 27 The reporting followed the Consolidated Criteria for Reporting Qualitative Research (COREQ; Supplemental Material) guidelines. 30
Participants and recruitment
Convenience and purposive sampling were used during 2022–2023 to recruit current and bereaved caregivers supporting family members of adults with high-grade glioma across various illness stages, including bereavement. Most caregivers (n = 14/18) were recruited either prior to or following the Tele-MAST program, 23 which was originally designed to primarily support individuals with brain tumour; however, in 2022 Tele-MAST was extended to support caregivers’ own psychological support needs. Snowball sampling was also employed via participants recruited for the Tele-MAST program, to include caregivers not seeking psychological support (n = 4). One of the approached caregivers declined to participate. Although there are no specific guidelines on sample size requirements for reflexive thematic analysis, Guest et al. 31 identified that 12 participants are typically adequate to achieve data sufficiency in qualitative studies. To reflect diverse experiences throughout the illness and including bereavement, we aimed to recruit 18 caregivers.
Data collection and ethical considerations
Ethical approval was obtained from Griffith University (HREC 2022/327) and Metro South Health (HREC/2022/QMS/83846) Human Research Ethics Committees in April-May 2022 prior to recruitment. Prospective participants were contacted via email or telephone and received the information and consent form. All participants provided verbal consent.
Interviews were conducted by experienced psychologists with doctoral qualifications (AB - female: Doctorate in Counselling Psychology; KL - female: Masters in Psychology & PhD). KL supervised a research training of a psychology honours student (AJ; male). AJ was involved in four interviews; he initially observed two interviews and then led two interviews with KL overseeing the process. Interviews followed a topic and question guide (Supplemental Material 1) that was developed by TO, KL and AJ, and piloted with the first caregiver interviewed. The topics and questions were deemed appropriate, and no changes were made. The questions covered the psychological support available to the caregiver at the time of the diagnosis, throughout treatment and end-of-life care of the person with high-grade glioma, satisfaction with support received, unmet needs and recommendations for caregiver support in the future. The interviews were conducted via telephone (n = 11) or videoconference (n = 7). Interviews took 10–76 min (M = 39.5, SD = 20.81) and were audio-recorded and transcribed verbatim.
Data analysis
Transcribed interviews were analysed using the six-phase methodological framework for conducting reflexive thematic analysis,27,28 which entailed an iterative approach involving: (1) repeated reading of manuscripts to gain familiarity and immersion in the data (KL and AJ); (2) initial code generation after discussing the first two transcripts (KL and AJ); (3) preliminary theme and category identification (KL, AJ and TO) after coding eight further transcripts as guided by Nowell et al. 32 (KL and AJ) (4) theme review and refinement following coding of subsequent interviews (KL) and research team discussions; (5) theme definition and labelling; and (6) preparing the manuscript using relevant exemplar quotes. The main strategies used to enhance rigour were the researchers’ use of a reflexive journal and consensus coding. NVivo (QSR International Pty Ltd; March 2022) was used to organise participant data into codes, subthemes and themes (Supplemental Material 2).
Results
Sample characteristics
Eighteen caregivers (n = 13 female; 73%) aged 33–69 years (M = 50.33, SD = 8.62) participated (Table 1). Of those currently supporting an individual with high-grade glioma (n = 11), the average time since diagnosis was 4 years (SD = 4.65). Seven caregivers were bereaved, with time since bereavement ranging from 2 weeks to 10 years. Most caregivers were spouses or partners (78%) and the most common diagnosis was glioblastoma (71%).
Participants’ demographic and illness characteristics for their relative.
