
Abstract
Background:
People with palliative care needs and their carers often rely on out-of-hours services to remain at home. Policymakers have recommended implementing telephone advice lines to ensure 24/7 access to support. However, the impact of these services on patient and carer outcomes, as well as the health care system, remains poorly understood.
Aim:
To evaluate the clinical- and cost-effectiveness of out-of-hours palliative care telephone advice lines, and to identify service characteristics associated with effectiveness.
Design:
Rapid systematic review (PROSPERO ID: CRD42023400370) with narrative synthesis.
Data sources:
Three databases (Medline, EMBASE and CINAHL) were searched in February 2023 for studies of any design reporting on telephone advice lines with at least partial out-of-hours availability. Study quality was assessed using the Mixed Methods Appraisal Tool, and quantitative and qualitative data were synthesised narratively.
Results:
Twenty-one studies, published 2000–2022, were included. Most studies were observational, none were experimental. While some evidence suggested that telephone advice lines offer guidance and reassurance, supporting care at home and potentially reducing avoidable emergency care use in the last months of life, variability in reporting and poor methodological quality across studies limit our understanding of patient/carer and health care system outcomes.
Conclusion:
Despite their increasing use, evidence for the clinical- and cost-effectiveness of palliative care telephone advice lines remains limited, primarily due to the lack of robust comparative studies. There is a need for more rigorous evaluations incorporating experimental or quasi-experimental methods and longer follow-up, and standardised reporting of telephone advice line models and outcomes, to guide policy and practice.
Urgent and unplanned emergency department and hospital admission is frequent for people in the final months of life.
Designated palliative care telephone advice lines have been recommended internationally to ensure round-the-clock access to support from trained professionals and are proposed to help reduce urgent and unplanned use of acute services.
While a range of palliative care telephone advice lines exist, the evidence base for their effectiveness, in terms of patient and health care system outcomes, is not known.
We demonstrate that existing evidence for the effectiveness of telephone advice lines is limited and largely based on observational studies of insufficient methodological quality.
Overall, telephone advice lines can offer guidance and reassurance that supports family carers in providing care at home, but there is very little evidence of health care system outcomes associated with using palliative care telephone advice lines, including health economic analysis.
Involvement of patients and carers in the design or reporting of studies evaluating telephone advice lines is rare.
Future development and evaluation of telephone advice lines need to include patients, carers and other stakeholders to better understand what needs and preferences should shape the services.
To address the limited and variable evidence identified, we provide a framework of key components of telephone advice line models that should be included in future research reporting.
Background
People with palliative care needs living at home and their carers often rely on out-of-hours service providers,1,2 particularly during periods of worsening symptoms, or changes in the individual’s condition. 3 Unscheduled care and out-of-hours care services are frequently accessed by people approaching the end of life,1,4,5 with emergency care utilisation rising considerably in the final month of life. 6 Still, a large proportion of palliative care is delivered in the community.7,8 Among those who die, almost 30% are seen by out-of-hours primary care services during their last 30 days of life. 9
Timely access to palliative care support and advice from trained professionals is essential for patients who prefer to be cared for, and die, at home (and their informal carers) who might face a complex array of symptoms and care needs.10,11 Despite international trends of increasing home deaths and the rising need for community-based palliative care, 12 access and provision of palliative care in the community is highly geographically variable.8,13,14
Palliative care telephone advice lines have been recommended in policy in several countries to provide timely support for people with end-of-life care needs and their carers, especially for those living in rural areas.15 –19 Variable availability and accessibility of palliative care telephone advice lines, particularly during out-of-hours periods, is still an issue, however.20,21 Consequently, many people rely on national emergency numbers (i.e. 999) and primary care service provision from out-of-hours General Practitioners and Community Nurses during these times. Though a wide variety of palliative care telephone advice line models are in use and under development, 20 the effectiveness and cost-effectiveness of different service models has not been assessed.
Aim
Our aim was to review the evidence for the clinical- and cost-effectiveness of out-of-hours palliative care telephone advice lines and report how service characteristics are associated with effectiveness. The objectives were to:
(1) identify and summarise data regarding use of telephone advice lines and reported impact on patient/carer and health care system outcomes;
(2) explore service characteristics associated with improved outcomes;
(3) evaluate the cost-effectiveness of implementing and maintaining out-of-hours telephone advice lines.
Methods
Study design
This rapid systematic review was planned and conducted in line with guidelines set out by Cochrane Rapid Reviews Methods Group 22 and the World Health Organization. 23 A rapid approach was used since telephone advice lines are receiving current attention by policymakers as a means of improving access to palliative care services for people living at home. A full systematic review is time-consuming and can take years from start to publication, whilst rapid reviews are particularly useful for timely synthesis to inform policy.22,23 The rapid review procedure is methodologically similar to a full systematic review but limits the scope and analytic process to provide a timely appraisal of existing evidence, for example, by assigning a single reviewer for screening or limiting sources beyond electronic databases. 24 The reporting adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist. 25 A protocol was developed prior to commencing the study and made publicly available on PROSPERO (CRD42023400370).
