
Abstract
Background:
Siblings of children requiring palliative care are often forgotten and overlooked, as the focus tends to be on the ill child and their parents. Limited knowledge of non-bereaved siblings’ perspectives makes it challenging to provide appropriate support for them. A review of existing literature is thus needed to better understand the experiences of these siblings and to identify research gaps that may require further examination.
Aim:
To consolidate the available qualitative evidence on the perspectives of non-bereaved healthy siblings regarding paediatric palliative care.
Design:
A qualitative systematic review using a meta-synthesis approach was conducted.
Data sources:
Six electronic databases (PubMed, CINAHL, PsycINFO, Embase, Scopus and ProQuest Dissertations and Theses Global) were searched from each database’s inception date until October 2022. The search included qualitative and mixed-method studies that reported the perceptions and associations of siblings of patients receiving paediatric palliative care. Data were synthesised using thematic analysis.
Results:
Eleven studies were included. The overarching theme of the review would be ‘A walking shadow: Living in the darkness shaped by the dying sibling’, and three key themes and nine subthemes were identified from the included articles: (1) Changing family dynamics; (2) Impact on school and socialisation and (3) Psychological impact and coping.
Conclusion:
Siblings demonstrated negative psychological impacts and were affected by changing family structure and relationships. However, socialisation with society, and varied coping skills such as cognitive coping and using distraction techniques, were significant for siblings to go through this journey and even led to some positive outcomes for them.
Siblings of paediatric palliative care patients are often forgotten and overlooked by caregivers/providers
All the existing reviews have focussed on children with life-threatening conditions, primarily on cancer
There is currently no existing review that covers the perspectives of siblings including all types of palliative conditions
The experiences of non-bereaved healthy siblings differ from those of bereaved siblings examined in the existing literature
This would be the first review exploring palliative care as an umbrella term integrating the perspectives of siblings with all types of diseases defined under palliative conditions
Potential ‘family-school-clinician’ partnership wherein all involved stakeholders are aware of the needs of siblings and provide timely support to prevent any undue distress.
Engaging relevant supports, like child life specialists, school counsellors or psychologists early in the illness trajectory to provide healthy siblings with the necessary support
Healthcare professionals to initiate education and involvement of healthy siblings in care planning early in the illness trajectory
Introduction
Paediatric conditions requiring palliative care are known to cause a ripple effect on the wider family networks. 1 Research has demonstrated the multidimensional impact that caring for a child with a palliative condition has on families, such as the emotional, physical, financial and spiritual consequences on their lives. 2 When exploring the demands of caregiving on family members, the predominant focus – both clinically and in research, is placed on the patient and their parents, while healthy siblings are often overlooked. 3 The knowledge of the effects of palliative illness on a child’s brother or sister is limited, which may also be due to the range of possible palliative conditions a child may be diagnosed with. Therefore, siblings living in the shadow of their severely ill siblings are often referred to as ‘forgotten’ mourners. 4 Overall, despite the strong influence siblings have on each other and the extent to which a child with palliative illness can influence entire family dynamics, research exploring the perspectives of these siblings is limited. 5
The experiences of siblings of individuals receiving palliative care can differ from those of the parents of these individuals. It is possible that different amounts of attention that each child is getting from their parents can lead to resentment and competitiveness arising from sibling rivalry. 6 Additionally, some studies have also reported that siblings of individuals with palliative conditions are at an increased risk for psychological maladjustments and other long-term issues like reduced quality of life.7–9 This can often affect other aspects of their life, such as family relationships and school functioning. 10 On the other hand, other studies have highlighted positive changes observed in siblings during the process of going through such a difficult period within their family. This includes increased maturity, family cohesion and empathy.11,12 Therefore, it is important to examine the experiences and perspectives of these siblings to identify existing gaps in research as well as the strengths and limitations in palliative care to better cater to their needs.
Presently, an expanding body of reviews worldwide has examined bereaved siblings of children receiving palliative care.13–19 Bereaved siblings refer to healthy, surviving siblings who have experienced the death of their ill sibling. These bereaved siblings have illustrated different perspectives, experiences and associations as compared with non-bereaved peers. 20 As the needs of healthy siblings generally vary depending on the condition that resulted in the ill sibling’s palliative care needs, 20 a qualitative review that explores the perspective and voice of the healthy sibling, including contemporaneous rather than retrospective reports of their experiences and associations is necessary.
Currently, there is no existing review integrating the experiences of non-bereaved siblings within the umbrella term of ‘palliative care’, which synthesises the varied perspectives associated with illnesses classified under the conceptually clarified definition of palliative conditions. Palliative conditions include all types of life-threatening and life-limiting conditions, regardless of age and the stage of illness. To improve the care provided for individuals with palliative conditions and their families, it is crucial to not only focus on these individuals and their parents but also their siblings. Hence, this review aims to consolidate the available qualitative evidence on healthy, non-bereaved siblings’ contemporaneous perspectives with paediatric palliative care.
Methods
Systematic literature review question
What is currently known about the perceptions of non-bereaved healthy siblings about paediatric palliative care?
