
Abstract
Background:
Deaths of people with intellectual disabilities are often unplanned for and poorly managed. Little is known about how to involve people with intellectual disabilities in end-of-life care planning.
Aim:
To explore the perspectives of people with intellectual disabilities, families, health and social care professionals and policy makers on end-of-life care planning within intellectual disability services.
Design:
A total of 11 focus groups and 1 semi-structured interview were analysed using qualitative framework and matrix analysis. The analysis was conducted inclusively with co-researchers with intellectual disabilities.
Setting/participants:
A total of 60 participants (14 people with intellectual disabilities, 9 family carers, 21 intellectual disability professionals, 8 healthcare professionals and 8 policy makers) from the UK.
Results:
There were differences in how end-of-life care planning was understood by stakeholder groups, covering four areas: funeral planning, illness planning, planning for living and talking about dying. This impacted when end-of-life care planning should happen and with whom. Participants agreed that end-of-life care planning was important, and most wanted to be involved, but in practice discussions were postponed. Barriers included issues with understanding, how or when to initiate the topic and a reluctance to talk about dying.
Conclusions:
To develop effective interventions and resources aiding end-of-life care planning with people with intellectual disabilities, clarity is needed around what is being planned for, with whom and when. Research and development are needed into supporting intellectual disability staff in end-of-life care planning conversations. Collaboration between intellectual disability staff and palliative care services may facilitate timely end-of-life care planning and thus optimal palliative end-of-life care.
Deaths of people with intellectual disabilities are often unanticipated, unplanned for and poorly managed.
Service providers in residential settings are at the forefront of supporting people with intellectual disabilities at the end-of-life, but staff lack skills, knowledge, confidence and support within the area.
In order to develop end-of-life care planning interventions that are welcomed by people with intellectual disabilities, their families and support staff, it is important to understand their perspectives, preferences and needs for end-of-life care planning.
Participant perspectives provided a detailed view of end-of-life care planning involving four areas ([i] funeral planning, [ii] illness planning, [iii] life planning and [iv] talking about dying); what area participants focused on affected their views on whether, when and with whose input they thought end-of-life care planning should happen.
Barriers to end-of-life care planning with people with intellectual disabilities included: reluctance to consider death and dying, with a preference to focus on ‘planning for living’; issues around understanding and communication; not knowing how to initiate conversations; dying being an abstract concept; and lack of staff training.
Planning for illness (the last phase of life) was particularly abstract and difficult to do in advance.
The definition of end-of-life care planning may be ambiguous, particularly for non-healthcare professionals. It should be clear what is meant and understood by people when using the term.
The development of future interventions, resources and approaches for end-of-life care planning with people with intellectual disabilities should address the need for clarity around what is being planned for.
Intellectual disability staff need help and guidance in knowing when and how to initiate the topic of dying and end-of-life care planning; reframing aspects of end-of-life care planning as ‘planning for living’ rather than ‘planning for dying’ and collaboration with palliative care professionals may help address barriers.
Background
Many people with intellectual disabilities have complex care needs and are at risk of health inequalities and premature death. 1 Their deaths are often unanticipated, 2 unplanned for and poorly managed. 3
Advance Care Planning may be a way to address this. It is a voluntary process of person-centred discussions about goals, values, preferences and priorities for future care, so that personal views inform care plans as the person approaches the end-of-life. Discussions should happen over time between the care provider, the person and those important to them, 4 and are associated with improved quality of life, reduced life-sustaining treatment, earlier hospice referrals and care aligned with patient preferences. 5
An investigation of the deaths of people with intellectual disabilities in England found that the majority lived in an intellectual disability care setting at the time of death. 6 These service providers are therefore at the forefront of supporting people at the end-of-life, but they lack expertise, skills, knowledge and confidence in this area. 7
This study originated following questions posed by two UK intellectual disability service providers, Dimensions and MacIntyre, who between them support over 5000 people. Managers were aware of requirements to involve people in end-of-life care planning but were unclear about how to achieve this. The terminology used by these service providers was ‘End-of-life Care Planning’ rather than ‘Advance Care Planning’, in line with the Care Quality Commission (England’s independent health and social care regulator and inspector). 8
Reviews and inquiries recommend that services do end-of-life care planning, involving people with intellectual disabilities and families.6,9 However, communication difficulties, capacity issues and a death avoidance culture often prevent this.7,10,11 There is also no guidance on what their involvement should look like. 12 Moreover, there are no studies evaluating the effectiveness of end-of-life care planning or the processes for following the wishes of people with intellectual disabilities about their end-of-life care decisions. 9
Aims
To explore the perspectives of people with intellectual disabilities, families, health and social care professionals and policy makers on end-of-life care planning within intellectual disability services.