Eligibility criteria
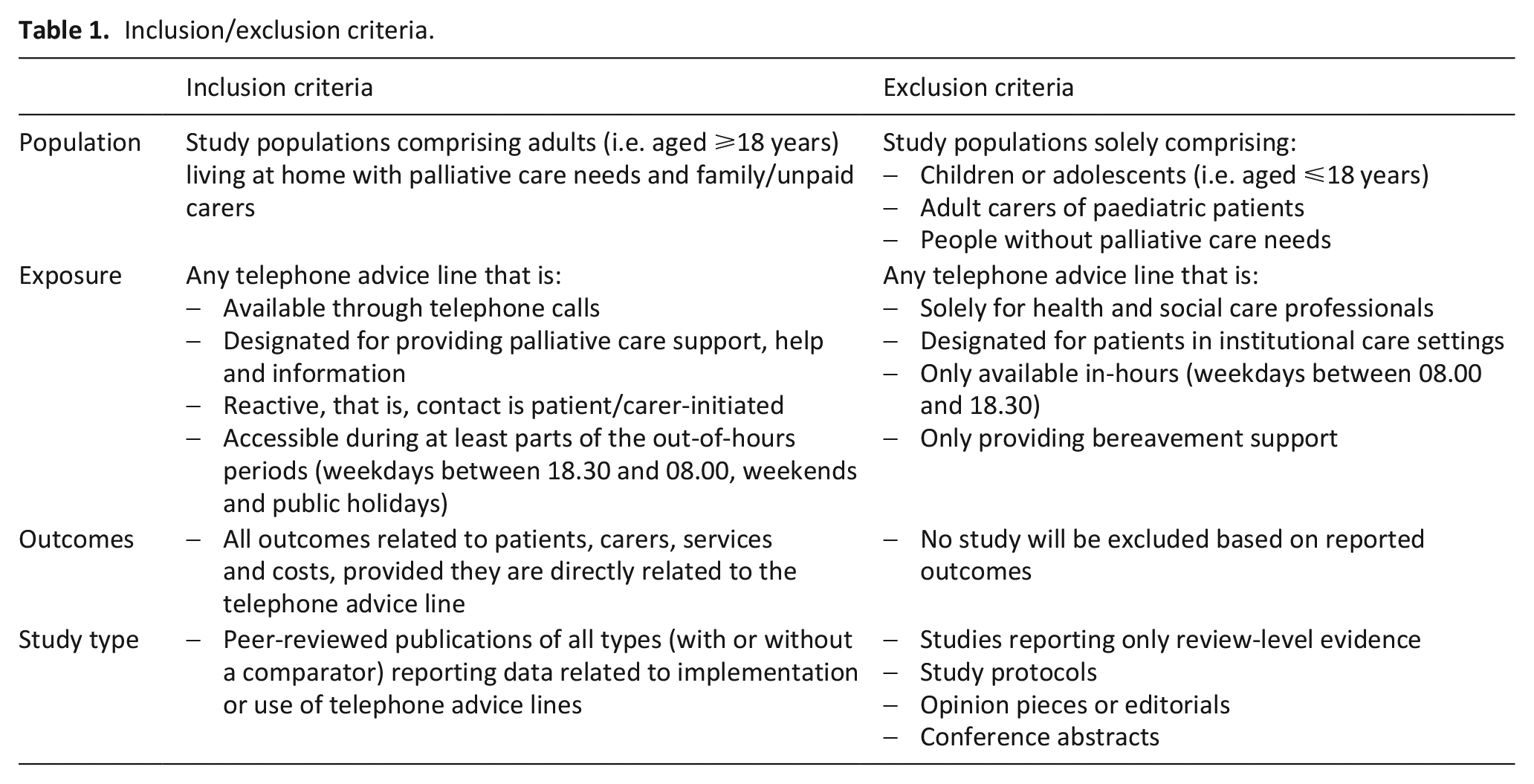
Any published study reporting on the use, effect or implementation of a telephone advice line available specifically for home-based adults with palliative care needs and their carers during at least part of the out-of-hours period was eligible, even if it was not the primary focus of an intervention. A broad definition was used to allow assessment of various types of telephone advice lines, provided there was a ‘reactive’ component (i.e. contact is patient/carer-initiated, as opposed to pre-booked appointments). Detailed inclusion and exclusion criteria are shown in Table 1.
Inclusion/exclusion criteria.
Search strategy
The searches were performed with assistance of an information specialist (SG) at Hull York Medical School, University of Hull. The search was developed in Medline by examining the indexing of known potentially relevant studies, designing and testing a search using these studies before translation into other databases. Three databases were searched: Medline All from 1946, EMBASE from 1974 (via OVID) and CINAHL Complete from 1937 via EbscoHost. The search used for Medline incorporated elements from previous strategies for palliative care by Rietjens et al. 26 and Sladek et al., 27 combining concepts of palliative care and out-of-hours telephone advice lines using both database specific indexed terms and free text terms. Filters were used to only retrieve primary studies written in English and to remove conference abstracts, books and editorials. No date limits were applied. All searches were performed on February 9, 2023. The full search strategies for all databases are provided in Supplemental File 1. Database results were downloaded into EndNote and duplicates were removed using a recognised method 28 before being uploaded into Covidence. 29
Study selection
The first author (TJ) screened titles and abstracts against the inclusion criteria using Covidence. To ensure screening consistency, a subsample was screened by a second reviewer (RC). Inter-rater agreement was 95% and conflicts were resolved by discussion. Full-text screening was performed independently by two reviewers (TJ and RC/MB), with any disagreements resolved by a third reviewer (AB).
Data extraction
A bespoke form for data extraction was constructed in Covidence (TJ). Data were extracted by one reviewer (TJ) and checked and verified by a second (RC/MB/TC). Data from each included study were extracted in Covidence and exported as a collated data set into Microsoft Excel for synthesis. Data for effectiveness assessment included any measure of the clinical or cost-related effect of the telephone advice lines on patients’ and carers’ health and wellbeing and care use. This included: changes to patients’ health status (symptom management, coping), impact on family members caring capacity, care seeking behaviours (emergency service use and hospitalisation), place of care, place of death, and experiences and satisfaction of service use. Data for cost effectiveness included: costs of providing the telephone advice line and related resource use (i.e., costs related to care service use). Due to the heterogeneity of study designs and reported outcomes, studies were not excluded from synthesis due to missing data. Since we did not summarise study findings statistically, missing data were accepted in any category of data extraction and the number of studies that reported relevant data are provided throughout the review.
Data synthesis
The quality of included studies was assessed using the Mixed Methods Appraisal Tool (MMAT), 30 which is a concise checklist that is particularly suitable for assessing a variety of study designs. 31 The MMAT yields a score ranging 1–5 that represents the number of quality criteria met for the specific study type. Given the scarcity of literature, all relevant studies were retained for synthesis regardless of their MMAT score.
Due to heterogeneity in aims, methods and outcomes of included studies, meta-analysis was not feasible. Instead, we performed a narrative summary of study findings, a method often referred to as narrative synthesis.32,33 Studies were grouped based on study design and, when possible, we summarised reported evidence of impact on patients and carers, and the health care system, with more weight given to methodologically robust studies.
The narrative synthesis was guided by Donabedian’s three-component framework for evaluating quality of care, 34 which encompasses structures (physical resources and staff to ensure the intervention is delivered), processes (how structural components are used and transactions between care recipients and providers) and outcomes (effects on patients’ and carers’ health and wellbeing, health-related behaviours and satisfaction with care).
During data synthesis, findings relating to telephone advice line characteristics, usage and reported study outcomes were mapped onto Donabedian’s framework. 34 We differentiated outcomes as patient/carer outcomes (i.e., health status, wellbeing and coping) and health care system outcomes (i.e., impact on the use of care services). We also differentiated cost-effectiveness as a separate outcome within the framework. Although Donabedian’s framework conceptualises patient satisfaction and experience as partly separate to outcomes, they were incorporated here as facets of patient/carer outcomes.
