
Abstract
Background:
The COVID-19 pandemic has caused millions of deaths worldwide, leading to symptoms of grief among the bereaved. Neither the burden of severe grief nor its predictors are fully known within the context of the pandemic.
Aim:
To determine the prevalence and predictors of severe grief in family members who were bereaved early in the COVID-19 pandemic.
Design:
Prospective, matched cohort study.
Setting/Participants:
Family members of people who died in an acute hospital in Ottawa, Canada between November 1, 2019 and August 31, 2020. We matched relatives of patients who died of COVID (COVID +ve) with those who died of non-COVID illness either during wave 1 of the pandemic (COVID −ve) or immediately prior to its onset (pre-COVID). We abstracted decedents’ medical records, contacted family members >6 months post loss, and assessed grief symptoms using the Inventory of Complicated Grief-revised.
Results:
We abstracted data for 425 decedents (85 COVID +ve, 170 COVID −ve, and 170 pre-COVID), and 110 of 165 contacted family members (67%) consented to participate. Pre-COVID family members were physically present more in the last 48 h of life; the COVID +ve cohort were more present virtually. Overall, 35 family members (28.9%) had severe grief symptoms, and the prevalence was similar among the cohorts (p = 0.91). Grief severity was not correlated with demographic factors, physical presence in the final 48 h of life, intubation, or relationship with the deceased.
Conclusion:
Severe grief is common among family members bereaved during the COVID-19 pandemic, regardless of the cause or circumstances of death, and even if their loss took place before the onset of the pandemic. This suggests that aspects of the pandemic itself contribute to severe grief, and factors that normally mitigate grief may not be as effective.
Early studies in the COVID-19 pandemic have suggested a high prevalence of severe grief symptoms, although most have used convenience or survey sampling methods which may bias the results, and most have assessed symptoms before pathological grief can be diagnosed (<6 months).
Little is known about how the burden of severe grief during the pandemic compares with pre-pandemic times, and whether the cause of death during the pandemic affects the grief experience.
This prospective, matched cohort study shows that almost 30% of bereaved family members experience severe grief during the pandemic. This prevalence is higher than reported pre-pandemic rates (2%–3%), and that the prevalence was not affected by the cause or the circumstances around the death.
There is an elevated risk of severe grief among family members of people who experience bereavement during the pandemic period, even if their family member died before the pandemic itself.
The severity of grief may not be affected by factors that normally mitigate severity of grief, such as being present at the time of death.
There is an urgent need for resources to identify and support people who lose loved ones during the COVID-19 pandemic.
Introduction
The COVID-19 pandemic has caused millions of deaths worldwide and affected end-of-life care through family separation due to visitor restrictions and public health measures, disruption of funeral rites, and restriction of social engagement during bereavement.1–13 Normally, death produces a grief response in family members and friends; severe grief, marked by profound emotional response and social dysfunction, is generally uncommon following a loss (2%–3%). 3 However, the combination of increased mortality (both COVID and non-COVID related) and disrupted end of life care during the pandemic could lead to a surge in severe grief. Early studies have suggested a high prevalence (29%–70%) of severe grief among those bereaved in the COVID-19 pandemic,4–8 but many of these studies have used convenience sampling, and focused on early bereavement (<6 months), before pathological grief can be diagnosed.3,9,10 Most also included only those bereaved due to COVID-19, precluding comparative analyses of how grief symptoms were influenced by the cause of death and the effect of restrictions.
To address these gaps in our knowledge, we sought to determine the prevalence and predictors of severe grief in a multicenter, prospectively-defined cohort of family members bereaved due to COVID-19 during the first wave of the pandemic in Ottawa, Canada, and compare the severity of their grief to family members of non-COVID and pre-pandemic decedent cohorts.
Methods
Design and setting. Prospective multicenter matched cohort study of family members of inpatient, acute care decedents in Ottawa (population 1.4 million) between November 1, 2019 and August 31, 2020. Ottawa’s three acute care hospitals and early pandemic details are described in the Appendix. The first reported case of COVID in Ottawa was diagnosed March 11, 2020.
Population
The first cohort (COVID +ve) included all 85 patients who died of COVID-19 infection at an acute hospital between March 1 and August 31, 2020. The second cohort (COVID −ve) included patients who died of a cause other than COVID-19, between March 1 and August 31, 2020. The third cohort (Pre-COVID) included patients who died of any cause between November 1, 2019 and February 29, 2020. The COVID −ve and pre-COVID cohort was matched 2:1 with the COVID +ve cohort patients for sex, age (within 5 years), and medical service at death (ICU or ward) for statistical comparison.
