
Abstract
Background:
Telephone advice lines have been recommended internationally to support around-the-clock care for people living at home with advanced illness. While they undoubtedly support care, there is little evidence about what elements are needed for success. A national picture is needed to understand, improve and standardise service delivery/care.
Aim:
To explore telephone advice lines for people living at home with advanced illness across the four UK nations, and to construct a practical framework to improve services.
Design:
A cross-national evaluation of telephone advice lines using structured qualitative interviews. A patient and public involvement workshop was conducted to refine the framework.
Setting/participants:
Professionals with responsibilities for how palliative care services are delivered and/or funded at a local or regional level, were purposively sampled.
Results:
Seventy-one interviews were conducted, covering 60 geographical areas. Five themes were identified. Availability: Ten advice line models were described. Variation led to confusion about who to call and when. Accessibility, awareness and promotion: It was assumed that patients/carers know who to call out-of-hours, but often they did not. Practicalities: Call handlers skills/expertise varied, which influenced how calls were managed. Possible responses ranged from signposting to organising home visits. Integration/continuity of care: Integration between care providers was limited by electronic medical records access/information sharing. Service structure/commissioning: Sustained funding was often an issue for charitably funded organisations.
Conclusions:
Our novel evidence-based practical framework could be transformative for service design/delivery, as it presents key considerations relating to the various elements of advice lines that may impact on the patient/carer experience.
People living at home with advanced illness and those that care for them need access to dedicated palliative and end-of-life care 24 h a day, 7-days a week.
While understanding of telephone advice lines often exists at a single service level, there is limited knowledge in terms of which elements are needed for success or how to ensure effective and equitable provision at a national level.
This paper provides an understanding of multiple telephone advice line services available, including at a national level, and identifies a lack of consistency and challenges with integration between available services.
Promotion of dedicated advice lines (or an area equivalent) needs to ensure that people with advanced illness are aware of how to access such support, but there is variation in how this is done.
Incorporating the views of patients with advanced illness and carers in the development of telephone advice is essential to ensure the care delivered is centred around their needs.
All people with advanced illness and their families should have ready access to a dedicated telephone advice line, which rapidly delivers the right care.
Telephone advice lines need good local or regional knowledge; national level services may not achieve this.
The novel practical framework developed in this research (using key considerations from professionals and patient and public involvement) can be used to guide how services are designed and delivered.
Background
Ageing populations, and the rapid projected rise in multiple health conditions, present global challenges for palliative care. 1 Demand for community-based palliative care is anticipated to increase worldwide, 1 but resources are lacking. 2 Palliative care has demonstrable benefits for people with advanced illness,3 –5 and to healthcare systems (where modest investments in community-based care have enabled fewer deaths in hospital).6 –10
Community-based palliative care is provided by numerous professionals with variable training and expertise.3,11,12 This includes primary and community care teams (e.g. GPs and district/community nurses), social care teams (e.g. home care workers) and specialist palliative care teams. 13 Increasing community-based provision is necessary for the growing demand and to reduce pressure on acute services,1,14 but is challenging and variable.2,5,15,16
Out-of-hours services (i.e. overnight, and weekends or public holidays) are responsible for providing healthcare for two-thirds of the week.17,18 Unscheduled out-of-hours care (e.g. symptom management) is often needed,19,20 and has been identified as a priority for patients, carers, and policymakers. 21 One means of providing round-the-clock palliative care is via dedicated telephone advice lines, which aim to provide immediate access to adequate support.14,22,23 They can be a useful tool for ensuring that palliative care is widely and readily available to all who need it (regardless of age, diagnosis or place of care), 24 and in supporting patients and carers through crises. 25
People living at home with advanced illness and their carers should have access to dedicated telephone advice and support 24/7,26–30 which has long been recommended as a minimum requirement of care in some countries.23,30,31 Yet, dedicated advice lines are still not universally available despite being recognised as beneficial to delivering care at home or being a priority to achieve. 23 There also remains a limited understanding of which elements are needed to ensure telephone advice lines work well. Nor has regional or national equity of access been considered.2,32–35
Aim
To explore telephone advice lines for people living at home with advanced illness across the four UK nations.
Objectives
(1) To explore professional perspectives on provision and delivery of telephone advice lines available for adults with advanced illness, and their family carers.
(2) To gain a cross-national perspective on the provision of telephone advice lines, including gaps and variations in care.
(3) To construct a novel practical framework of key considerations for improving telephone advice line services.
Methods
We report this study according to the Standards for Reporting Qualitative Research (Supplemental File 1), 36 and patient and public involvement (PPI) in line with the GRIPP2 – Short Form 37 (Supplemental File 2).
Defining telephone advice lines.
Study design
A cross-national evaluation of telephone advice lines using structured qualitative interviews to explore professionals’ perspectives regarding telephone advice lines for those with advanced illness and their family carers in their local area. Further details are summarised elsewhere (see Better End of life Report). 2
Setting
We focussed on obtaining a UK-wide understanding (in relation to different geographies – local/regional) from professionals in the direct provision of palliative care. Interviews were conducted remotely, either via Microsoft Teams or telephone.