Findings from the review were discussed with the project patient and public involvement (PPI) advisory group, as well as in an online workshop with ten volunteers identified through the PPI forums of King’s College London and University of Hull, to help shape the synthesis and recommendations. 35 Advice from PPI members was sought on interpreting key messages, understanding essential characteristics of telephone advice lines and how the findings resonated with their lived experience. The PPI workshop led to the inclusion of geographical region, funding and PPI involvement in the development of telephone advice lines, as important characteristics of service models in the synthesis.
Results
The database searches identified 622 articles. After removing duplicates, 388 articles remained for screening based on title and abstract (of which 80 randomly selected articles were dual screened). In total, 340 articles were excluded, leaving 48 for full text review. Twenty-one articles were included in the review. The PRISMA flow chart is presented in Figure 1, stating reasons for exclusion at each stage.
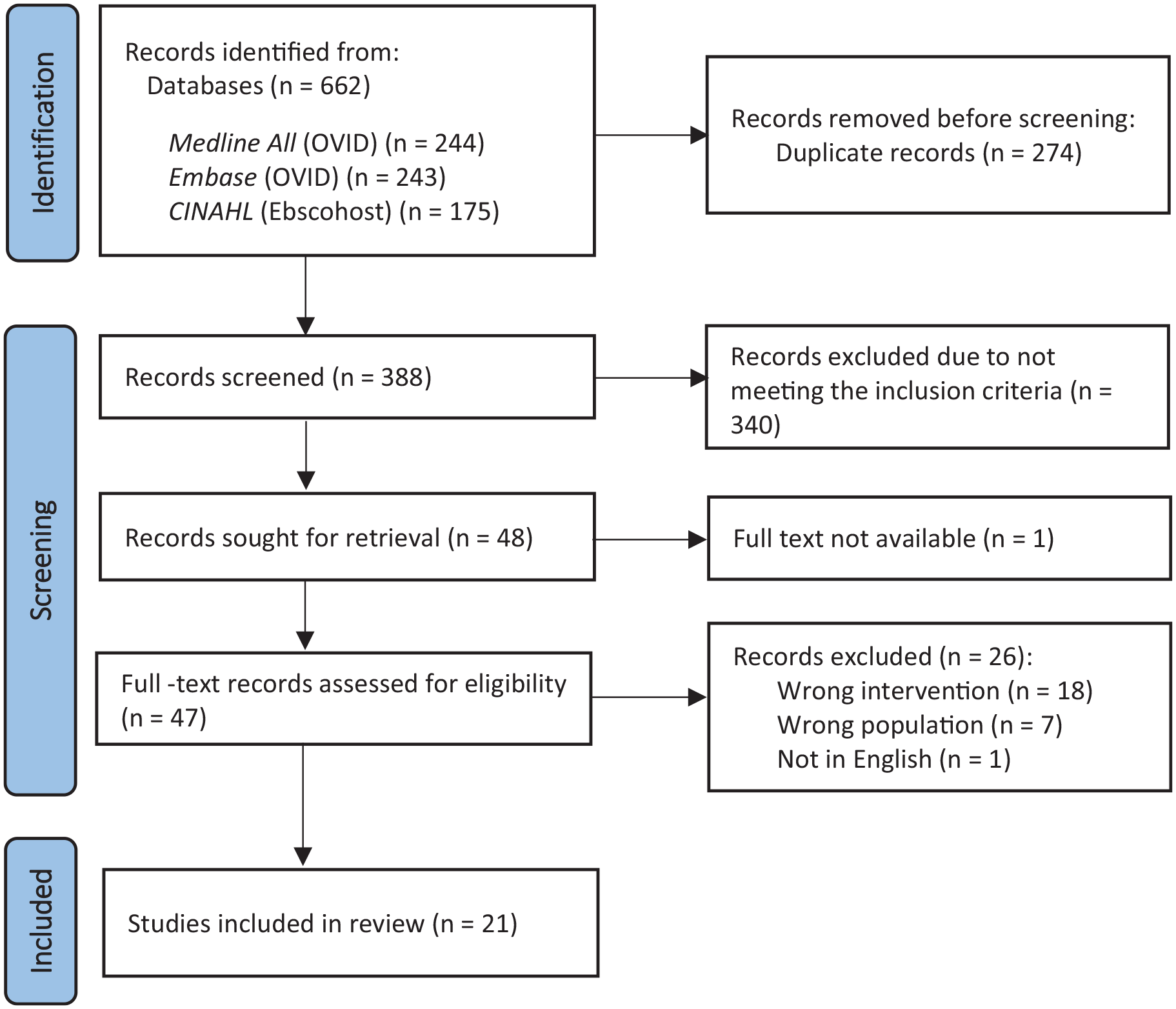
PRISMA flow diagram for systematic literature search results.
Study descriptives
The 21 included studies were published between 2000 and 2022. Around half were conducted in the United Kingdom (n = 11),36 –46 with the remaining studies coming from Australia (n = 4),47 –50 the United States (n = 2),51,52 Canada (n = 1), 53 The Netherlands (n = 1), 54 Singapore (n = 1) 55 and Taiwan (n = 1). 56
Eight of the studies were quantitative (of which three were comparative),44,47,48,51,52,54 –56 five used mixed-methods,38,39,41,42,50 and one was qualitative. 45 Seven studies did not specify a methodology. Of these, four reported quantitative and qualitative data37,40,43,53 and three presented quantitative data only.36,46,49
Most studies were retrospective observational studies or audits, using quantitative data either from existing call logs or purpose-built proformas for incoming calls to the telephone advice line as the primary source of data (n = 15). Qualitative data were usually collected through feedback surveys or follow-up interviews with a sub-sample of callers. Table 2 presents the methodology of included studies.
Overview of the methodology of included studies, grouped according to study type and ordered according to quality appraisal score.