Enrollment and data collection
Data about clinical care, demographics, and physical or virtual visits were abstracted from decedents’ medical records; 154 (35%) underwent duplicate abstraction to confirm accuracy. Decedents’ clinical data will be reported separately. Phone contact was attempted with the next-of-kin >6 monthsafter death to offer enrollment; additional close family members were offered enrollment if they expressed a strong, spontaneous desire to participate (e.g. if the deceased had multiple children, each with a strong desire to participate). We collected demographic data from the next-of-kin; we assessed closeness to the deceased using the 16-item Brief Family Relationship Scale (BFRS; higher scores indicate a closer relationship) 11 ; and used the Inventory for Complicated Grief-revised (ICG-r) to determine the presence of severe grief (ICG score >25). 12 We also collected data about spirituality, previous mental illness, and the involvement of social supports or other interventions to reduce grief symptoms; these will be reported separately.
Analysis
Clinical and other characteristics were compared according to COVID group, as well as between participating and non-participating family members, using a chi-square test for categorical variables, and an ANOVA or Kruskal-Wallis test for continuous variables, as appropriate. We evaluated associations between severe grief and COVID status and other known factors associated with grief severity, including family relationship, 13 physical presence in the last 48 h of life, 14 and intubation status 14 using bivariate logistic regression, reporting unadjusted odds ratios (OR) and 95% confidence intervals (CI). There was no missing data for the parameters included in the analyses. We hypothesized that grief symptoms would be worse among those bereaved during the pandemic than those bereaved pre-pandemic, but that symptoms would be similar between COVID and non-COVID deaths in the pandemic.
Ethics
This study was approved by the Research Ethics Boards at all participating hospitals: Ottawa Health Science Network-REB (20200653-01H, December 18th 2020); Hôpital Montfort REB (20-21-10-032, December 2nd 2020); and Queensway Carleton Hospital REB (20-06, December 1st 2020).
Results
Data were abstracted for 425 decedents (85 COVID +ve, 170 COVID −ve, and 170 pre-COVID). Of the 425 next-of-kin approached, 165 (38.8%) were contacted and 110/165 (67%) consented to enrollment (Figure 1). A second and third family member subsequently enrolled (at their request) in 10 and 1 cases, respectively, for a total of 121 bereaved family members (30 (24.8%) COVID +ve, 46 (38.0%) COVID −ve, and 45 (37.2%) pre-COVID). There was no significant difference in measured patient characteristics (death location, intubation rate, age, sex, referral source, duration of stay, or number of interactions with the patient or family) between participating and non-participating family members (data not shown).
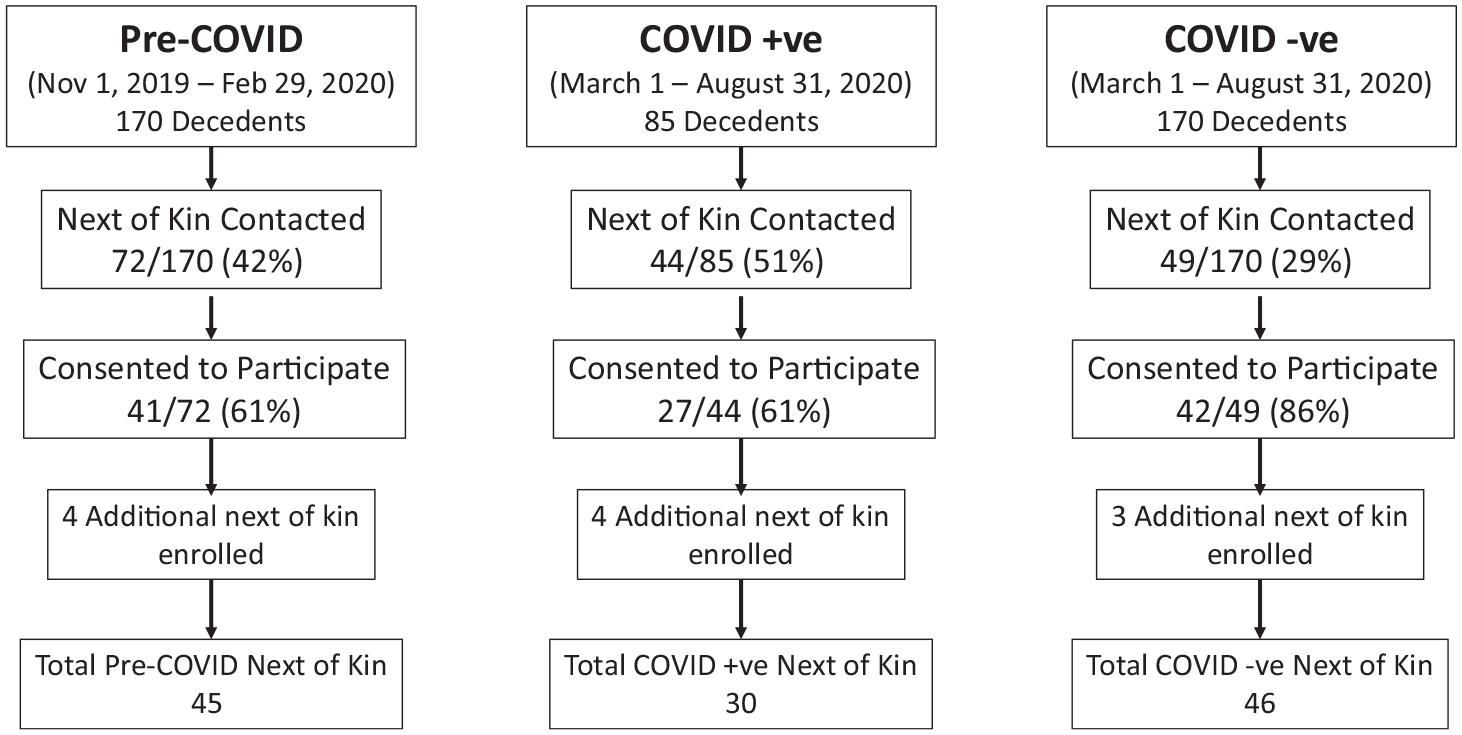
Screening and enrolment of participants.