Design
To obtain a comprehensive overview of siblings’ perceptions regarding palliative care, a qualitative systematic review was conducted. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 21 (see Supplemental Appendix 1) and the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) 22 were used to guide the reporting of this qualitative review.
Search strategy
Six electronic databases (CINAHL, Embase, PsycINFO, PubMed, Scopus and ProQuest Dissertations and Theses Global) were searched systematically by two reviewers (PR and SS) from the inception of each database to October 2022 for published and unpublished English language studies. Consultations with the medicine librarian were made to develop an effective search strategy. The search strategy included three fundamental concepts: ‘siblings’ AND ‘paediatric’ AND ‘palliative care’ (see Supplemental Appendix 2). Keywords, subject headings and combinations were further refined to optimise the search results for each database. The bibliographies of relevant studies were hand-searched to prevent the exclusion of potential studies.
Eligibility criteria
The inclusion criteria were studies involving: (i) healthy siblings of children below 18 years old receiving palliative care, hospice care, terminal care, end-of-life needs or with existing life-limiting or life-threatening conditions, (ii) non-bereaved, (iii) with healthy siblings aged above 6 years of age or (iv) parents’ excerpts specifically highlighting the experiences and perspectives of healthy siblings below 11 years old were also included especially if the included studies mentioned that young siblings were unable to accurately provide their accounts. Studies that reported both parent and sibling perspectives were excluded unless siblings’ reports could be separately extracted. All relevant qualitative studies with varied methodologies such as phenomenology and ethnography as well as mixed-methods studies where qualitative data could be exclusively extracted were included in this review.
Studies were also excluded if they: (i) reported perspectives of siblings of healthy children, (ii) combined experiences of both bereaved siblings and siblings of an ill child where results specific to non-bereaved siblings cannot be extracted separately, (iv) focussed solely on interventions and (v) not available in English. Additionally, quantitative studies, conference proceedings, editorials, reports and/or reviews were also excluded. The EndNote X9 programme 23 was used to import and remove duplicate studies. Two reviewers (PR and SS) independently screened studies and had 95% agreement on the extracted data from the included studies. Any discrepancies were clarified with the other co-authors until the consensus was achieved.
Quality appraisal
The Critical Skills Appraisal Programme (CASP) tool was used by two independent researchers to appraise the quality of individual qualitative studies and the extracted qualitative data from the mixed methods studies. 24 As selecting studies based on methodological quality may introduce selection bias and inconsistency, no studies were excluded to ensure all relevant data on siblings were consolidated and interpreted.25,26 Any disagreements that arose were resolved through discussions to consensus.
Data extraction
The authors’ developed extraction form was used and the following relevant data were extracted: (i) author(s), year and country; (ii) study design and aim(s); (iv) sample characteristics; (v) methodology and (vi) findings or themes and subthemes related to siblings’ perceptions and associations with paediatric palliative care.
Data synthesis
Data synthesis was undertaken independently by two reviewers (PR and SS) following Sandelowski and Barroso’s two-step approach. 27 This approach entails a preliminary meta-summary phase followed by a subsequent meta-synthesis phase. The initial meta-summary phase consists of (i) identifying and extracting precise research findings from both primary (participants' quotes) and secondary constructs (primary authors’ interpretations of the findings), (ii) separating these findings from other data and findings about the perspectives of healthy siblings, (iii) grouping the segregated findings based on their topical similarity (see Table 1) and (iv) abstracting, refining and condensing findings into more concise explanations. Subsequently, in the meta-synthesis phase, Thomas and Harden’s 28 thematic analysis approach was used to categorise pertinent codes relating to healthy siblings’ perceptions into descriptive themes and subthemes. Thereafter, these descriptive themes underwent a continuous iterative process involving re-reading and re-comparing with the data from the included studies. This led to the development of analytical themes, which in turn offered comprehensive, novel and insightful interpretations into the realm of siblings’ perceptions around the paediatric palliative care of their sick sibling. Any discrepancies that arose were discussed between the two reviewers until a consensus was reached, before the finalisation of the analytical themes. Triangulation of the findings was maintained throughout the meta-syntheses through constant targeted comparison of individual studies to unravel and meta-synthesise novel and systematic understandings of healthy siblings’ perspectives.