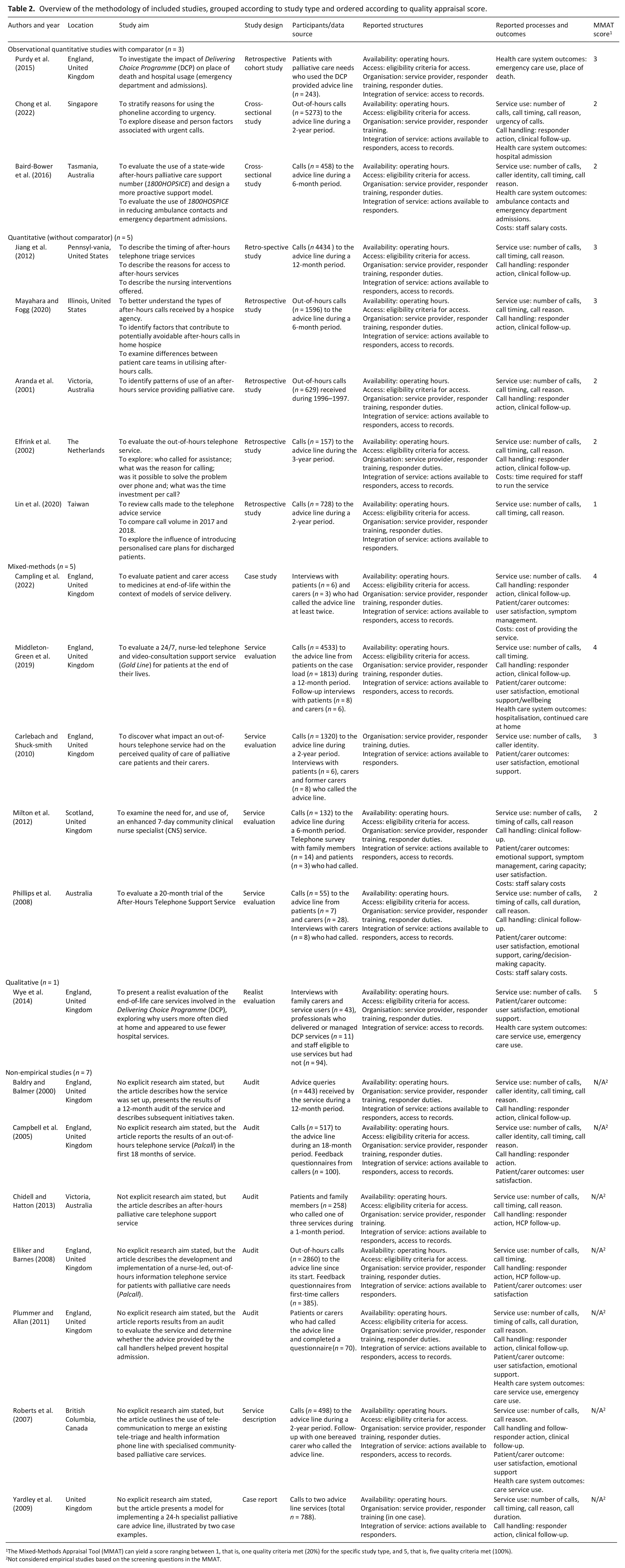
The Mixed-Methods Appraisal Tool (MMAT) can yield a score ranging between 1, that is, one quality criteria met (20%) for the specific study type, and 5, that is, five quality criteria met (100%).
Not considered empirical studies based on the screening questions in the MMAT.
Synthesis
Study quality
Overall, the quality appraisal found that few studies were empirically robust. Seven studies could not be appraised as they lacked an explicit study aim or research question, and therefore did not meet the MMAT screening criteria for empirical studies.36,37,40,43,46,49,53 Of the 14 that were appraised, most had moderate or low MMAT scores (three or lower, corresponding to meeting 60% of quality criteria or less), primarily due to either poor or poorly described study methodology. MMAT results for each study are presented in Table 2.
Structures of care
The 21 included studies featured 20 unique telephone advice lines, with one appearing in two studies (Delivering Choice Programme’s out-of-hours advice line)44,45 and one being reported post-implementation and re-evaluated after 3 years (Palcall telephone advice line).37,40 One further study reported two different telephone advice lines. 46
The main characteristics of the telephone advice lines in each study are provided in Table 3, with a summary of findings presented in Figure 2. Overall, 13 of the telephone advice lines were available for calls 24/7 and six were available during parts of the out-of-hours periods. One study did not state availability. 39 All services used telephone-based technology, with telephone calls being the primary means of contact. Fifteen of the telephone advice lines were accessible only for patients known to palliative care services or listed on palliative care registers (and their carers), but information on how they were promoted or explained to patients and carers was uncommon. Information about the structure of the telephone advice lines was scant. Fewer than half of the studies described the location and coverage of the telephone advice line. The majority of services were not diagnosis-specific, with just one being restricted to cancer patients. 54 When reported, telephone advice lines were either financed by time-specific grants or funded internally by the service (Table 3).
Characteristics of telephone advice line services reported in the included studies.