The mean age of the family members was 58.4 years, and the majority were Caucasian (76%), female (66%), married (44%) or widowed (21%), and the child of a decedent (62%) (Table 1). The mean BFRS score was 14/16, suggesting a close relationship to the deceased, and 79% were physically present in the final 48 h of life. Family members in the pre-COVID cohort were physically present in the last 48 h of life more frequently than those in the COVID +ve and COVID −ve cohorts (97.8% vs 56.7% and 73.9%, respectively; p < 0.01), whereas virtual presence occurred more frequently in the COVID +ve cohort than in the COVID −ve and pre-COVID cohorts (40% vs 13% and 0%, respectively; p < 0.01). Cohorts did not differ in relation to ICU admission, endotracheal intubation, age, sex, service, or length of stay.
Demographics of participants and care details of decedents.
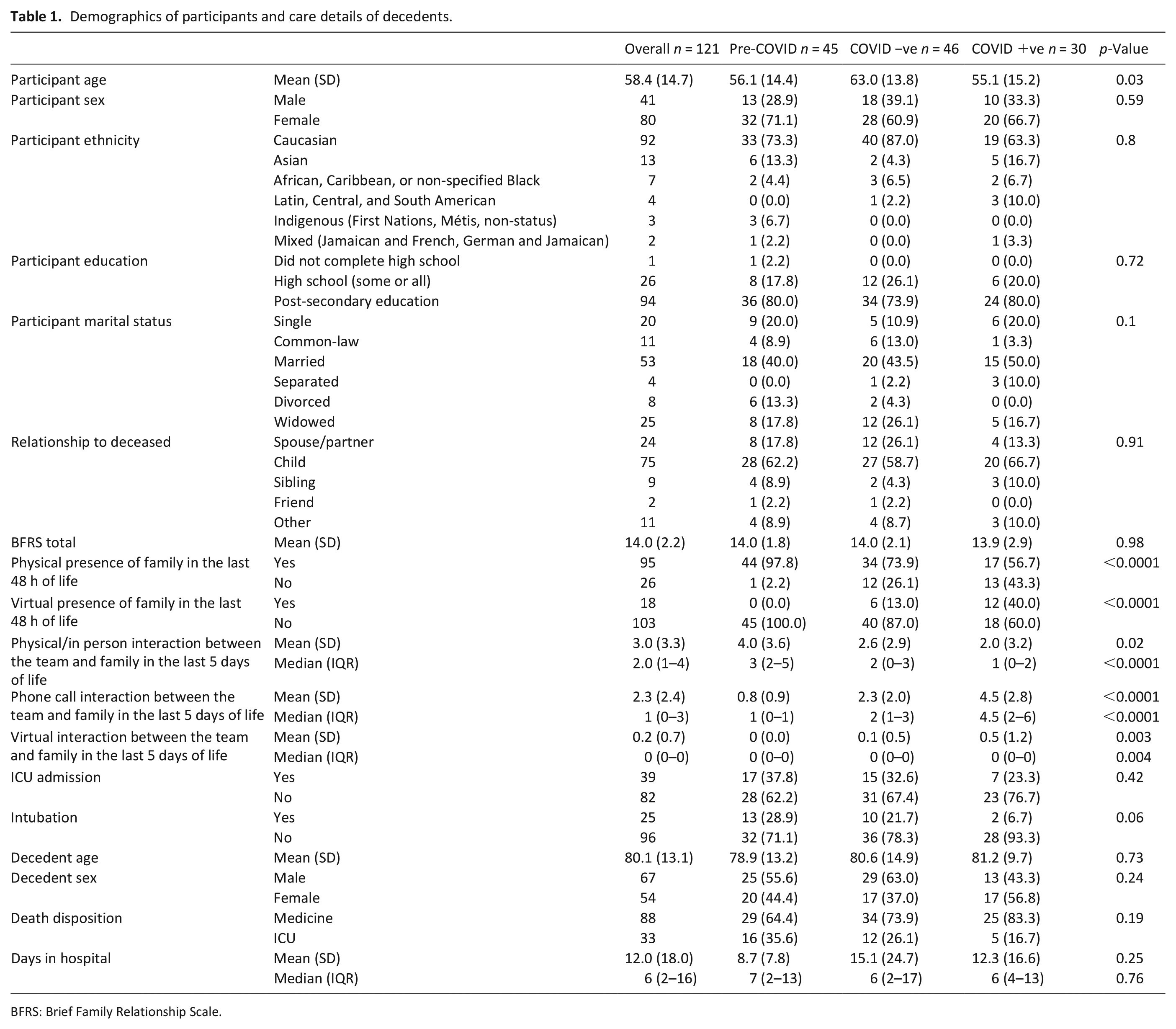
BFRS: Brief Family Relationship Scale.
Overall, complicated grief was observed at >6 months post-death in 9/30 (30%) relatives of COVID +ve decedents, compared to 14/46 (30.4%) and 12/45 (26.7%) of relatives of COVID −ve and pre-COVID decedents, respectively (Table 2). Neither the presence of severe grief nor the ICG-r score itself were associated with COVID status, BFRS, physical presence in the last 48 h of life, or endotracheal intubation.
Association between severe grief and participant characteristics and care details.
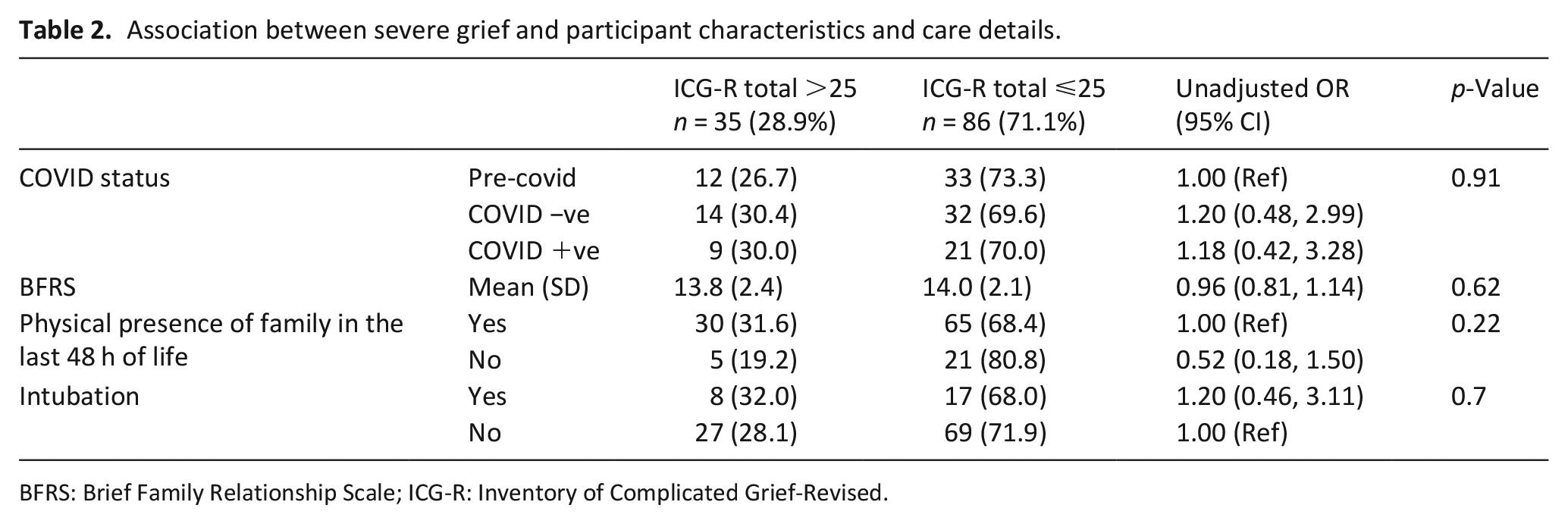
BFRS: Brief Family Relationship Scale; ICG-R: Inventory of Complicated Grief-Revised.