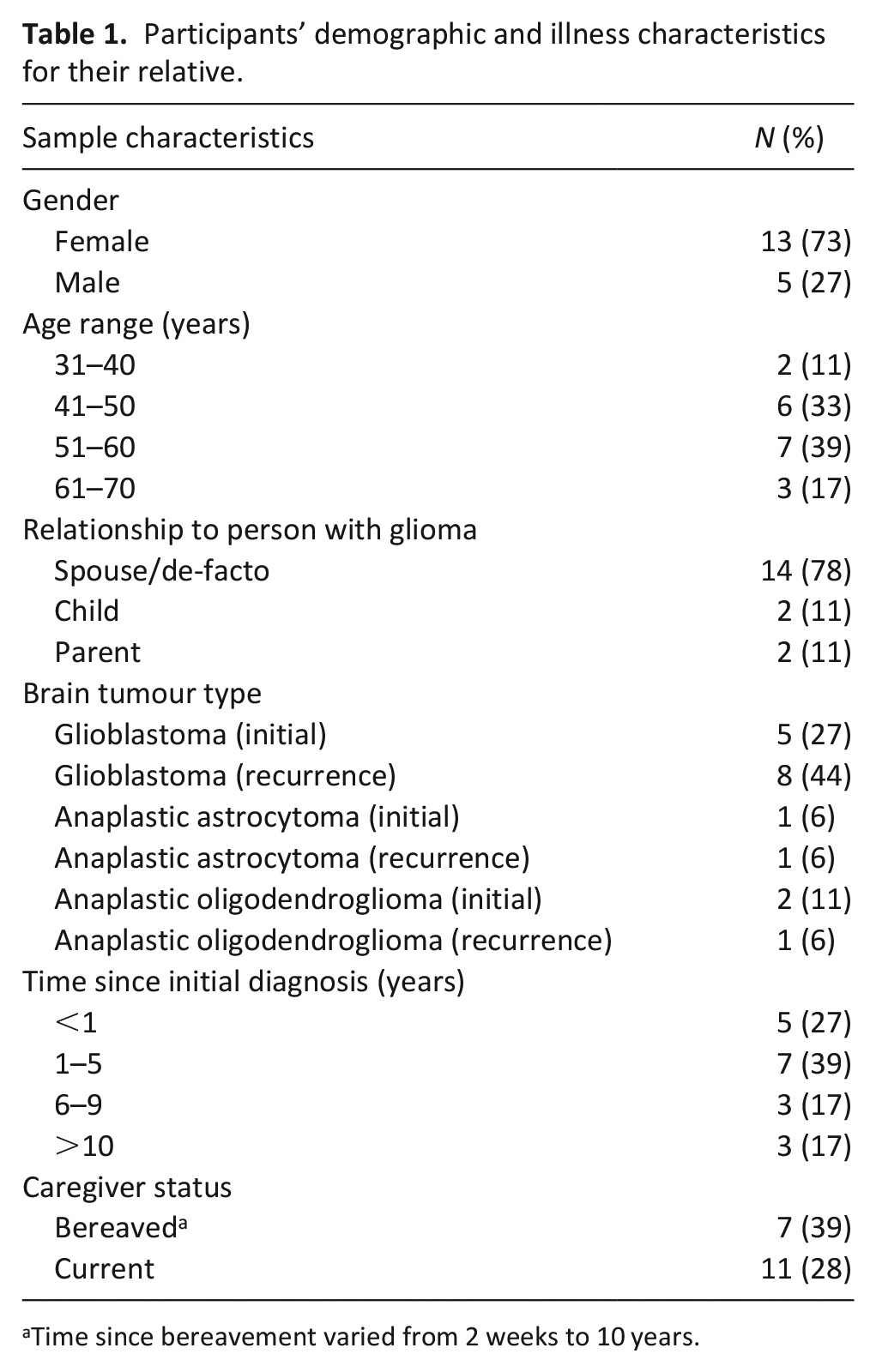
Time since bereavement varied from 2 weeks to 10 years.
Themes
The analysis generated two overarching themes: (1) ‘It was never about me’: Caregivers’ priorities and mismatch in needs and support and (2) Continuous, coordinated and personalised support; both of which had four subthemes (Figure 1). Theme one characterises caregiver priorities for the individual with high-grade glioma to be well supported, with their own support needs often being overlooked and unmet. Theme two highlights the importance of care and service coordination, accessing practical support and brain-tumour-specific psychological support to meet caregivers’ diverse needs across the illness trajectory.