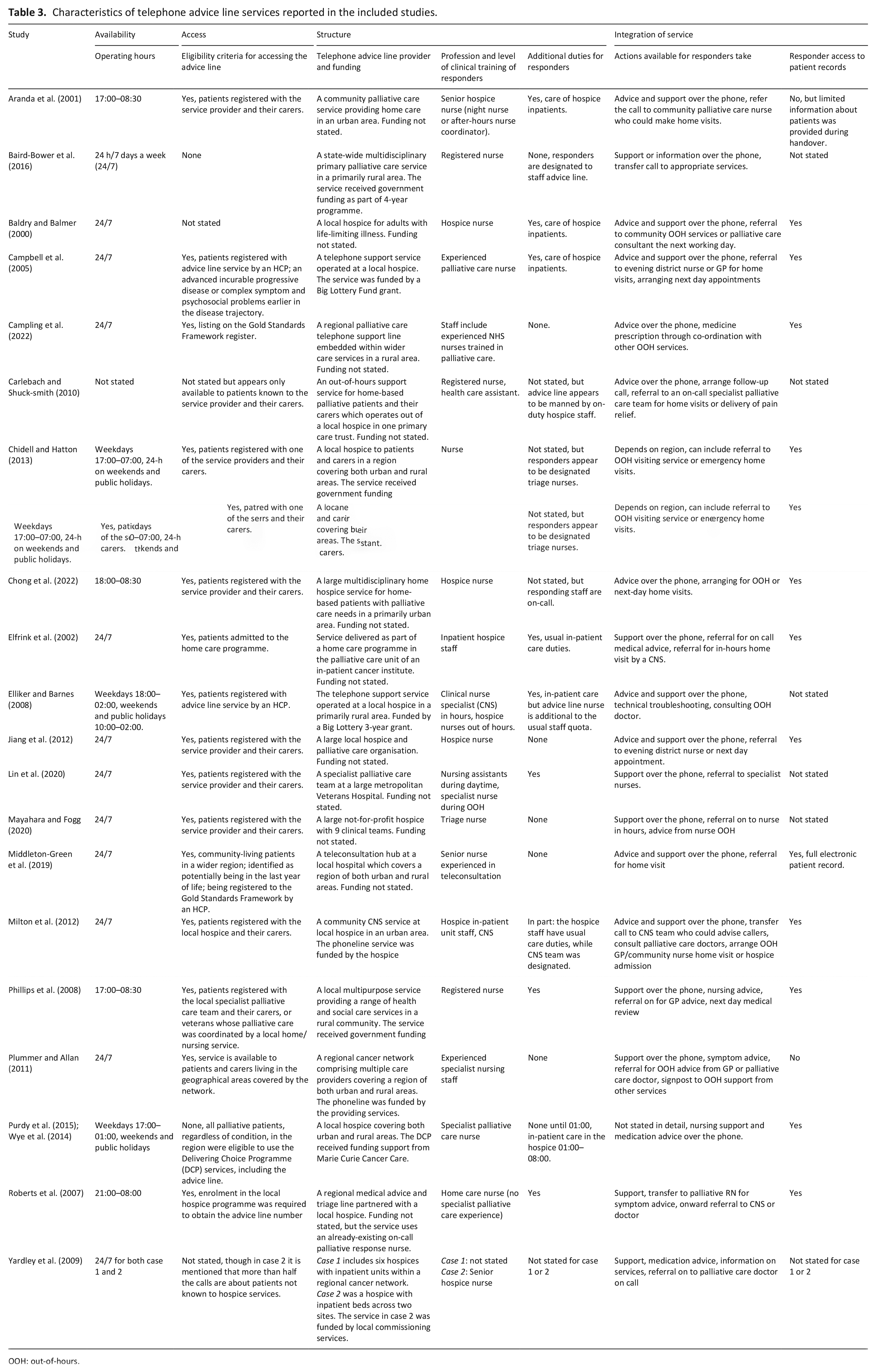
OOH: out-of-hours.
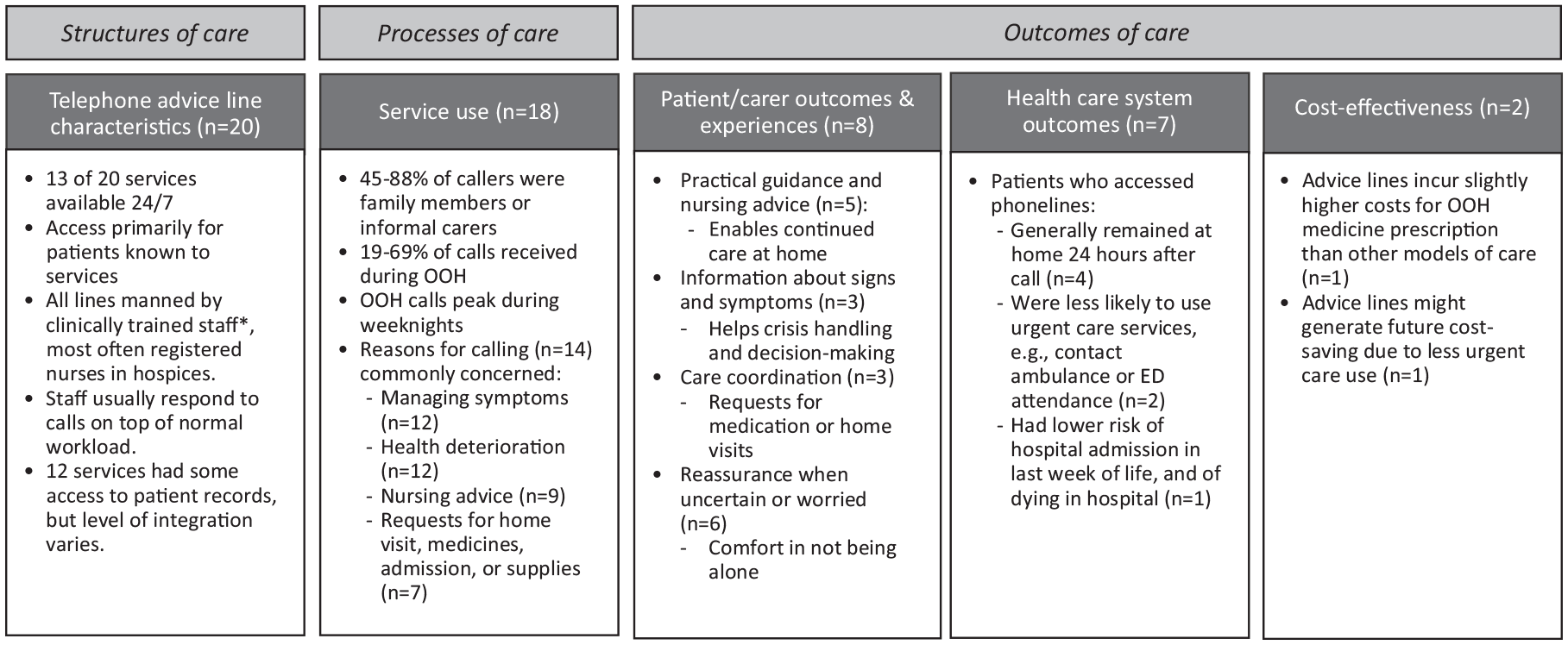
Summary of reported study findings applied to Donabedian’s framework of structures, processes and outcomes of care.
While the process of designing and implementing the telephone advice line service was described in several studies,37,40,42,43,46,47,50,53,54 PPI or stakeholder consultation was rarely mentioned and only two studies reported involving patients and carers during development and feasibility testing of services.37,40 Two further studies mentioned consulting key stakeholders during development but provided no detailed information on who or what this entailed.46,50
Processes of care
Aspects of service use were reported in 18 of 21 studies, usually relating to call volumes, timing of calls, identities of callers, reasons for calling and information on how the call was handled by the responder or the organisation (Figure 2).
