
Abstract
Background:
Family caregivers play a crucial role in providing home palliative care for non-cancer patients with advanced illnesses. Given the complexity and heterogeneity of end-of-life caregiving experiences, there is a need to understand factors influencing caregiver outcomes for different profiles of caregivers. It is also crucial to consider the influence of cultural values on caregiving experiences, particularly in Asian settings.
Aim:
To explore the lived experiences of caregivers of non-cancer patients with advanced illnesses in Singapore.
Design:
A secondary qualitative analysis of transcripts from interviews conducted as part of a realist evaluation of a non-cancer home-based palliative care programme. Framework analysis was carried out using a combined theoretical framework to identify determinants, mediators and outcomes of caregiving. Analysis was stratified according to five caregiver profiles characterised based on the perceived burdens and benefits of caregiving.
Setting/participants:
Twenty interview transcripts of family caregivers of non-cancer patients with advanced illnesses were analysed.
Results:
Two, eight, three and seven family caregivers were profiled to have ‘Intensive’, ‘Balanced’, ‘Relationship’ and ‘Satisfied’ caregiving experiences respectively. Across all profiles, caregivers’ psychological outcomes were found to be more prominent than physical outcomes. Caregivers with ‘Intensive’’ and ‘Balanced’ profiles experienced greater caregiving intensity and poorer psychological well-being, as compared to caregivers with ‘Relationship’ and ‘Satisfied’ profiles. Caregiver appraisal and quality of relationship with others were found as key mitigating factors impacting caregiving demands on well-being.
Conclusions:
Insights gleaned from this study can be used to develop resources for home palliative providers, tailored to the different caregiving profiles.
Caregivers of patients with advanced illnesses may experience both burdens and benefits of caregiving. The outcomes of caregiving are influenced by different determinants, such as intensity of caregiving and mediators, such as caregiver appraisal and quality of relationship with others.
Determinants, mediators and outcomes of caregiving were identified for different profiles of caregivers of non-cancer patients with advanced illnesses in an Asian setting. Caregiver appraisal and the quality of relationship with others involved in the caregiving were key mediators mitigating the impact of caregiving demands on well-being.
Strategies to enhance caregiver appraisal and improve the relationship between caregivers, healthcare professionals and domestic helpers should be tailored for different profile of caregivers to support them.
Introduction
There is an increasing demand for home palliative care for non-cancer patients globally as patients with advanced illnesses opt to receive end-of-life care at home. 1 Family caregivers (subsequently referred to as caregivers) are the backbone of home palliative care and provide up to 80% of patient care at home, 2 including assisting patients’ activities of daily living and acting as proxy decision makers. 3 Yet, they are often overlooked by end-of-life care policies. 4 There is an imperative need to understand the experiences of caregivers to identify areas of unmet needs and inform policies and programmes to support them.4,5
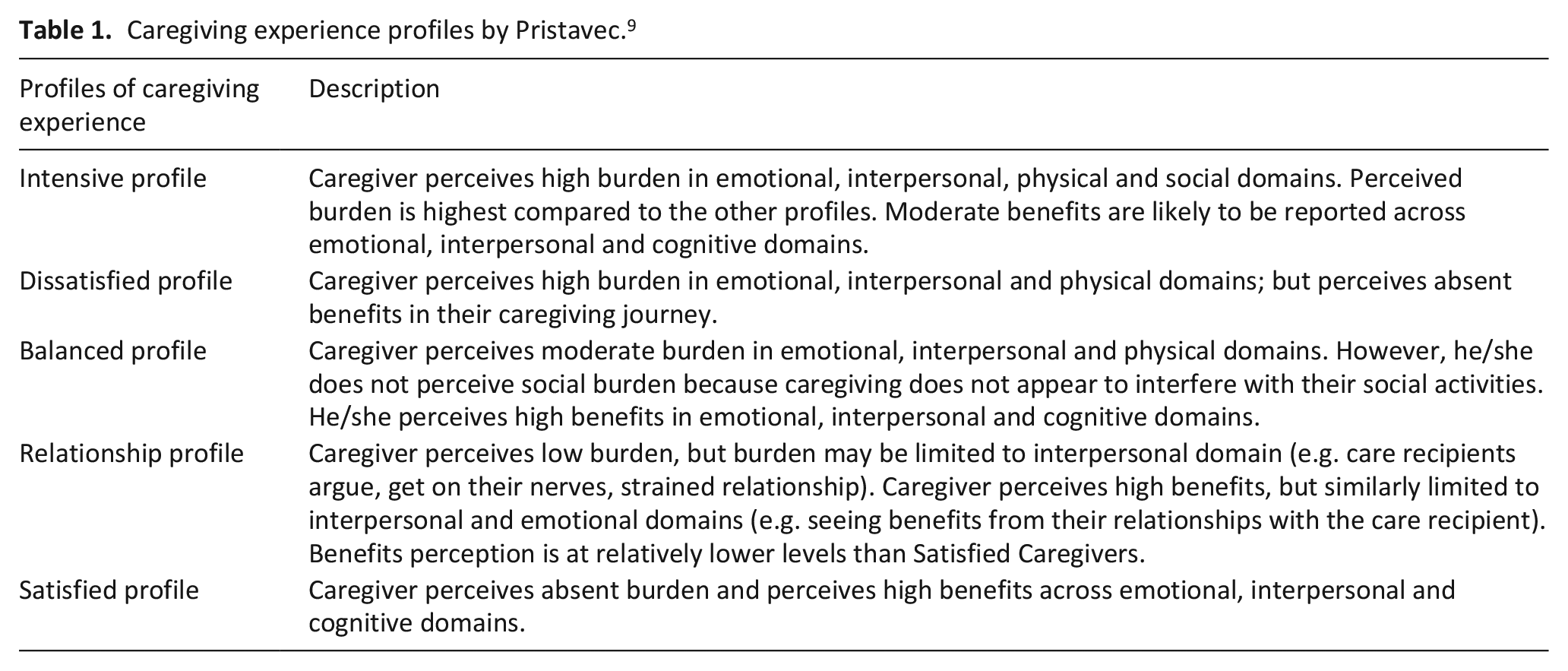
Caregiving for patients with advanced illnesses is a multifaceted and heterogenous experience. Different outcomes of caregiving have been reported, including negative outcomes such as anxiety, depression and low quality of life,6–8 and positive outcomes such as developing resilience and fostering a sense of accomplishment.8,9 Pristavec proposed five distinguishable types of caregiving experience profiles, which are characterised by different levels of co-existing burdens and benefits across several domains such as physical, emotional and interpersonal. 9 Descriptions of the five profiles, ‘Intensive’, ‘Dissatisfied’, ‘Balanced’, ‘Relationship’ and ‘Satisfied’, are detailed in Table 1 below.