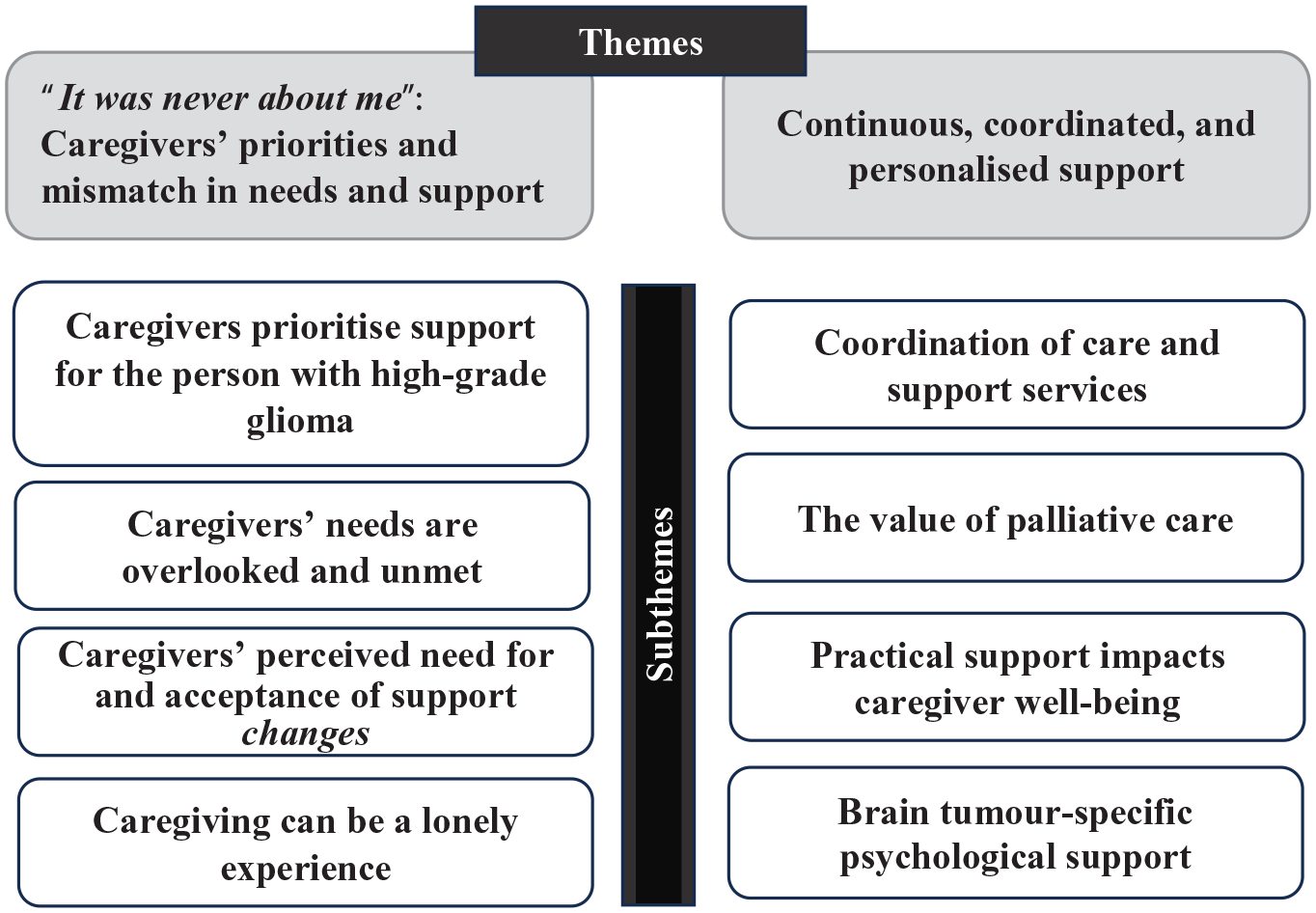
Themes and subthemes depicting caregivers’ perceptions of support.
Theme 1: ‘It was never about me’: Caregivers’ priorities and mismatch in needs and support
Caregivers’ perception ‘it was never about me’ had a double meaning, whereby caregivers prioritised their loved one’s support needs, whilst simultaneously recognising that their own support needs were often unmet or overlooked.
Caregivers prioritise support for the person with high-grade glioma
Participants described prioritising support for the person with high-grade glioma; ‘It was always my mission to do whatever I needed to do for him. He needed me to be strong for him. So that’s what I did. I just stayed staunch’ (C001, wife, bereaved). This often meant that caregivers advocated on behalf of the person with high-grade glioma; ‘I advocated quite heavily with the medical team about the drug Avastin to be used for him’ (C008, partner, bereaved). Such advocacy was deemed necessary for their relative to access timely care, whereas caregivers did not recognise their own support needs or viewed these as secondary; ‘I didn’t actually look for any support for myself. I was just happy to make sure she got the support she needs’ (C005, husband, current caregiver).