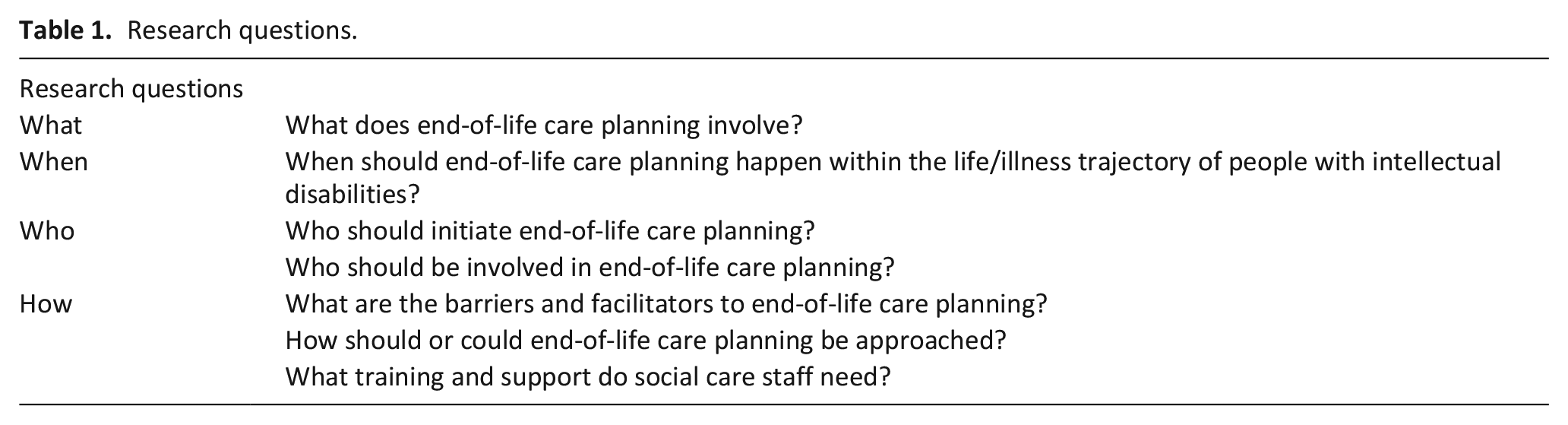
The research questions are listed in Table 1.
Research questions.
This study was the second stage in a project aiming to co-produce resources for end-of-life care planning with people with intellectual disabilities within social care settings. The first stage involved an evidence review of end-of-life care planning resources and approaches.
Methods
Study design
A co-produced focus group study with a phenomenological research design, with content analysis using the framework method. 13 The Consolidated Criteria for Reporting Qualitative Research was followed. 14
Research team
The research team comprised a Professor [IT-W] with 20+ years experience in end-of-life research involving people with intellectual disabilities; three Research Associates [AB, RA-K and SG] with experience in co-producing qualitative research including within palliative care; three Research Assistants with intellectual disabilities [AC, RK-B and LJ] 15 with some research training 16 and end-of-life research experience (15, 2 and 1 years respectively); and a Research Assistant [JG], with end-of-life experience, supporting them. All were involved in data collection and analysis.
Collaborators were Dimensions and MacIntyre. The study was supported by a Research Advisory Group involving a range of stakeholders.
