
Abstract
Background:
Telepalliative care is increasingly used in palliative care, but has yet to be examined from a patient and family perspective. A synthesis of evidence may provide knowledge on how to plan and provide telepalliative care that caters specifically to patients and families’ needs.
Objective:
To synthesise evidence on patients and families’ perspectives on telepalliative care.
Design:
A systematic integrative review (PROSPERO #CRD42022301206) reported in accordance with PRISMA 2020 guidelines. Inclusion criteria; primary peer-reviewed studies published 2011–2022, patient and family perspective, >18 years, telepalliative care and English/Danish language. Quality was appraised using the mixed-methods appraisal tool, version 2020. Guided by Toronto and Remington, data were extracted, thematically analysed and synthesised.
Data sources:
MEDLINE, EMBASE, PsycINFO and CINAHL were searched in March 2022 and updated in February 2023.
Results:
Forty-four studies were included. Analysis revealed five themes; the effect of the Covid-19 pandemic on telepalliative care, adding value for patients and families, synchronous and asynchronous telepalliative care, the integration of telepalliative care with other services and the tailoring and timing of telepalliative care.
Conclusion:
Enhanced access to care and convenience, as attributes of telepalliative care, are highly valued. Patients and families have varying needs during the illness trajectory that may be addressed by early integration of telepalliative care based on models of care that are flexible and combine synchronous and asynchronous solutions. Further research should examine telepalliative care in a post-pandemic context, use of models of care and identify meaningful outcome measures from patient and family perspectives for evaluation of telepalliative care.
The Covid-19 pandemic contributed to wider use of telepalliative care, especially in high income countries
Telepalliative care improves outcomes for patients and families.
A knowledge gap exists regarding a patient and family perspective on telepalliative care.
Patient and family acceptance is highly reliant on value-adding attributes
Patients and families’ experiences of telepalliative care during the Covid-19 pandemic vary substantially
Patients and families’ varying needs can be addressed using individually tailored telepalliative care.
Models of care and model workflows add structure and may enhance integration with other services
Outcome measures should build on patient and family experiences of value-adding attributes of telepalliative care
Patient and family representatives should be involved in the design of telepalliative care interventions.
Introduction
Telepalliative care involves the use of telehealth in palliative care, allowing patients and families to connect virtually with palliative care providers. 1 It has existed for over twenty years, largely in high-income countries (HIC).1,2 Telepalliative care can increase active family involvement in palliative care3,4 leading to increased comfort and peace of mind among patients and families. 4 Family, defined as those who the patient says they are, is not only restricted to relatives, but may include partners, friends and neighbours. 5 Serious illness in one family member can negatively affect other family members; socially, financially, emotionally and in relation to health and well-being.6,7 This necessitates a holistic and family focused approach to the patient and family as a unit of care, that aims to improve the health of the unit as a whole. 8 Similarly, best practice in telepalliative care aims to improve patient experiences and encourage family participation. 9 Therefore, developing an understanding of patients and families perspectives on telepalliative care is central to delivering family focussed telepalliative care.
A recent review (n = 40) on home-based telepalliative care highlights advantages such as the possibility for patients to remain at home, build interpersonal relationships with providers and self-report symptoms, but also disadvantages such as barriers related to inflexible symptom reporting tools. 10 While a comprehensive synthesis of patients’ use of telepalliative care in home-care is provided, little attention is paid to the role of family in telepalliative care. However, family remains the mainstay of the support network for patients with palliative care needs in the community, 11 and their role in telepalliative care cannot be underestimated. A recent meta-review (n = 16) noted that tailoring care to the preferences and capabilities of patients and families is an important facilitator in telepalliative care, 12 reinforcing family’s role. Likewise, a systematic review of randomised controlled trials (RCTs) (n = 30) found evidence of positive outcomes for patients and caregivers in telepalliative care interventions that target patients and families. 13 However, most interventions were patient-specific with a low number of interventions for patients and families (n = 5), arguing that greater family involvement in telepalliative care and support for family caregivers may benefit patients and their families, although research in family perspectives is limited. 13 These findings are echoed in a review of telepalliative care in nursing homes (n = 14), which found improved outcomes for nursing home residents, staff, and administrators; both residents and families reported positive experiences and families were positive in relation to quicker access to care, more frequent visits, and participation in video consultations. 14 Albeit, only two of the included studies represented a resident and family perspective, necessitating further research. 14 In summary, while previous reviews demonstrate positive outcomes and benefits when family are involved in telepalliative care, they also highlight a lack of evidence in this area. The proliferation of recent studies coupled with the importance of family involvement in telepalliative care warrants a review of the evidence to illustrate what matters most to patients and families in telepalliative care. Therefore, the objective of this integrative review is to synthesise evidence from studies that involve both patient and family perspectives on telepalliative care.