Caregiving experience profiles by Pristavec. 9
There remains a gap in understanding the holistic experiences of each profile, particularly in identifying potential modifiable factors for targeted intervention. Factors that influence caregiving outcomes can be broadly categorised into determinants, which occur prior to and have an impact on outcomes, and mediators, which explain the processes by which determinants influence outcomes and are possible targets for intervention. The former includes the severity of patients’ symptoms 10 and motivations to be a caregiver, 11 while the latter includes the subjective appraisal of the caregiver and how the caregiver understands his situation. 12 These factors help researchers comprehensively understand the trajectories of caregiving experiences, 13 but have not been adequately studied for each caregiver profile.
Furthermore, the caregiving experiences in Asian contexts have been understudied. Caregiver burden is a significant problem in Asia where higher caregiver burden scores have been observed, as compared to non-Asian countries. 14 Among caregivers of patients with advanced illnesses, the prevalence of caregiver burden ranges from 68.6% in India, 15 47.4% in Malaysia, 16 to over 50% in Singapore. 10 This is worrying as caregiver burden not only affects the individual’s physical and mental well-being negatively, but also has far-reaching consequences on society, including reduced work productivity and increased healthcare resource utilisation among caregivers. 17
Caregiving in Singapore, a highly developed Asian country with a majority Chinese population, is fundamentally influenced by filial piety, a cultural value upholding respect, obedience and care towards one’s elders.3,18 There are societal expectations of family being the first line of support; Singaporeans often feel a sense of responsibility towards their sick family members. 3 In addition, due to shifting sociodemographic circumstances such as female participation in the workforce, more urbanised Asian countries like Singapore, Malaysia and Hong Kong are turning to employing live-in domestic helpers to assist in caring for elderly family members.19–21 Caregivers who had available informal paid help were found to have lower burden scores, showing that domestic helpers can help to provide respite for caregivers. 10 Nonetheless, the relationship and interactions between domestic helpers and caregivers and how this might affect caregiving experiences have not been adequately explored. 22 Given the sociocultural setting in Singapore, it is valuable to gain an in-depth understanding of the unique experiences of caregiving in the Asian context.
Prior research efforts have sought to identify different caregiving experience types in Singapore and their association with depressive symptoms and quality of life. 23 There has been lesser focus on identifying factors relevant for caregiving outcomes of different profiles of caregivers, which may be important targets for intervention. Therefore, this study aims to add to the growing body of knowledge on family caregiving in the Asian context by exploring the lived experiences of caregivers of non-cancer patients with advanced illnesses in Singapore. Specifically, we aim to answer the following research questions: (RQ1) What are the different profiles for caregivers of non-cancer patients with advanced illnesses in Singapore? (RQ2) What are the key determinants and mediators that affect outcomes of different profiles of caregivers?