Population
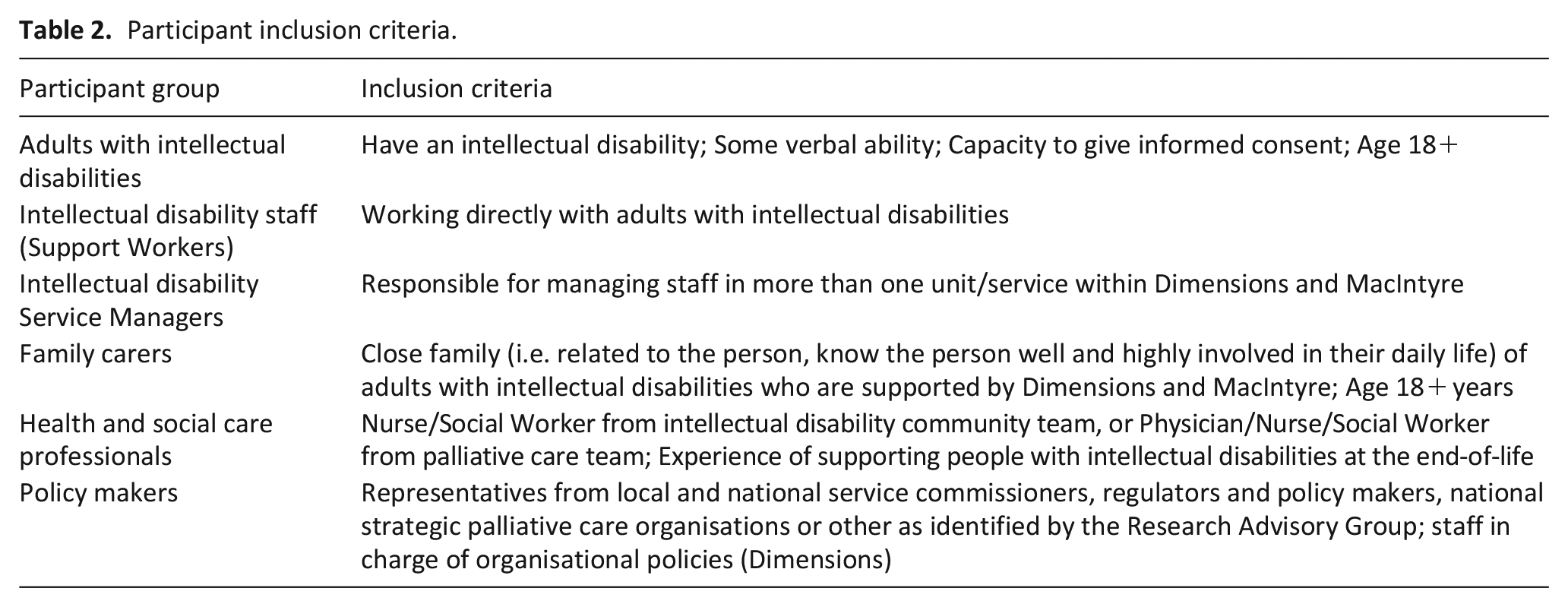
Participants were adults with intellectual disabilities, family carers, intellectual disability staff, health and social care professionals and policy makers. Table 2 describes the inclusion criteria.
Participant inclusion criteria.
Setting
Intellectual disability service providers in England.
Sample
Participants were purposively selected to take part in single-stakeholder focus groups.
Recruitment
Dimensions and MacIntyre circulated study information to potential participants. Informed consent was obtained by the researchers. Researchers contacted potential health and social care professionals and policy makers via email, following suggestions from the Research Advisory Group.
Study information was in easy-read for people with intellectual disabilities and included an information video for everyone.
Data collection
Topic guides centred around the research questions in Table 1 and can be found in Supplemental File 1.
Data collection tools for focus groups with people with intellectual disabilities were developed, piloted with three groups of people with intellectual disabilities (n = 16) and refined together with researchers with intellectual disabilities. Questions were framed as ‘games’ (e.g. picture-based storytelling 17 ).
Two focus groups with people with intellectual disabilities involved two 2-h sessions over one or two days, held in a local community venue and a private café space. Non-research participant Support Workers were present for support. One focus group with people with intellectual disabilities was held on Zoom (4 h). These groups were facilitated by four researchers, including one researcher with intellectual disabilities. All other groups were held on Zoom (2 h) and facilitated by one or two researchers.
Sessions were video-recorded, and researchers wrote field notes during and/or after each session. Researchers with intellectual disabilities discussed their thoughts with colleagues and those were added to the notes.
Data were collected from August to December 2022.
Data analysis
Video-recordings were transcribed verbatim. Analysis involved all researchers and a co-production group with people with intellectual disabilities, support staff, families and health and social care professionals.
Content analysis following the framework method was applied, which has the advantage of being adaptable and allowing engagement of people without qualitative research experience. 13 The method was adapted to enable inclusive team discussions.
A matrix of deductive codes was produced based on the topic guides (Supplemental File 2). Following discussions about each focus group, one researcher populated the sections and inductive codes were added. Transcripts were read by two researchers to check that all themes were represented in the analysis. One researcher re-watched recordings for verification and extraction of key quotes. Thematic saturation was reached, as no new themes were identified from the final focus groups.
Preliminary analyses were presented to the co-production group and the Research Advisory Group for discussion and agreement.
Results
A total of 60 participants participated in 11 focus groups and one individual interview. Table 3 describes participants’ demographics.
Participants’ demographics.
