
Abstract
Background:
Severe grief is highly distressing and prevalent up to 1 year post-death among people bereaved during the first wave of COVID-19, but no study has assessed changes in grief severity beyond this timeframe.
Aim:
Understand the trajectory of grief during the pandemic by reassessing grief symptoms in our original cohort 12–18 months post-death.
Design:
Prospective matched cohort study.
Settings/participants:
Family members of decedents who died in an acute care hospital between November 1, 2019 and August 31, 2020 in Ottawa, Canada. Family members of patients who died of COVID (COVID +ve) were matched 2:1 with those who died of non-COVID illness (COVID −ve) during pandemic wave 1 or immediately prior to its onset (pre-COVID). Grief was assessed using the Inventory of Complicated Grief (ICG).
Results:
Follow-up assessment was completed by 92% (111/121) of family members in the initial cohort. Mean ICG score on the 12–18-month assessment was 19.9 (SD = 11.8), and severe grief (ICG > 25) was present in 28.8% of participants. One-third (33.3%) had either a persistently high (>25) or worsening ICG score (⩾4-point increase between assessments). Using a modified Poisson regression analysis, persistently high or worsening ICG scores were associated with endotracheal intubation in the deceased, but not cause of death (COVID +ve, COVID −ve, pre-COVID) or physical presence of the family member in the final 48 h of life.
Conclusions:
Severe grief is a substantial source of psychological morbidity in the wake of the COVID-19 pandemic, persisting more than a year post-death. Our findings highlight an acute need for effective and scalable means of addressing severe grief.
Previous research demonstrates a high prevalence of severe grief symptoms up to a year post-death of a loved one among those who experienced bereavement during the COVID-19 pandemic.
No previous study has assessed changes in the severity of grief more than a year after the death of a loved one during the COVID-19 pandemic.
This prospective cohort follow-up study found the prevalence of severe grief reaction remained high (28.8%) at 12–18 months post- family member death.
One-third (33.3%) of family members experienced persistently high or worsening grief symptoms at the time of their 12–18-month assessment compared to baseline 6–12-month assessment.
Grief severity was associated with endotracheal intubation in the deceased, but not with the cause of death (e.g., COVID vs non-COVID illness) or physical presence/absence of the family member at the bedside in the final 48 h of life.
There is a persistent, elevated risk of severe grief among family members who experience bereavement during the pandemic period, even up to 18 months post-death of the decedent.
There is an urgent need for effective and scalable means of addressing severe grief in the wake of the COVID-19 pandemic.
Introduction
The COVID-19 pandemic has impacted the bereavement process for many people who experienced the death of a family member or loved one.1–4 The pandemic resulted in widespread restrictions on travel and gatherings, which made it difficult for people to be with their family members during their final moments or to attend funerals and other rituals to mark their deaths.5,6 In addition, many experienced pronounced feelings of isolation and disconnection at a time when they most needed a sense of support and community.7,8 The pandemic also disrupted many of the usual ways that people cope with grief, such as participating in community or religious activities9,10; they were forced to interact virtually or by telephone, and find new ways to cope with their grief.11,12
Grief is a natural and normal response to the death of a loved one, but for some people, the grief process can be more intense and prolonged (e.g., >6 months), leading to a severe grief reaction characterized by intense and persistent feelings of sadness, despair, and difficulty functioning in daily life. It may also involve changes in sleep patterns or difficulty concentrating.13,14 We previously found a high prevalence of severe grief symptoms among a cohort of people who experienced bereavement during the first wave of COVID-19, regardless of the cause of death or even if the death occurred prior to the onset of the pandemic. 15 Notably, our study looked at grief symptoms more than 6 months following the death of the decedent, which is standard in grief research 16 ; other studies had measured symptoms closer to the death itself, which can lead to an overestimation of severe grief given that symptoms often decline over time. 17 However, no previous work has assessed changes in the severity of grief more than a year after the death of a loved one during the COVID-19 pandemic. To better understand the trajectory of grief symptoms among those bereaved during the pandemic, we reassessed grief symptoms in our original cohort at least 6 months following their initial assessment (12–18 months post-death of the decedent), and examined factors associated with changes in grief severity.