Methods
The reporting methods are guided by the consolidated criteria for reporting qualitative studies (COREQ). 24
Study design
This study is a secondary qualitative analysis of a realist evaluation of the Violet Programme, a home-based palliative care programme for non-cancer patients with advanced illnesses in Singapore. 25 The main evaluation study was rooted in a realist philosophy: it subscribes to a post-positivist ontology, which recognises the researcher’s influence on interpreting reality, and a constructivist epistemology, which seeks to identify the meanings that humans give to experiences. 26 To explore lived experiences, we adopted a phenomenological approach, emphasizing openness, questioning preconceptions and having a reflective attitude. 27
Framework analysis was chosen as the qualitative method due to its structured approach in analysing data with a predetermined framework. 28 The chosen theoretical framework, described in a previous study, 22 combines the Informal Caregiving Integrative Model, 13 Inherent Tension of Caregiving, 29 and Risk and Resistance Model of Adjustment 30 to identify caregiver demands, resources and impact of the caregiving environment on outcomes (refer to Figure 1). These models were developed specifically to examine caregiving outcomes of family caregivers or encompassed key factors that were relevant for our study, thus were well-suited for the available data. An a priori template of codes was deductively derived from this combined framework, and inductive processes were also undertaken to generate codes from the data. This hybrid approach has demonstrated rigour in phenomenology studies, ensuring completeness in the analysis. 31
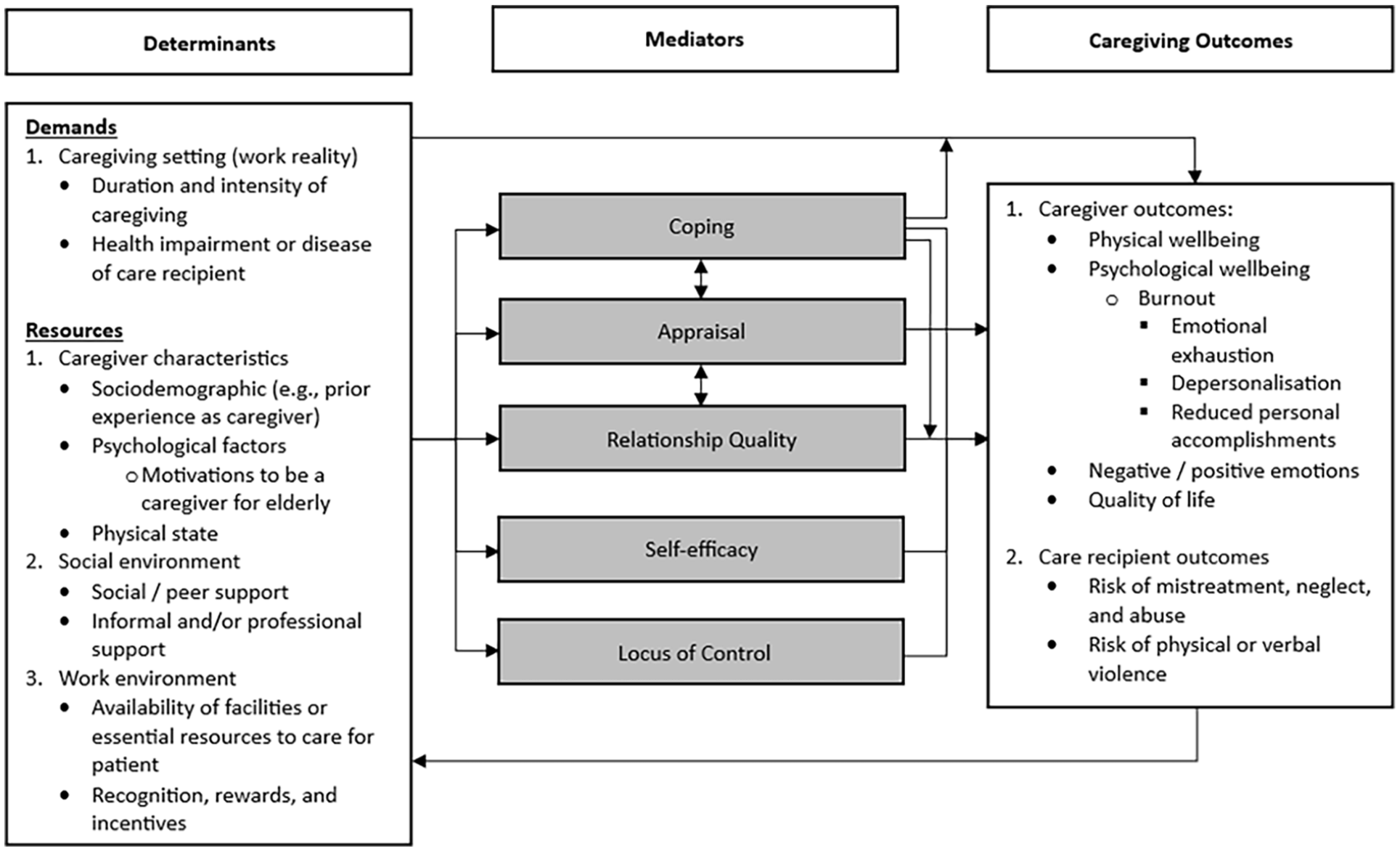
Combined theoretical framework for identifying the determinants, mediators and caregiving outcomes. 22
Recruitment and data collection
A text message was sent to caregivers of the Violet Programme patients through convenience sampling to invite them for an interview about their caregiving experiences. Thirteen caregivers agreed to participate, and one caregiver additionally recruited her sister to join her in a joint interview. Another seven caregivers were recruited through snowball sampling after recruiting their domestic helpers for the main evaluation study. In total, 21 caregivers participated in the study and 20 interviews were conducted (refer to Figure 2).