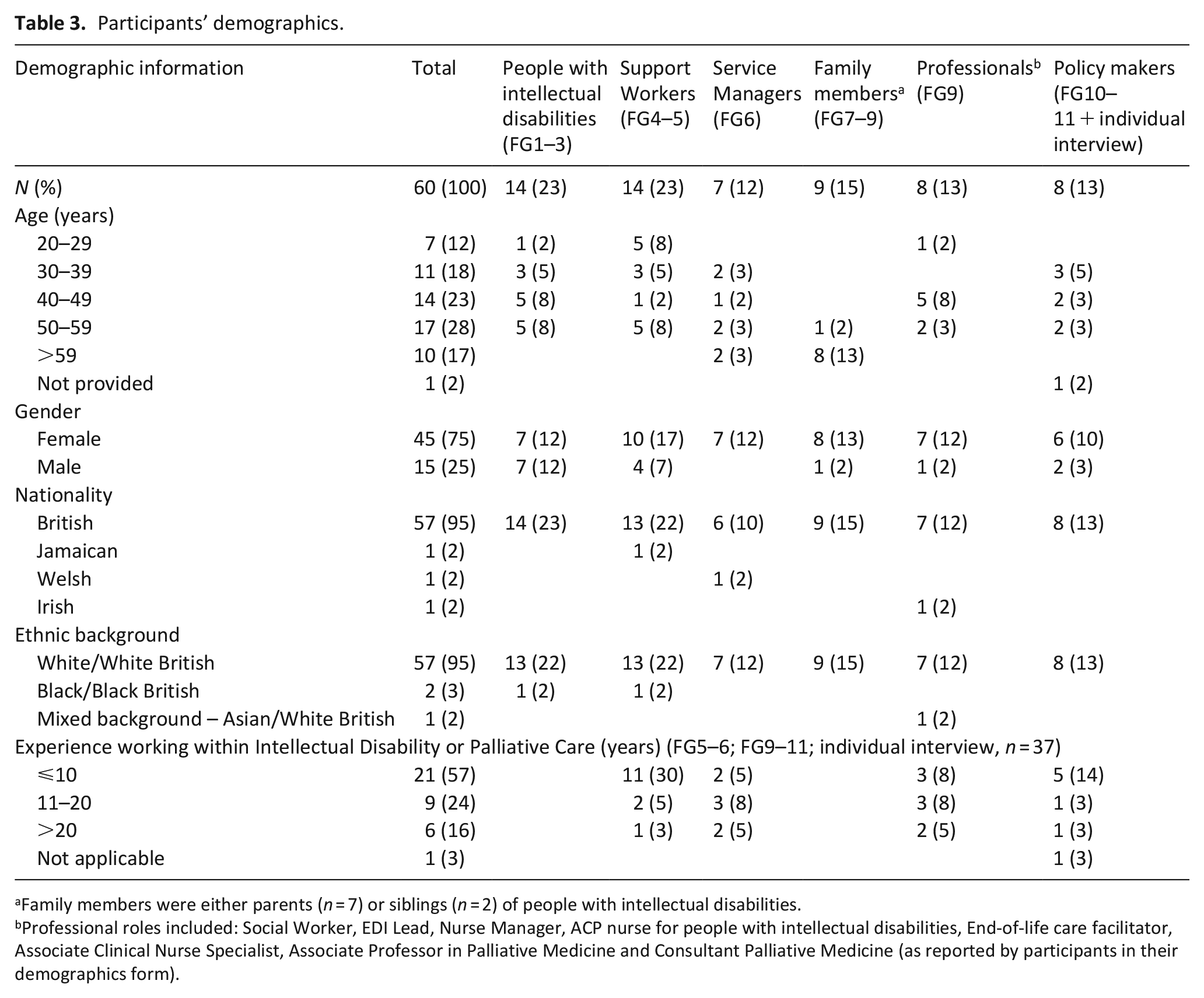
Family members were either parents (n = 7) or siblings (n = 2) of people with intellectual disabilities.
Professional roles included: Social Worker, EDI Lead, Nurse Manager, ACP nurse for people with intellectual disabilities, End-of-life care facilitator, Associate Clinical Nurse Specialist, Associate Professor in Palliative Medicine and Consultant Palliative Medicine (as reported by participants in their demographics form).
The main themes identified from the matrix template domains are presented based on the research questions and illustrated by participant quotes.
Importance of end-of-life care planning (why)
Some participants indicated that not all people with intellectual disabilities want to be involved in end-of-life care planning. However, participants agreed that end-of-life care planning was important to ensure that wishes were respected. People with intellectual disabilities stressed that they wanted to be involved and have choice and control of their lives.
