
Abstract
Background:
Growing global demand for palliative care services has prompted generalist clinicians to provide adjunct support to specialist teams. Paramedics are uniquely placed to respond to these patients in the community. However, embedding palliative care principles into their core business will require multifactorial interventions at structural, healthcare service and individual clinician and consumer levels.
Aim:
To develop a palliative paramedicine framework suitable for national implementation, to standardise best practice in Australia.
Design:
Delphi study utilising questionnaire completion; each round informed the need for, and content of, the next round. Free text comments were also sought in Round 1. Two rounds of Delphi were undertaken.
Setting/participants:
Sixty-eight participants took part in Round 1, representing six countries, and 66 in Round 2. Participants included paramedics, palliative care doctors and nurses, general practitioners, researchers and carers with lived experience and expertise in palliative paramedicine.
Results:
Seventeen of the original 24 components gained consensus; 6 components were modified; and 9 new components arose from Round 1. All modified and new components gained consensus in Round 2. Only one original component did not gain consensus across both rounds and was excluded from the final 32-component framework.
Conclusion:
This study has developed a comprehensive national framework addressing the macro-, meso- and micro-level interventions required to standardise palliative paramedicine across Australia. Future research ought to engage a multidisciplinary team to create an implementation strategy, addressing any perceived barriers, facilitators and challenges for applying the framework into policy and practice.
Keywords
When adequately trained and supported, paramedics can enhance person-centred care, reduce avoidable hospitalisations and facilitate the fulfilment of one’s preferred place of death.
Embedding palliative and end-of-life care into paramedics’ core business will require multifactorial interventions at structural, healthcare service and individual clinician and consumer levels.
The Delphi technique is a method of systematically collating expert consultation and building consensus. It is particularly useful for establishing frameworks in complex settings such as palliative paramedicine.
This study gained consensus from an international multidisciplinary expert panel on 32 macro-, meso- and micro-level components of a palliative paramedicine framework, suitable for implementation to standardise practice at a national level.
The expert panel called for stronger inclusion of bi-directional training and multidisciplinary debriefing opportunities between ambulance services and other palliative care providers.
Our findings suggest paramedics should be supported to make complex clinical decisions specific to palliative care contexts with confidence and navigate holistic care pathways that prioritise referral functions available to other community-based clinicians.
Future research should engage a multidisciplinary team to create an implementation strategy, which would reflect any perceived barriers, facilitators and challenges for applying the framework into policy and practice.
In developing the implementation strategy, endorsement of relevant professional associations should be sought, a theory applied to guide next steps and the time and resources required to standardise palliative paramedicine practice across Australia acknowledged. Findings from testing the strategy could have resonance for palliative care providers and ambulance services worldwide.
Background
Growing global demand for palliative care services, and rising international preference for home-based deaths, 1 have prompted an increasing number of generalist clinicians to provide adjunct palliative and end-of-life care support to specialist teams.2–4 The COVID-19 pandemic accelerated this shift towards interdisciplinary palliative care, 5 highlighting the role primary care settings can play in this context. Paramedics already play an integral role in providing unscheduled care to patients in community-based settings worldwide. For example, a recent British retrospective cohort study analysed unscheduled and out-of-hours care for people in their last year of life, following patients as they pass from primary care to ambulance service, to emergency department, to finally being admitted into an in-patient ward. 6 The study identified that the extent of unscheduled care delivered to people in their last year of life, including by paramedics, is significantly greater and more varied than previously reported. The study’s authors concluded that managing more unscheduled care episodes in the community has the potential to reduce hospital admissions and overall costs. 6
Paramedics are uniquely placed to respond to palliative and end-of-life care patients in the community, particularly after-hours when specialist palliative care services might be unavailable. 7 When adequately trained and supported, paramedics can enhance person-centred care, reduce avoidable hospitalisations and facilitate the fulfilment of one’s preferred place of death.1,8 However, attitudes towards expanding paramedics’ role to deliver palliative and end-of-life care in communities varies considerably within ambulance services, across health professions and throughout cultures.9–12
Embedding palliative and end-of-life care into paramedics’ core business will require multifactorial interventions at structural, healthcare service and individual clinician and consumer levels. Previous studies have argued for greater inclusion of paramedicine in palliative care policies and frameworks; 10 discussed whether the role of palliative care ought to be relegated to specialist community paramedics;13,14 identified the barriers to understanding and utilising advance care planning documentation in American pre-hospital settings; 15 explored Finnish paramedics’ palliative and end-of-life care clinical protocol and educational needs; 16 and investigated the essential elements to implementing a Canadian paramedic palliative model of care. 17 However, to our knowledge, no previous studies have outlined the strategies necessary to develop a comprehensive whole-of-system approach to palliative paramedicine.