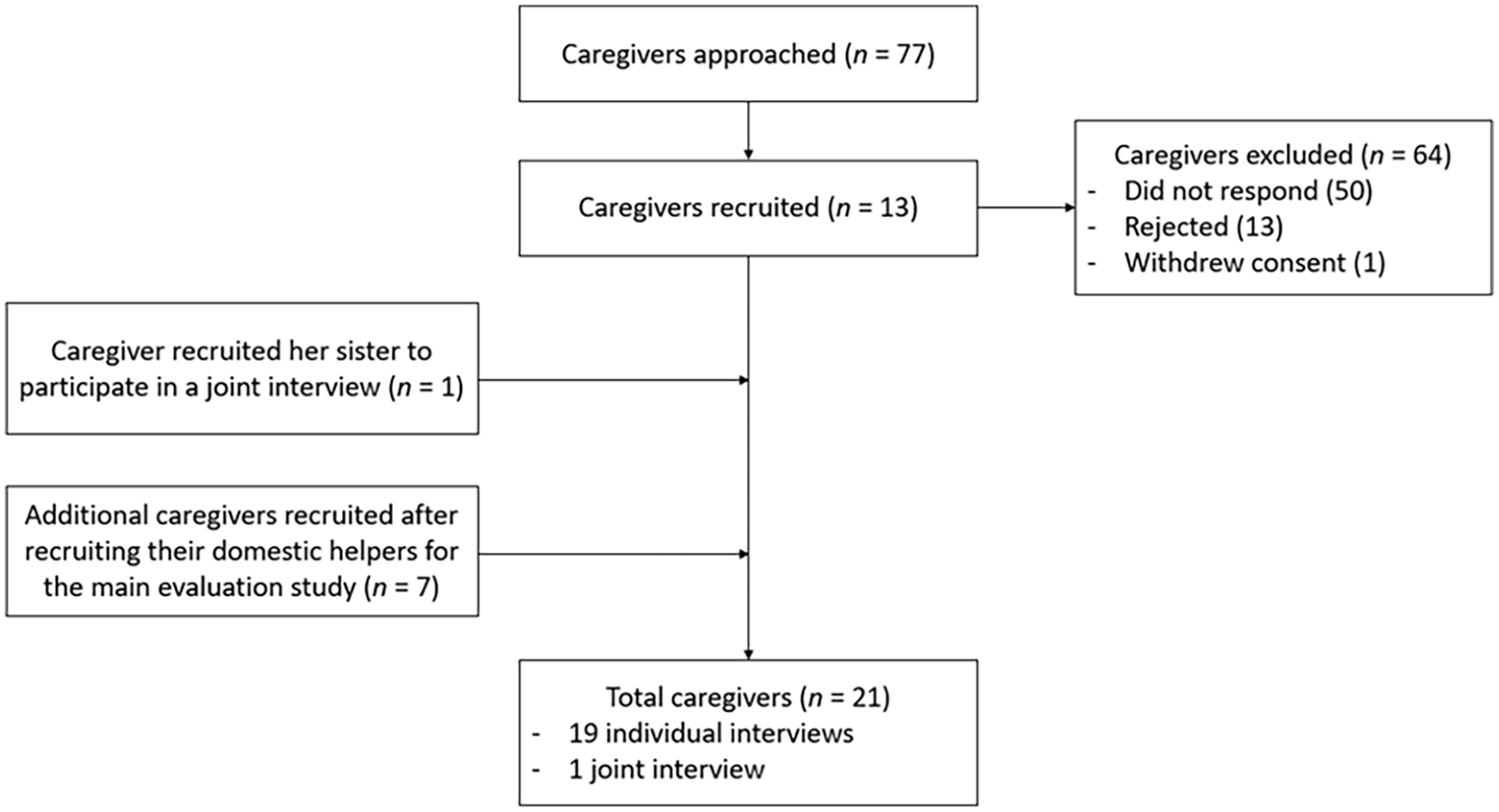
Flowchart of participant recruitment.
An interview guide for the main evaluation study was developed based on realist principles that aimed to elicit the context, mechanisms and outcomes of the programme 25 (refer to Annex 1). Semi-structured interviews were conducted by four public health researchers who are experienced in qualitative research on palliative care: MN (Female, MPH), EH (Male, MA), LJY (Female, BPsychSci (Hons)) and CT (Female, MScR). Researchers and participants were not mutually acquainted beforehand. To prevent possible biases, researchers were not involved in providing clinical services to participants. The interviews were conducted without repeats in English (n = 17) and Mandarin (n = 3) between May 2022 and February 2023, lasted between 22 and 82 min, and were conducted in a private space at the caregiver’s homes, in the hospital or over Zoom teleconferencing. Field notes were written during the interviews to help researchers engage in reflexive bracketing. 32 The interviews were audio-recorded and transcribed verbatim into English. The transcripts were not returned to participants for comments, nor did they provide feedback on the findings.
Data analysis
The original data collection yielded an appropriate and sufficient amount of data to address the aims of our secondary analysis. Clean, uncoded transcripts were coded using NVivo. Only parts of the transcripts that were related to caregiver experience were analysed. To ensure methodological rigour and credibility, investigator triangulation was achieved by involving several coders (LJY, MN, LKLK and TZAL). 33 Two transcripts were randomly selected and coded independently by all coders. Codes were compared and differences were resolved through discussion. An acceptable level of inter-rater reliability was achieved (Cohen’s kappa = 0.73). The rest of the transcripts were then coded independently. Throughout the analysis process, the data was coded in an iterative manner as regular meetings were held to refine codes and achieve a consensus. After coding was completed, each caregiver was qualitatively categorised into five different profiles of caregiving experience as described by Pristavec. 9
Research ethics
The SingHealth Centralised Institutional Review Board reviewed the study protocol (CIRB Ref: 2020/3039) and determined that further ethical deliberation was not required as it is a programme evaluation project. Written informed consent was obtained from participants prior to the interviews. Participation was entirely voluntary and participants were reimbursed for their time after completing the interviews. De-identified data was used for this analysis and accessible only to study team members to maintain the confidentiality of participants.