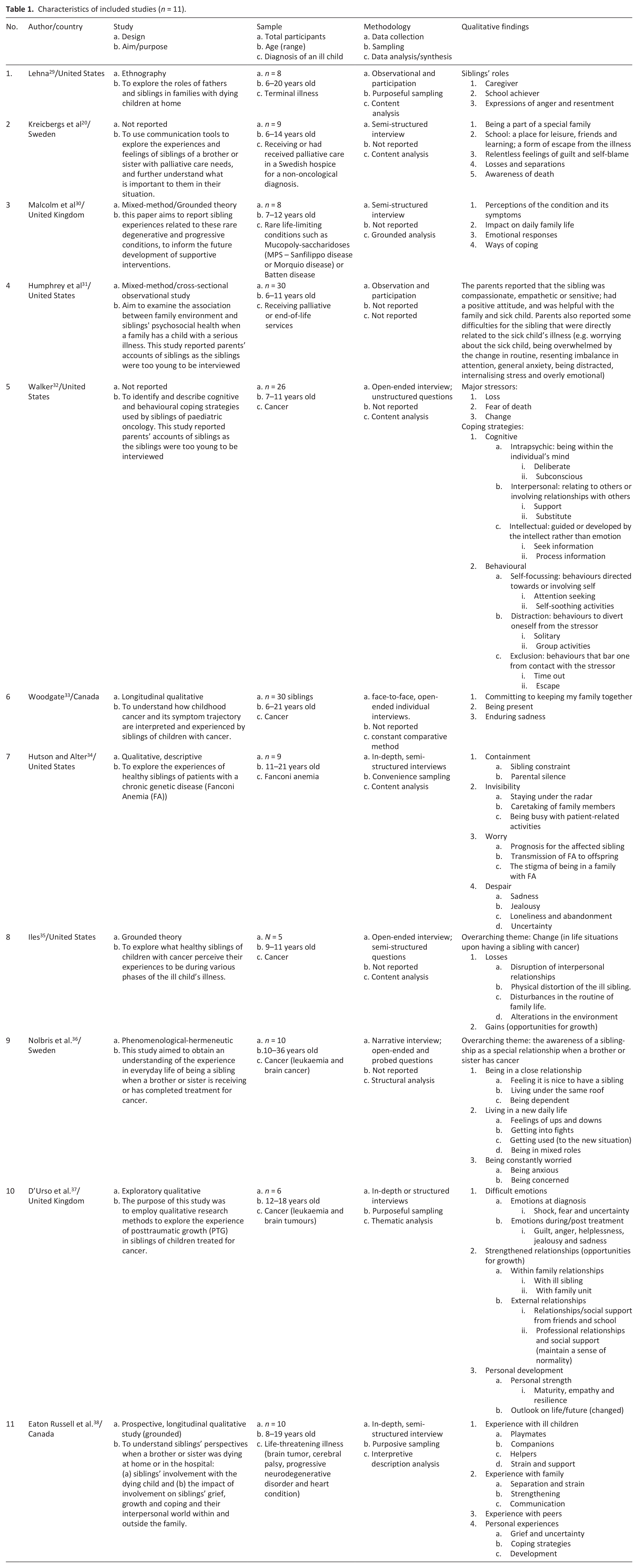
Characteristics of included studies (n = 11).
Results
Search outcomes
A total of 4494 studies were retrieved and upon removing duplicates, 3192 titles and abstracts were screened for relevance. The full texts of 113 studies were further assessed for eligibility. In total, 11 qualitative studies were finalised and included in this review. The detailed PRISMA flow diagram is presented in Figure 1.
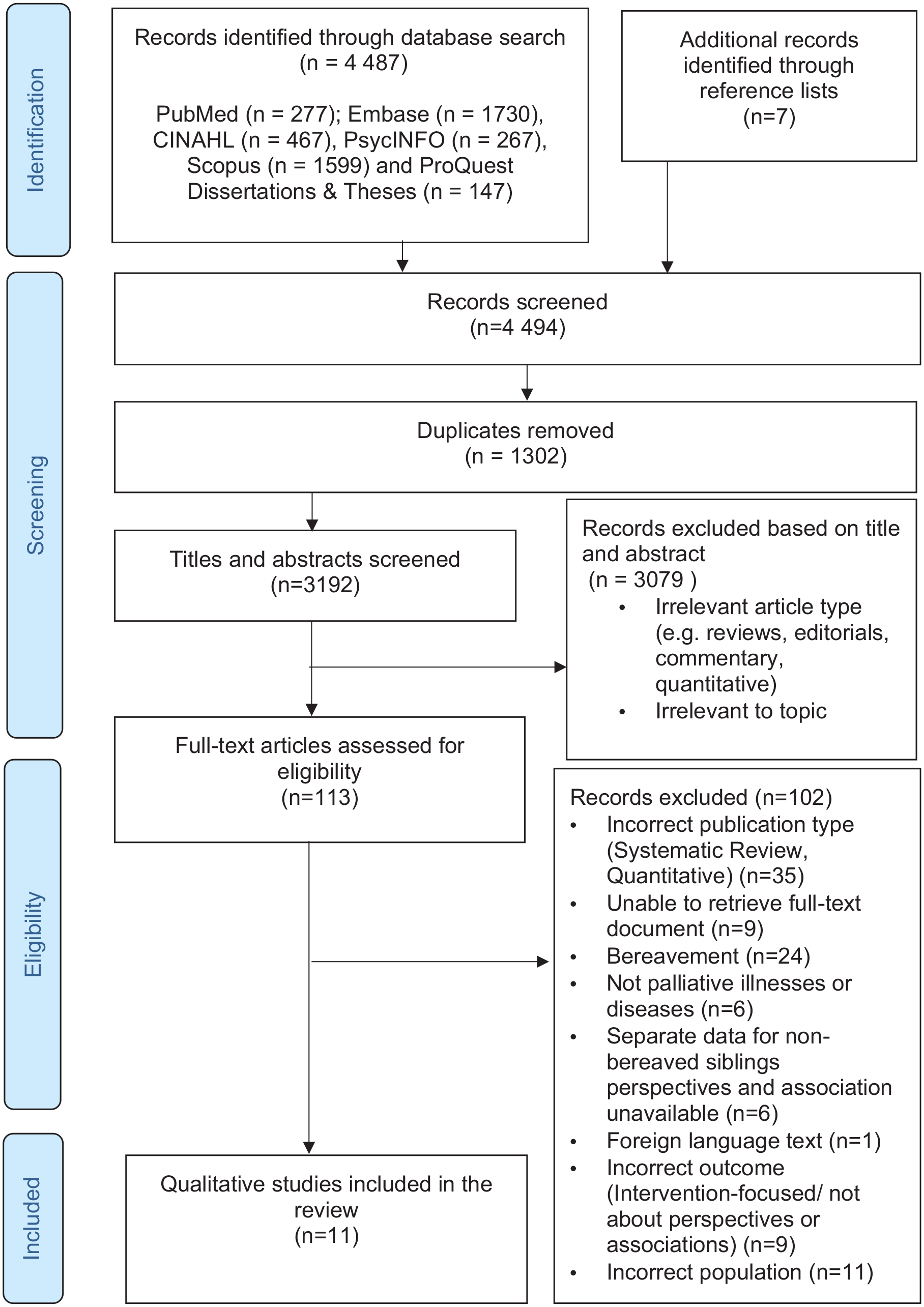
PRISMA flow diagram.