Past experience tells us that people with a learning disability have things done to them, and decisions made about them without even asking them. So, I definitely think that they need it to be there to be offered if they wish it.
(Intellectual disability Service Manager, M507)
Participants described difficult situations where decisions had to be made where end-of-life care planning had not occurred.
Defining end-of-life care planning (what)
Participants described four aspects of end-of-life care planning: (i) funeral planning, (ii) terminal illness planning, (iii) life planning and (iv) talking about dying.
Funeral planning
Most people with intellectual disabilities, families and support staff focused on funerals when defining end-of-life care planning.
Is he going to get cremated or buried?
(Person with intellectual disabilities, L2b01)
They described decisions around what happens after death, rather than care at the end-of-life.
Planning for illness
Health and social care professionals had the strongest focus on care at the end-of-life, although most other participant groups also acknowledged this aspect. They mentioned aspects such as where to be cared for, pain management and who should care for them. Family members (particularly those supporting someone with severe/profound intellectual disabilities) explained why this was important.
I always think about the physical aspect of it really you know how is [my son] going to be cared for when he’s clearly dying. He’s terrified of hospitals and refuses to go to hospitals actually, unless he sort of absolutely has to. So, my dread is that he would die in a hospital surrounded by people he doesn’t know.
(Mother, F604)
Planning for living
When describing decisions relevant to funeral planning and illness planning, participants also expressed the importance of knowing how someone wants to live their life and what matters to them. Healthcare professionals identified this as a key aspect of end-of-life care planning.
It’s more about. How do you want to live the rest of your life? What’s important to you? What do you want? What do you think other people need to know about you to be able to give you the care that you need?
(End-of-life Facilitator, H805)
Talking about dying
It was apparent that end-of-life care planning involved talking about dying, and was difficult to do without introducing the topic of death. It was important to elicit the person’s experience and understanding of death. However, this was not always easy for staff.
When I was at school there was a big conversation about death and a lot of us were quite scared about it.
(Support Worker, S306)
The challenging nature of talking about dying presented a major barrier.
Timing (when)
People with intellectual disabilities, families and support staff all expressed that end-of-life care planning should be done as early as possible, as the future was uncertain and unexpected events may happen.
Yeah, I really do, because none of us know what’s around the corner. None of us.
(Mother, F703)
Participants were concerned that if no plans were in place, things could go wrong. Planning ensured that the person’s wishes could be respected, particularly if they could no longer speak for themself.
Whilst many people with intellectual disabilities wanted to be involved, most thought that now was too early.
I want to do it but not yet. I’ve got a lot more life in me yet.
(Person with intellectual disabilities, L2a04)
Other participants shared this concern and further noted it was important to review decisions to reflect changes in preferences.
Timing dependent on end-of-life-care planning aspect
Timing depended on the area being discussed. Funerals were something concrete that most participants were able think about, including those with intellectual disabilities. However, illness decisions were more complex to make in advance. The healthcare professionals acknowledged this difficulty.
I think the word advance is really problematic. Because actually nobody does it in advance, or they do it like, you know thirty seconds in advance.
(Associate Professor and Consultant in Palliative Medicine, H807)
Participants thought that life planning should be done throughout life and not only at the end-of-life. They mentioned person-centred support plans and to update these annually.
People involved (who)
Participants listed a variety of people who should be involved in end-of-life care planning. People with intellectual disabilities were clear about who they wanted involved, mostly family and carers.
I would talk to support staff, but I would also talk to my mum and my family.
(Person with intellectual disabilities, L2a01)
Family members wanted to be involved but acknowledged that end-of-life care planning is done with key Support Workers. Support staff said their involvement was crucial as they were highly involved in the daily lives of people they support and therefore knew them well. Ultimately, end-of-life care planning was seen as management’s responsibility. Families and intellectual disability professionals only mentioned healthcare professionals in relation to ‘illness planning’, where they were deemed important.
Relationship with the person
Quality of the relationship with the person with intellectual disabilities was crucial regarding someone’s involvement in end-of-life care planning. Knowing the person well was seen as essential. This was particularly important if the person had severe/profound intellectual disabilities.
She desperately needs staff who know her really, really well. She’s no language. She doesn’t demonstrate pain. So, you’ve really got to look very hard at what is going on.
(Mother, F702)
Trust was also essential to have sensitive end-of-life care planning conversations.
The process (how)
People with intellectual disabilities may need end-of-life care planning discussion in inclusive formats with accessible information adapting to their individual understanding and communication needs. They preferred creative and fun activities such as games, also reflecting the applied focus group methodology. Other groups also listed visual and creative ways such as videos and picture stories.
