
Abstract
Background:
Paramedic practice is diversifying to accommodate evolving global health trends, including community paramedicine models and growing expertise in palliative and end-of-life care. However, despite palliative care specific clinical practice guidelines and existing training, paramedics still lack the skills, confidence and clinical support to provide this type of care.
Aim:
To elicit paramedics’, palliative care doctors and nurses’, general practitioners’, residential aged care nurses’ and bereaved families and carers’ experiences, perspectives, and attitudes on the role, barriers and enablers of paramedics delivering palliative and end-of-life care in community-based settings.
Design:
A qualitative study employing reflexive thematic analysis of data collected from semi-structured online interviews was utilised.
Setting/participants:
A purposive sample of 50 stakeholders from all Australian jurisdictions participated.
Results:
Five themes were identified: positioning the paramedic (a dichotomy between the life saver and community responder); creating an identity (the trusted clinician in a crisis), fear and threat (feeling afraid of caring for the dying), permission to care (seeking consent to take a palliative approach) and the harsh reality (navigating the role in a limiting and siloed environment).
Conclusion:
Paramedics were perceived to have a revered public identity, shaped by their ability to fix a crisis. However, paramedics and other health professionals also expressed fear and vulnerability when taking a palliative approach to care. Paramedics may require consent to move beyond a culture of curative care, yet all participant groups recognised their important adjunct role to support community-based palliative care.
Keywords
Since its inception, paramedic practice has diversified beyond emergency care to include community paramedicine models and growing expertise in palliative and end-of-life care.
The traditionalist orthodoxy of treatment and compulsory transfer to hospital is now being questioned.
Palliative care clinical practice guidelines and training to support paramedics in this aspect of care have been developed in some jurisdictions.
Paramedics have a revered public identity, shaped by a perceived ability to fix a crisis. However, a dichotomy exists regarding their role as a lifesaver and community responder.
While mostly supportive of palliative paramedicine, paramedics express vulnerabilities when taking this approach to care and need support to move beyond conventional models of curative care.
Participants described inconsistencies in ambulance services’ governance, training, and interdisciplinary approaches. Anecdotes of greater specialisation pathways and growing unity between ambulance and palliative care services were also articulated.
Balancing competing priorities of what might be the appropriate goals of care for a person who appears to be dying, and the family’s expectations, requires a high degree of clinical skill and discretion amongst paramedics, perhaps facilitated in the future by universal paramedic access to electronic medical records.
Ambulance services ought to review current palliative care guidelines, training and interdisciplinary practice to optimise their role in this context.
Future research could investigate strategies for overcoming prohibitive paramedicine cultural norms related to palliative and end-of-life care, potentially enabling a smoother transition for paramedics to provide high quality care for people with life-limiting illnesses, reduce avoidable hospital admissions and facilitate more home-based deaths.
Background
Since their inception, ambulance services have been responding to acute emergencies and unexpected deaths in communities worldwide. 1 However, global health trends are shifting as we live longer, with greater levels of chronic disease, and increasing preferences to live and die at home.2,3 As a result, paramedic practice is diversifying to include community paramedicine models,4 –7and growing expertise in palliative and end-of-life care.8 –10
Yet, as paramedics respond to increasing numbers of palliative and end-of-life care patients in the community, the traditionalist orthodoxy of treatment and compulsory transfer to hospital is being questioned9,10,11 Palliative paramedicine clinical practice guidelines 12 and training programmes 4 are emerging, alongside interdisciplinary palliative care teams that include paramedics, 13 to broaden scopes of practice and facilitate more home-based deaths. However, paramedics reportedly still lack the skills, confidence and clinical support to provide palliative and end-of-life care in the community.8,14 –16
Previous studies have qualitatively explored the importance, feasibility and challenges of palliative paramedicine in one country 14 ; bereaved family members’ experiences of ambulance care at end-of-life17,18; the alignment of paramedics’ identity with providing palliative care at home 19 ; and the educational needs of paramedics providing this type of care. 20 However, a gap remains in understanding multidisciplinary stakeholders’ perspectives of the current impediments and facilitators of palliative paramedicine practice; the findings of which could have resonance for ambulance and palliative care services worldwide. Thus, the aims of this study are to elicit paramedics’, palliative care doctors and nurses’, general practitioners’, residential aged care nurses’ and bereaved families and carers’ experiences, perspectives, and attitudes on the role, barriers and enablers of paramedics delivering palliative and end-of-life care in home-based settings.