Study characteristics
The included studies were published between 1979 and 2022. The majority of the studies were published in the United States (n = 5) followed by two papers each in Canada, the United Kingdom and Sweden. Cumulatively, a total of 151 siblings ranging from 6 to 36 years old were analysed in this review. Mixed methods were used in two of the studies for data collection, however only qualitative data was extracted for this review. Of the nine included qualitative studies, grounded theory app-roaches, ethnography, descriptive and phenomenological-heuristic approaches were used, and two studies did not report any specific qualitative approach in their study. Two studies included in the review included parents’ reports31,32 due to the healthy siblings’ young age of between 6 and 11 years old and reported by the authors of the included studies that the siblings were too young to be interviewed.
Detailed characteristics of the included studies are presented in Table 1 while further elaborations of the themes and subthemes as identified in the included studies are appended as Supplemental Appendix 3. Details of the quality appraisal of the included studies are appended in Supplemental Appendix 4.
The overarching theme identified was ‘A walking shadow: Living in the darkness shaped by the dying sibling’. Siblings living in the shadow of a severely ill brother or sister are glossed over within the confines of their family with their lived experiences often forgotten and overlooked. The synthesis of findings identified three main themes and nine sub-themes, and further details are provided in Supplemental Appendix 5 and the following section (Figure 2).
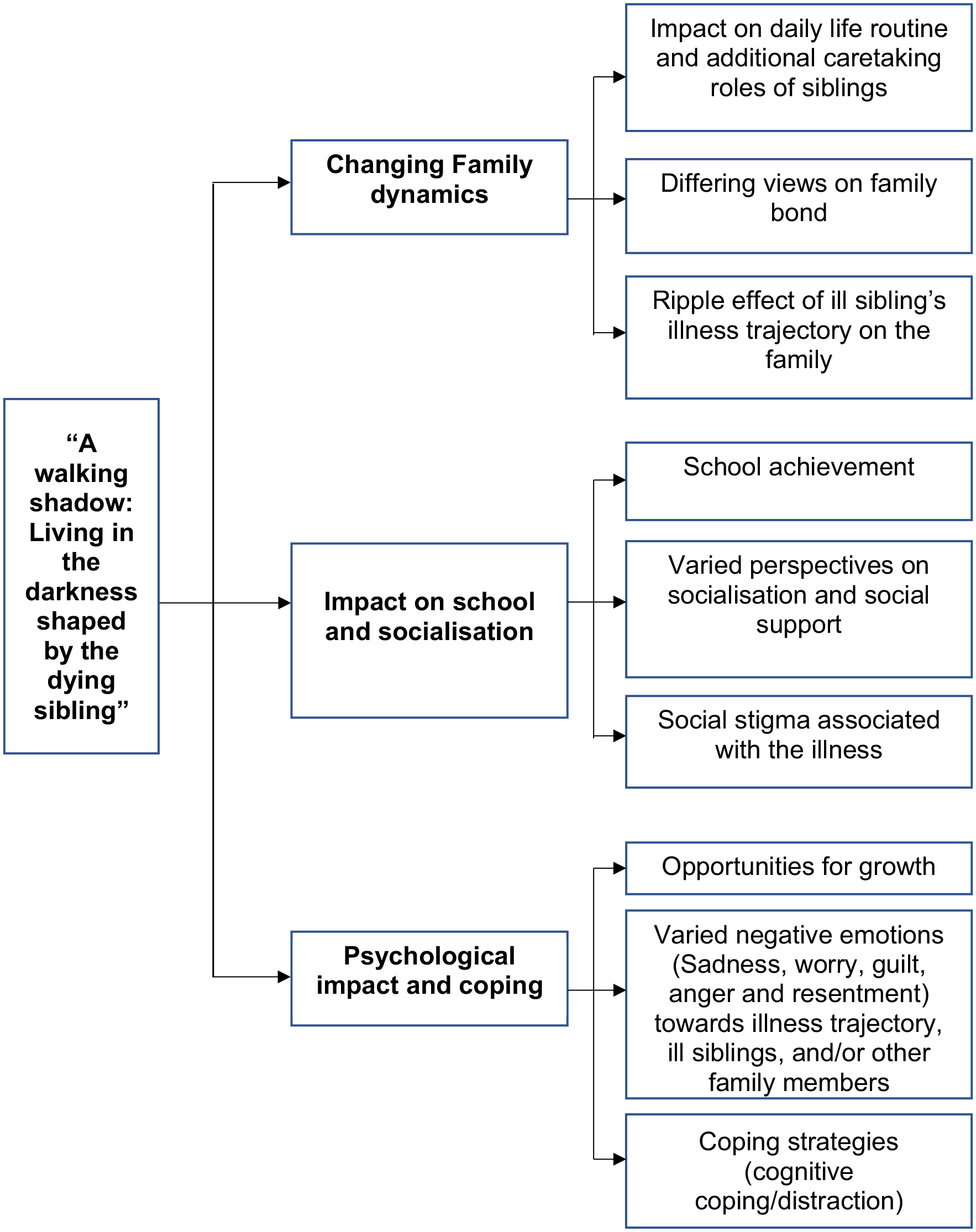
Overview of themes and subthemes.
Theme 1: Changing family dynamics
This theme examined siblings’ perceptions of change in the family dynamics.
Impact on daily life routine and additional caretaking roles of siblings
Healthy siblings perceived disruption in their family routine and a loss of normality due to the sick child’s condition and several expressed being overwhelmed and stressed by the change.20,31,32,35,36 Siblings expressed a change in routine family activities (e.g. meal times), alterations in the environment (e.g. making way for the child’s medical equipment) and family events (e.g. holidays) have to be planned around the sick child and their needs.33,35 While some siblings expressed their desire to return to the period before the illness diagnosis, or ‘how it used to be’, 35 therefore, mourning over their lost routines, some siblings understood that this may not be possible. Understanding the situation and learning to familiarise themselves with the new routine allowed them to be accustomed to the new normal as highlighted by one sibling in a recent study ‘So, in one way you lose your regular life. But now this has become my regular life, so in one way I haven’t lost it. . .’20,36
However, a pervading change in family dynamics among the majority of the studies would be the additional caretaking roles adopted by the healthy siblings such as shouldering additional household chores and responsibilities within the family to help ease the burden on their parents.31,33 They also undertook the caring or protective role similar to a parent or caregiver as they demonstrated an increased sense of responsibility in helping to care for their sick siblings.32,36 The healthy siblings wanted to be part of the ‘taking care’ experience of their ill sibling33,34 and were proud of the range of physical, personal, social and emotional care they can execute regarding the care of their ill siblings.29,35 Therefore, besides undertaking responsibilities such as cooking and cleaning, healthy siblings also provided direct physical care for the ill child and this included feeding, toileting, dressing, putting in the car seat and carrying children who were unable to walk29,38 as one 17-year-old female siblings noted ‘I moved back here and took care of my sister and mom. Mom was a wreck. So, I more or less cooked, cleaned and was the shoulder for everybody’. 33
Differing views on family bond
On one end of the spectrum, siblings expressed the struggles endured by the family while transitioning through the palliative illness, whereas on the other end working together and sharing a housing environment helped them to get closer as a family. As shared by one of the siblings ‘‘do more things within the family, like eating dinner and lunch’ 36 strengthened their familial bonds with their parents and ill siblings.33,38 This growing sense of closeness could be felt when the family members were physically together and healthy siblings actively wanted to engage in activities together during the times when the sick child was not hospitalised but also included a shared understanding and appreciation over time spent together extending beyond physical boundaries.37,38
In sharp contrast, most siblings also illustrated feeling less cared for within their family unit or rather ‘being invisible’, especially during frequent and/or prolonged absences from the home consequently resulting in unmet needs due to the increased attention required by their ill brother or sister.20,33,35,36 While some studies reported siblings’ resentment and jealousy towards the imbalance in attention,21,33,34 it is critical to highlight that these feelings were not directed towards their sick sibling as they were able to recognise the necessity behind their parents diverting their attention to the needs of the ill sibling.33,38