The Delphi technique is a method of systematically collating expert consultation and building consensus. It is inherently constructivist in nature, and particularly useful for establishing frameworks in complex settings such as this one. 18 The aim of this study was to develop a palliative paramedicine framework suitable for national implementation, by determining the components considered most essential for improving the role of paramedics delivering palliative and end-of-life care in Australian communities. It is hoped the findings will shape a best practice framework suitable for national implementation.
Methods
Design
We employed a Delphi methodology to build systematic consensus from a broad range of experts, underpinned by a social constructivist epistemology. 18 This approach has previously been used in palliative care research to gather international perspectives and develop best practice guidelines and frameworks, especially when clinical trials and large-scale observational research were not possible.18–21 The study adopted the four key methodological features of a Delphi: (1) a group of experts participated on a panel and were questioned about the issue of interest; (2) the process was anonymous to avoid conformity to a dominant view; (3) the procedure was iterative, comprising repeated rounds of enquiry and; (4) the design of subsequent rounds was informed by the summary of group responses from Round 1.18,22 We adhered to the ‘Guidance on Conducting and REporting DElphi Studies’ (CREDES) to ensure robust methodology and reporting. 18
Setting
The focus of this Delphi study was paramedics delivering palliative and end-of-life care in community-based settings. An Anglo-American lens of ambulance services, where paramedics provide care to patients with medical oversight, was adopted throughout, in contrast to the Franco-German emergency physician-led model. 23
Population
To broaden participation and encourage a wide range of international expertise, the target population to be recruited were healthcare professionals, academics and family carers with lived experience and significant expertise in palliative paramedicine in Australia and/or abroad. The healthcare professional and academic discipline sub-groups included paramedicine, palliative care, general practice and emergency medicine.
Sampling approach
We adopted a purposive, then snowballing approach to recruit participants who would become part of an expert panel. Firstly, potential health professional and academic participants were identified through their affiliation with the Australasian Palliative Paramedicine Advisory Group. This study-developed group was comprised of medical directors and senior clinical managers from all Australian and New Zealand ambulance services, and an experienced emergency nurse/palliative paramedicine researcher. We then approached health professional collegial networks with a targeted invitation, including the Australasian College of Paramedicine, Australasian College of Paramedicine Deans, Royal Australasian College of Physicians Chapter of Palliative Medicine, Palliative Care Nurses Australia and Royal Australian College of General Practitioners. International palliative paramedicine opinion leaders with publicly available email addresses were also invited to participate in the Delphi, as well as health professional and family carer participants of our previous study – a qualitative exploration of palliative paramedicine – who demonstrated strong interest and expertise in the topic. Then using a snowballing approach, all initial recipients of the Delphi invitation were also encouraged to forward the email to colleagues and affiliates they believed would be suitable and interested to participate in the study.
Recruitment
All potential participants were initially contacted by email and provided a participant consent form and information sheet, including a background on the topic, the purpose of the study, the intended Delphi process and contact details of the research team. Participants were invited to contact MJ via email to indicate they wished to take part.