Methods
Design and setting
A prospective multi-center matched cohort study of family members of inpatient, acute care decedents in Ottawa (population 1.4 million), Canada. The study’s decedents were inpatients in three regional hospitals (see Appendix for details).
Population
We previously enrolled a cohort of 121 bereaved family members of people who died in an acute care hospital during or shortly before the first wave of the COVID-19 pandemic. The patient cohort and the care they received has been described previously. 15 It included 85 patients who died of COVID-19 infection between March 1 and August 31, 2020 (COVID +ve) matched 2:1 with patients who died of a cause other than COVID-19 between March 1 and August 31, 2020 (COVID −ve, n = 170) and those who died between November 1, 2019 and March 1, 2020 (pre-COVID, n = 170). The bereaved cohort in the present study (30 COVID +ve, 46 COVID −ve, and 45 pre-COVID) were the listed next-of-kin of the decedents in each of these groups who agreed to participate in our initial bereavement study.
Enrollment and data collection
Phone contact was attempted with family members who participated in our initial bereavement study; we contacted them 12 to 18 months after their family member’s death, and at least 6 months after we had contacted them for the initial study. For those who consented to participate, we administered the Inventory of Complicated Grief (ICG) over the phone. The ICG assesses emotions, behaviors, and thoughts associated with complicated grief, such as difficulty accepting the death of a loved one, intense yearning or longing for the person who died, feeling that life is empty or meaningless without the loved one, and difficulty trusting or relying on others. Participants rated the frequency of each of the 19 ICG items on a 5-point scale ranging from 0 (Never), 1 (Rarely), 2 (Sometimes), 3 (Often), and 4 (Always). We defined severe grief as a total ICG score >25, consistent with previous studies. 16
Analysis
We compared ICG scores at baseline (6–12 months) and follow-up (12–18 months) using a paired sample t-test, and compared the proportion with ICG score >25 using a Chi-square test. In a post-hoc analysis to identify factors associated with persistent or worsening severe grief [either ICG >25 on both baseline and follow-up or ICG score increasing by four or more (equal to half of one standard deviation of the change in ICG score)], we used a modified Poisson regression with robust error variance 18 to estimate relative risks of this occurring in each group within the cohort (pre-COVID, COVID +ve, COVID −ve), if the family member was physically present or absent in the last 48 h of life, or if the deceased patient had been endotracheally intubated prior to death. These latter factors are known to be associated with more severe grief. 19 Participants were only included in the analysis if data were available for both 6–12 months and 12–18 months.
Ethics
This study was approved by the Research Ethics Boards at all participating hospitals: Ottawa Health Science Network-REB (20200653-01H, December 18th 2020); Hôpital Montfort REB (20-21-10-032, December 2nd 2020); and Queensway Carleton Hospital REB (20-06, December 1st 2020). Informed consent was obtained from all participants prior to their participation, and all participants were provided with information about available bereavement supports, including a free virtual bereavement support group.
Results
Of the 121 family members in the initial bereaved cohort, 111 (92%) completed the follow-up assessment. Five family members no longer wished to participate and five could not be contacted through their provided phone numbers. Of the 111, 41 (36.9%) family members were from the pre-COVID cohort, 27 (24.8%) from the COVID +ve cohort, and 43 (38.7%) from the COVID −ve cohort. The mean age of the 111 family members was 58.2 years, and the majority were Caucasian (76.6%), female (67.7%), married (44.1%) or widowed (19.8%), and the child of a decedent (62.2%) (Table 1).
Demographics of bereaved participants and their deceased family members.