The ripple effect of an ill sibling’s illness trajectory on the family
The healthy siblings identified an association between the sick child’s illness trajectory and their impact on their family 36 as one sibling highlighted ‘Things are always a bit like “down” . . . like my mum and dad won’t be the same. . .’. 30 The family members’ lives often revolved around their sick sibling’s illness given the chronic uncertainty surrounding the treatment regimen, particularly during the active treatment stage where there was a sense of family life ‘standing still’.33,37 ‘Good periods’ in the disease trajectory caused a positive ripple effect on the family, and in contrast, the ill child’s deterioration of health and increased symptom distress impacted the family negatively. 36 This is illustrated in the escalating anxieties reported by the healthy siblings during the active treatment phases.30,33 The siblings also recognised that each new illness event caused their family unit to become more separated and escalated their parents’ suffering.30,33
Theme 2: Impact on school and socialisation
School achievement
Academic achievements and activities within the school setting were viewed as highly significant among healthy siblings with several declaring their ambitious goals for their future working life.20,29 Healthy siblings tend to want to stay under the radar to avoid conflict and to earn the approval of their parents by meeting their parents’ expectations of them. 34
Varied perspectives on socialisation and social support
Siblings reported their main sources of interpersonal support being family members as well as their peers who were most supportive and understanding of their familial situation, hence, providing them with an avenue to share their feelings openly and as an escape from the illness.20,30,32,37 Additionally, eliciting social support externally via professionals who empathise with them, provide them with a safe space to process what was happening. 37 However, despite understanding the significance of connecting with hobbies and social or extracurricular activities in allowing them to maintain a sense of normality, identity and routine in their lives, healthy siblings had limited time to spare to engage in social, and extracurricular activities and hobbies such as listening to music. 30 This is attributed to their involvement in the ill child’s care.30,34,35,37,38 Healthy siblings were also affected by limitations in their family’s social experiences and activities stemming from the ill child’s needs as one sibling highlighted how he felt ‘really like, upset . . . It’s like when we can’t go out as a family if he’s got a cough or something ‘cause . . . on Christmas we were supposed to go to my granddad but (my brother) wasn’t well so it was just me and my sister who went up’. 30
The social stigma associated with the illness
Negative social attitudes surrounding palliative conditions were a worry experienced by healthy siblings as, despite peer groups functioning as a crucial source of support and escape, their feelings of rejection were further compounded by the inability to talk about the illness with their friends.30,34 Some siblings highlighted how financial constraints in their family which were often a result of overwhelming medical expenses caused embarrassment at school. 34 This prejudice in schools and within the community manifested as healthy siblings being repeatedly teased because of the sick child’s condition or directed towards ill siblings. 30 This was further exacerbated by how authority figures had not, to their knowledge, intervened to manage the situation. 30 Several healthy siblings reported that these tensions in the school environment arose from the ill sibling having an altered appearance and/or frequent absences for clinic and hospital purposes wherein one sibling revealed, ‘l have to go to the teacher sometimes to threaten the kids (who make fun of ill sibling)’. 35
Theme 3: Psychological impact and coping
Varied negative emotions
Healthy siblings largely described feelings such as worry, anxiety, stress and sadness associated directly with the changes experienced in their family and family way of life and with concerns they have over the ill sibling’s health given the progressive and degenerative nature of these conditions and the fear of inevitable death and its impact on family life.30–34,36,38 Healthy siblings also reported anger and resentment, and in some instances, these were often related to events happening within the family and directed towards their parents or healthy brothers or sisters and not directed towards their ill brother or sister. 20 However, on the flip side, it was directed towards their ill sibling with a rather opposing understanding of how the situation was indeed not their fault.29,36