Data collection
To gain consensus on which components should be included in a Palliative Paramedicine Framework (Framework), an online Delphi process was conducted using the Welphi platform, 24 incorporating subsequent rounds of feedback until consensus was reached. Materials provided to the expert panel throughout the study, including the participant information statement and round questionnaires, were carefully reviewed and piloted by the research team, to examine understandability and balance. To maintain confidentiality, each participant was assigned a unique identifier which remained consistent throughout the Delphi rounds.
Original proposed framework components
Based on analysis of broader literature and the findings of our three previous studies,3,7,9,13,17,25,26 24 original proposed Framework components were created by the research team for consideration by the expert panel. These components were categorised according to systems-based macro-level interventions, service and community-based meso-level interventions and individual clinician and consumer-based micro-level interventions.27,28 This specific number and typology of components derived primarily from the findings of our previous qualitative study, which sought the attitudes, experiences and perspectives of clinicians and family carers with lived experience of palliative paramedicine. 9 A key finding arising from the study highlighted the need for any future framework to engage a multifactorial approach, thereby capturing the broad scope of components required to standardise practice and evoke sustainable change across the sector. 9 MJ drafted the original components and shared these with the research team for multiple rounds of discussion and refinement, before informal consensus was met and the team was satisfied to put these components to the expert panel in the round 1 questionnaire (Appendix 1).
Round 1 Delphi
A Round 1 Welphi link was sent to all registered participants via email in March 2023, and the questionnaire was open for 2 weeks. The participants completed a short demographic survey within this round to allow the sample to be described. The Round 1 questionnaire included 23 original components separated into three sections: macro-level; meso-level; and micro-level. Participants were asked to rate their level of agreement for each component to be included in the final Framework using a 5-point Likert scale: 1 – strongly disagree, 2 – disagree, 3 – neither agree nor disagree, 4 – agree, 5 – strongly agree. Free text comment boxes were also included after each component in this round, for participants to provide specific feedback and suggest modifications for consideration in Round 2. After each section, participants also had the opportunity to highlight anything that was missing and make suggestions for new components via free text comment boxes. The Delphi Round 1 questionnaire is available in Appendix 1.
Round 2 Delphi
A Round 2 Welphi link was sent to all Round 1 respondents in April 2023, and the questionnaire was open for 2 weeks. The Round 2 questionnaire included 16 original, new and modified components separated into the same three sections. During this round, participants were given the opportunity to revise their responses for any original components that did not reach consensus during round 1. The collective feedback of the expert panel from Round 1 was visible to participants for these original components to help guide their decision making. Participants were also asked to rate their level of agreement for the new and modified components arising from Round 1 feedback, using the same Likert scale. Participants were unable to provide feedback for any of the components via free text comments boxes during this round.
Data analysis
Percentages, median values and interquartile ranges (IQRs) were calculated for each component to describe the spread of answers. These values were then used to determine the level of agreement across the expert panel:18,20
Very high agreement: median = 5; percentage agreement ⩾80%; IQR 0
High agreement: median = 4 or 5; percentage agreement ⩾80%; IQR 1
Moderate agreement: median ⩽ 4; percentage agreement ⩾60%–79%; IQR ⩾1
Low agreement: median < 4; percentage agreement <60%; IQR >1
An a priori criterion for consensus was defined by the research team as a component receiving ‘very high agreement’ or ‘high agreement’ from the expert panel. Those components that received these levels of agreement were retained for the Framework. Those components that received ‘low’ agreement were removed after one round. Those components that received ‘moderate’ agreement were presented to participants for further rounds of rating, after which if they still didn’t reach ‘high’ or ‘very high’ agreement, they would be removed from the Framework.