Caregivers perceived a need for inner strength to support the person with high-grade glioma when receiving distressing news from medical professionals; ‘that’s their skill or lack of skill in being able to analyse the patient and work out what they can and can’t take. So then, oh don’t worry we won’t upset them, we’ll just upset the carer. They can deal with it’ (C003, wife, bereaved). Prioritising their loved one’s needs extended to self-educating about high-grade glioma, aspects of caregiving and available support, ‘I’ve sort of been all over stuff and had done a lot of research and I don’t feel confident in many things, but I do feel confident in looking after him’ (C002, wife, current caregiver).
Caregivers’ needs are overlooked and unmet
Despite mainly viewing their own support needs as secondary, caregivers recalled timepoints throughout the illness where their needs were overlooked and unmet. At the time of diagnosis, caregivers experienced their own shock and disbelief; yet, compassion and empathy were often lacking in delivery of the news.
The surgeon, which was amazing, just walked in and said, ‘He’s got glioblastoma, stage four. It’s the wild one and he’s got a maximum of two and a half years’ and walked out. . . and we’re like, what the? (C006, wife, current caregiver).
As the person with high-grade glioma experienced rapid changes in their health, caregivers’ distress regarding the poor prognosis was compounded by increased workloads; ‘Everything was heavy in our life at that time and the bucket gets full with heavy stuff and then it starts overflowing and you kind of max out’ (C010, husband, bereaved).
The little available support was typically directed towards the person with high-grade glioma; ‘It was never about me. They weren’t specifically asking about me and what did I need. It was more, what did I need for him’ (C001, wife, bereaved). Caregivers who sought support for themselves were typically unable to access this in a timely manner: ‘By the time they called me back and I was off the waiting list I was past the challenge of that time’ (C002, wife, current caregiver). This was also the case for caregivers who experienced bereavement, ‘So I went to the GP [general practitioner] because I was struggling. So, that wasn’t something that was kind of proactively offered’ (C009, son, bereaved).
Caregivers’ perceived need for and acceptance of support changes
Caregivers’ perceived need for and readiness for support was found to vary over time. Initially, their focus was on appointments, accessing information and coming to terms with the diagnosis and hence they often felt unready to reach out for or accept support: ‘You may need support, but you also need to process this. What’s your greater need, processing it or getting support from others? And trying to balance up your needs in that early part. I think you just get on with things and it’s very hard, while you’re getting on with things, to process that stuff’ (C017, wife, current caregiver). Some caregivers who eventually sought help initially delayed seeking this due to the burden of additional responsibilities: ‘I’m still trying to figure out where I’m going to fit in, where I’m going to get the time to have any session (. . .) I don’t want to even be hopeful of getting any kind of emotional support if I’m not going to be able to fit it into my day. (. . .). So, it’s kind of like, I feel like giving up before beginning’. (C007, wife, current caregiver).
Caregivers’ perceived need for psychological support often increased over time but was unmet: ‘I would rather just be left alone [at the beginning] whereas now we’re past all that, so it’s a bit depressing now’ (C014, wife, current caregiver).
Caregiving can be a lonely experience
The unique challenges of caring for a person with high-grade glioma and the lack of psychological support often left caregivers feeling misunderstood by and isolated from their family and friends. As one caregiver explained, ‘Most of them just don’t get that my whole life has changed as well. It doesn’t only affect the person going through it. It affects our children’ (C004, wife, current caregiver). The sense of loneliness was compounded when caregivers were the only family member providing care: ‘I mean, my dad was there but he was pretty hopeless in terms of being able to provide care at all, so it was pretty much just me’ (C009, son, bereaved). Support from family and friends was also often described as limited and unhelpful, therefore some caregivers preferred self-reliance to avoid burdening others or due to their lack of confidence in support: ‘We’ve been on this journey for so long and you just feel like you wear your friends out’ (C002, wife, current caregiver). The same participant found that connecting with other caregivers mitigated the sense of loneliness and feeling misunderstood: ‘I think the fact that you talk to other people, other carers who are also brain cancer carers, is really powerful for me because the whole thing with this is that people don’t get it.’