The sadness was mostly implicit engendering a sense of helplessness, expressed especially when they addressed the suffering they perceived their ill sibling to be experiencing given the invasive treatment regimens and illness symptoms.33,34 Siblings also diminished their sense of self and affirmed a sense of guilt within themselves, replacing a sense of initial shock, fear and uncertainty following the diagnosis of the palliative condition, thereby feeling that they should have been the one with the palliative condition instead.33,37 Profound grief for past losses already endured was interestingly identified by healthy siblings, which was described to be further compounded by present struggles with the situation and an uncertain future. 38 Whilst the topic of death came more naturally to siblings of children with rare diseases in contrast to siblings of children with palliative care needs due to an accident as their worries were related to living with uncertainty and generally expressed feelings of guilt and self-blame. 20
Coping strategies (cognitive coping/distraction)
Healthy siblings pursued other sources of information due to curiosity stemming from parental silence intended as a form of containment of emotions and information from them. 34 This can be distinguished as intellectual or cognitive coping via seeking information and gaining knowledge on the ill sibling’s illness and medication thereby being able to recognise deterioration20,30,32,35 albeit several siblings obscuring this from their parent's awareness for fear of adding to the parental burden. 30 Behavioural coping strategies utilised by some healthy siblings either in solitary or by engaging in group activities included playing alone or turning to music and quiet or strenuous activities respectively. 32 Turning to faith, spending time with the ill child or completely stowing away their feelings were some coping strategies employed by healthy siblings to cope with their feelings and experiences. 38
Opportunities for growth
The circumstances, difficulties and changes experienced by the healthy siblings afforded growth opportunities.35,37 Healthy siblings alluded to positive growth outcomes including increased empathy for parents’ needs, cognitive understanding and respect for the ill sibling, enhanced self-concept, a sense of increased maturity, empathy and in some cases feelings of increased confidence in speaking up for themselves.35,37
Discussion
This qualitative systematic review explored and integrated the findings from 11 studies on healthy non-bereaved siblings’ perceptions of paediatric palliative care. The three broad themes synthesised from across studies highlighted the significant impact of a child’s illness on siblings’ lived experiences, feelings and coping abilities. Generally, our findings were similar to other reviews exploring siblings of children with specified diseases or illnesses such as those focussed on life-threatening conditions, 39 cancer exclusively,40,41 and included cancer as part of a variety of chronic illnesses rather than under the broader term of palliative conditions.10,42
Changing family dynamics has been noted to be prevalent among other reviews, which reported siblings experiencing significant disruption to their family’s routine, and perception of normality.39–41 The family routine was especially disturbed during increased active treatment phases or intensive periods, wherein the ill child had frequent hospitalisations. This led to healthy siblings being placed in the care of substitute caregivers such as neighbours or grandparents, which contributed to the further separation of healthy siblings from their families. Therefore, this leaves healthy siblings feeling invisible, isolated and lonely in unfamiliar environments.43–45 Given the importance of family relationships and communications in shaping the siblings’ experiences, it would be beneficial to encourage open communication and keep healthy siblings informed about the ill child’s status, and disease trajectory and involve them in the treatment regimen. This could also aid in strengthening family ties between the members as well as the siblings and is crucial in helping them understand the changes in the family structure and adapt to the new normal.15,46–51
The family systems health model emphasises the complex interactions between the illness, the ill child and the family. 52 It proposes that the different disease attributes, illness stages and treatment phases can pose varying psychosocial challenges. The model illustrates the increased family cohesion and closeness during the serious illness, which sequentially may galvanise healthy siblings to undertake increased caregiving responsibilities. 52 Healthy siblings may self-identify a duty in an attempt to maintain a close family unit and to ease the burden felt by their parents demonstrating how the subthemes are at interplay with each other.10,12,53,54 However, the chronic demands of caregiving roles may lead to conflict with school and other activities which may lead to an endless cycle of further loss of normal family routine and security and compromise child development.12,40,41,55 Hence, while siblings’ contribution to caregiving should be acknowledged and valued, they should be encouraged to widen their personal development. The potential ways to do so can be explored via professionals such as school counsellors or psychologists. 53