Population
Participants were professionals with responsibilities for how palliative care services are delivered and/or funded at a local or regional level (e.g. service managers, senior clinicians and commissioners).
Sampling
To ensure regional and national perspectives were fully represented, we purposively sampled by geographical area and nation. The UK has around 860 palliative and end-of-life care services, serving over 65 million people, with ~1.3 services per 100,000. 38 Professionals were recruited purposively by approaching the 42 Integrated Care Systems in England, the seven Health Boards in Wales, the 14 Health Boards in Scotland, and the five Health and Social Care Trusts in Northern Ireland (see Appendix 1). We subsequently employed a snowball sampling approach to ensure purposive sampling criteria were met.
Recruitment
An initial invitation template was provided to those helping us to identify potential participants, which gave a brief explanation about the study and invited them to contact the research team if they wished to participate. Those who expressed willingness to participate were referred to the research associate (SP), who corresponded with potential participants via email and provided them with the participant information sheet.
Data collection
Interviews were scheduled at a suitable date/time via telephone or video link with those wishing to take part. Verbal consent was obtained using a consent script prior to conducting the interview. Interviews were audio recorded using an encrypted digital voice recorder. A topic guide (see Appendix 2) was developed around aspects of out-of-hours care that have been identified as important by patients, carers and professionals as part of a previously conducted Delphi study. 39 This included whether a dedicated advice line for patients with advanced illness and carers was available (including out-of-hours), expertise of call responders, call responder’s access to clinical information and availability of electronic coordination systems. Data were collected between the 21st December 2021 and 1st June 2022. Interviews were conducted by a non-clinical postgraduate research associate experienced in qualitative research (SP), and previously known in a professional capacity to two participants recruited. SP transcribed several interviews (alongside AM, RLC and PGM) or reviewed for clarity, which ensured immersion in the data. Anonymised electronic copies of transcripts were sent to participants for respondent checking.
Data analysis
NVivo 40 was used to support data analysis. Drawing on Braun and Clarke’s 41 approach, an inductive thematic analysis was conducted by SP. We sought to identify, analyse and report patterned meaning relevant to the research question (i.e. considering its breadth and purpose) and perspectival diversity in the data (such as local context). An iterative approach was used rather than treating phases as distinct and unidirectional. 41 SP read and re-read the transcripts to gain a sense of participants’ perspectives. Data were coded by SP following scrutiny of the transcripts in the familiarisation phase to maintain consistent interpretation and classification of the data, detailing descriptive and semantic participant-driven codes to reflect explicitly-expressed meanings. Coding was shared and discussed with other members of the research team to allow for further reflexivity, acknowledging the research team’s experiences and beliefs influencing the interpretative analysis of the data. Initial themes were generated, and then further developed, reviewed and refined using consecutive rounds of discussions among the research team to build the overall ‘story’ that could answer the research question. Identified themes were then used to construct a practical framework.
Saturation (i.e. data-, thematic- or code-) was not considered a useful concept in this approach. Instead, focus was given to the desired diversity in the sample to reflect the varied approaches to funding and delivering services across geographies, and analytic goals. Quotes are presented by geographical area.
Patient and public involvement
This mapping exercise only recruited professionals, as it has been noted that public misconceptions about palliative care limits knowledge of services.2,42 –44 However, we worked with a PPI group to ensure insights from people living with advanced illness and carers were included. A workshop was held online with 13 patients and/or carers to review findings, and bring the lived experience perspective to help shape these, using an independent facilitator in June 2023 (see Supplemental File 3 for more details).
Ethical approval
Ethical approval was granted by the Hull York Medical School Ethics Committee (Reference 21/22 7). Local governance approvals from ICBs, Boards and Trusts were obtained as required.