Methods
Design
This paper draws on data from a larger study exploring the experiences of palliative paramedicine in Australian communities, from the perspectives of both health professionals and bereaved family members and carers. A qualitative study design was underpinned by a social constructivist epistemology, 21 contending that experiences and perspectives are socially constructed by participants as they engage with the world, rather than reflections of objective truth. This study is reported following the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 22
Setting
Each Australian State and Territory has a respective ambulance service providing emergency care 24 h a day, 7 days a week across a range of metropolitan, regional, rural and remote locations. Every ambulance service maintains an emergency call-taker centre, where emergency calls are received and, based on the information received, an ambulance is dispatched into the community. In line with other Anglo-American ambulance services, Australian ambulances are usually crewed by two registered paramedics with university-level qualifications and autonomous clinical decision-making capacity. 1 However, the scope of palliative paramedicine practice remains heterogenous across the country: only five of eight Australian ambulance services have palliative care specific clinical practice guidelines to standardise practice, and many jurisdictions rely solely on specialist roles, such as Extended Care Paramedics (ECPs), to deliver palliative and end-of-life care in the community. 12
Population
Health professionals and bereaved family members and carers were eligible to participate in this study if they were aged 18 years or older and were involved in the care of someone – during any period of their life and/or career – with palliative care needs who encountered paramedics towards the end of their lives in the community. Health professional sub-groups included paramedics, general practitioners (GPs), palliative care nurses, palliative care doctors and residential aged care home managers.
Sampling/recruitment
Participants were purposively sampled to ensure a range of demographics and clinical experience were represented. Health professional participants were recruited through professional organisations, and family and carer participants were recruited through a national organisation’s register of palliative care consumers and carers. An advertisement about the research was published in each respective online newsletter and an email was sent to each organisation’s members outlining the study and inviting them to contact the research team if they were interested in participating. An invitation was also circulated through collegial networks and sent to opinion leaders with publicly available email addresses, outlining the study, inclusion criteria and contact details of the research team. Once an interested person contacted the research team, they had the opportunity to talk to a researcher to ask questions before their participation was confirmed. The study was approved by the University of Sydney Human Research Ethics Committee (2021/607; 2021/608).
Data collection