Findings from previous primary studies56,57 and a review 10 reported that higher rates of absenteeism and poorer concentration during classes translated to poorer academic outcomes among siblings of children with chronic illnesses when compared to the general population. However, this review highlighted contrary findings of positive academic achievements. This could be a reflection of how the ill child’s palliative condition can be a constructive experience for the siblings to learn to conceptualise and utilise their resources to cope with the experience as well as to gain acknowledgement and approval from their parents. 52 Healthy siblings also perform well academically as a form of coping mechanism. 14 Findings from this review in terms of socialisation identified varying levels of support from peers and teachers at school. Healthy siblings who received social support from peers at school have been reported by previous studies to have a higher quality of life scores and decreased levels of depression, anxiety or behaviour problems when compared to children who received less social support during their sibling’s illness.58,59 This review has highlighted how several siblings have limited time to spare to engage in social, and extracurricular activities and hobbies such as listening to music, and despite siblings being willing to sacrifice their social life to spend time with the ill child, most still hoped to participate in their social milieu. 30 Hence, perhaps blocking periods dedicated to activities outside of their families and school would greatly benefit the healthy siblings as these are typically encouraged as a form of distraction to cope with the illness experience and to maintain a sense of normalcy. 60
The community’s stigma towards palliative conditions was often approached with confusion by the healthy siblings and impacted them negatively as they felt unsupported and bullied. 30 Some healthy siblings in other studies have also demonstrated avoiding discussing the palliative conditions with their peers or at school due to the fear of not being understood or due to compartmentalisation of school and home.54,61,62 This is related to the other negative psychological impacts experienced by the healthy siblings as highlighted by the studies included in this review20,30–34,36–38 which was due to uncertainty about the illness trajectory and in feeling isolated in their illness experience. This was congruent with previous studies on siblings of cancer patients.63–67 Sibling support groups have been shown to enhance siblings’ psychological state, their knowledge of disabilities and their understanding of the family situation which would also help them feel less lonely in their experience. 68 This therefore steers towards engaging siblings wherein healthcare providers include healthy siblings in family discussions regarding the ill child’s illness trajectory. Previous reviews7,10 have also highlighted a potential ‘family-school-clinician’ partnership wherein there is a need for teachers to be educated and aware of the possible psychosocial presentations of siblings at school, signs of maladaptive coping and sibling experiences as well as to be more involved in intervening in any signs of harassment of the healthy siblings. This review identified that siblings cope with feelings of fear and uncertainty by employing the cognitive coping strategy, as substantiated by Lazarus and Folkman’s theory on coping. 69 This illustrates the healthy siblings’ problem-focussed approach to navigating through the changing situation imposed by the sick child’s illness by seeking information. This could be via medical pamphlets at the hospital and talking to healthcare professionals as emphasised in prior studies.45,70 The information learned offered healthy siblings a sense of self-control, which in turn helped siblings cope with uncertainty and has been shown to enable siblings to better manage other negative psychological impacts such as their anxiety.39,63 Engaging relevant supports, like child life specialists, early in the disease course who are well-positioned to help explain a complex situation in an age-appropriate manner and to develop strategies to cope with uncertainty may be useful in shifting to more family-centred care involving the siblings, thereby enabling them to adjust psychosocially. 10
This review’s findings highlighted that some siblings demonstrated increased maturity and empathy amidst other gains, which can be substantiated by literature, which describes positive psychological adjustments in siblings as they appear to demonstrate more resilience.40,53 This is further substantiated by previous research which also highlighted positive self-perception of their social functioning and self-esteem among siblings with ill children in their households when compared to the sex and aged-matched population controls. 71 However, this could also be attributed to the post-traumatic growth (PTG) phenomenon where positive change is observed due to the sibling’s experience of trauma and adversity. 72 Takedomi and colleagues 73 identified emotional support, emotion-focussed coping and problem-solving as factors that can influence posttraumatic growth in bereaved families of cancer patients. Those who interpret the situation in a positive light tend to have higher emotion-focussed learned coping skills and tend to experience reduced anxiety and have better emotional adjustment. Adequate palliative care has also been shown to improve family outcomes by improving their understanding of the palliative condition, and treatment trajectory as well as managing their fears and concerns. 74 Therefore, further research is needed to highlight factors specifically affecting the adjustment of healthy siblings to enhance the effectiveness of palliative care for them.