Results
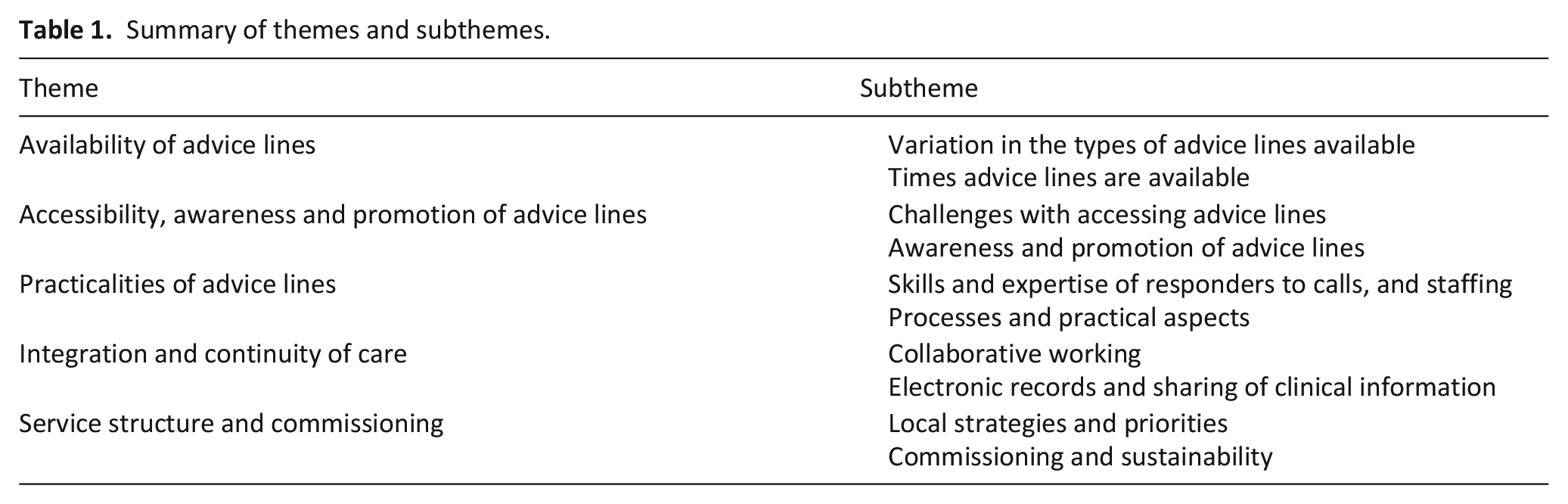
Interviews were conducted with 71 professionals, relating to 60 geographical areas across the UK (see Appendix 3). Of those interviewed, 27 were strategic/clinical leads or managers of service(s), 21 had responsibilities for the planning/funding of local services, 36 were senior clinicians and three had a specific service development role (16 professionals had more than one role). Their average years of experience was 19.3 years (range 3–40) years. Five themes were identified (see Table 1).
Summary of themes and subthemes.
Availability of advice lines
Variation in the types of advice lines available
Professionals described 10 distinct types of telephone advice lines (see Table 2). The route to accessing help (particularly out-of-hours) was complicated by the variety of different advice lines available, which often resulted in patients and their family carers defaulting to national provision that addressed all urgent health issues (e.g. emergency and non-emergency medical helplines).
Types of advice lines, as discussed by participants.
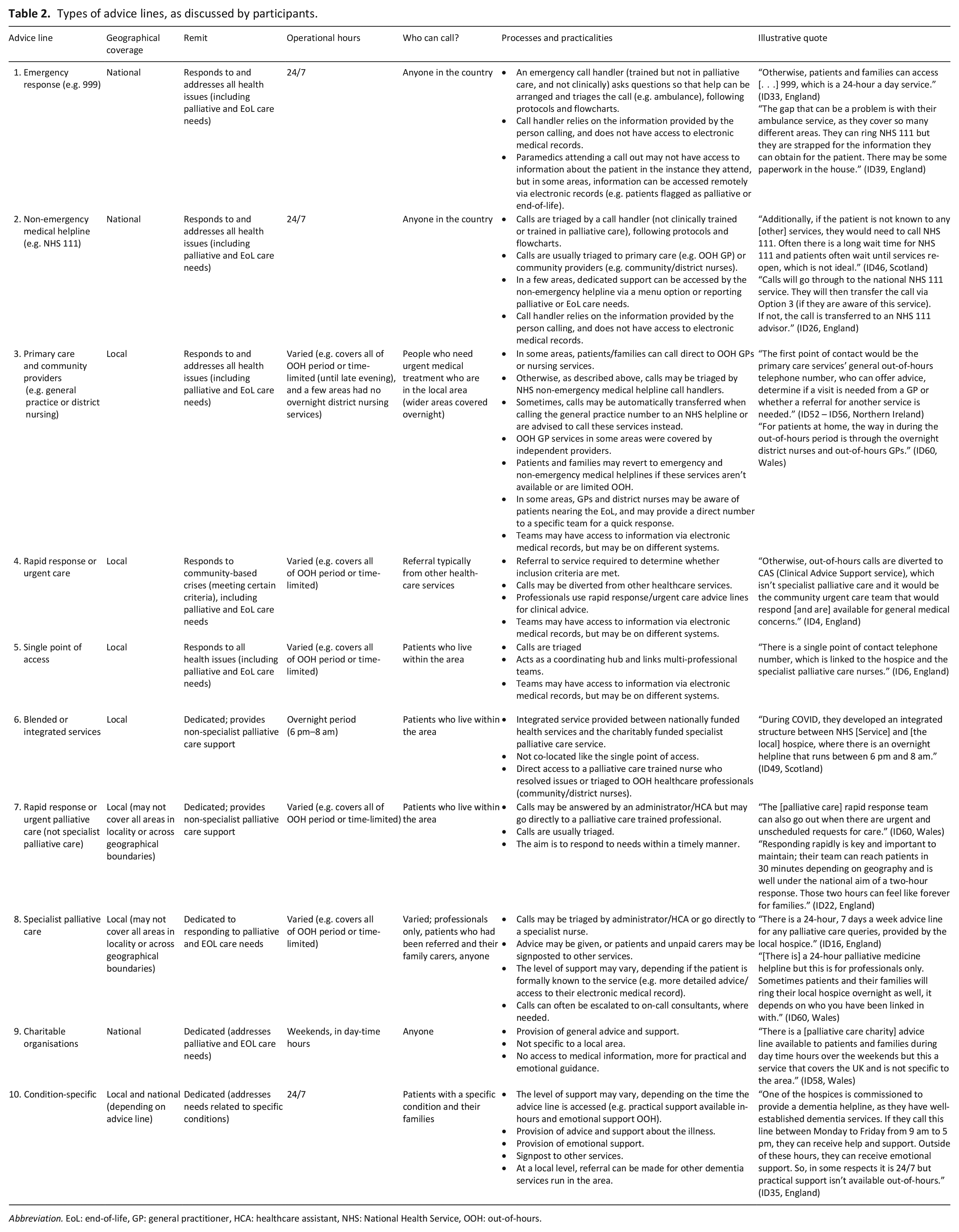
Abbreviation. EoL: end-of-life, GP: general practitioner, HCA: healthcare assistant, NHS: National Health Service, OOH: out-of-hours.