Results
Study participants by caregiving experience profile
Twenty interview transcripts of caregivers of non-cancer patients with advanced illnesses were included in this secondary analysis. Two, eight, three and seven caregivers were classified with ‘Intensive’, ‘Balanced’, ‘Relationship’ and ‘Satisfied’ profiles respectively. None of the caregivers were classified with a ‘Dissatisfied’ profile. Table 2 describes participants’ characteristics by caregiving profile.
Characteristics of family caregivers by caregiving profiles.
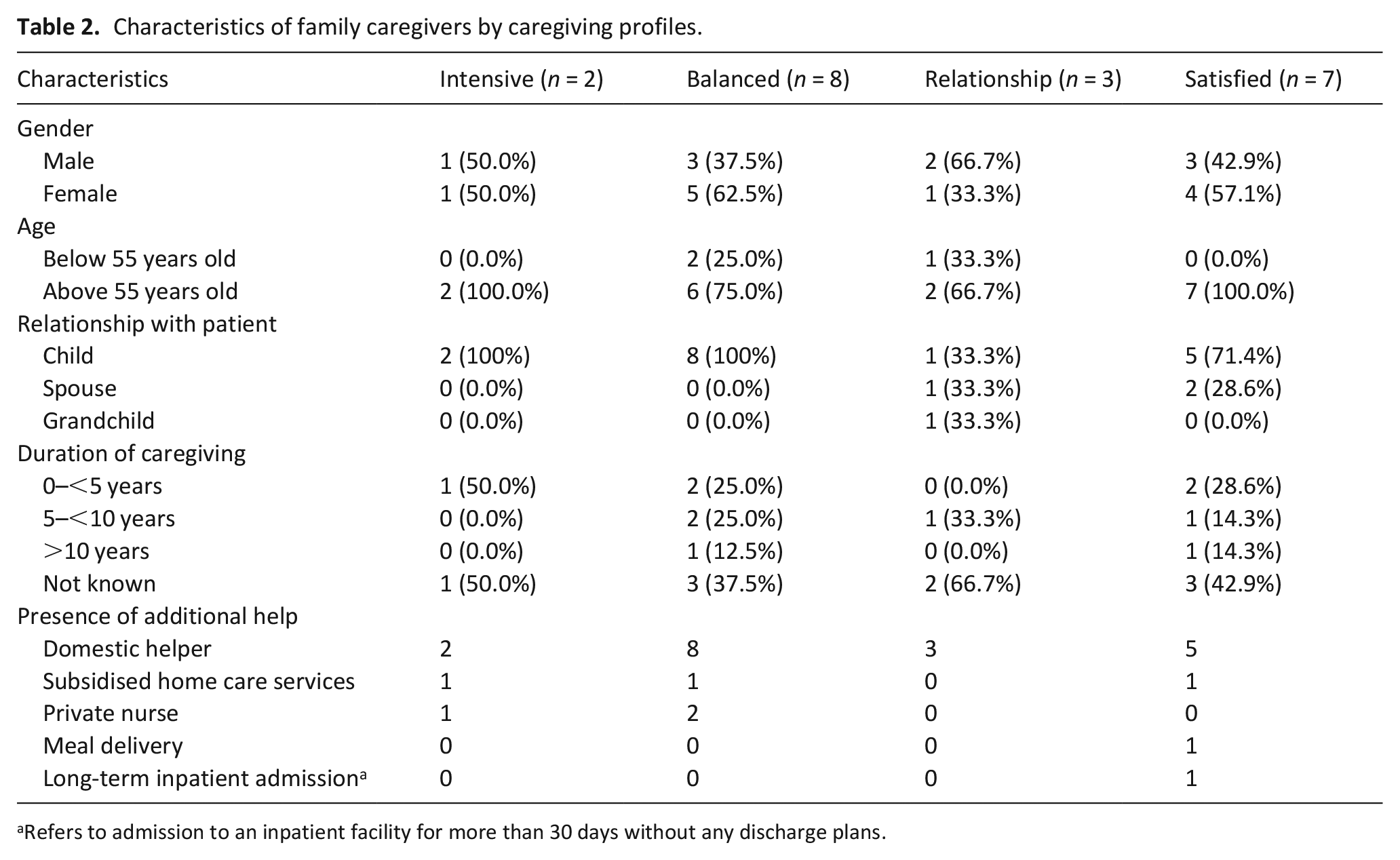
Refers to admission to an inpatient facility for more than 30 days without any discharge plans.