Virtual semi-structured interviews were conducted via Zoom between November 2021 and April 2022. Development of separate interview guides for health professional participants and family/carer participants was informed by discussions with the study-created Australasian Palliative Paramedicine Advisory Group (a multidisciplinary community of practice comprised of jurisdictional palliative care and paramedicine representatives), a comparative policy study of Australian and Anglo-American palliative paramedicine guidelines, 12 and a systematic integrative review on the topic. 8 Interview guides were then pilot tested amongst the research team. See Supplemental Appendices 1 and 2 for finalised interview guides.
Two female health researchers (MJ and CP) unknown to participants independently conducted the interviews online. Both researchers had completed training and were experienced in qualitative research methods. Participants were informed the purpose of the interviews was to further research into improving palliative paramedicine in community-based settings. Participant recruitment ceased when no new themes became apparent within each sub-group across three consecutive interviews. With participant consent, interviews were audio-recorded and transcribed verbatim by an external company, Pacific Transcription Inc. The researchers also took field notes for reflection during data collection.
Data analysis
Drawing on Braun and Clarke’s six-phase guide in reflexive thematic analysis, 23 an inductive approach was employed, coupled with the researchers’ existing knowledge, to progressively refine themes based on codes identified in the data. Acknowledging the research team’s personally held beliefs influencing the interpretive analysis of the data, all members approached the topic with a positive perspective of the role paramedics can play in providing palliative and end-of-life care in communities. However, we remained mindful of this and invited all participant perspectives to be captured, reporting both negative and positive cases.
MJ read all the transcripts and familiarised herself with the content, then independently identified potential codes and met with CP, JC and PB to discuss and develop the codebook, allowing for consistent interpretation and classification of the data. This codebook was then used to guide coding of the remaining transcripts by MJ. Consecutive rounds of discussions were held with MJ, JC, PB, CP, MB and PS to capture multidisciplinary perspectives and enhance the analytical framework. NVivo was used to store, organise and support analysis of the anonymised data. 24
Results
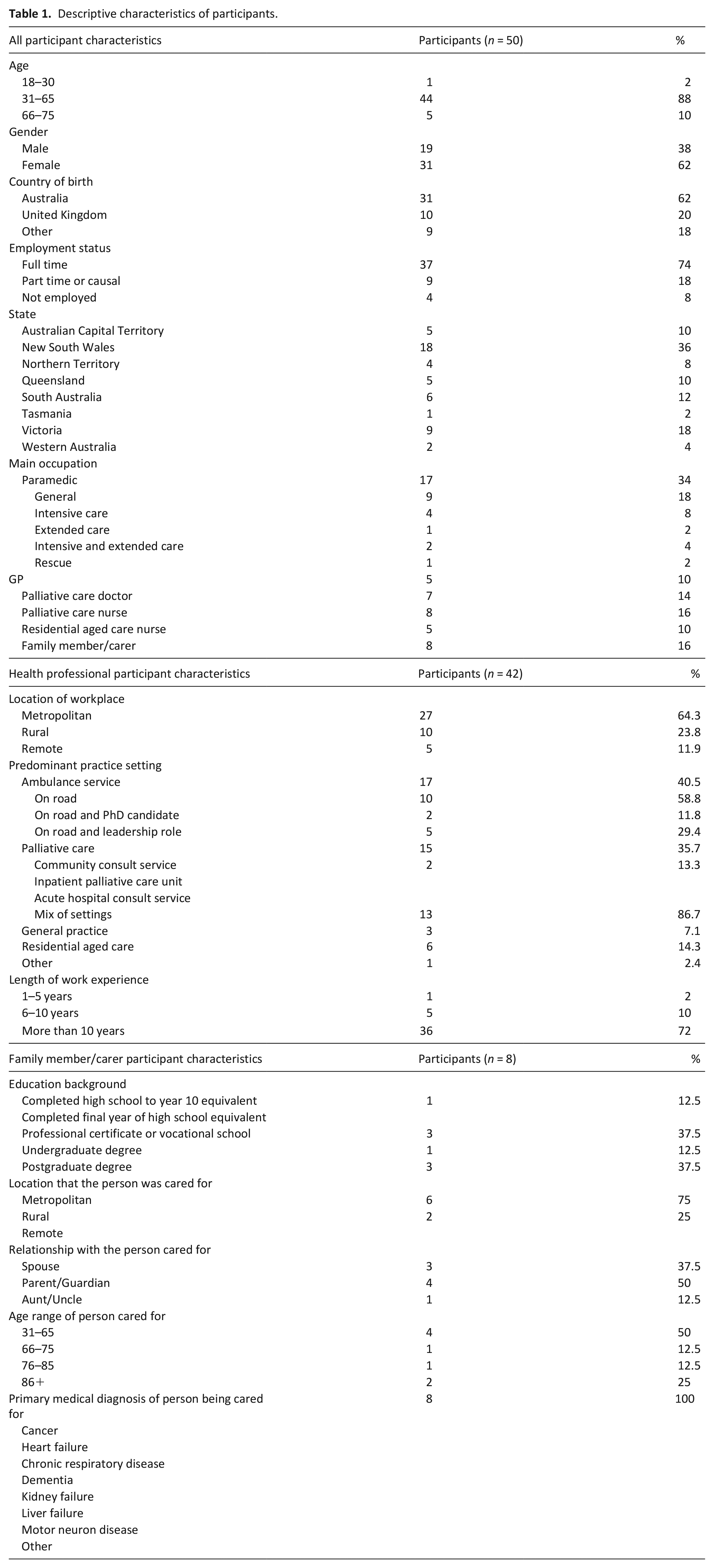
We sought to capture the experiences, perspectives and views of various stakeholders with comprehensive detail to be confident we were representing the differing participant sub-groups. As a result, a total of 50 individual interviews were conducted between November 2021 and April 2022, including 17 paramedics, five GPs, seven palliative care doctors, eight palliative care nurses, five residential aged care nurses and eight bereaved family members and carers deriving from all states and territories of Australia. Participant characteristics are outlines in Table 1. The interviews ranged in duration between 18 and 64 min (mean 43.64 min). We identified five themes: positioning the paramedic (life savers vs community responders), creating an identity, fear and threat, permission to care and the harsh reality. A thematic diagram of the themes and sub-themes is illustrated in Figure 1. Below, themes are illustrated by quotes, identified by role and ID number.
Descriptive characteristics of participants.
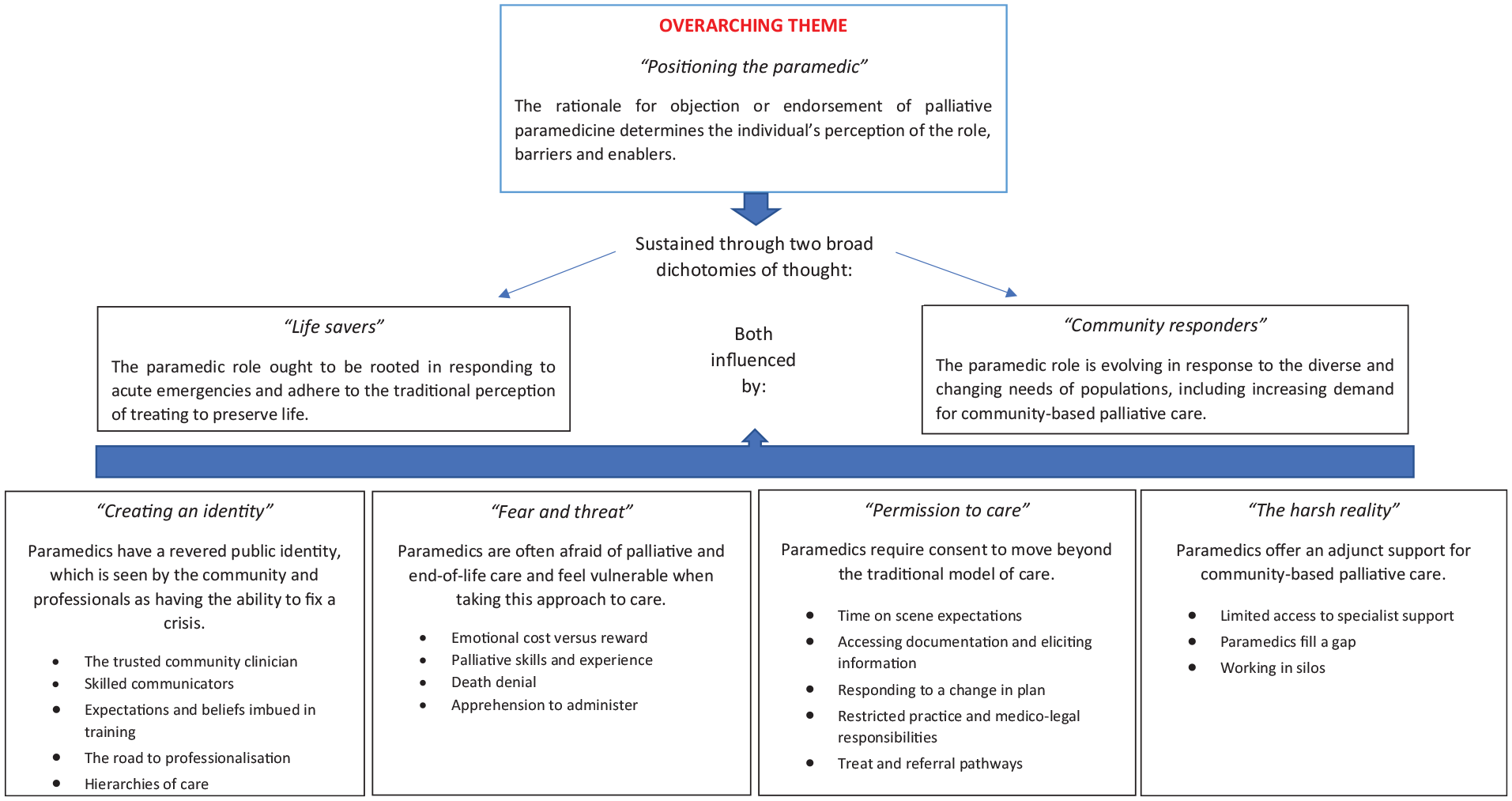
Thematic summary.