Methods
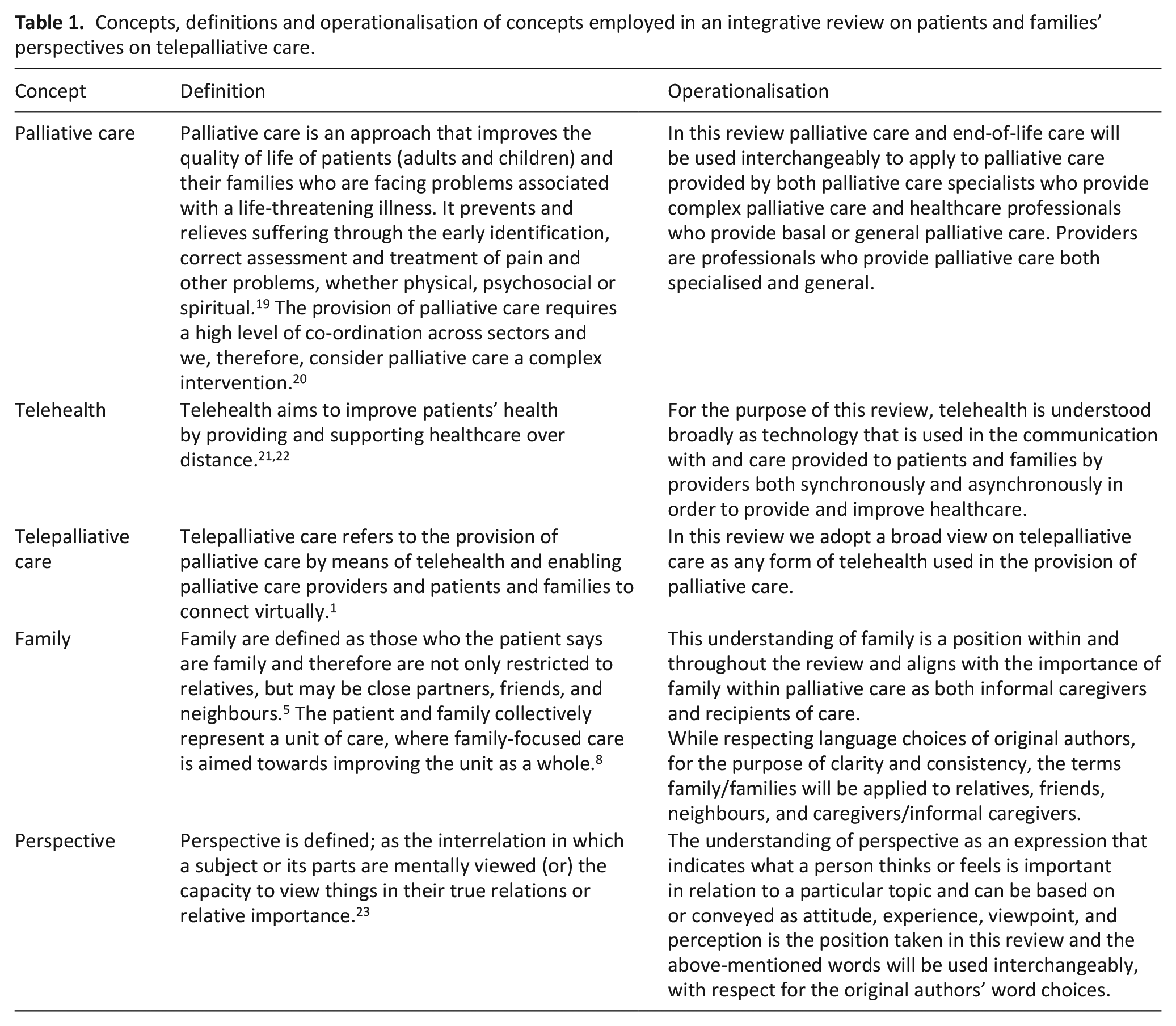
We performed an integrative review, in order to produce a new understanding of a narrow topic through a broad search and synthesis of available data guided by the methodology of Toronto and Remmington. 15 Searches and findings are reported according to the PRISMA2020 (Preferred Reporting Items for Systematic reviews and Meta-Analyses) statement. 16 The review was prospectively reported to PROSPERO 06.06.2022 #CRD42022301206. 17 Deviations from the published protocol 18 are accounted for (Supplemental Appendix 1). Concepts in this review are further defined and operationalised in Table 1.