All caregivers and patients received professional home palliative care services which included home visits and access to an after-hours hotline. All caregivers received government financial subsidies to defray medical expenses. Caregivers with ‘Relationship’ and ‘Satisfied’ profiles had more robust social support, for example, being able to consistently rely on family members to help in the caregiving duties. Caregivers with ‘Intensive’ and ‘Balanced’ profiles used different coping strategies to manage the stress of caregiving, while those with ‘Relationship’ and ‘Satisfied’ profiles did not report using any coping strategies. All caregivers reported moderate levels of self-efficacy after receiving caregiver training from healthcare professionals. In general, caregivers’ psychological outcomes were found to be more prominent than physical outcomes. Figure 3 provides a summary of the determinants, mediators and outcomes by caregiver profiles. The following subsections describe each caregiver profile in detail.
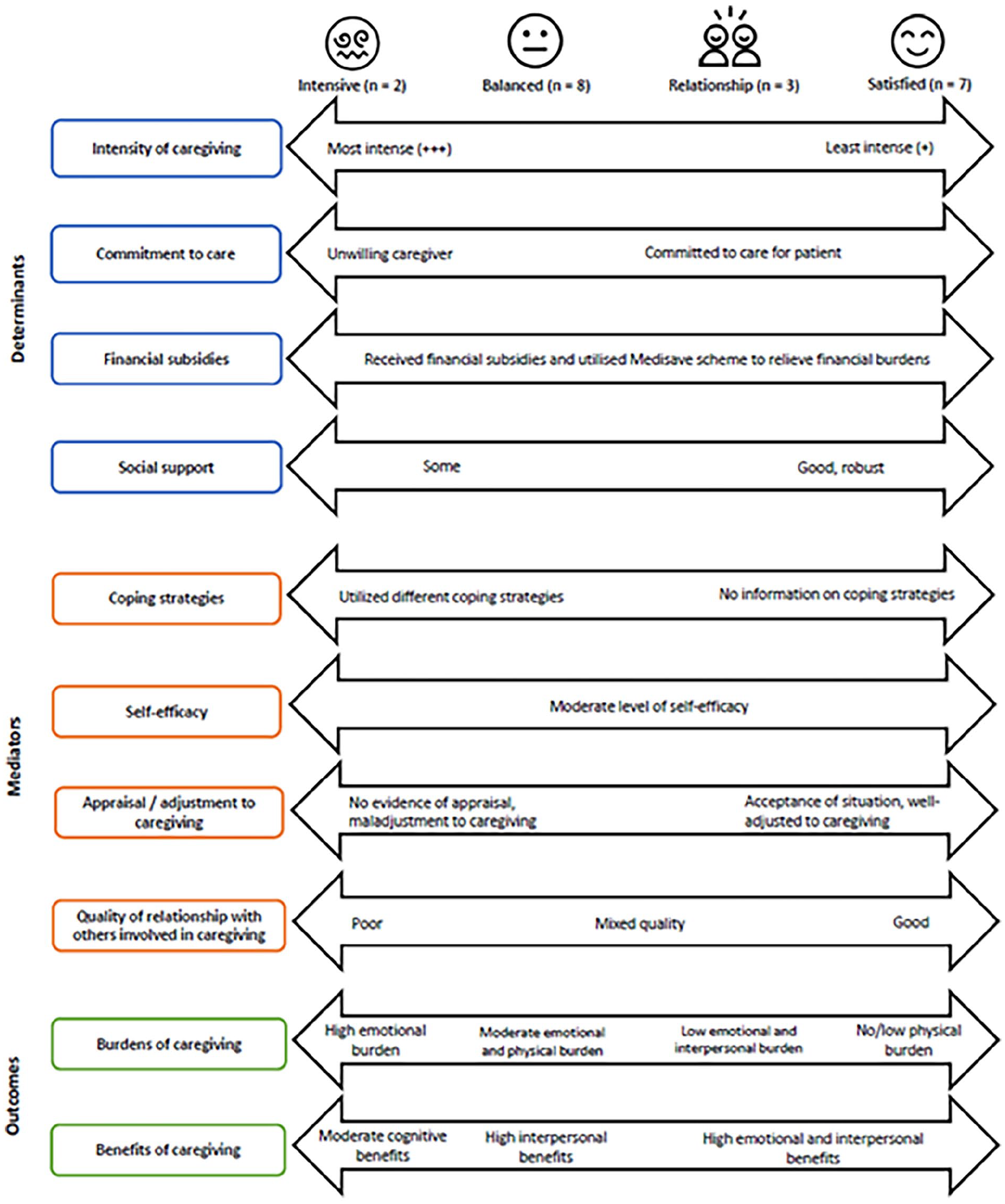
Summary of the determinants, mediators and outcomes of caregiving by caregiver profiles.
‘Intensive’ caregivers
Caregivers with an ‘Intensive’ profile faced the highest intensity of caregiving in the physical, emotional and interpersonal domains. Patients’ frequent night awakenings reportedly caused anxiety and insomnia in caregivers. Caregivers also felt forced to take up the caregiving role and perceived a lack of choice given their family circumstance.
I I have been taking care of my parents for years. . . There’s no one left. It is usually left to the singles to take care of their parents.
Caregivers described maladjustment to their caregiving roles and struggled in managing the immense responsibilities. They also had poor and strained relationships with their domestic helpers, perceiving them to be more of a burden than a help; and healthcare professionals, perceiving them to be unempathetic and lacking understanding.