Theme 2: Continuous, coordinated and personalised support
The second theme encapsulates the variations in support caregivers receive and perceptions of what constitutes optimal psychological support for caregivers. Although some types of support discussed were not psychological in nature, caregivers perceived that multi-faceted support that included care and support coordination, access to practical support and tailored brain tumour-specific psychological support impacted their psychological well-being across the illness.
Coordination of care and support services
Caregivers’ accounts reflected their struggle and the stress associated with navigating hospital systems, treatment and medication protocols, appointments and support services. Most caregivers identified a care coordinator as critical for the person with high-grade glioma and their own support needs. A bereaved caregiver recounted, ‘if they’d said, ‘here’s a support person who’s gonna sit with you and can work through all aspects of your medical treatment’, then we would’ve jumped at it’ (C003, wife, bereaved). Those supported by neuro-oncology care coordinators (usually nurses) described the benefits of information, guidance and compassion:
You could just ring her and, if she didn’t answer, you’d leave a message. . . She would always get back to you and give you information, or just listen and give me advice but she was just absolutely amazing (C015, daughter, bereaved).
Some caregivers reflected on the gap in the role of the general practitioners who were in a position to facilitate access to support for caregivers: ‘I think GPs could also play a role in sort of, working with caregivers to say these are your options if you need support’ (C009, son, bereaved). However, for other caregivers, the need to access services via general practitioners’ referral was considered an unnecessary burden: ‘to go and speak to the GP about the referral and why we need it. (. . .) there’s this doubling up stuff that doesn’t really understand the plight of the person in it’ (C016, husband, current caregiver).
Timely access to information was seen as vital to caregivers’ psychological well-being and self-efficacy. However, due to limited availability of oncology nurses, many caregivers needed to coordinate their loved one’s support during times of high distress; ‘that was one of my memories from when she was first diagnosed. You get 1000 brochures and there are all these support groups that can help and it’s all great and it’s also very overwhelming’ (C010, husband, bereaved). Support coordination needs extended to accessing disability funding packages to provide therapies and respite services. Such applications were often rejected due to administrative barriers which were only rectified after caregivers were linked to a brain tumour advocacy service:
They did the (application). I just didn’t have the time or, to be honest, I didn’t have the strength to do it because it’s just forms, forms, forms and interviews and I just can’t do it. They first denied our (application) and then we had to redo it (C006, wife, current caregiver).
The value of palliative care
Caregivers highlighted the ‘amazing’ value of support provided by palliative care services. However, most perceived such referrals as coming too late and ‘all of a sudden’ (C003, wife, bereaved). One caregiver whose family member was referred early and alongside oncology treatment, perceived palliative care services as valuable despite being ‘a bit confronting’ (C007, wife, current caregiver). Medical assistance and information from palliative care services helped caregivers to reduce hospital visits and provide better care within their home, especially when coordinated with general practitioner’s support: ‘But now with the palliative team, and my GP, I now just have to give him clonazepam when he has a seizure, so we don’t go to the hospital. We are at home and we deal with it together’ (C006, wife, current caregiver). Some perceived mutual benefits of palliative care for the person with high-grade glioma and caregiver: ‘for me to have a respite, or for mum to have a respite’ (C015, daughter, bereaved).
Bereaved caregivers recalled the value of emotional support, especially from nurses as the main point of contact, ‘sharing that journey with me to an extent’ (C009, son, bereaved). However, such support ended as soon as their relative died: ‘as soon as she died, it was like, it’s over (. . .) no follow up. Also, all the people I’ve been sharing this journey with for the last sort of couple of months, we’re now cut off from each other because their job ends when you leave the hospital’ (C009, son, bereaved). Only one caregiver who was recently bereaved had accessed counselling after their spouse’s death: ‘I think I can get three sessions; there was indication they could do a couple more or then it becomes a paid for thing’ (C003, wife, bereaved).
Practical support impacts caregiver well-being
Practical support directed towards caregivers’ needs was viewed as important for reducing caregiver burden and contributing to their well-being, yet this was difficult to obtain and typically unavailable from support organisations; ‘They’re hard to get onto and that’s a big assessment over the phone with me and I told them what we wanted, and I’ve never heard from them since, (. . .) And all they were going to offer was 20 hours of support’ (C018, mother, current caregiver).