Availability of dedicated advice lines varied. A dedicated advice line was sometimes considered an impractical approach for managing out-of-hours care in sparsely populated regions, and statutory NHS out-of-hours services were considered able to address palliative and end-of-life care needs.
They do not have one telephone line dedicated to palliative and end-of-life care needs/advice across the whole of North Wales for patients and their families, as it would not be practical. Patients will phone their key workers when they need support and there is always someone to call. For patients at home, the way in during out-of-hours period is through the overnight district nurses and out-of-hours GP. ID60, Wales
The availability of different numbers to call for out-of-hours services could lead to confusion about who patients and family carers could call for help. Knowing who to call was dependent on what numbers had been provided to the patient and their family carer throughout their interactions with healthcare providers, and would vary on a person-by-person basis.
[Patients and family carers] can have a clutch of numbers, and in a crisis situation, it’s challenging to know who to ring – all of them, none of them or 999. It would depend on the family caregiver and how they cope with the situations they are managing. ID1, England
There was also local variation in numbers available to call between in- and out-of-hours; sometimes patients and family carers needed to call a different number/select from a menu of options based on their area.
[One area] are served by community nurses from [the local hospice]. These clinical nurse specialists are on-call and this team have a telephone line for their patients that can be accessed out-of-hours. For patients in [another area], they have a much smaller team covering the area, who are available from 9am until 5pm between Monday and Sunday. From 5pm until 9am, they have an arrangement that the [hospice] nurses cover their area. So, patients from [one area] will have access to the same one number, whilst patients from [the other] will have two numbers (one for in-hours Monday to Sunday, and out-of-hours). ID42, England
Dedicated advice lines were perceived by professionals as likely to lead to more timely care for patients with advanced illness, with generic lines sometimes leading to long waits and taking time and effort to navigate.
For patients at home, the way in during out-of-hours period is through the overnight district nurses and out-of-hours GPs. [. . .] [The region aims for] response times [that] are within the hour but there may be some delays depending on staffing and clinical demands at that time. ID60, Wales
Times advice lines are available
Operating hours of advice lines varied. Numerous advice lines were available 24/7. These included emergency services, non-emergency medical helplines, some primary care and community nursing providers and some dedicated advice lines. Variation in when services were available created complexity and inconsistency, and sometimes left gaps.
In [the area], there is a blended service [i.e. advice line between NHS services and the hospice] with out-of-hours. This service starts at 7pm, so there is a gap between 5pm and 7pm. In [the city], the out-of-hours nursing is from 5pm until 7am. In all areas, there is a gap in services between 7am and 8am. ID48, Scotland
Accessibility, awareness and promotion of advice lines
Accessibility
Access to dedicated advice lines was often influenced by whether a person was known to specialist palliative care services or not, and out-of-hours referral/registration were only possible in some areas.
If you aren’t known, then you do get the raw deal on everything, as you just don’t have that support available. They would then just have to go via NHS 111, which would likely result in an ambulance attending and being taken to hospital when that was not necessarily what was wanted or needed. ID35, England
Awareness and promotion of advice lines
Most areas offering dedicated advice lines wanted all relevant patients and family carers to know what support is available and how to access it, but recognised that this was not always achieved.
There is an issue of people knowing and recognising what is available to them at home in terms of care and support. There is an assumption that someone else might inform the patient about what is available out-of-hours, and it is important to empower them and review their situation. ID41, England
Some dedicated advice lines were extensively advertised. In other areas, it was acknowledged that patients and family carers would often be unaware of dedicated advice lines available, and would instead use other more general advice lines (e.g. emergency and non-emergency medical helplines). Nevertheless, there was an assumption that patients and their carers could locate the number.
The advice line would be patchy in the sense that not everyone would be aware of it. It is not necessarily advertised. Unless you were looking for it, you would not find it. This is potentially the bigger issue as there are advice lines available but people don’t always know about it. ID11, England
Different approaches for promotion were used, including: word of mouth, websites, leaflets, care packs/folders and local communications (for professionals to share with patients and carers).
Practicalities of advice lines
Skills/expertise of call resp onders
The skills and expertise of call responders varied and usually related to the advice line model, with more general lines being less likely to have responders either clinically trained or trained in communicating about palliative and end-of-life needs.