Participants described how using opportunities and events such as a relative dying could open the discussion and be used to elicit end-of-life care preferences.
I think this year it’s been a bit easier to approach the subject, especially with the Queen’s passing. I think that’s sort of like helped. I don’t mean this horribly, but that’s helped quite a lot for people to think about what they want.
(Intellectual disability Service Manager, M503)
Barriers and facilitators
Barriers
Communication
The main barrier was the sensitive and emotional aspect of the topic, where it was seen as scary, difficult and upsetting by support staff. People with intellectual disabilities also expressed that they were not given opportunities to talk about dying.
This is a very first time, and we don’t speak about dying very much. So, to get it out. It’s quite a good thing.
(Person with intellectual disabilities, L2b02)
Some family members shared concerns about including people with intellectual disabilities in these discussions because of issues with understanding death. They worried about the emotional aspect and a potential ‘hyperfocus’ on death. Some families could never imagine themselves having these conversations with their relatives.
I think it’s probably better for him not to know, because one of his major anxieties is people, is death, because of what death means. But he, when he WhatsApps me each day, it’s always so and so’s died, so and so’s died, so and so is not going to die. You’re not going to die. So, it’s there as a real anxiety. And I think it’s because he doesn’t understand it.
(Mother, F604)
Death as a complicated, abstract concept was also highlighted. Communication needs could also present challenges, particularly for people with autism, who may need unambiguous language and may find uncertain futures difficult to understand.
Initiating the conversation
Participants were unsure who should initiate end-of-life care planning.
Often what happens is people who don’t know the person very well say ‘Oh, it’d be better done by somebody who knows them really well’. And yet the people who know the person really well say it would be better done by somebody else, because it’s a difficult thing to do.
(Associate Professor and Consultant in Palliative Medicine, H807)
Both families and Support Workers thought that if they did not initiate end-of-life care planning, then it would not happen. However, most did not have these conversations, often due to their sensitive nature. Part of the difficulty was not knowing how to initiate them.
Lack of skills and training
Support staff described a lack of training and knowledge about end-of-life care planning and resources to support them.
We must have about 24 mandatory training courses within Dimensions, and not one of them is about end of life.
(Support Worker, S403)
The lack of skills and support was acknowledged by managers as well.
Support staff leaving
Staff turnover was seen as a huge barrier. People with intellectual disabilities expressed how hard it was when staff who knew them well could no longer support them in decision-making. The difficulty also included not knowing who would support them in the future.
Because they moved on. They got different jobs. They got different responsibilities. (. . .) She couldn’t make that decision because she’s moved on.
(Person with intellectual disabilities, L2b02)
Other participant groups agreed, and it was particularly challenging when having to make decisions where no one had in-depth knowledge about the person.
Facilitators
Helpful ways of doing end-of-life care planning are highlighted in the how section.
Re-framing discussions in terms of planning for living was a potential facilitator.
Making it easier for families by creating a kind of subtle pathway to the final conversation. I think talking about death is, you know, it’s a really massive thing, and it brings up a lot. (. . .) there is some kind of parts of that end-of-life planning that don’t have to have the word death in it at all.
(Mother, F602)
This point was also demonstrated in one of the focus groups with people with intellectual disabilities. One participant did not want to think about things she wanted to do before she died, but re-framing the question as what to do when she was still alive was welcomed.
Discussion
Main findings
End-of-life care planning with people with intellectual disabilities involved four aspects (i.e. funeral planning, illness planning, life planning and talking about death) that influenced when it should happen and with whom. Participants’ views on their own role were mostly one of positive involvement, but in practice discussions were often postponed. This was linked to a reluctance to consider death and a lack of skill or confidence. Accessible approaches, real-life opportunities and focusing on wishes for living may facilitate these conversations.
What this study adds?