Round 1 Delphi
Descriptive statistics were automatically generated via the Welphi platform 24 and cross-checked by MJ using Excel. 29 Percentages, median values and IQRs were calculated for each Round 1 component to describe the spread of answers and determine the level of agreement across the panel. MJ qualitatively analysed the free text comments for each section, employing principles of content analysis 30 to categorise feedback accordingly: (1) already addressed in existing component(s); (2) additional information constitutes a new component; and (3) could be used to modify, and thus enhance an existing component(s). MJ read all of the free text comments, familiarised herself with their content, independently identified potential new and modified components, and met with the team to discuss and develop these components. Consecutive dialogues facilitated multidisciplinary perspectives and allowed for consistent interpretation and classification of the feedback data into Round 2 components.
Round 2 Delphi
Percentages, median values and IQRs were again calculated for each Round 2 component to describe the spread of answers and determine the level of agreement across the panel. The a priori criterion for conducting a subsequent round was not met and, therefore, no further rounds were conducted.
Results
Participation
Of the 87 invited experts, 19 declined to participate due to too many other commitments and/or a self-perceived lack of expertise in the area to contribute meaningfully to the Delphi. Sixty-eight participants took part in Round 1, representing six countries and all jurisdictions of Australia, while 66 participants took part in Round 2, representing the same six countries. Table 1 shows demographic and professional characteristics of participants across the two rounds of the Delphi. In Round 1 and 2, 37% and 38% of the expert panel were aged between 45 and 54 years, respectively, 65% and 62% were female, respectively, 44% had a palliative care background and 59% had more than 20 years experience in their profession.
Descriptive characteristics of participants.
Percentages rounded to nearest whole number.
Round 1 Delphi
Seventeen of the original components from Round 1 gained consensus: and were included in the final Framework, as depicted in Figure 1 and Table 3. Six original components gained consensus; however, considering feedback from the expert panel, modifications were made to enhance each of these components for participants to reconsider in Round 2. Nine new components arose from Round 1 feedback: three macro-level, four meso-level and two micro-level. Only one