The participants reported differing rationales for objecting to or endorsing palliative paramedicine within Australian communities, ultimately determining their perception of the role, barriers and enablers paramedics and other stakeholders face. These rationales fell into a dichotomy: lifesavers versus community responders.
Life savers
Participants from a range of groups considered the paramedic role ought to be rooted in responding to acute emergencies and adhere to the traditional perception of ‘ambulance services really being there to save lives’ (Family member ID44). One paramedic asserted, ‘our major role is to transport a patient’ (ID2). Another clinician affirmed paramedics’ scope of practice should remain curative, ‘not palliative care focussed’ (residential aged care nurse, ID39). Family members also expressed hesitancy in calling an ambulance unless their family member wanted every active intervention possible to keep them alive. Participants suggested these were long-held perspectives about paramedics:
“Since I was a kid, an ambulance was always that thing where you’re saving someone from a heart attack or you’re saving people. . . you’re saving a life.” (Palliative care doctor, ID29)
Community responders
Conversely, other participants described the role of a paramedic as evolving in response to the diverse and changing needs of populations, including an increasing demand for community-based palliative and end-of-life care. Participants noted the importance of placing the patient firmly at the centre of care, with all health professionals, including paramedics, having an obligation to provide good end of life care when the need arises. They also noted that generalists, as well as specialists, can and should deliver that care:
“The whole notion of palliative care is not just about specialist palliative care, and I’m a specialist palliative care provider. I think there’s a whole host of services that provide palliative care, and paramedics and ambulance services are certainly one of them. It doesn’t mean that patients not known to a specialist palliative care service aren’t provided with palliative care. It’s about the patient at the centre and their care needs. Members of the health care services, which includes paramedics, have an obligation I think to provide good end of life care.” (Palliative care doctor, ID25)
Participants suggested paramedics have a revered public identity, which is seen by the community and professionals as having the ability to fix a crisis:
The trusted community clinician
Family members and carers expressed significant trust towards paramedics, often calling upon them in times of a palliative care emergency. All groups noted that this trust results in paramedics often being the health professionals called upon to identify and explain end of life situations and support family and carers in taking an end-of-life approach, an often highly appreciated contribution:
“They certainly had a role in making my husband comfortable in his last stages of life and they had a role in how I felt towards it. They assured me everything was ok, explained what was happening and I felt completely not in any fear. I just felt calm.” (Family member, ID48)
“I wish we didn’t need to have this support from paramedics. We should have it under control, but sometimes we need a little bit of support because the families, and sometimes the residents,. . .sadly, sometimes the respect and acceptance is not as high as when they see someone in a different uniform coming and saying there is not much we can do for you.” (Residential aged care nurse, ID39)
Conversely, participants noted this trustful identity sometimes promoted unrealistic expectations that a life could be saved, when indeed the patient was nearing the terminal phase, making it more difficult for paramedics to provide end-of-life care:
“I think they’re pushed by families and carers to act, and they come from a place of acting.” (Palliative care doctor, ID25)
Skilled communicators
Paramedics noted that their existing skills and experience in difficult communication tasks in the acute care setting, such as breaking the news that a patient had died, can readily be transferred to the palliative setting. Other clinicians also recognised the ‘advanced communication skills’ paramedics already possess, which can be ‘transferred over for when a patient is actually dying’ (palliative care nurse, ID33), as evidence of their suitability for providing end-of-life care.