Discussion
In this matched cohort study, almost one third of family members who experienced bereavement during the early COVID-19 pandemic had symptoms of severe grief. Most were physically present around the time of death, and symptom severity was not associated with any measured factor related to family members or patient care, nor did it vary according to whether the decedent died of COVID-19 or a non-COVID illness. Grief symptoms were equally high even among those who lost family prior to the pandemic, but went through their grief experience during the pandemic period.
Our findings confirm that the burden of severe grief symptoms during the COVID-19 pandemic is far in excess of normal times.3–8 Prior to the pandemic, we reported a multicenter Canadian study in which only 19% of family members of ICU decedents (another high risk group) had ICG scores >25. 15 Contrary to our hypothesis, grief severity in the current study was equally high among all participants who experienced bereavement during the pandemic, even if their loss occurred prior to the onset of the pandemic. Grief severity was also not affected by the family relationship style; close relatives usually have higher risk of developing severe grief than more distant relatives,6,16 and psychomorbidity is greater among bereaved from families with conflicted relationships. 13 Eisma et al. 17 reported that grief symptoms among those bereaved due to COVID-19 were more severe than for other causes of death, and they found in a multivariable model that the unexpectedness of the COVID-19 deaths mediated this effect. Unlike these studies, we examined symptoms >6 months post-loss and so even our pre-COVID cohort of family members was likely affected by the pandemic’s social restrictions during their bereavement. Murata et al. 7 found that loneliness during the pandemic was a substantial driver of psychiatric morbidity, particularly among adolescents and young adults. If so, our findings suggest that ongoing social restrictions during the pandemic may have interrupted the normal process of grieving such that even low-risk family members who were present and well-supported at the time of an expected death, or those who lost family prior to the pandemic, are at elevated risk of developing severe grief.
This study’s strengths include the prospective design, and enrollment of family members of acute care decedents representative of an urban population of >1 million people. Our findings may therefore be less biased than those from convenience samples, which reported higher prevalence of severe symtoms.4–8 We also waited >6 months from the death; diagnoses of Complicated Grief and either Persistent Complex Bereavement Disorder or Prolonged Grief Disorder can only be made after 6 3 and 12 months, 9 respectively. Earlier assessments may overestimate the burden of severe grief. Finally, we compared symptoms among family members of matched cohorts of patients to better understand how grief related to the cause of death, the care provided, the ability of the family to be present at the time of death, and the availability of normal social activities during the grieving process.
Limitations include an enrollment restricted to family members of acute care decedents; most early COVID-19-related deaths in Canada occurred among long-term care residents. 18 Moreover, our contact and response rate was low, which is unavoidable in bereavement studies; we cannot exclude a participation bias. Our definition of severe grief may differ from that used in other studies; bereavement is an evolving field of study, and debate continues about which definition best represents the pathological condition of interest.10,19 A recent meta-analysis suggested that the ICG-r is superior to other grief measurement tools for measuring the effect of bereavement interventions, 16 but a number of new diagnostic tools have been developed for severe grief reactions in recent years. A brief, 5-item Pandemic Grief Scale has shown promise for identifying dysfunctional grief in the pandemic. 20 We did not report associations of grief symptoms with spirituality or previous mental illness, or the involvement of social supports or other interventions to reduce grief symptoms; these will be reported separately. Finally, in some cases we enrolled a second or third family member of the same deceased individual, which could raise concerns about a “nesting” effect. However, since the number of second or third family members was small and the family relationship score did not correlate with grief, it is unlikely that nesting would explain our findings.
In conclusion, our study found that almost one third of family members who experienced loss or whose bereavement took place during the COVID-19 pandemic had severe grief symptoms, regardless of the cause of death. This suggests that aspects of the pandemic itself contribute to severe grief, and factors that normally mitigate grief may not be as effective. Longitudinal follow up of these participants using mixed methods will evaluate their long-term outcomes and explore their experience of bereavement support. Our study highlights a compelling need for effective means of preventing and treating the ongoing pandemic of grief that is following the pandemic of COVID.
Footnotes
Appendix
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the University of Ottawa COVID-19 Pandemic Response Funding Program, and with funding from Health Canada’s Health Care Policy and Strategies Program through the Pan-Canadian Palliative Care Research Collaborative. The views expressed herein do not necessarily represent the views of Health Canada.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.