original component did not reach consensus in Round 1: Include a routine question within an ambulance call taker’s algorithm that prompts further questioning about a patient’s palliative care status and notify paramedics before they arrive on scene. This component remained unmodified, for participants to reconsider in Round 2. Table 2 highlights the expert panel feedback from Round 1, including the experts panel’s comments for the component that did not reach consensus, as well as the modified and new components.
Flowchart of Delphi process.
Modifications and additions to Round 2 following free text comments from Round 1.
Levels of agreement for components in Round 1.
Round 2 Delphi
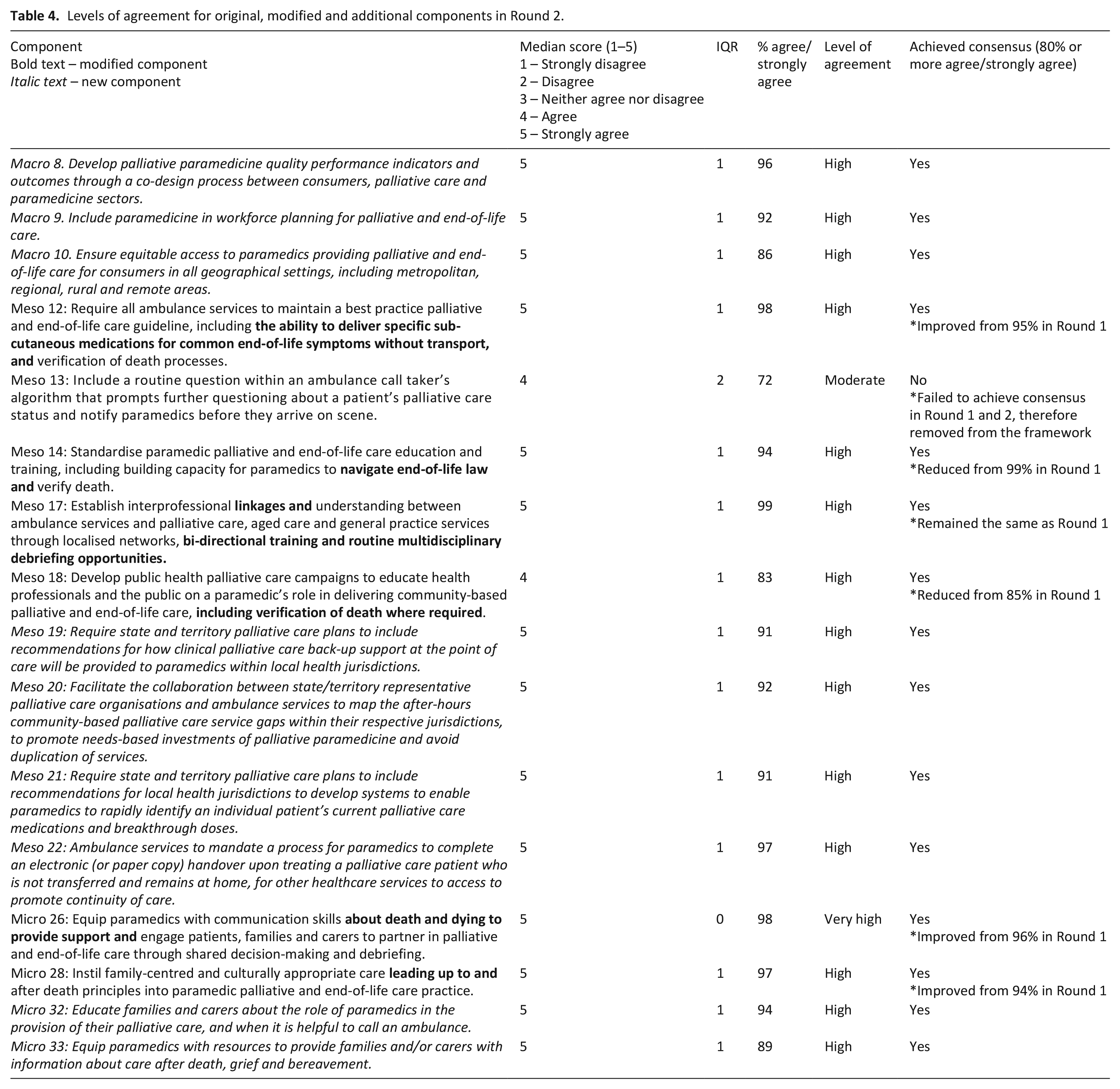
The six modified components and nine new components arising from Round 1, gained consensus in Round 2 and were included in the Framework. The remaining original component failed to gain consensus in Round 2, reducing its consensus score from 75% agree/strongly agree (median 4, IQR 1) in Round 1, to 72% (median 4, IQR 2) in Round 2. These results rendered the exclusion of the component from the Framework. Given all components had now either reached consensus or been removed, no further rounds of Delphi were required. Table 4 highlights the results from Round 2, and Table 5 illustrates the final components of the Framework.
Levels of agreement for original, modified and additional components in Round 2.
Final framework components.

Discussion
Main findings from the study
Paramedic provision of palliative and end-of-life care is an emerging frontier for the discipline globally, with significant potential to assist other palliative care services, specialist and generalist alike, in their provision of care.3,11 However, standardising best-practice to optimise the role paramedics can play requires a multifactorial approach 9 and geographical nuance, especially in a country as large and diverse as Australia. 13 This study allowed a group of international multidisciplinary experts the chance to deliberate the best available evidence, employing their experiential expertise to achieve consensus on a comprehensive range of 10 macro-, 11 meso- and 11 micro-level components for inclusion in the final Framework, suitable for national implementation. Australians were the largest participant pool of the sample, but international experts were added to provide a wider perspective and increase the likelihood the Framework could be relevant in other comparable health systems. The components included structural, healthcare service, community, clinician and consumer-level interventions.