However, some paramedics acknowledged that communication can be more difficult for expected deaths, where family and carers may be exhausted after a prolonged period of providing care: “But being comfortable around an inevitable death and how you talk about that again is very different. I think potentially that just weighs a little harder. I think it’s a much rawer or fatigued form of grief, rather than a purely emotional outburst that we see when we go to more acute cases, or people who have died by trauma or unexpectedly. It’s very hard to articulate, but it looks, sounds and feels different. . .” (Paramedic, ID8)
Participants also acknowledged that the traditional emergency response mentality instilled in junior paramedics did not match well with the more relationship-based, continuity of care approach required in palliative care:
“It’s so ingrained in paramedics. Walk in, identify that sick patient, okay, primary survey, can someone get some monitoring on, taking over that scene control in quite often a non-emotive state. It’s an efficient state and when you apply that onto a palliative care patient it’s quite abrupt.” (Paramedic, ID13)
Expectations and beliefs imbued in training
Participants described an entrenched ‘culture of curative care’ (paramedic, ID10) that is fostered amongst all clinical disciplines. However, paramedics noted this focus and capability is particularly emphasised in their ongoing education and maintained throughout the trajectory of their careers:
“We’re taught about what to do in a cardiac arrest. We’re taught what to do when someone’s deceased, but we’re never actually taught the in-between.” (Paramedic, ID4)
Others suggested paramedicine attracts a certain type of individual who seeks, is skilled in, and thrives in emergency situations. Such individuals may struggle more with the holistic aspects of palliative care: “The people who go into paramedics tend to be very decisive, problem-solving, adrenaline-seeking individuals, who are not fazed being put under extreme stress. They’ve got to think quickly, act quickly, and the idea of stepping back and thinking more reflectively and potentially coming to a decision that you don’t do anything active is often difficult for some people.” (GP, ID19)
Participants suggested paramedics will need training to fill in gaps in their current education and provide the specific skills required in palliative care: “Paramedics should be trained to assess all palliative patients, provide emergency symptom control, make assessments around goals of care and also consider the requirement to come to hospital” (Palliative care doctor, ID26).
“We’re literally there when people expire, and we don’t necessarily have great tools unless you’ve been involved in an Extended Care Paramedic program, or something like that. . . That it’s not part of general ambulance practice to give a sub-cut injection, for example, or to put a sub-cut line in, is worrying. It’s a mechanical skill, but it’s not something that we do generically.” (Paramedic, ID13)
The road to professionalisation
Participants highlighted traditional perceptions of paramedics as ambulance drivers had historically limited expanded conceptualisations of this role. Paramedics cited interprofessional reluctance, a lack of rigorous evidence of the feasibility and efficacy of paramedic involvement in palliative care, and limited drivers to initiate change, as hindering the movement beyond an ambulance-based model of care:
“I think there are some barriers to paramedics working outside of ambulance services. The health services need to be open for paramedics to work within it and see the value that paramedics provide. . . . I don’t think we’ve had any significant change agents yet that have really proven that paramedics have capacity to work outside of an ambulance service.” (Paramedic, ID12)
However, palliative care specialists acknowledged the recent introduction of professional registration for paramedics and subsequent broadening of clinical roles were slowly challenging this stereotype:
“I do think legislatively things changed. But it’s taken a long time for the systems to sort of catch up. But I think they’ve got an increasingly expanding role, and the thrust of working beyond an ambulance response is new and exciting. It’s really going through that transitions that nurse practitioners went through about 10 to 12 years ago. So, they’re just beginning that journey.” (Palliative care doctor, 26)
Hierarchies of care
Participants described professional and gender hierarchies within clinical disciplines, which sometimes hinder interprofessional collaboration. They noted the male-dominated paramedic profession might under-value the quieter, more considered approach required for palliative care, while other professions may be concerned about losing their palliative care patients if shared care with paramedics became the accepted model:
“I felt like the male paramedic dominated the women in the space and disregarded the expertise of the palliative care nurses. I felt like they had the clinical expertise in that situation, but it wasn’t acknowledged.” (Family member, ID47)
“I think not many GPs would be willing to share all their records about the patient with other health professionals because they could become a little bit defensive about that.” (GP, ID20)
However, aged care nurses described mostly positive multidisciplinary engagements within ambulance staff:
“Paramedics are quite responsive and willing to partner. I see them speak with our nurses and they share the information. . ., it’s always a collaboration.” (Residential aged care nurse, ID39)
Participants suggested health professionals are often afraid of palliative and end-of-life care and feel vulnerable when taking this approach to care.