In the seven studies that had 24/7 telephone advice line availability and reported call data, between 19% and 69% of calls were received during out-of-hours periods.36,38,41,46,49,55,56 Of these, most out-of-hours calls (35%–78%) were received on weeknights before midnight, though the level of detail in reports differed.37,39,40,42 –45,47,48,50 –54
In the 12 studies that distinguished caller identities, callers were primarily identified as family members or informal carers (ranging 45%–88% of calls in the studies).36,37,39,40,43,48,50,51,54 –56 Additional characteristics of out-of-hours callers, such as sociodemographic information, were presented in two studies. A study from Singapore by Chong et al. 55 reported gender (48.6% male), age (mean age 75.5 years), cancer diagnosis (80.9%), ethnicity (80.3% Chinese, 9.5% Malay, 5.2% Indian and 5.0% Other) and marital status (62.0% married, 26.9% widowed, 6.5% single and 4.6% divorced or separated). An American study by Mayahara et al. 52 reported ethnicity (patients: 73% White, 5% Black, 2% Asian, 20% Other; carers: 50% White, 25% Black, 25% Asian and 5% Other) and gender (60% female patients, 80% female carers), as well as diagnoses (most patients had ‘senile degeneration of the brain’ (n = 212) and/or Alzheimer’s disease (n = 116), heart failure (n = 71), chronic obstructive pulmonary disease (n = 58) or other advanced illnesses). Four studies reported basic demographics such as diagnosis, age, gender or household composition for a wider patient sample registered with or eligible to access, the service.41,44,47,54 Baird-Bower et al. 48 collected some sociodemographic information of callers by linking call log data to patient records, but only reported callers’ location.
Reasons for calling were presented in 12 studies, with varying degrees of detail. The most reported call reason was managing symptoms and/or medication (n = 10), with other reasons including health deterioration, nursing advice, requests for new or additional medication or equipment or reporting that the patient had died.36,37,42,43,46,47,50,51,54,55 Since few studies provided information about follow-up periods, data about when in the care trajectory calls were made were scarce. Purdy et al. 44 found that median time for accessing the telephone advice line was 10 days before death, and Jiang et al. 51 reported that most calls occurred between the first days of home hospice admission and the last 3 days of life. Roberts et al. 53 and Middleton-Green et al. 41 presented qualitative data indicating that people call in the final days of life for advice and support when the patient is dying, as exemplified by this carer: ‘I think I just asked the question ‘is this what I think it is?’ And I think all they said was “yes, probably”’. 41
Fifteen studies gave some information about call handling. Actions available to responders differed between telephone advice lines and were variably described. Overall, the most reported actions taken by responders involved providing support and nursing advice appropriate to their level of clinical training, and transferring or signposting callers to other services. Responders in some telephone advice lines also contacted on-call teams for urgent home visits (n = 5), arranged next-working-day follow-up at home or over the telephone (n = 9) and, less commonly, helped with prescribing or collecting medication (n = 4; Table 3). Ten studies reported that responders successfully handled many calls directly through over-the-phone support.36,37,41,43,47,49,51,53,54,56 In cases when a responder could not adequately help a caller, calls were usually passed on to more senior healthcare professionals, commonly senior palliative care nurses, clinical nurse specialists or GPs, who were either available on-call or in-house (n = 11).36,38,41,43,45 –47,49,51,53,54 These professionals could generally provide more advanced medical advice, arrange home-visits, make referrals and occasionally, prescribe or dispatch medicines. However, the proportion of calls passed on was rarely reported.
Outcomes and experiences of care
Patient and carer outcomes
Reported outcomes in the studies primarily related to patients’ and carers’ accounts of using a service and derived from open-ended survey questions or interviews. No study provided quantitative data about effects on patient and carer outcomes, that is, impact of patient’s and carer’s health (such as reduced anxiety or improved symptom management). However, there was qualitative evidence of patients’ and carers’ reports of benefit from using telephone advice lines.
Patient and carer experiences of using the telephone advice lines were reported in eight studies using qualitative data, and were overwhelmingly positive.38,39,41 –43,45,50,53 Patients and carers reported that the telephone advice lines provided general information, medical advice and practical guidance about symptom management or care procedures.39,41,43,45,50 This was exemplified by a carer in Phillips et al.’s 50 study stating that ‘You have the information but when you go to do it, it is really scary. It was so good to have someone just telling me I was doing the right thing’. The same study found that accessing advice enabled carers to continue caring at home, and Carlebach and Shucksmith 39 highlighted how this promoted independence for patients. A recurring finding was that the telephone advice lines provided valuable opportunity for patients and carers to ask about signs and symptoms and be informed about the disease trajectory or the dying process, so that callers can better understand whether these are ‘normal’ or expected.41,45,53 This was exemplified by a carer quoted by Middleton-Green et al.: 41
‘[It] helped, just that somebody could tell me what was, reassure me that what I was seeing and experiencing . . . it meant that I could just be in the moment with her. It gave me sort of control over my feelings, which ultimately meant that she was looked after better than she would have been’
Receiving appropriate information was also reported to aid decision-making and help prevent unnecessary hospital admission and promote appropriate use of care services, as patients and carers noted that they might otherwise have contacted emergency care services.41,45,50
Some studies reported how telephone advice line staff would liaise with other services on patients’ behalf, which was advantageous when callers were requesting medication, care equipment or home visits.38,41 Carlebach and Shucksmith 39 highlighted callers sense of comfort when responders were familiar with the patient’s case. Similarly, access to patient records was described as valued by callers who did not have to re-explain the situation, as described by a carer quoted by Campling et al. 38 : ‘You don’t have to go through the rigmarole of explaining everything. They’ve got your records there; they can see clearly what’s going on. . .’. The few negative experiences that were reported related to when continuity of care was perceived lacking, for example, when information was not shared between services.
Calls were generally triggered by a patient crisis or carer uncertainty. Both patients and carers emphasised feeling reassured by the knowledge that the service was available for them whenever they might need it, both in medical crises and when the caller was feeling worried.39,41,43,45,50,53 In Milton et al.’ 42 study, feedback from a carer stated that ‘There was comfort in knowing [staff] were on standby when you needed them; [it] made things easier, not being alone here’. In demanding situations, only having one phone number to call to get direct access to experienced staff was helpful. Wye et al., 45 for example, presented a carer who noted that: ‘I didn't ever have to phone for ambulances or anything, all that was done and it wasn't done through the GP or the district nurse. . . you could just phone one number’.