End-of-life care planning is a requirement for service providers who provide life-long support of people with intellectual disabilities. For palliative care professionals, the term ‘end-of-life care planning’ is one aspect of Advance Care Planning, which refers to care at the end-of-life. However, many study participants, including people with intellectual disabilities, understood end-of-life care planning to be primarily funeral planning. This echoes research showing that patients and families tend to orient to funerals and wills, rather than what happens at the end-of-life. 18 It points to a discrepancy in understanding between those with intellectual disabilities who may receive palliative end-of-life care (and their families and support staff) and those providing it. In practice, end-of-life care planning in intellectual disability services is not focused on care at the end-of-life, but rather limited to making funeral plans. A study on Advance Care Planning with four people with intellectual disabilities showed that support staff covered treatment preferences and advance directives in a superficial way, indicating limited comfort and skill in discussing such issues. 19 The authors suggests that increased collaboration between support staff and palliative care professionals could address these issues and enable services to complement each other’s skill set. This aligns with the palliative care approach, which should be provided within a multi-professional and interdisciplinary framework with continuous communication and collaboration between professions and disciplines. 20
Change in terminology may be one way to ensure clarity about what the planning involves and requires. ‘End-of-life care planning’ was used in this study in line with terminology used by the service collaborators. Using ‘Advance Care Planning’ may have elicited different results. However, the Advance Care Planning research field is complex with varying definitions.21,22 Recently, it has been proposed to use ‘Future Care Planning’. 23 How these terms are understood and can be operationalised with people with cognitive impairment needs further exploration.
Funeral planning involves specific choices, which may explain why this aspect was emphasised and potentially also why people with intellectual disabilities could imagine being involved in it. However, it was difficult for them to imagine being close to death. This posed a dilemma, as people with intellectual disabilities struggle with abstract concepts and may need clear choices. However, end-of-life choices are not clear; they are complex, uncertain and influenced by a range of factors (e.g. the person’s preferences, family preferences, functional levels, culture, clinician advice and caregiver burden), which change over time. 24 This general complexity around planning represents a gap between hypothetical scenarios and actual decision-making processes. Illness planning needs to start when it becomes relevant with healthcare professionals who clarify options. 22 Another study with people with intellectual disabilities also stressed that it was preferable to start end-of-life care planning as early as possible following a life-limiting diagnosis. 19
Planning for living aligns with ‘what matters most’ conversations within palliative care. 25 It also aligns with person-centred planning within intellectual disability services and what is captured in general healthcare documentation (e.g. ‘Hospital Passport’ 26 ). A study found that people with intellectual disabilities who were terminally ill wanted to focus on life rather than dying. 19 How to meaningfully integrate ‘life plans’ with end-of-life care plans needs further exploration.
Talking about dying is related to organisational and family cultures around death. 11 It has been highlighted that intellectual disability service policies on dying and death are not offering people the adequate time and assistance to understand what is happening when they (or someone they know) are dying, let alone to make care decisions. 27 However, a general death avoidance culture should also be considered. It has been recommended that conversations and stories about everyday death and dying become common within society. 28 The study findings show that support staff need training and skills in having end-of-life care planning discussions. This aligns with findings from a UK-wide survey of intellectual disability support staff on communicating about death and dying with adults with intellectual disabilities who are terminally ill or bereaved. 29 Study participants rated training in both end-of-life care, advance care planning, breaking bad news and communication and bereavement as being quite or extremely useful. It is crucial that organisations ensure that support staff receive training and support in having end-of-life care planning discussions. Palliative care professionals could support such training and also help normalise conversations around death.
Participants mentioned the importance of involving support staff and families in end-of-life care planning, which echoes recommendations by the Palliative Care for People with Learning Disabilities Network 30 and the European Association for Palliative Care. 31 The latter also stresses that anyone (including services) with expertise to offer at the end-of-life should be identified as early as possible in the care pathway and involved if there is a need. 31 This aligns with the study finding that palliative and healthcare professionals are involved when illness planning becomes relevant and needed. It has been further stressed that collaboration and coordination between those involved in end-of-life care are important.30,31
This study show that end-of-life care planning discussions with people with intellectual disabilities should be carried out in inclusive formats. The European Association for Palliative Care has stressed that ensuring good communication with people with intellectual disabilities is of high importance, 31 and (good) communication has also been described as a facilitator for palliative care provision with this population. 7 People with intellectual disabilities should be allowed time to understand information and receive tailored communication to their needs, supplemented with verbal and written information with clear words and pictures to promote understanding. 31 Intellectual disability services should have inclusive and accessible resources and materials ready to aide support staff in having these discussions.
Strengths and limitations
The study included 60 participants sharing their experiences of end-of-life care planning with people with intellectual disabilities. It involved multiple stakeholder views, including people with intellectual disabilities themselves and co-production throughout.
The study sample lacks organisational, cultural and ethnic diversity. A follow-up study is underway, involving people from minoritised ethnic groups within smaller intellectual disability services.
The study did not include people with intellectual disabilities who were terminally ill and/or at the end-of-life. As the study showed that illness planning should happen when it becomes relevant, their views should be further explored.
As participants had to have some verbal ability, people with severe/profound intellectual disabilities could not participate directly in the study. Their views were represented by proxy. Future research could further explore their perspectives.