Emotional cost versus reward
Paramedics described palliative and end-of-life care as emotionally draining, and questioned whether they therefore tended to avoid such an approach:
“I wonder if maybe it’s because paramedics don’t want to get too touchy feely because that’s where the risk is for us to become emotionally attached to the job.” (Paramedic, ID17)
Yet, they recounted fulfilment when a good death was facilitated:
“It’s a tough job but it’s one of the most rewarding. To me it’s a privilege being there at the end of someone’s life, and I get great satisfaction from helping a family go through that moment and just supporting them and making it a nice death. Because so many people don’t get that option. So, if I can be there to make things a little bit easier then to me that’s an honour to be there.” (Paramedic, ID1)
Palliative skills and experience
Participants highlighted the heterogeneity of paramedics’ skills and expertise, and that a clinician’s previous experience and exposure to end-of-life determines their propensity to fear palliative approaches to care:
“You’re really relying on individual (paramedics) rather than on a process.” (Palliative care nurse, ID30)
“If they’ve been around for a while, they know what a dying person looks like and when dying is not going to be reversible. After you’ve been in the job for a while, you’ll see where the line between potential success and inevitable failure is.” (GP, ID18)
Thus, with age and experience, a palliative care approach may become more acceptable and easier to deliver for paramedics. Yet, participants suggested some older paramedics may be more likely to reluctant change, subscribing to the traditional role and resisting shared decision making:
“They want to be black and white, . . . and they’re just like, if this person needs to be transferred to hospital, let’s transfer this person to hospital.” (Residential aged care nurse, ID41)
Death denial
Participants described a broader society lacking adequate knowledge, skills and awareness to compassionately respond to death:
“We’ve outsourced death and dying. We don’t do it anymore. We don’t support people. We put old people in nursing homes, so we don’t see it, unless you’re in a situation where it’s happening to someone you care about, and then often I think it’s not done very well, because people don’t know what to do.” (Family member, ID50)
Some suggested that death denial amongst families can prevent planning, communication and acceptance; all of which facilitate paramedics to take a palliative approach:
“When someone’s dying, the family may not be accepting of that. It might be cultural. It might be the care home has provided really poor care and they’re blaming them and don’t want their loved one in that care home anymore. They’re missing the fact that their loved one is actually deteriorating and dying.” (Palliative care nurse, ID30)
Participants reported clinicians may also experience death anxiety, which can hinder communication.
They noted, clinicians ‘aided and abetted the dysfunction in refusing to talk about the nature of the condition’ (family member, ID45). One palliative care nurse suggested, ‘sometimes it’s because clinicians don’t feel comfortable having those conversations’ (ID35), while a GP asserted, ‘one of the reasons GPs don’t do death well is our own fear of death’ (ID21).
Apprehension to administer
Paramedics, GPs and aged care nurses expressed fear in administering palliative medications that they may inadvertently cause, and be held responsible for, death. Family members expressed similar apprehension when the responsibility fell on them:
Participants suggested paramedics require consent to move beyond traditional models of curative care.
Time on scene expectations
Participants commonly expressed a belief that paramedics worked under a very time-pressured environment, which conflicted with the potentially long time it takes to manage a palliative care patient. Some paramedics referenced ambulance services setting key performance indicators which restricted them to a maximum 20 minutes on scene. Numerous participants endorsed the sentiment of this policy:
“When someone’s dying or approaching death, in my experiences when paramedics are called, they can’t spend hours with someone, unless it’s trying to keep them alive or stabilise them. They’re called for emergencies. Their role is an emergency role.” (Family member, ID50)
However, other participants supported ‘discretion for staying on scene’ in palliative care situations (Paramedic, 10). Specialist roles were discussed by participants as a solution to avoiding taking an operational ambulance out of the system:
“I think there’s always a role for Extended Care Paramedics in palliative care as well. Because I think we’ve got a bit more specialist training, we run around as singles; we don’t have a stretcher resource, we’re not tying up an emergency ambulance.” (Paramedic, ID6)
Accessing documentation and eliciting information
All participants emphasised the importance of paramedics being able to access information in a timely manner to make sound clinical decisions. Palliative care doctors recounted experiences where paramedics have called them in otherwise avoidable circumstances because they did not have sufficient information to guide care. Participants universally felt paramedics ought to have greater access to Electronic Medical Records (EMR) and standardised advance care planning documentation, given that they are a recognised part of the health system.
“{They phoned me because] things have not been clearly documented and a decision hasn’t been made whether the patient is to return to hospital or not” (ID24), [because the ambulance service] “can’t access EMR” (Palliative care doctor, ID27).
Some clinicians suggested eliciting information about advance care planning from families and carers could sometimes be difficult as they were too stressed to remember its relevance or location:
“Forget about documentation during times of crisis because they’re worried, they may not recognise this could be the end” (GP, ID19).