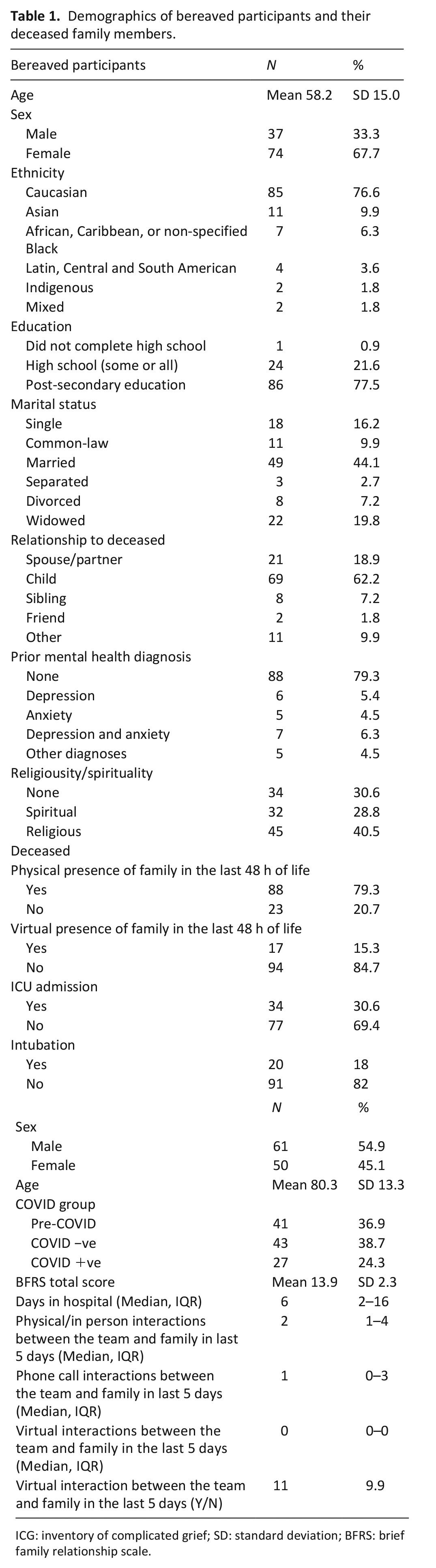
ICG: inventory of complicated grief; SD: standard deviation; BFRS: brief family relationship scale.
The mean ICG score on the 12–18-month assessment was 19.9 (SD = 11.8), which was unchanged from the 6 to 12-month assessment (19.9, SD = 10.7). This value was also not significantly different than the 6–12-month assessment for the 10 participants who were lost to follow-up (mean ICG 18.6, SD 13.3, p = 0.741). Severe grief (ICG > 25) was present in 32 family members (28.8%) at follow-up, which was also unchanged from baseline (28.8%). Twenty-two (19.8%) family members had ICG scores >25 at both baseline and follow-up, while 26 (23.4%) had a ⩾4-point increase on the ICG from baseline to follow-up. A total of 37 (33.3%) family members had either a persistently high or worsening ICG score (>25 or a ⩾4-point increase) (Table 2).
Grief scores among participants.
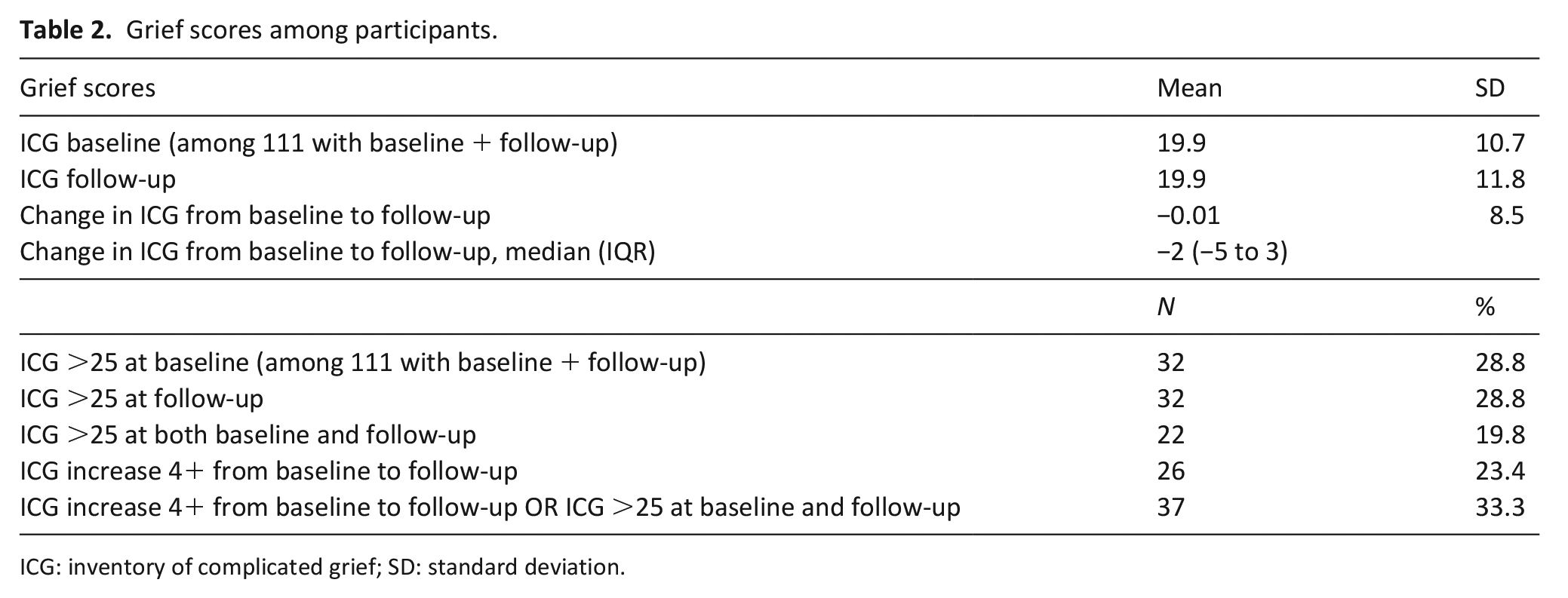
ICG: inventory of complicated grief; SD: standard deviation.
Using a modified Poisson regression analysis, we found the presence of persistently severe or worsening grief symptoms in the bereaved was not associated with the cause of death (COVID +ve, COVID −ve, or Pre-COVID) or physical presence/absence of the bereaved in the final 48 h of life (Table 3). The adjusted analysis found endotracheal intubation in the deceased was associated with an elevated risk of persistently severe or worsening grief symptoms (RR 1.71, 95% CI 1.01–2.88).