I cannot monitor [my domestic helper]. . . She’s very strongheaded and stubborn-headed. She wants to do her way. . . So this is something I’m struggling with. (C033, child, “Intensive” profile)
They experienced the poorest psychological well-being and greatest emotional exhaustion amongst all the caregivers.
At that point,
‘Balanced’ caregivers
Caregivers with a ‘Balanced’ profile faced moderate intensity in caregiving. They felt physically tired, as many were elderly themselves. These caregivers exhibited strong motivation and commitment to care for the patient and took on the caregiving role willingly.
To me, it’s a duty of love, it’s not like a job.
Importantly, they appraised the caregiving situation positively and viewed challenges as opportunities for learning and growth. This motivated them to take active steps to overcome the difficulties in caregiving. Caregivers also turned to different strategies such as setting priorities and having personal relaxation time to cope with the caregiving demands, helping them to adjust well to the caregiving role.
Caregivers had mixed experiences with others involved in the caregiving. Some had negative experiences with their domestic helpers, encountering problems such as illegal money borrowing. Others perceived their domestic helpers to be a great help and were grateful for the close relationship they had with the patient. Similarly, some caregivers were satisfied with the services provided by healthcare professionals while others felt that more could have been done, such as more regular home visits.
We had a helper for seven months. . . but [she] gave us lots of problem. . .
Given the demands of caregiving, these caregivers experienced moderate levels of emotional and physical exhaustion, which negatively affected their psychological well-being.
Honestly. . . if I’m alone, doing it alone,
‘Relationship’ caregivers
Caregivers with a ‘Relationship’ profile faced low intensity of caregiving in the physical domain of care. They did not face many problems and were able to manage the responsibilities of caregiving. They also felt an obligation to care for the patient, which helped to maintain their commitment to care.
Actually, there’s nothing much to do for my wife. . . The only thing is when giving her a shower and changing her diapers, you need at least two [persons]. . .
These caregivers were well-adjusted to the caregiving role. They had a positive and realistic appraisal of their role as a caregiver and the realities of the patients’ medical condition.
I didn’t expect that time that my wife’s condition will deteriorate. So, I was hoping that time that it [was] just some kind of sickness that it can be cured. . . But since she deteriorated like that and then with the advice from the hospital, the nurses, doctors,
These caregivers shared a good and close relationship with their domestic helpers. This aided their caregiving journey greatly as they could count on their domestic helpers as a reliable source of help. However, they had mixed relationships with healthcare professionals: some were satisfied with the services while others voiced their dissatisfaction with the lack of professionalism.
Then the last round I was very unhappy. . . Suddenly [my mother had] a lot of phlegm. . . And I urgently called the [hotline]. . .
In general, caregivers felt stressed when caring for the patient, and experienced reduced quality of life due to sacrificing their personal time. This had some negative impact on their psychological well-being.
[I cannot do] certain things like important matters that I have to attend to outside. . .
‘Satisfied’ caregivers
Like caregivers with a ‘Relationship’ profile, caregivers with a ‘Satisfied’ Profile faced low intensity of caregiving in the physical domain of care. They showed a resolute commitment to care for the patient, such as giving up their jobs to take on a full-time caregiver role.
These caregivers showed a realistic appraisal and acceptance of the patient’s condition, helping them to adjust well to the caregiving role. They also enjoyed good and close relationships with their domestic helpers and healthcare professionals. Their domestic helpers took on a sizeable share of the caregiving load, which was a great source of help and relieved their stress. Caregivers also noted that the personable nature of the healthcare professionals was important to them, and it helped to foster a collaborative working relationship with the care team.
I’m very confident that [the domestic helper] can handle, because she’s with ah ma (grandmother) [for] so long already. . . She also knows how to call the nurse, call the doctor.
As most of the caregiving duties were shared or taken by other parties such as the domestic helper or the healthcare professionals from the inpatient ward, these caregivers enjoyed the highest level of psychological well-being.
We are also happy. I mean, knowing that she is taken care of. I mean it is a
Discussion
In this secondary qualitative analysis, we explored the lived experiences of caregivers of non-cancer patients with advanced illnesses in Singapore, and identified key determinants, mediators and outcomes of caregiving that characterised the different profiles of caregivers. Caregivers with an ‘Intensive’ profile faced the greatest demands of caregiving, had poor quality of relationships with others, and reported the poorest psychological well-being. This concurs with the Informal Caregiving Integrative Model where demands from the caregiving setting, negative appraisals and poor relationship quality are expected to result in intense emotional exhaustion and caregiver burnout. 13
Caregivers with a ‘Balanced’ profile faced moderate intensity of caregiving, but this was buffered by a positive appraisal of the situation and commitment to care for the patient out of love. They had mixed quality of relationships with others and moderate levels of emotional exhaustion which negatively affected their psychological well-being. These findings support the Inherent Tension of Caregiving framework which posits that the coexistence of reasons to care and burdens of care results in caregiver stress. 29 Nonetheless, their motivations to express love and gratitude to the patient exemplified filial piety, allowing them to find meaning in the caregiving journey. 11
Caregivers with a ‘Relationship’ profile faced low intensity of caregiving and were well-adjusted to the caregiving role, but experienced some negative impact on their psychological well-being. Caregivers with a ‘Satisfied’ profile had the lowest intensity of caregiving, were realistic and accepting of the patient’s condition, and had the highest level of psychological well-being. Caregivers with these two profiles showed commitment to care and exhibited filial piety, which contributed to a nurturance of caregiver well-being. 11 The quality of relationship with domestic helpers was also shown to be a crucial dimension that affects caregivers’ psychological outcomes: caregivers with ‘Relationship’ and ‘Satisfied’ profiles who had good relationships with their domestic helpers had better psychological outcomes, compared to caregivers with ‘Intensive’ profiles who had poor relationships with their domestic helpers.