On one end of the continuum were NHS call handlers, who were not clinically trained (following checklists directed towards generic health concerns) and unlikely to have received training related to palliative and end-of-life care. In contrast, dedicated advice lines were predominantly answered by nurse specialists (with different levels of seniority), who were clinically trained in palliative care. Training initiatives and resources were considered essential to support call responders in strengthening skills, competencies and comfort, particularly for those without clinical expertise.
They are currently trialling a healthcare support worker taking the first call because they find that they are better able to signpost people and solving their problems straight away. Particularly with some calls where specialist intervention is not required, where it may just be that the person has run out of continence pads or [is] unable to reach their GP. Healthcare support workers are great at getting people through to the right place. ID7, England
Processes and practical aspects
Patients and family carers would call for a number of reasons, including symptom management/medications, and nursing and urgent care needs, especially when health is deteriorating. Family Carers were the main callers to advice lines. It was emphasised that those calling did not always need practical advice, but often reassurance and psychological support alone.
If you have a well-fielded call from a family in distress, you can ensure the patient is where they need to be (such as home). A phone call can be enough to allay their fears. Out-of-hours or telephone support has an important part to play. Their team has avoided an admission by talking [about] what is happening with the family. ID38, England
A range of processes were described, including signposting, triaging, advice, medication management/prescribing, home visits (if needed) and follow-up. For dedicated advice lines, signposting to other services was common, especially when patients were not known to the service provider. This could lead to delays in obtaining help, but could also mean care was coordinated on the patient’s behalf.
A lot of the calls might be signposted elsewhere, such as GPs, hospitals and Macmillan nurses. The hospice will contact other professionals on the patient’s behalf if needed. ID16, England
Triaging was a common process across advice lines (particularly for the non-emergency medical helpline and some dedicated advice lines), where calls would be fielded by a telephone responder and then forwarded to an appropriate professional. Participants reflected that this sometimes delayed access to support; avoiding elongated processes was seen as essential.
Out-of-hours GP’s used to have a direct number that patients could ring, including palliative care patients. They are in the process of moving over to NHS 111, which now means that calls are triaged by NHS 111 and then referred on to the appropriate service (e.g. district nursing, out-of-hours GP). ID58, Wales
Some generic advice lines had processes which enable identification/prioritisation of patients with advanced illness, but again, this occurred only if previously known to palliative care services.
If a patient calls 111 and they have a special note on their [clinical record] indicating they are palliative or end-of-life, they will go straight through to a clinician (instead of a call handler). ID30, England
Patients and carers were reported to receive more timely advice when call handlers with clinical expertise were directly accessible, which was primarily through dedicated advice lines. With dedicated advice lines, staged advice could also be provided (from nurse specialists to consultants) when calls need to be escalated. In some areas, patients and family carers would seek advice by contacting their local hospice, despite these hospices not being commissioned to provide a dedicated advice line.
The local hospice can be contacted for advice between 8am and 8pm, but there is less capacity for visiting and it is not a dedicated service as it is in [neighbouring area]. There is no specific helpline but patients [sometimes] call the general number of their local hospice. Otherwise, patients and families can access 111 or 999, which is a 24-hour a day service. ID31, England
Where services were limited out-of-hours, there was a concern about providing advice without clinical backup if a visit is required.
It was quite problematic for part of the area, as they don’t have a visiting GP service out-of-hours, and there was concern about how palliative care advice could be given, as you want to ensure there is clinical backup if a review is needed. ID42, England
Integration and continuity of care
Collaborative working
Joined up working was seen as essential to delivering good care. Advice lines that functioned within a single point of access where multidisciplinary professionals (e.g. non-medical prescribed, specialists and physiotherapists) were co-located were perceived as promoting joined up working between healthcare providers in the area, acted as a centralised access point and helped guide the care delivered to patients and family carers.
An integrated service means that there is consistency in the advice, documentation, and guidance for palliative care and specialist palliative care across the area. So that when people ring for advice they will always get the same advice and that all the guidance is exactly the same, and it only changes when it needs to and where ever people come across a patient the documentation will be the same. ID13, England
Electronic records and sharing of clinical information
The access to and sharing of a patient’s clinical information was considered essential to provide safe, timely and informed care out-of-hours.
Challenges exist with the infrastructure and how the systems communicate with each other, which can delay the sharing of information. ID57, Wales
One particular challenge was the use of multiple electronic platforms and whether ‘read’ and/or ‘write’ permissions were given to teams working in the community, which could be particularly challenging across geographical boundaries. This meant a number of call responders would be reliant on the information provided by the patient or family carer.
Particularly with cross-boundary patients there can be difficulties in accessing information with a neighbouring Health Board, for example, district nursing falls under one Health Board’s remit and GP service within another. ID57, Wales
In some instances, dedicated platforms (electronic palliative care coordination systems) were developed to share essential information between different professions. However, these were often used variably.
An electronic palliative care coordination system is currently being embedded into SystmOne [electronic medical record system] and is being widely implemented so that it is freely available for everybody but there is variable use [. . .] creating and accessing records. It is still in the implementation phase, so it is not possible to say that all providers have access to information. The hospice can register a patient on SystmOne if they get an enquiry, and setup a share but it depends on getting the necessary permissions in the other direction as well, which is challenging out-of-hours. ID1, England
Service structure and commissioning
Local strategy and priorities
A few areas conducted mapping exercises to enable understanding of the level of support available, and how services are structured and used. However, funding to conduct such mapping activities was not always available.