Health care system outcomes
Seven studies used patient records to assess outcomes relating to callers’ subsequent care service use but only two of these were comparative. These linked calls to routine data over a defined follow-up period. Both demonstrated that patients who accessed telephone advice lines were less likely to use emergency care services subsequently. Baird-Bower et al. 48 examined patient records and mortality data up to six months after service use and found that users were less likely to call for an ambulance (χ2 = 70.094, p < 0.01) or visit an emergency department (χ2 = 78.286, p < 0.01) compared to people who never called. Purdy et al. 44 had a shorter follow-up period but found that emergency department attendance was lower among callers compared to a cohort without access to a telephone advice line service both 30 (OR 0.60, p = 0.007) and 7 days before death (OR 0.34, p = 0.003). They also showed that callers were less likely to be admitted to hospital in the last week of life (OR 0.44, p = 0.005) and to die in hospital (OR 0.34, p < 0.001) compared to patients who did not use the service. 44
While there was little evidence for whether calls influence patients’ and carers’ subsequent care seeking behaviour, six studies demonstrated that, overall, only between 1.5% and 9.0% calls led to hospitalisation or admission of patients.41,42,49,51,53,55 This suggests that hospitalisation is infrequent following out-of-hours calls, although the lack of data makes it hard to determine the effect of telephone advice lines on subsequent admission. Three retrospective cross-sectional studies reported that 73%–95% of patients who contacted the telephone advice line remained at home 24 h after the call.41,43,53 There was, however, no further follow-up. Aranda et al. 47 reported that 37% of all deaths during the study period occurred at home, but this was not temporally or causally linked to use of the telephone advice line.
Cost effectiveness
There was very scant evidence regarding costs or cost effectiveness of telephone advice lines, with a few studies using patient records to estimate costs or cost-savings in relation to expected benefits. Three studies presented rough estimations of costs associated with implementing telephone advice lines within a specific service, suggesting they were generally ‘resource-effective’ for providing palliative care during out-of-hours periods, but did not provide detailed cost breakdowns or include cost-savings related to potential benefits of the service.42,50,54 Mayahara and Fogg 52 argued that reducing avoidable out-of-hours home visits in response to, for example, medication or equipment requests would save overall health system costs but did not provide a cost-analysis. 52
Two studies provided wider cost-benefit estimations, but both were based on estimated rather than observed impact. Baird-Bower et al. 48 estimated that use of the telephone advice line could lead to general cost savings associated with less use of avoidable emergency care for people who want to die at home, with projections of 28% lower emergency department attendance saving 121,647 Australian dollars and a 35% reduction in ambulance calls saving 112,700 Australian dollars. 48 Campling et al., 38 on the other hand, reported that for the purposes of improving out-of-hours access to medicines for patients at home, the telephone advice line model incurred slightly higher costs than other models of care (1-year cost of prescribing for an assumed English patient population with palliative care needs estimated to £60,075,302, compared to £49,483,750 for standard general practice prescriptions and £43,267,634 for clinical nurse specialist prescriptions). 38
Discussion
Although telephone advice lines are recommended in palliative care policy and guidelines, and widely implemented at local levels, our study found very limited empirical evidence for their clinical and cost-effectiveness. Most studies report process measures, for example, service use and handling of calls, whereas the potential impact on patient and carer health, wellbeing and caring capacity or influence on subsequent service use and costs is rarely assessed in a rigorous manner.
Findings from the more methodologically robust studies suggest possible support for the clinical effectiveness of telephone advice lines, with use being associated with remaining at home following the call and less contact with emergency care services41,44,48,53 However, most studies were observational, often of low methodological quality without control or comparator groups and can therefore not establish causality. Similarly, qualitative data indicate that the mechanism of action for reducing unnecessary or inappropriate emergency care use is the provision of care advice and emotional reassurance from trained staff, which enables patients and carers to better cope with care provision at home, if the patient prefers this. The possible influence on emotional wellbeing and caring capacity is a promising finding considering projected rises of home deaths and increasing work for informal carers when palliative care provision shifts towards being community-based,57,58 especially since anxiety has been shown to contribute strongly to urgent care-seeking behaviour. 59
Telephone advice line models varied according to accessibility, structure of service provision and integration with other care services. Limitations of the synthesised data, for example, poor quality and inconsistent or insufficient reporting, prevented meaningful assessment of which telephone advice line models are most effective. Taken together, however, the included studies suggest that telephone advice lines might provide patients and carers at home with a viable alternative to emergency care when health deteriorates outside of normal working hours of care services, which is in line with other studies exploring reasons for contacting care services out-of-hours at the end of life.60 –62
Most of the evidence was derived from studies on telephone advice lines services that are accessible primarily to people known to the providing care services (often a specialist palliative care service), which raises questions regarding equity of access, as the wider population of people with palliative care needs in the community remain under-served. While a few studies considered differences in the use of telephone advice lines according to diagnosis,44,47,55 no studies analysed patterns of use according to socioeconomic position or ethnicity. Our PPI workshop highlighted potential challenges for misunderstandings due to language barriers when telephone advice lines are used by marginalised communities. Limited language proficiency was not addressed by any included study, even though language barriers constitutes a key challenge associated with worse quality of care, 63 and higher rates of emergency care use at the end of life. 64
Another gap in the existing literature relates to integration with other services, for example, the extent to which patient records were accessible to staff responding to calls and shared with other health care professionals. Inadequate integration with the wider health care system has previously been identified as contributing to inequity in access to community-based palliative care and may limit benefits for patients and carers. 65 While it was not possible to assess whether access to patient records influences the effectiveness of telephone advice lines, the included studies suggest that such access to records allows responding staff to better understand the patient’s circumstances and provide appropriate advice.
Several of the included articles were based on internal audits rather than empirical research studies, which limits the generalisability of the evidence. In addition, most articles only encompassed service users, who might not be representative of the larger population of home-based adults with palliative care needs. Another potential source of bias is that authors in eight of the included articles were evaluating telephone advice lines services in which they had clinical or managerial roles. 66 The additional finding that patient and public involvement during stages of planning, designing and evaluating telephone advice lines processes was uncommon, or at least rarely reported, further emphasises that the current literature relies heavily on the professional perspective. Inadequate use and reporting of PPI makes it difficult to gauge whether existing telephone advice lines are meeting the needs and preferences of the patients and carers they intend to serve. Involving patients and carers in co-design and evaluation is imperative to ensure relevance and patient-centred care delivery and will help identify hindering and facilitating factors for use.13,67 Use of guidelines, such as Guidance for Reporting Involvement of Patients and the Public 68 in future studies is strongly recommended.
What this review adds?