However, family members and carers recalled more positive experiences:
“They suggested that he had blood poisoning. . .. They then said, well we’re going to now intubate him and keep him alive, and I said, well he’s got a certificate here from the doctor to say that he doesn’t want to be kept alive. . .. So, I had to go and get that form which they read through very, very thoroughly. . . and then they said, yep, we completely understand, put it aside and then just explained to me how to make him comfortable.” (Family member, ID48)
Responding to a change in plan
Although patients and their families may prefer and plan for a home-based death, participants suggested paramedics facilitate the transport of a palliative patient to hospital if this option is no longer feasible due to uncontrolled symptoms or family exhaustion. Family members sometimes expressed feelings of guilt associated with changing the plan:
“People need permission to know that it’s okay, that they haven’t failed anyone if they can’t be at home, or they need to go to hospital.” (Family member, ID46)
However, others noted the reassurance of knowing that transport to hospital was an option facilitated their decision to change the plan:
“Even though his intention was to pass away at home, it just became too much for us to handle. The nurses. . . said ‘look, all it takes is a phone call and the ambulance patient transport will come, and we’ll take him over to the hospital.’.” (Family member, ID46)
Some paramedics also voiced apprehension in responding to a change of plan, but recognised the need to take family-centred approaches to palliative care:
“You’ve tried to advocate for what the patient’s wishes were, to die at home. . . But then the family members sometimes are screaming at you to take them back to the hospital, because they don’t want them to die there. There are significant emotional challenges associated with dealing with the family. . . But you’ve got to remember that the family are also your patients in palliative medicine as well.” (Paramedic, ID15)
Restricted practice and medico-legal responsibilities
Participants reported ambulance services have inflexible policies and procedures, which often limit their scope of practice to treat a palliative patient. The recent registration of paramedicine has added further legal complexities to palliative care, making services even more fearful of being seen to do the wrong thing:
“Having rigid protocols really becomes an impediment for, I believe, paramedics to enact patient-based care that’s based on the particular situation. Instead, they’re following more of an algorithm associated with that”. (Paramedic, ID12)
“Even if I truly believe I’m acting in the best interests of the patient. . . we’re really fearful here of - and probably as an ambulance service thing in general - getting a complaint and then not being supported by the service.” (Paramedic, ID7)
Treat and referral pathways
Palliative care specialists noted a shift towards paramedics wanting to keep people at home, which has led to ambulance services ‘connecting with the palliative care services in a more structured way’ (Palliative care doctor, ID24). Participants described the benefits of engaging multidisciplinary teams for clinical back-up and support, which allowed paramedics to initiate palliative approaches to care where they would otherwise be uncertain:
“When I go to a patient with unidentified palliative care needs, because I have the number for the palliative care service, I’ve got the confidence to talk to them, I’m then happy to consult the patient almost as a referral.” (Paramedic, ID10)
Despite the preferences of some participants to maintain a paramedic focus on emergency care, all participants recognised paramedics should offer an adjunct support for community-based palliative care because often they are the only health professional available.
Limited access to specialist support
All groups reported specialist palliative care services were not always available, especially out-of-hours, due to funding constraints:
“After-hours specialist support was inconsistent at best, and it was non-existent at worst.” (Family member, ID46)
Paramedics fill a gap
Participants highlighted the significant support paramedics offer when specialist palliative care services were unavailable, particularly in rural areas:
“We were called because of his deterioration and the family weren’t sure what to do. They’d called the palliative care team, but they were an hour or two away, so we were called as a bridging service, I guess.” (Paramedic, ID14)
“In regional and remote areas, it’s the ambulance that gets called because that’s all there is.” (Palliative care doctor, ID23)
GPs also acknowledged their increasingly practice-based model of care requires ambulance services to be available for home visits in an emergency, to help fill the community in-reach gap:
“There are lots of GPs who don’t have scope or interest in doing home visits anymore, and there are very few nursing services where medication can be initiated without involvement of a medical officer. . . The effective use of paramedic protocols in end-of-life care goes some way to filling that gap.” (GP, ID18)
Working in silos
Participants reported accessing multidisciplinary services was often disjointed and inconsistent, relying on the knowledge and networks of individual clinicians rather than a streamlined approach. Accordingly, ambulance services and GPs often worked alone, lacking integrated approaches with other services:
“Paramedics are predominantly employed and work within a centralised service for a state. But then they have to operate within all these individual health services, who aren’t always all on the same page.” (Paramedic, ID15)
“We work in silos. We don’t communicate well.” (GP, ID22)
However, specialist palliative care providers expressed a desire to collaborate more in ‘shared care models’ (Palliative care doctor, ID23) with ambulance services and other healthcare providers in the future.
Discussion
Main findings/results
The broad range of perspectives and experiences captured in this study reflect a diversity of cultures within, and across, healthcare disciplines and communities. A dichotomy of thought was expressed amongst the participants. Some participants in our study described inconsistencies in ambulance services’ governance, training, and interdisciplinary approaches. Conversely, anecdotes of greater specialisation pathways and growing unity between ambulance and palliative care services were also articulated.
What this study adds
The main findings of our study align with broader literature, which suggest although paramedics are increasingly attending palliative and end-of-life care patients in the community, a divergence of opinion exists within the discipline regarding their capacity to provide this type of care at the expense of other emergencies. Some argue palliative paramedicine is not for everyone, but rather for those paramedic ‘champions’ who have a passion for palliative care.25,26 We agree with this sentiment, but also call for a generalist palliative care capacity for all paramedics, and specialist roles for those demonstrating interest and aptitude.
In 2018, paramedics entered the National Registration and Accreditation Scheme for Health Practitioners in Australia. 27 One study described the experience as a transition from a discipline with a disparate framework of employer-based regulation and governance, to a nationally regulated profession with self-determination over standards and practice. 28 This significant step towards paramedicine professionalisation in Australia has aligned with an increasing scope of autonomy, roles and practice relevant to the provision of community-based care internationally.10,16,28 Registration has precipitated similar changes within the United Kingdom’s paramedic workforce a decade earlier, 29 resulting in the emergence of paramedic practitioner roles, including those specialising in palliative care.30,31 However, the Canadian paramedic workforce – a pioneering leader in community and palliative paramedicine4,32 – remains registered provincially, rather than nationally, and trains clinicians through vocational pathways in preference to university degree programmes. 33 This raises the pertinent question: does paramedicine professionalisation drive the emerging scope of palliative and end-of-life care, or do community needs and ambulance service innovation have a greater influence? We believe both factors have an impact; the latter being most critical.