The ICS put a bid together to try and secure additional funding to do a mapping of what support is available via telephone, identify gaps and try and level up but their bid was unsuccessful. ID1 and ID2, England
Areas acknowledged the challenges with identifying patients with advanced illness to enable access to appropriate services and support.
One of the avenues they are exploring for [area name] is having a single point of access for all patients, because historically the area has not been good identifying the most appropriate patients. ID35, England
In some areas, the development and organisation of dedicated advice lines was reported to be influenced by how palliative care was prioritised within local strategy.
Over the last year and a half, they have developed their 5-year strategy plan and a dedicated out-of-hours telephone advice line is one of the key elements. [The area is] in the early scoping stages of identifying what the advice and coordination hub would look like. ID38, England
A few areas described the involvement of patients and family carers, alongside other stakeholders, in the development of local palliative care provision, but these were the exception.
There is also a clinical engagement group, which brings together the professionals involved in palliative care provision. There is also a user and carer subgroup, which brings together people who are at the end-of-life and those who care for people at the end-of-life. They have the opportunity to inform the work of the regional programme board. ID52 – ID56, Northern Ireland
Commissioning and sustainability
Participants described the importance of access to out-of-hours palliative care, and were aware of NICE guidance on this. They recognised the need for appropriate resourcing of these services but acknowledged challenges with funding.
Commissioners need to work with providers. It is very complicated in palliative and end-of-life care because much of the funding is donated via the charitable sector. It is important for commissioners to work to support both the hospice and the statutory providers to provide a NICE-compliant service. ID41, England
Dedicated advice lines were often provided by hospices, but were sometimes hosted by the specialist palliative care team in the community or hospital. The way advice lines were structured was considered a priority for commissioners in some areas, and sometimes lack of integration was recognised.
There is a call centre that runs as part of the district nursing out-of-hours service, and [the specialist palliative care] have been challenged as to why they have a separate telephone line [. . .]. But when this has been evaluated, it was noticed as people on that line do not have specialist knowledge, and tasks will often get passed back to [the specialist palliative care number] anyway. It then just goes a longer route round, [. . .] their experience is that patients then receive a worse service because of this. ID7, England
Equitable access to dedicated advice lines was considered essential, as services that are responsive to palliative and end-of-life care needs were seen to be beneficial to other local services (e.g. community nursing services) and in improving patient and family carer experiences.
Equitable access to these services is so important, wherever you are. The challenges are that the community teams are so stretched, that services tend to take on additional work to support those strained services and it can become difficult to unload that work once it has been taken on. Responding rapidly is key and important to maintain; their team can reach patients in 30 minutes depending on geography and is well under the national aim of a two-hour response. ID22, England
Building a case for sustaining advice lines was crucial, and usually achieved via auditing/evaluation. The volume and timing of calls were considered as one possible criterion to measure service demand, and assess whether resources were used effectively. However, these varied greatly (including different of patterns across in- and out-of-hours).
They are putting together a business case to get the phone line commissioned at the end of the pilot. The pilot has been well received so far. Prior to the pilot line, patients would call the single point of access line for community palliative and end-of-life services (accessed via NHS 111) but this is not available overnight. ID3, England
A reduction in hospital admissions were noted with dedicated advice lines. Although, challenges in capturing this were acknowledged.
Developing a practical framework and PPI reflections
The data collected from the interviews was used to create a practical framework that presents key considerations when developing/maintaining advice lines for community-dwelling patients with advanced illness and their carers. Reflections from the PPI workshop, accompanying this work, largely mirrored the discussion from the interviews with professionals, but also provided new insights. Essential and novel considerations were incorporated into the practical framework (see Figure 1 and Supplemental File 3).