Items included in the framework
Perhaps most prominent amongst the experts’ first round of feedback was the demand for stronger inclusion of bi-directional training and multidisciplinary debriefing opportunities between ambulance services and other palliative care providers, as reflected by our modification to meso 17 in Round 2. These findings are supported by Canadian and American models of palliative paramedicine practice, which substantiate the power of formalising communication and education channels between paramedics and palliative care clinicians.17,31 By requiring each jurisdiction to establish training and debriefing networks between ambulance services and local palliative care providers (including GPs and aged care), mutual understanding of capacities, strengths and weaknesses could be fostered, leading to greater awareness of interdisciplinary palliative care capabilities and a reduction in siloed care.
To continue challenging the curative treatment and transport orthodoxy of ambulance services worldwide, paramedics need to be supported to make complex clinical decisions with confidence, and navigate holistic care pathways that prioritise referral functions available to other community-based clinicians.9,13 Another omission from our original components, as identified by the expert panels’ feedback and new meso-level component 19, was the need for clinical back-up support pathways for paramedics at the point of care. Our authorship team assumed this would already occur in a generalist sense, without articulating it in the Australian context, as some jurisdictions already have these processes in place. However, the Round 1 feedback indicated the expert panel considered specialist palliative care support a desirable Framework component, even if only available via telehealth. This is consistent with the findings of a German study, where emergency medical services personnel perceived paediatric palliative care emergencies to be particularly stressful, and requested a local palliative care contact be available 24/7 to provide clinical guidance and backup where necessary. 32 Furthermore, a Canadian study highlighted the utility of patients with a life-limiting illness being enrolled into a novel treat and refer palliative paramedicine clinical pathway. In sixty-eight percent of cases where this pathway was in place, paramedics engaged in a remote clinical consultation to facilitate care in the home, demonstrating how imperative clinical support can be in mitigating risk and reducing unnecessary conveyance to hospital. 1 In conjunction with formalising training and debriefing opportunities between ambulance services and other palliative care providers, ensuring Australian paramedics have a round-the-clock phone number to call for specialist palliative care clinical support will be an integral step towards incorporating paramedicine into the multidisciplinary palliative care landscape.
The only component to not gain consensus across both rounds pertained to modifying ambulance services’ call algorithms to prompt further questioning about a patient’s palliative care status and notify paramedics when they arrive on scene. While suggested by participants in our previous research to help with triaging, some of the expert panel commented this could be risky strategy and challenging to implement, as detailed in Table 2. Some common justifications provided by the expert panel included the potential insensitivity of the question to a distressed caller, and the increased chance for the non-medically trained call-taker to incorrectly divert an emergency ambulance if they deemed the palliative care patient to be low-acuity.
Future research ought to explore the barriers, facilitators and challenges that the sector, services, communities and individuals would face implementing the components that gained consensus, to inform a strategy to ensure successful translation of the Framework into routine care.17,33 Researchers should seek endorsement for the arising implementation strategy from professional associations, apply a theory to guide the next steps, and acknowledge the time and resources required to standardise palliative paramedicine practice across Australia; the findings of which could have resonance for palliative care providers and ambulance services worldwide.
Implementing the framework in Australia and other contexts
We envisage this newly developed Framework could play an instrumental role in standardising the practice of palliative paramedicine across different jurisdictions in Australia by specifying targeted interventions of change for individual paramedics and other generalist and specialist palliative care clinicians; state and territory-based ambulance services and broader healthcare services involved in community-based palliative and end-of-life care; and national palliative care policies and practices. Incremental phasing in of the Framework components in differing states and territories could allow for efficacious process evaluation and adaption to compliment the diverse needs of metropolitan, regional, rural and remote communities and healthcare systems. To ensure the Framework is fulfilling its intended purpose, a comprehensive evaluation, including cost-benefit analysis, is recommended. This evaluation ought to examine the efficacy of all individual components of the Framework, in addition to the collective whole, to determine its suitability and ensure its sustainability into the future.