Some participants expressed strong-held beliefs of restricted time on scene and the necessity to treat and transport all patients to hospital, which are seemingly driven by individual perceptions, creating a culture of paramedicine at odds with what is reflected in clinical practice guidelines and accordingly permitted by ambulance service management. 12 Furthermore, community expectations and media responses to ambulance waiting times could be proliferating these assumptions. Future research could investigate strategies for overcoming such cultural norms, potentially enabling a smoother transition for paramedics to reduce avoidable hospital admissions and facilitate more home-based deaths.
Multidisciplinary approaches to palliative care were praised by participants and supported by literature.34,35 The Australian and New Zealand Society of Palliative Medicine has previously called for a greater focus on expanding the practice of specialist palliative care teams to better support primary palliative care providers through consultative or consortium arrangements. 36 Despite these assertions, paramedicine is still lacking from palliative care policies,16,37 and remains an under recognised palliative care asset within international frameworks. 38 Moreover, paramedicine has traditionally prided itself as a discipline of independence and autonomy, perhaps reinforcing hierarchies and siloes of care, and hindering opportunities for establishing communities of palliative care practice.19,39
However, the COVID-19 pandemic has expediated the settings in which paramedics can work, highlighting opportunities for these skilled clinicians to join multidisciplinary teams in general practice and palliative care settings.1,40 This approach has resulted in congenial relationships across disciplines, foreshadowing opportunities for future integrated models of community-based palliative care. One study highlighted collaborative relationships with paramedics require professional acknowledgement, respect and reciprocity to strengthen their willingness to share knowledge and skills. 41 To foster sustainable networks of interdisciplinary learning and care across paramedicine, palliative care and community-based health services, a contextual awareness and understanding of operational culture, barriers and enablers will be required.
Finally, advance care planning processes can help mitigate unwanted interventions and crisis-fuelled decision making for palliative care emergencies.15,42 However, timely access to legible advance care planning documentation remains a key challenge for paramedics globally.11,43 –45 The previous use of paper-based standardised palliative care documentation for paramedics offered a solution for one Australian jurisdiction, while rendering significant challenges along the way. 46 Participants of our study also raised the importance for families to be able to ‘change the plan’ in cases of carer burnout and distress. Balancing these competing priorities in the future will require a high degree of clinical skill and discretion amongst paramedics, perhaps facilitated by universal paramedic access to electronic medical records.
Strengths and limitations of the study
This study explored participant perspectives of paramedic practice in Australia, which follows an Anglo-American ambulance system. However, we believe the findings of this study are relevant to ambulance services in many countries given the important role that paramedics may have in providing palliative and end-of-life care in home-based settings. A key strength of this study was the sizeable and varied sample of participants, coming from six important stakeholder groups and all jurisdictions of Australia, allowing for in-depth analysis and transferability of the data. Self-selection and recall bias are potential limitations of this study. Opportunities also exist to investigate the lived experience of patients with palliative care needs in the future.
Conclusion
Palliative paramedicine is an emerging scope of practice within ambulance services internationally, but findings from this study align with literature from different countries which, suggests a dichotomy of thought exists regarding what the role of a paramedic ought to be. They have a revered public identity, shaped by a perceived ability to fix a crisis. However, paramedics and other health professionals sometimes express fear and vulnerability when taking a palliative approach to care. They require consent to move beyond a culture of curative care and will offer an adjunct support for community-based palliative care. Future research could investigate strategies for overcoming prohibitive paramedicine cultural norms related to palliative and end-of-life care, and explore the practical steps required to overcome barriers and introduce facilitators addressed in future research to improve paramedic interdisciplinary practice with palliative and primary care services.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163231186451 – Supplemental material for ‘It breaks a narrative of paramedics, that we’re lifesavers’: A qualitative study of health professionals’, bereaved family members’ and carers’ perceptions and experiences of palliative paramedicine
Supplemental material, sj-docx-1-pmj-10.1177_02692163231186451 for ‘It breaks a narrative of paramedics, that we’re lifesavers’: A qualitative study of health professionals’, bereaved family members’ and carers’ perceptions and experiences of palliative paramedicine by Madeleine L Juhrmann, Phyllis N Butow, Cara M Platts, Paul Simpson, Mark Boughey and Josephine M Clayton in Palliative Medicine
Footnotes
Acknowledgements
The search strategy was developed by MJ, JC, PB and CP in consultation with the Australian Palliative Paramedicine Advisory Group. The interviews were conducted by MJ and CP. MJ conducted the thematic analysis, which was cross-checked by JC, PB and CP. MJ drafted the manuscript. All authors critically revised the manuscript, making substantial contributions and approving the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for research, authorship and/or publication of this article: MJ received PhD funding from The HammondCare Foundation.
Ethics approval
Ethics approval was sought from the University of Sydney Human Ethics Committee (registration number 2021/607 and 2021/608). This study was conducted in accordance with the relevant guidelines and regulations. All participants gave their written informed consent to participate.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.