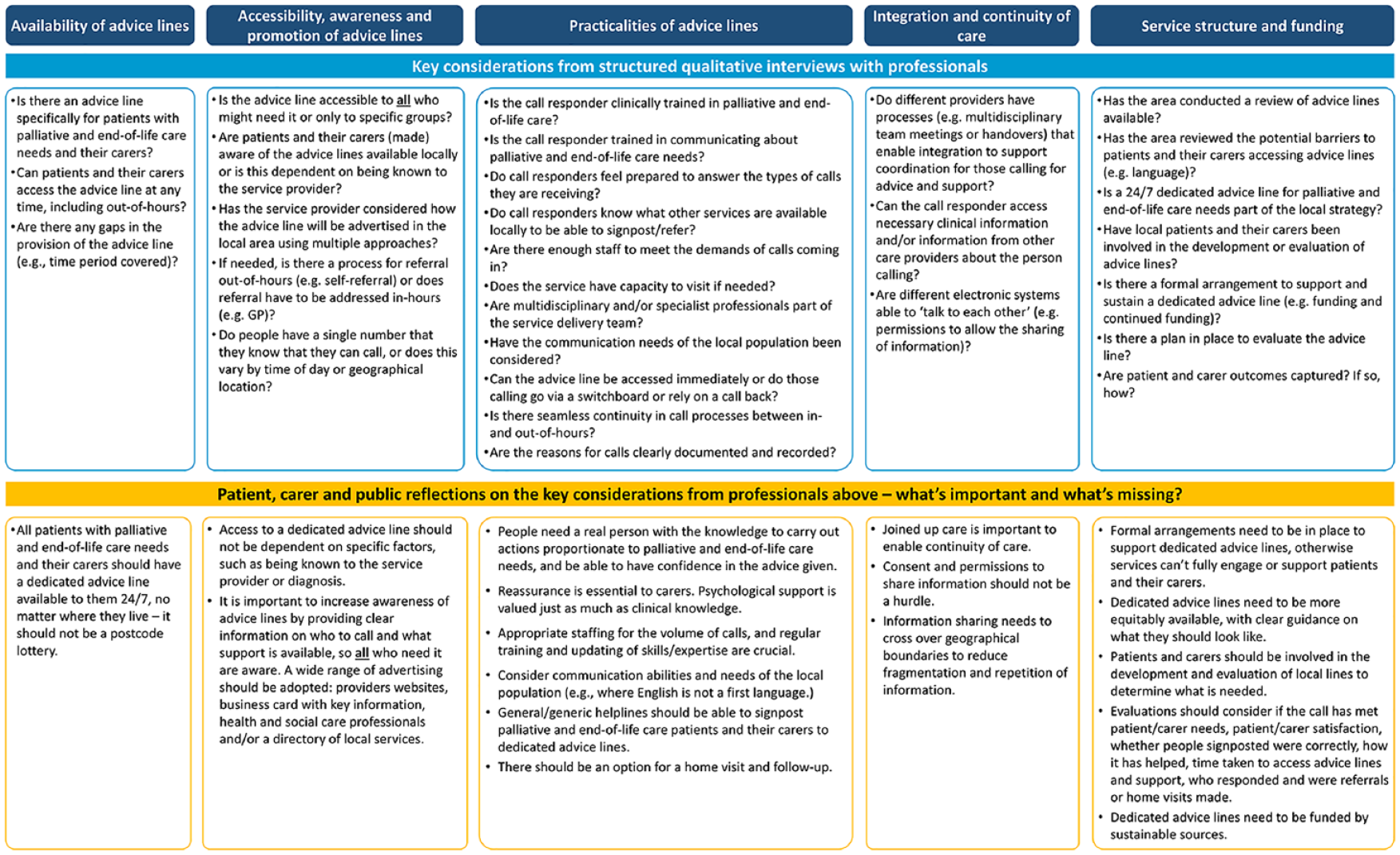
Practical framework for guiding advice lines for patients living in the community with advanced illness and their carers.
Discussion
Main findings/results of the study
Our findings provide, for the first time, an in-depth understanding of advice lines for community-dwelling patients with advanced illness and their family carers at a national level. The delivery of telephone advice lines is a complicated patchwork across the four nations of the UK; this complexity leads to uneven access, considerable delays and notable inefficiency. People with advanced illness and their families are sometimes not able to access care, and even if care is accessed, it may not be timely. Getting to the right person with the right skills and expertise is often challenging. Telephone advice lines delivered at a national level often do not have the local or regional knowledge to be effective. Generic advice lines are challenging for patients with advanced illness and their carers to navigate (e.g. an emergency advice line). The novel framework we provide can guide the way in which services are designed and delivered to meet patient and family carers needs, and to support them to remain at home.
What this study adds?
Key requirements to facilitate good practice mirror previous research, including: round-the-clock availability; a single telephone number; adequate resourcing; competent professionals to answer calls; a compassionate and practical response; clear lines of responsibility where issues can be escalated; ongoing staff training and service review; access to medical records; a standardised form to collect call-related information; and advertising to raise community awareness.25,45 Our data also raises issues around identification of patients with advanced illness and referral processes, especially when self-referral is not available out-of-hours when calling dedicated advice lines. Multi-modal approaches to advertising are needed to promote services available out-of-hours. Better understanding of where palliative care is offered may improve access to this care,43,46 and using novel strategies to address the multiple barriers with access and identification would be useful (e.g. reframing from a health services challenge to a community one).47,48
Difficulties with accessing care in-hours has been associated with increased use of out-of-hours services. 49 Urgent and unplanned emergency department attendance is frequent for people in the last year of life.2,19 The rising demand for unscheduled care is a major burden on healthcare systems, 19 and high-quality ‘out-of-hours’ advice lines are an important way to mitigate this.25,50 Ensuring full integration of palliative care into statutory healthcare systems, rather than parallel delivery, will enable consistency of care across settings.51,52 However, investment in workforce and multidisciplinary collaboration is needed to make this happen, 53 including training out-of-hours health and care professionals, improving sharing of clinical information and how advice lines are evaluated (i.e. choosing meaningful patient and family carer outcomes rather than focussing on service utilisation).54–56 Our interviews indicated that some initiatives were short-lived or developed in response to the pandemic. Palliative care services have demonstrated considerable flexibility and ‘frugal’ innovation in the context of the pandemic, 57 but the longevity of these initiatives are important to consider.