Although initially difficult to navigate, once approved, disability funding packages for the person with high-grade glioma enabled practical support including support workers, carer respite and assistance with home maintenance: ‘We’re doing a little bit of house cleaning. I’m looking at doing a little bit of maintenance, such as getting the windows clean and getting someone to come and help him with some odd jobs’ (C004, wife, current caregiver). Support workers had many benefits, including providing respite for caregivers, enabling them time for social, work and household activities which contributed to better psychological well-being; ‘I had a sense of release. His support workers would be with him so I could go and see my friends’ (C008, partner, bereaved).
Brain tumour-specific psychological support for caregivers
Caregivers expressed the need to access psychological support from psychologists and counselling services with relevant expertise in brain tumour and to also meet other caregivers of people with high-grade glioma. One caregiver described feeling understood and less isolated after meeting other caregivers; ‘They get it, they’ve lived it, they know and it makes you feel you’re not alone’ (C004, wife, current caregiver). Some community-based cancer support agencies were perceived as less supportive due to their broad approach to cancer information: ‘(Cancer Community Service) gives you a booklet and that booklet’s fine, but it’s more for generalised cancer’ (C006, wife, current caregiver). Conversely, caregivers connected to brain tumour-specific services conveyed feeling validated by personalised support.
Psychologists with specialised knowledge of brain tumour and programs that supported both people with high-grade glioma and caregivers were perceived to provide a more personalised and tailored approach. Caregivers who had previously taken part in a brain tumour-specific psychological support program reported experiencing a sense of hope and validation. One caregiver expressed: ‘At this stage, we had done our sessions with (psychologist) and found them ridiculously uplifting and meaningful’ (C008, partner, bereaved). Another caregiver viewed the same program as enabling him to communicate at a deeper level after his wife passed away and that it normalised his experience.
I didn’t realise how much I needed it until we were into it. Because I don’t talk with anyone else, to that depth. And I think (psychologist) gave me hope that what I was going through was normal, my reactions were normal and that things will get better over time (C010, husband, bereaved).
Discussion
Main findings of the study
This study aimed to understand caregivers’ previous experience of psychological support and identify their unmet needs and what constitutes optimal psychological support. Findings depicted how caregivers prioritised the support needs of their relatives with high-grade glioma over their own and the disparity between caregiver needs and available support. Optimal support for caregivers encompassed care and support coordination, timely access to palliative care, practical support and brain tumour-specific psychological support from professionals and other caregivers across the illness trajectory including bereavement.
What this study adds?
Contributing to the current evidence base, caregivers prioritised their loved ones’ support needs through advocacy, self-educating, organising and attending appointments and taking care of practical matters including funding for services (e.g. respite care). Caregivers viewed access to their own support concerning their increased workload and distress as secondary; however, they experienced many unmet emotional, informational and practical support needs. These findings align with previous brain tumour research suggesting that caregivers put the support needs of their loved ones first and may not seek or accept support.10,15 Francis et al. 33 found that caregivers were exhausted and suppressed their own emotional needs to meet caregiver responsibilities. Similar to other research,13,14 our findings highlighted the importance of sensitive communication by health professionals, especially around prognosis, to reduce caregiver distress. Overall, the present findings underscore that caregivers have distinct support needs from the person with high-grade glioma and likely require expertise to identify since the caregiver may not be forthcoming in asking for support. This exploration of support needs could be provided by primary care providers such as general practitioners, with whom patients and caregivers often have a pre-existing relationship, are usually their first point of contact and can provide early referral to professional services (e.g. palliative care and psychology).