Several potential participants declined to participate in the study, as they did not want to talk about death. This meant that the research team experienced inclusion bias towards participants who were willing to talk about death. In future studies it is important to hear from people who are reluctant to talk about this topic, to gain further insight into barriers and facilitators.
Conclusion
As end-of-life care planning with people with intellectual disabilities covers several areas and terminologies differ, it needs to be clear what is being planned for to develop interventions to facilitate each area in an appropriate and timely manner. Families and support staff who know the person intimately have a crucial role but need support in normalising end-of-life conversations and understanding end-of-life (‘illness’) choices. Closer collaboration between intellectual disability and palliative care services and proactive engagement are needed to facilitate optimal end-of-life care.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163241250218 – Supplemental material for What are we planning, exactly? The perspectives of people with intellectual disabilities, their carers and professionals on end-of-life care planning: A focus group study
Supplemental material, sj-pdf-1-pmj-10.1177_02692163241250218 for What are we planning, exactly? The perspectives of people with intellectual disabilities, their carers and professionals on end-of-life care planning: A focus group study by Andrea Bruun, Amanda Cresswell, Leon Jordan, Richard Keagan-Bull, Jo Giles, Sarah L Gibson, Rebecca Anderson-Kittow and Irene Tuffrey-Wijne in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163241250218 – Supplemental material for What are we planning, exactly? The perspectives of people with intellectual disabilities, their carers and professionals on end-of-life care planning: A focus group study
Supplemental material, sj-pdf-2-pmj-10.1177_02692163241250218 for What are we planning, exactly? The perspectives of people with intellectual disabilities, their carers and professionals on end-of-life care planning: A focus group study by Andrea Bruun, Amanda Cresswell, Leon Jordan, Richard Keagan-Bull, Jo Giles, Sarah L Gibson, Rebecca Anderson-Kittow and Irene Tuffrey-Wijne in Palliative Medicine
Footnotes
Acknowledgements
We would like to thank our intellectual disability service collaborators, Dimensions and MacIntyre, and all the participants who took part in the study.
We would also like to thank our Research Advisory Group members for valuable input throughout the study: Adrienne Betteley, Macmillan Cancer Support; Dr Annie Stewart, PCPLD Network; Dr Catherine Millington-Sanders, RCGP & Marie Curie; Chris O’Donnell, Enfield Integrated Learning Disability Service; Gary Bourlet, Learning Disability England; Hille Voss, Ben Sajet centrum; Jean Willson OBE, Centre 404; Joanna McIlmurray, Battersea Healthcare CIC; Justine Button, Care Quality Commission; Kathryn Mannix; Lucy Winter, L’Arche UK; Making Families Count; Melanie Taylor, Hospice UK; NHS England; Dr Nic McKenzie; Peter Allum, GRASSroots and PCPLD Network; Sarah Pope, Enfield Integrated Learning Disability Service; Sam Royston, Marie Curie; Samantha Clark, Learning Disability England; Sarah Offley, Dudley Voices for Choice; Simon Blake; Sue Marsden, Greenwich & Bexley Community Hospice; Usha Grieve, Compassion in Dying; and Vince Peters, Dudley Voices for Choice.
Author contributions
Study design: IT-W, RA-K. Data collection: AB, AC, GJ, IT-W, LJ, RA-K, RK-B, SG. Data analysis: AB, AC, GJ, IT-W, LJ, RA-K, RK-B, SG. Manuscript writing: AB, IT-W. Manuscript approval: AB, AC, GJ, IT-W, LJ, RA-K, RK-B, SG.
Data management and sharing
Descriptive metadata will be made available on the Kingston University London Research Data Repository in 2024. Full data will not be available, as they are not anonymised.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was part of a research project funded by The National Institute for Health Research (NIHR) Research for Social Care (RfSC), Research for Patient Benefit (RfPB) Programme (NIHR202963).
Research ethics and participant consent
The study received ethical approval from West Midlands – Coventry & Warwickshire Research Ethics Committee (22/WM0026) on 22/04/2022. All study participants had to read and understand a detailed Participant Information Sheet and provided informed written consent to participate in the study. People with intellectual disabilities received support to understand the easy-read study information with local support staff. Focus group sessions with people with intellectual disabilities were initiated by repeating study information to further ensure participants’ consent to participate in the study. Capacity to consent was assessed in all participants, with extra care taken for participants with intellectual disabilities. Capacity to consent was assumed as per the Mental Capacity Act unless there was reason to suggest otherwise. Personal identifiers in quotes included in this paper have been anonymised.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.