Associations of COVID status, physical presence/absence of the bereaved, and intubation on grief outcomes.
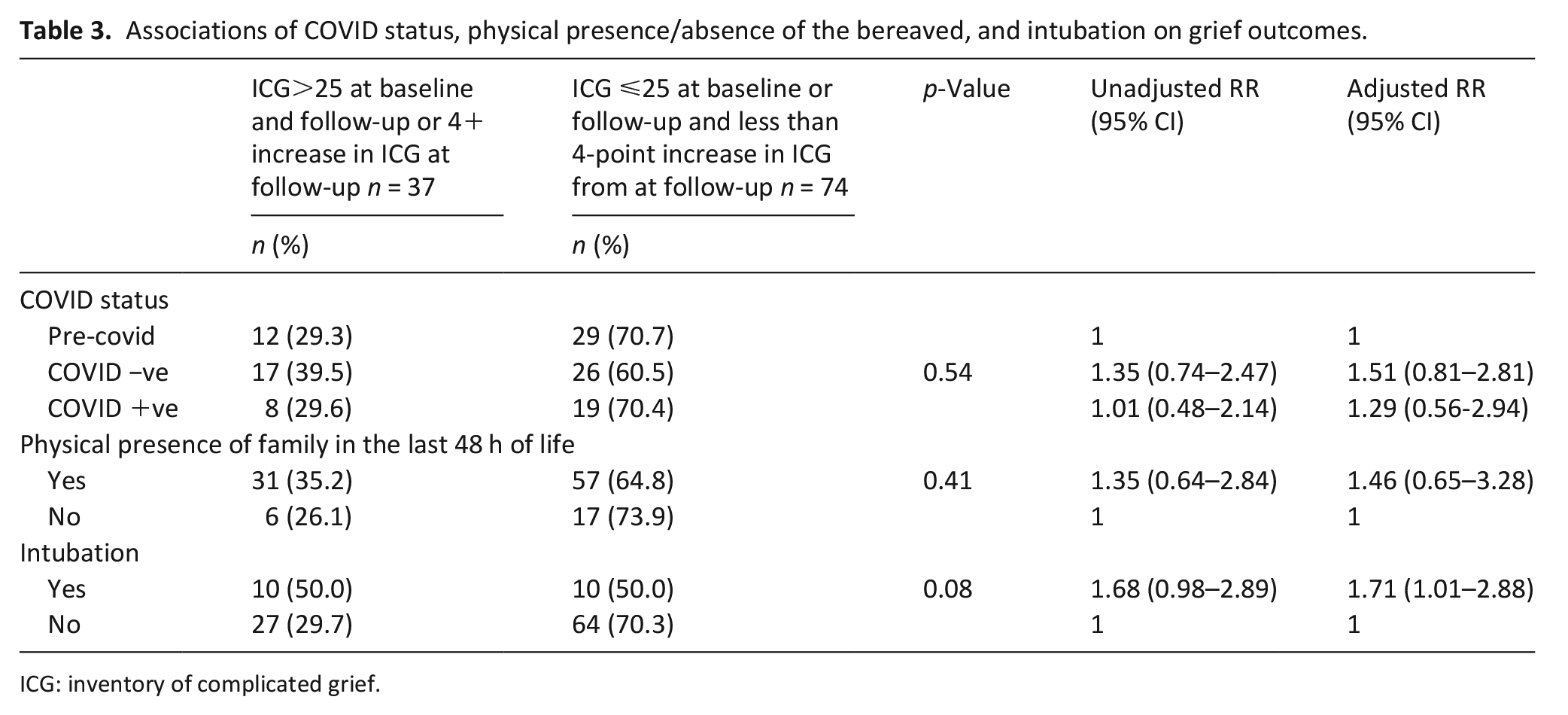
ICG: inventory of complicated grief.
Discussion
Main findings
In this study of the long-term follow-up of a cohort of family members bereaved from a death in the first wave of COVID-19, we found the prevalence of severe grief symptoms at 12–18 months post-death was high and unchanged from 6 to 12 months post-death. While some family members had grief symptoms that improved, more than a quarter of the cohort saw their symptoms worsen substantially in the time between assessments.
Interpretation
Few studies have prospectively followed cohorts of bereaved family members for up to 18 months and, to our knowledge, no published study has looked at long-term follow-up of bereavement outcomes during the COVID-19 pandemic. Health administrative data studies have shown a substantially increased risk for mental illness and cardiovascular disease in the decade following the death of a spouse, 20 and population-level comparative surveys have shown impaired mental health and social function for up to 4 years after the death of a close friend. 21 A randomized-controlled study of two different psychotherapeutic approaches found grief scores in both groups decreased approximately 25% between 6 and 24 months following the therapy. 17 Grief following mass-casualty events (such as a pandemic) may be particularly slow to resolve. One study of Norwegian parents or siblings bereaved after the Utoya Island massacre found symptoms had still not resolved for approximately 75% of participants after 40 months. 22 Another study of Swedish people bereaved following the Indian Ocean tsunami of 2004 found grief symptoms did not start to improve until 3 years later. 23
We had previously found that the severity of bereavement symptoms in this cohort was not correlated with the physical presence or absence of the bereaved in the final 48 h of life, or whether or not the deceased had been intubated at some point. 15 These factors were shown in pre-pandemic studies to be associated with the severity of grief symptoms. 19 In the present study, on an adjusted analysis, we found a significant association between persistently high or worsening grief symptoms and intubation but not physical presence or COVID-19 status. Given many family members in our cohort would not have been present at the bedside to witness intubation due to pandemic-related isolation and visiting restrictions, it is unclear from these findings whether endotracheal intubation is a marker for other factors driving changes in severe grief (e.g., patients who receive critical care and intubation may have had closer relationships with the family members who advocated for this care; these patients may also have been healthier at baseline, prompting family members to advocate for more aggressive care), or whether intubation itself, or perhaps simply the mental conception of intubation and rumination on this image, contributes to greater grief severity. We propose this may be an area for future research.