Extending upon previous studies,20,21 these findings highlight the importance of continuity and personalisation of support for caregivers from diagnosis until bereavement. Access to neuro-oncology care coordinators and palliative care services made a significant difference in terms of meeting caregivers’ information and emotional support needs. Trad et al. 34 similarly asserted that neuro-oncology nurses and care coordinators are well-positioned to facilitate psychological support and needs assessment; however, in the Australian context, these are not available in all treatment settings due to limited funding.18,34 This need could be addressed in part by better integration (especially early referrals) between neuro-oncology and palliative care.2,21 The results also highlight the need for better integration of services with primary care providers, including general practitioners and community nurses. Although most caregivers found their general practitioners supportive, they highlighted the additional burden of extra visits to obtain referrals to access other services and the lack of information integration (e.g. availability of health records to care providers) between different services. These findings are in line with general practitioners’ own experiences and practices as reported by Cavers et al. 35
Our findings highlighted that people with high-grade glioma are usually referred to palliative care near end-of-life and, while support was highly valued at this time, this ceased when the person died. Bereavement support for families has been recognised as a core component of palliative care,21,36 yet, this was non-existent or limited for caregivers in the current study, who needed to seek this from other sources (e.g. general practitioners or community-based psychologists). Therefore, there is scope to extend the role of community-based primary care to provide consistent support for caregivers of people with high-grade glioma across all phases of illness.18,35,37 The potential role of primary care in supporting caregivers has been also highlighted in other oncological 38 and neurological conditions. 39 However, as reported by Cavers et al., 35 general practitioners are often unsure about their responsibilities and the specific needs of people with high-grade glioma and their caregivers. Therefore, training and resources focussed on specific informational, emotional and practical support needs of people with high-grade glioma and caregivers would be beneficial for primary care providers to increase their knowledge and capacity to support the dyad.
Interestingly, although the interview focussed on psychological support, our analysis revealed the importance of practical support for caregivers’ psychological well-being. While some caregivers faced barriers to accessing practical support (e.g. respite services and home maintenance), those who received advocacy support from a brain tumour-specific service to navigate disability funding schemes reported significant benefits for their own well-being. Previous research has highlighted many unmet support needs related to managing caregiving demands, practical issues (e.g. transport and respite)16,40 and financial difficulties 41 which in turn contribute to caregiver strain and distress. Hence, access to advocacy services is important as part of care coordination that impacts caregiver well-being.
Furthermore, access to brain tumour-specific psychological support emerged as a key element of caregivers’ perceptions of optimal support across the illness including bereavement. This included peer support, which has previously been found to validate caregivers’ experiences and provide emotional support. 42 As most caregivers were recruited as part of the Tele-MAST program,23,24 many had experience with brain tumour-specific psychological support. In contrast to general cancer counselling services, this program was perceived to provide a more personalised and tailored approach through supporting caregivers to cope with brain tumour-related issues and, following bereavement, navigate the transition from being a caregiver to focussing on other life priorities. Yet, there are few interventions developed specifically for caregivers in the literature. 22
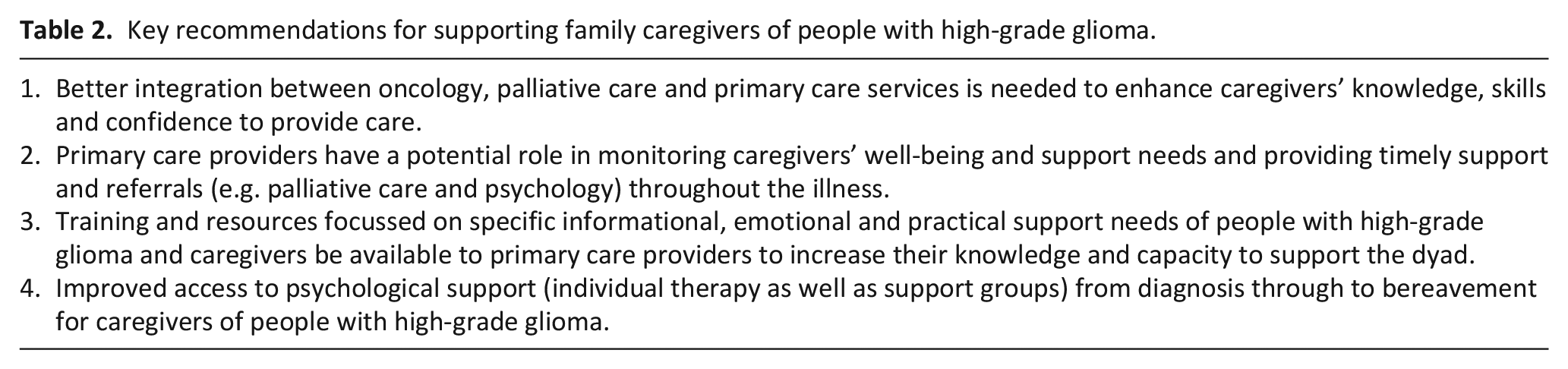
In terms of clinical implications, the findings reinforce previous research highlighting the importance of caregiver appraisals concerning their ability to cope and sense of being supported.43,44 For some, caregiving may be viewed as their ‘mission’, whereby caregivers recognise their inner strength and derive positive meaning from their role. Conversely, caregivers may also at times feel overburdened by the role and unsupported, which intensifies feelings of distress and loneliness. In addition to identifying unmet support needs, it is recommended that health professionals seek to understand how caregivers make sense of and cope with challenges associated with caregiving, including the meaning derived from their role and appraisals regarding their own support needs. As noted by Pasman and Koekkoek, 2 research on the benefits of early palliative care and routine integration with neuro-oncological care and primary care is needed along with brain tumour-specific psychological support for caregivers. The key recommendations and implications for policy and practice arising from the study are summarised in Table 2.