The insufficient evidence base for telephone advice lines that we identify here stems largely from a lack of comprehensive and robust evaluations. The predominance of descriptive results (focussing on who calls, when and why they call and how calls are handled by responding staff) reflects findings from previous reviews of telehealth 69 and digital technologies used in palliative care practice without a strong evidence base.70,71
To determine the effectiveness of telephone advice lines on an individual and population level in relation to costs, prospective studies with longer follow-up periods and linked to routine data identifying service use 72 are necessary. Adhering to such standards would promote more rigorous and comparable research and help build an evidence base for effectiveness.
Consistent description of advice line models will facilitate future evaluations; a framework to describe key components of telephone advice line models is proposed in Supplemental File 2.
Strengths and limitations
A major strength of this review is its relevance and rapidity. Finding specific and evidence-based ways to improve community-based palliative and end of life care is important if the growing demand for community-based care is to be met. Telephone advice lines are currently garnering much interest in policy and practice and it is important to provide a synthesised evidence-base to inform future development and implementation of these services. The decision to include all relevant articles identified in our search, regardless of their quality appraisal also strengthens the study, as we could demonstrate the poor scientific standard of the existing literature, with a third of the identified studies not judged as reaching the criteria of empirical research. By only including peer-reviewed articles, however, we might have missed relevant evaluations of additional telephone advice lines in published but not peer-reviewed reports, which is a limitation. Notably, not searching grey literature sources might have led us to overlook pilot studies, reports or audits from governments or organisations. Grey literature, however, can be challenging to include in rapid reviews since they are often complicated to search for, extract data from and assess quality of. 73 While exclusion of grey literature might lead to overestimating intervention effects, it has been found to have a minimal impact on the risk of bias of reviews. 74 The choice of a rapid approach resulted in searching a limited number of databases and supplementary searching of forward and backward citation searching was not utilised. However, this is in line with recommendations for rapid review methodology. 22 Moreover, our search strategies were carefully designed and tested against known relevant studies by an experienced information specialist, strengthening the rigour of the review.75,76
Most of the abstract and title screening was conducted by a single reviewer. This was useful to accelerate the review while providing consistency in approach, but might have increased the risk of missing relevant studies. 74 Nevertheless, single screening has been found to be equally sensitive for providing a sufficient evidence base in studies with focussed clinical review questions as dual screening. 77 In addition, the use of a single reviewer to extract data with verification by a second has been found to be an acceptable timesaver that does not increase the risk of bias. 74
The inclusion of PPI throughout this review, including discussions with PPI representatives with lived experience of end-of-life care at several stages of the study process, using both one-time and continuous approaches, 35 to guide data extraction, synthesis and presentation of results, is a strength and enhances the relevance of the study for patients and carers.
Conclusion
Despite being recommended in policy and increasingly used in community-based palliative care services, evidence for the clinical and cost effectiveness of telephone advice lines is limited. Existing evidence primarily constitutes descriptive reports of service use and service structures, and qualitative accounts of carers’ and patients’ experiences of using telephone advice lines. Overall, our findings suggest that telephone advice lines offer guidance and reassurance that can support care at home and reduce avoidable emergency care use in the last months of life. However, the variability in reporting, and poor methodological quality, across studies hindered meaningful synthesis evidence regarding patient or carer and health care system outcomes. Development of new telephone advice line services must include patients and carers to ensure that needs and preferences of intended users are considered. Robust comparative studies using quasi-experimental or experimental methods with longer follow-up periods are necessary to guide policy and practice. We provide a framework of components to describe telephone advice line models in research reporting to strengthen the evidence base.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241248544 – Supplemental material for The effectiveness of out-of-hours palliative care telephone advice lines: A rapid systematic review
Supplemental material, sj-docx-1-pmj-10.1177_02692163241248544 for The effectiveness of out-of-hours palliative care telephone advice lines: A rapid systematic review by Therese Johansson, Rachel L. Chambers, Thomas Curtis, Sophie Pask, Sarah Greenley, Molly Brittain, Anna E. Bone, Lynn Laidlaw, Ikumi Okamoto, Stephen Barclay, Irene J. Higginson, Fliss E.M. Murtagh and Katherine E. Sleeman in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241248544 – Supplemental material for The effectiveness of out-of-hours palliative care telephone advice lines: A rapid systematic review
Supplemental material, sj-docx-2-pmj-10.1177_02692163241248544 for The effectiveness of out-of-hours palliative care telephone advice lines: A rapid systematic review by Therese Johansson, Rachel L. Chambers, Thomas Curtis, Sophie Pask, Sarah Greenley, Molly Brittain, Anna E. Bone, Lynn Laidlaw, Ikumi Okamoto, Stephen Barclay, Irene J. Higginson, Fliss E.M. Murtagh and Katherine E. Sleeman in Palliative Medicine
Footnotes
Author contributions
T.J. was responsible for the design of the study, with critical input from all authors. S.G., T.J. and S.P. developed the search strategy and S.G conducted the searches. T.J., T.C., R.C., M.B. and A. E. B. screened articles for inclusion, extracted data and performed quality appraisal. K.E.S., I.J.H, F.E.M.M and S.B. won funding. All authors contributed to analysis and interpretation of data. T.J. was responsible for drafting and revising the manuscript. All authors critically revised the manuscript for intellectual content, and read and approved the final manuscript.
Data availability statement
This review is registered on the PROSPERO database (CRD42023400370, available at crd.york.ac.uk/prospero/display_record.php?RecordID=400370) and the full search strategy is provided in the Supplemental Material. Inclusion/exclusion criteria and quality appraisal results are available in the article. Additional data will be made available upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of the Better End of Life Programme which is funded by Marie Curie (grant MCSON-20-102) and carried out by King’s College London in collaboration with Hull York Medical School, University of Hull and University of Cambridge. The funder was not involved in the study design, analysis or interpretation of results. K.E.S. is the Laing Galazka Chair in palliative care at King’s College London, funded by an endowment from Cicely Saunders International and the Kirby Laing Foundation. I.J.H. is an NIHR Senior Investigator Emeritus. F.E.M.M. is a National Institute for Health Research (NIHR) Senior Investigator. I.J.H. and S.B. are supported by the NIHR Applied Research Collaboration (ARC) South London and NIHR ARC East of England, respectively. The views expressed in the report are those of the authors and not necessarily those of the NIHR, or the Department of Health and Social Care.
Ethical approval and consent
Ethical approval was not required for this review as there was no direct patient contact or access to individual participant data.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.