Implications for clinical practice
The key mediators found in our study were caregiver appraisal and quality of relationship with others involved in the caregiving, and tailored strategies can be proposed for different profiles of caregivers. Strategies to improve caregiver appraisal are appropriate for caregivers with ‘Intensive’ profile who experienced difficulties in adjusting to their caregiver situation. Short term strategies that can be achieved within a short time frame of weeks to months include improving caregivers’ coping skills, meeting any unmet needs, 34 and having healthcare professionals share medical information in a sensitive and timely manner. 35 Long term strategies that target larger objectives and span across years include reducing social stigma for illnesses like dementia 34 and fostering a culture of openness towards death, which is especially important in Asian settings where death is viewed as a ‘taboo’. Having positive attitudes towards death may improve caregivers’ appraisal of the patient’s situation and foster acceptance rather than denial of the end-of-life process, making the caregiving journey more meaningful.
Strategies to improve the quality of relationship between caregivers and domestic helpers are appropriate for caregivers with ‘Intensive’ and ‘Balanced’ profiles who had poor relationship with their helpers. This can include enhancing domestic helpers’ individual coping strategies and leveraging on their personal resources to help them cope better with the demands of caregiving. 22 This would improve the quality of care they deliver, assuring caregivers of their competence. 22
Strategies to improve the quality of relationship between caregivers and healthcare professionals are appropriate for caregivers with ‘Intensive’, ‘Balanced’ and ‘Relationship’ profiles. Short term strategies include training for healthcare professionals to improve their competence in end-of-life communication skills, as many providers feel uncomfortable discussing end-of-life issues.36,37 Long term strategies include increasing public awareness and legitimation of palliative care services to improve the collaboration between caregivers and healthcare professionals. 38
Strengths and limitations
A key strength of this study is the use of a robust theoretical framework which underpinned the data analysis. Integrating elements from the Informal Caregiving Integrative Model, the Inherent Tension of Caregiving and the Risk and Resistance Model of Adjustment ensured a comprehensive analysis of the determinants and mediators that influenced caregiver outcomes. Another strength is the use of existing data, which allows us to generate new insights in a highly efficient manner.
However, we acknowledge selection bias as a limitation as caregivers who responded to our invitation might have had more positive caregiving experiences and would be more willing to participate in the study. This can be seen by how none of the caregivers had a ‘Dissatisfied’ profile. Generalisability is also limited as the sample of caregivers have all received professional help under the Violet Programme.
Recommendation for future research
Our findings highlight the influence of culture on caregiving experiences. Our study concurs with previous research that demonstrates that cultural values of filial piety as motivation to care for family members may have both positive and negative impacts on caregivers.3,11 These findings may be transferable to other Asian countries or regions with large Asian populations which similarly endorse values of filial piety and where family caregiving is the norm. 14 The profiles of caregivers and the experiences they face are likely to be comparable, hence similar strategies to target the mediators might be applicable as well. Further research is warranted for other Asian regions which are dissimilar to Singapore, such as rural areas with fewer support and healthcare services available. 39 Understanding the experiences of caregivers in rural areas and identifying similarities and differences to urban areas will inform the different types and level of support needed for caregivers in different settings. Cross-country learning can also be facilitated to draw on the strengths of different Asian countries. 40
Conclusion
This study provides valuable insights into the unique caregiving experiences of different profiles of caregivers caring for non-cancer patients with advanced illnesses in an Asian context. The findings have also demonstrated the complex interplay of determinants and mediators for each profile of caregiver and its influence on caregiving outcomes. A rich understanding of the diverse caregiving experiences can foster deeper empathy for caregivers and guide palliative providers to deliver tailored care to the different profiles of caregivers and their loved ones.
Footnotes
Annex 1: Topic guide for interview with caregivers (English)
In today’s interview, we are going to ask you about your experiences with the Violet Programme (ViP) Home Palliative team. Please note that there are no right or wrong answers, and your responses will be kept confidential.
Acknowledgements
The authors would like to thank Charlotte Tan and Ezra Ho for helping to conduct the interviews and study participants for sharing their experiences.
Author contributions
MN conceptualised and designed this study. LJY, MN, LKLK and TZAL analysed the data. TZAL and MN drafted the first and final version of the manuscript. All authors read, provided suggestions for revision and approved the final manuscript.
Data management and sharing
Anonymised data will be made available upon request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LKLK, LOKA and KLH are directly involved in the provision of care for individuals enrolled in the Violet Programme. All authors declare that there are no other competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 10th Singapore Millenia Foundation (SMF) grant awarded by Temasek Foundation, Singapore. The publication of this work is supported by the National Medical Research Council (NMRC) through the SingHealth PULSES II Centre Grant (CG21APR1013). Funders have no role in the design of the study and writing the manuscript.