Key recommendations for supporting family caregivers of people with high-grade glioma.
Strengths and limitations of the study
As a potential limitation, different researchers were involved in conducting the interviews. Despite using the same interview topic and question guide, differing interviewing styles may have introduced variability in the way questions were asked and nature of prompts. Further, most caregivers were recruited prior to, or after participating in Tele-MAST. Although this was appropriate for exploring prior experiences of psychological support, these accounts largely reflect the experiences of caregivers who seek support, including both current and bereaved caregivers. None of the interviewers were involved in the Tele-MAST intervention delivery for caregiver participants; however, KL was involved in screening and assessment as the Tele-MAST project coordinator with two caregivers who had already completed the intervention with SJ as the therapist. In line with reflexive thematic analysis, 27 the researchers engaged in reflective practice and consultation with a senior researcher (TO) to consider the influence of their prior experience and assumptions on interpretation of the findings.
Some caregivers were supporting individuals living beyond the median survival time for high-grade glioma and time since bereavement varied from 2 weeks up to 10 years which may impact caregivers’ perceptions of their support needs and experiences. Furthermore, the timing of referrals, commencement and duration of palliative care services were not specifically addressed in the interviews. Additionally, in line with previous research26,45 most of the recruited caregivers were female (13/18). As qualitative research aims to reflect diverse experiences, some issues related to the experiences of male caregivers could have been overlooked in our study. More generally, the relevance of these findings may vary according to the clinical setting and sociocultural context.
Notwithstanding these issues, the present study advances understanding of caregivers’ experiences of psychological support and what constitutes optimal support in the context of high-grade glioma from caregivers’ own perspectives. It is recommended that future research evaluate multi-component interventions addressing caregivers’ informational, practical and psychological support needs.
Conclusions
Overall, the findings highlighted that the support needs of caregivers of individuals with high-grade glioma are typically overlooked and they may deprioritise their own needs. There is a need for better continuity and personalisation of support through timely access to care coordination, palliative care, practical support and brain tumour-specific psychological support.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241261211 – Supplemental material for ‘It was never about me’: A qualitative inquiry into the experiences of psychological support and perceived support needs of family caregivers of people with high-grade glioma
Supplemental material, sj-docx-1-pmj-10.1177_02692163241261211 for ‘It was never about me’: A qualitative inquiry into the experiences of psychological support and perceived support needs of family caregivers of people with high-grade glioma by Katarzyna M Lion, Anthony Jamieson, Abigail Billin, Stephanie Jones, Mark B Pinkham and Tamara Ownsworth in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank the study participants and the hospital and community organisations involved in recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study forms part of Brain cancer Rehabilitation, Assessment, Intervention of Survivor Needs (BRAINS), a program funded by a Medical Research Future Fund, 2019 Brain Cancer Survivorship Grant (ID: MRFBC000016).
Ethical approval
Ethical approval was obtained from Griffith University (HREC 2022/327) and Metro South Health (HREC/2022/QMS/83846) Human Research Ethics Committees in April–May 2022.
Data availability statement
Data are held securely by the research team and may be available upon reasonable request and with relevant approvals in place.
Supplemental material
Supplemental material for this article is available online.