This review illustrated the multi-dimensionality and complexity of siblings’ experiences as well as how various relationships were concurrently a source of both support and strain. Another review conducted by Silva 75 focussing on palliative care provided to siblings of children with various serious illnesses has found significant room for improvement. Greater information, instrumental, appraisal and emotional support can be offered to these siblings. For instance, siblings can be provided a comprehensive description of the illness that the child is going through and the possible side effects of treatment. 75 This would enable siblings to adjust better to the changes that the patient would experience and be prepared for possible challenges or even grief. Furthermore, providing them with formal opportunities to accompany and discuss their feelings, such as adding this as a part of patient’s (sick child’s) health assessments/ physical checks and organising support groups where siblings can meet other siblings who may have similar experiences, may result in an improved adjustment to the illness experience as a whole and family life. 76 To improve early intervention and support for families of children with palliative conditions, clinicians should assess the psychosocial state of parents and healthy siblings. This would enable clinicians to help parents understand the need for siblings to feel supported throughout the illness trajectory. 39
Additionally, this review exclusively consolidated non-bereaved siblings’ perspectives as they confront different challenges than bereaved siblings and have an additional aspect of grief and loss that should be considered in understanding their perspectives.40,60 This allows a highly focussed and tailored approach to address the contemporaneous needs of the healthy siblings.
Strengths and what this study adds?
To the best of our knowledge, this is the first review of its kind that explored sibling’s perspectives of all palliative conditions as compared to prior reviews which only explored siblings’ perspectives of children with cancer or other highly specific diseases. This review also addressed a significant gap identified in prior reviews by focussing exclusively on non-bereaved siblings. Lastly, to consolidate all available data, all studies from as far back as the study from 1979 were included.
Limitations and future directions
Included articles majorly represented the Western population which might be reflective of a disparate set of healthcare systems reflecting different needs and cultures. Hence, future studies in varied geographical distributions representing the influence of cultural, spiritual and religious beliefs or traditions on siblings’ coping and adaption could be conducted to help inform future interventions. Two studies in the review included parents’ reports31,32 due to the siblings’ young age of between 6 and 11 years old. This may not accurately reflect the siblings’ perspectives as they are not obtained directly from the siblings themselves. However, these accounts are still valuable as they contributed to a more in-depth understanding of the experiences that siblings of younger ages go through. Triangulating the findings by exploring the roles of extended family members (e.g. grandparents), other caregivers and the community (e.g. support groups, religious or cultural communities) could also be considered in understanding a holistic view of the phenomenon of interest and in providing siblings with needed support. The studies with varied methodological qualities were included, which may limit the credibility of the findings. Additionally, given the highly evolving arena of disease management and qualitative research, some of these experiences may be outdated and using the same appraisal checklist to assess the quality of older studies may pose challenges. Therefore, reviews that explore the changes in paediatric palliative care over time and consider the evolving landscape of conducting qualitative research would be valuable in understanding the changing needs of siblings.
Conclusion
This review consolidated the available evidence around siblings’ varied experiences, which highlighted the multi-dimensionality of siblings’ perception of palliative care and could be considered as a starting framework for approaching and supporting healthy siblings of paediatric palliative patients. The findings of this review identified a shift in family dynamics, and social and psychological impacts as experienced by healthy siblings thereby emphasising the need of supporting siblings on a variable continuum which are tailored to the needs of these siblings along the trajectory of illness of their ill sibling.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231217597 – Supplemental material for Healthy siblings’ perspectives about paediatric palliative care: A qualitative systematic review and meta-synthesis
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231217597 for Healthy siblings’ perspectives about paediatric palliative care: A qualitative systematic review and meta-synthesis by Priyadharshni Rajendran, Gabija Jarasiunaite-Fedosejeva, Gözde Gökçe İsbir and Shefaly Shorey in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank the National University of Singapore Research Support Unit, for editing the language and format of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.