Whilst Australians were the largest participant pool of the expert panel in the Delphi study, international experts were also added to provide a wider perspective and increase the likelihood the Framework could be relevant and applicable to other comparable health systems. Opportunities exist to translate our findings and the resulting Framework into other contexts, including in Franco-German ambulance services, where palliative paramedicine is well under way.12,16,34 In addition, the Framework could be adapted for low and middle-income countries, including South Africa and Brazil, where significant gaps in paramedic practice have been established and collaborations already fostered.35,36 Investigating the applicability of our Framework in alternate settings, through qualitative interviews and quantitative surveys with key stakeholders, could assist in the first stages of translating our Framework into future international context-specific policy and best practice.
Strengths and limitations
A consensus method and the use of a Delphi technique were well-suited to developing a framework in this complex, emerging area of palliative care. This study employed a rigorous approach, engaging a large panel of international and multidisciplinary experts. However, we acknowledge that what is ‘important’ in palliative care should be determined, in part, by patients and their families, and this will vary, depending on culture, experience and values. There is evidence of diverse expert panel membership with thirteen countries of origin and Australian First Nations members included in this study, but most panel members are highly educated, of European heritage and living and working in Australia.
Another limitation of this study was the research team selecting experts for the process, potentially leading to preferential selection of participants favourable to our intended research goals and perspectives. However, we aimed to counteract this limitation by clearly defining the target population and sampling approach beforehand and inviting participants to share the invitation within their networks to enhance diversity of the expert panel. This Delphi study did not include the opinions of government policy makers on the expert panel, which could have been a missed opportunity. However, these key decision makers will be important stakeholders to engage in the next phase of the research, when developing an implementation strategy for the Framework.
Conclusion
Despite their traditional emergency response function, paramedic scope of practice is evolving, and they can offer valuable adjunct generalist capability to specialist services in community-based palliative and end-of-life care provision. This study has developed a national Framework with 32 components addressing the macro-, meso- and micro-level interventions required to standardise palliative paramedicine across Australia. The findings may be highly relevant for translation into other countries with similar health systems and services. Future research ought to engage a multidisciplinary team to create an implementation strategy, addressing any perceived barriers, facilitators and challenges for applying the Framework into policy and practice.
Footnotes
Appendix 1: Delphi Round 1 Questionnaire
Acknowledgements
We would like to acknowledge the following experts who participated in the study and wish to be named: Alix Carter, Amy Gomes, Andrew Noble, Angela Vaughan, Annie Jorgensen, Barry Baulch, Ben White, Bill Lord, Brendan Shannon, Caleb Gage, Carol Treyvaud, Christine Sanderson, Claire Johnson, David Anderson, David Long, David Reid, Duncan McConnell, Erika Fisher, Esther McMillan-Drendel, Evelien Spelter, Felicity Burns, Frances Logan, Fraser Watson, Georgina Taylor, Harpreet Kalsi, Janelle White, Joel Rhee, Kate Swetenham, Kathryn Hooper, Lachlan Parker, Louis Christie, Louise Reynolds, Mark Molloy, Melanie Benson, Melanie Lovell, Mike McDermott, Minna Peake, Natalie Anderson, Nicola Champion, Nicola Gorwell, Nikki Pease, Norieul Kinross, Olivia Hedges, Patricia Davidson, Patsy Yates, Peter Roach, Rachel Hughes, Robin Pap, Robyn Keall, Sally Coppock, Sam Perillo, Samantha Chandler, Shannon MacFarlane, Sonja Maria, Stephen Ginsborg, Sue Berry, Tamara Hollman, Tania Blackmore, Tom Bennetts, Tom Evens and Tony Hucker.
Author contributions
The search strategy and Round 1 questionnaire were developed by MJ, JC, PB, PS and MB. The Delphi rounds were coordinated by MJ. All authors contributed to the data analysis and development of Round 2 questionnaire. MJ drafted the manuscript. All authors critically revised the manuscript, making substantial contributions and approving the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MJ received PhD funding from The HammondCare Foundation.
Ethics approval
Ethics approval was sought from the University of Sydney Human Ethics Committee (registration number 2022/914). This study was conducted in accordance with the relevant guidelines and regulations. All participants gave their written informed consent to participate.