Strengths and weaknesses/limitations of the study
Evidence on advice lines is limited, and often orientated around evaluation of single services, including in other countries. 58 There remains a lack of robust evaluation of these types of service. 14 One main strength of this study was providing a national picture, beyond descriptive reports of individual service use/structure. It highlights the variation and gaps in provision, as well as provides a clear structure of advice line elements. This includes how advice lines are situated in healthcare systems and how services are provided. Although these results may be limited in their transferability, elements of the developed framework could have some practical applicability to other high-income countries, and/or potential to guide service development.
Although we endeavoured to maximise geographical coverage to reflect the differences in how services are funded, it was not possible to cover all areas due to resource limitations (i.e. staffing/time). A purposive sampling frame was adopted to support representation from different areas. Another limitation was that only professionals were interviewed, as palliative care services continue to be accessed late in the course of advanced illness.2,42,59 Incorporating patients and family carer priorities/preferences in the planning and development of out-of-hours palliative care services is essential to ensuring that care is person-centred and addresses safety concerns, and has seldom been done with dedicated advice lines.56,60 Therefore, we conducted a PPI workshop and integrated reflections on the evidence provided by professionals.
Implications for clinical practice, policy and research
It has long been recommended that help should be available 24/7 to patients and their family carers.23,31 Yet our understanding of advice lines has advanced on a small scale via audits/evaluations, and remains largely descriptive.14,25,45,56,61–65 Our novel framework is directly informed by evidence and intended to facilitate more effective approaches to developing, enabling and evaluating such services with consideration to all elements that contribute towards the setup and delivery. We recommend:
Service users should be part of service design.
All people with advanced illness and their families should have ready access to a dedicated telephone advice line, which rapidly delivers the right care.
Telephone advice lines need good local or regional knowledge; national level services may not achieve this.
Whilst our results are based on data from the four nations of the UK, the practical framework could be applied to other geographies to assess provision, variations and inequalities, as well as be used in the setting up of new services or in improving the delivery of existing telephone advice lines. Further understanding is needed around the benefits and effectiveness of advice lines (e.g. cost-effectiveness), and which patient and family carer outcomes to evaluate. Patients and their carers need to be involved in the development, implementation and evaluation of advice lines. PPI reflections identified new aspects that require further consideration, including communication needs (such as language/cultural barriers).
Conclusion
Our novel evidence-based practical framework could be transformative for service design and delivery, as it presents key considerations relating to the various elements of advice lines that may impact on the patient and family carer experience. Additionally, the practical framework presented can provide a more robust approach to considering the essential elements involved. Improving the way in which advice lines are accessed and delivered could help patients to remain at home, where possible. Dedicated advice lines are viewed as useful for streamlining and responding to palliative and end-of-life care needs, as long as they are implemented well.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163241242329 – Supplemental material for Telephone advice lines for adults with advanced illness and their family carers: a qualitative analysis and novel practical framework
Supplemental material, sj-pdf-1-pmj-10.1177_02692163241242329 for Telephone advice lines for adults with advanced illness and their family carers: a qualitative analysis and novel practical framework by Sophie Pask, Allen Omoruyi, Ahmed Mohamed, Rachel L Chambers, Phillippa G McFarlane, Therese Johansson, Rashmi Kumar, Andy Woodhead, Ikumi Okamoto, Stephen Barclay, Irene J Higginson, Katherine E Sleeman and Fliss EM Murtagh in Palliative Medicine
Footnotes
Appendix 1: Purposive sampling strategy by nation
Appendix 2: Topic guide
Appendix 3: Map of geographical areas covered by interviews (adapted from Pask et al. 2 )
Acknowledgements
We would like to thank those who took part in the study for their time. We would also like to thank Hopkins Van Mil for contributing to the online workshop with patients and family carers.
Author contributions
SP, FEMM, KES and SB were responsible for the conceptualisation and design of the study, with critical input from all authors. SP conducted all structured interviews with professionals. Interviews were transcribed by SP, RLC, AM and PGM, and analysed by SP, with all authors providing guidance on and the development of themes. SP was responsible for drafting and revising the manuscript. All authors critically reviewed and revised the manuscript, and read and approved the final manuscript. RK and AW led on the development of PPI activities in this study and how PPI reflections could be integrated alongside the data from professionals.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of the Better End of Life Programme, which is funded by Marie Curie (grant MCSON-20-102) and awarded to KES, IJH, FEMM and SB. The research was carried out by King’s College London in collaboration with Hull York Medical School, University of Hull, and University of Cambridge. The funder was not involved in the study design, data collection and analysis or interpretation of results. KES is the Laing Galazka Chair in palliative care at King’s College London, funded by an endowment from Cicely Saunders International and the Kirby Laing Foundation. IJH is an NIHR Senior Investigator Emeritus. FEMM is a National Institute for Health Research (NIHR) Senior Investigator. IJH and SB are supported by the NIHR Applied Research Collaboration (ARC) South London (SL) and NIHR ARC East of England, respectively. The views expressed in the report are those of the authors and not necessarily those of the NIHR, or the Department of Health and Social Care.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.