Together, our findings once again underscore that the severity of grief in the pandemic was likely influenced as much or more by experiencing the grief and bereavement process during the pandemic rather than by the timing of the death itself, specific circumstances of the decedent person, or the care they received prior to death. Given COVID-19 practices around endotracheal intubation and family visiting changed during subsequent waves of the pandemic, future studies may lead to a better understanding of the relationship between care, physical presence, and grief symptoms in the pandemic.
Strengths and limitations
Strengths of this study include the very high participation rate of the cohort, with <10% loss to follow-up from the 6 to 12-month assessment and no significant difference in ICG score between those lost to follow-up and the current cohort (although the initial cohort had a 67% participation rate). This minimizes the risk of attrition bias or other factors confounding the results. Our study was also prospectively designed to include all acute care deaths in Wave 1 of COVID-19 for an urban community of >1 million people, which minimizes the risk of selection or responder bias that would occur with convenience sampling or surveys. The latter have shown higher prevalence of severe grief symptoms.24–28 Moreover, our use of matched cohorts allows a better understanding of the role of the illness itself (i.e., COVID-19) in driving grief.
Limitations include a focus on acute care decedents, when much of the Wave 1 mortality in Canada occurred in the long-term care setting. 29 There is no universally-accepted metric for severe grief reaction, so we used the ICG score because of familiarity within our research group and to facilitate comparison to our previous work. Other studies of bereavement in the COVID-19 pandemic have used a variety of different metrics.30,31 We did not study the association of grief symptoms with the involvement of social supports or other interventions to reduce grief symptoms; no participants reported using any formal bereavement supports, despite being given information on how to access these. Generalizability may also be affected by the fact that participants were majority Caucasian and had at least some post-secondary education, though the distribution we observed in our cohort is similar to that of the larger population in the study setting (Ottawa, Canada). 32
Conclusion
Severe grief was and is a substantial source of psychological morbidity among bereaved family members during the COVID-19 pandemic. Since these data reflect only the first wave of the COVID-19 pandemic, we can anticipate similar waves of severe and prolonged grief following subsequent waves, many of which caused greater mortality than the first. Our findings highlight an acute need for effective, scalable, and acceptable means of addressing severe grief for this population.
Footnotes
Appendix
Acknowledgements
PGL, HAP, LC, VG, RM, GW, AB, KB, CD, PE, ID, KW, SHB, PT, and JD receive an Academic Protected Time Award from the Department of Medicine, University of Ottawa, Ottawa, Canada. PT is supported by a PSI Graham Farquharson Knowledge Translation Fellowship.
Authorship
JD, JL, and KA were the primary writers of the manuscript. JD, PGL, JL, CW, HAP, LC, and VG were responsible for study design and methods. SHB, SRI, PT, and BV-W also consulted on study methods. KA, PGL, MK, CN, BH, HAP, LC, VG, EB, SA, RM, GW, AB, KB, CD, PE, ID, KW, KA-M, DB, AI, and JD contributed to data collection. CW, JL, KA, JD, and PGL were responsible for data analysis planning and/or execution. All authors reviewed the manuscript prior to submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the University of Ottawa COVID-19 Pandemic Response Funding Program, and with funding from Health Canada’s Health Care Policy and Strategies Program through the Pan-Canadian Palliative Care Research Collaborative. The views expressed herein do not necessarily represent the views of either funder.
Ethics and consent
This study was approved by the Research Ethics Boards at all participating hospitals: Ottawa Health Science Network-REB (20200653-01H, December 18th 2020); Hôpital Montfort REB (20-21-10-032, December 2nd 2020); and Queensway Carleton Hospital REB (20-06, December 1st 2020). All participants provided first-person informed consent for their participation in the study.
Data sharing
Inquiries about data sharing can be directed by email to the corresponding author, Dr. James Downar: jdownar@toh.ca.