Concepts, definitions and operationalisation of concepts employed in an integrative review on patients and families’ perspectives on telepalliative care.
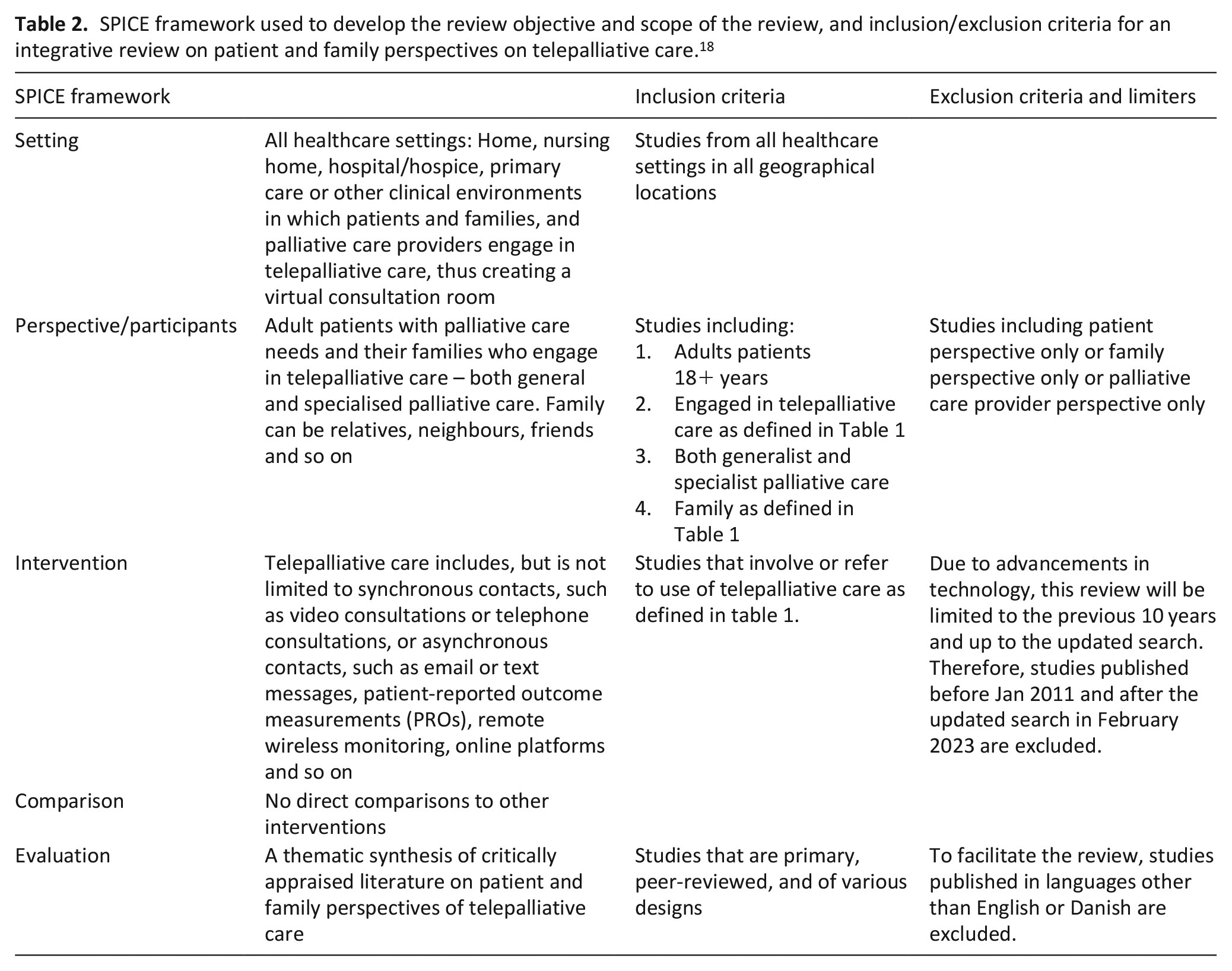
We applied the setting, perspective, intervention, comparison, and evaluation (SPICE) framework to the research objective to develop the scope of the review, aligned with the inclusion/exclusion criteria (Table 2). 24
SPICE framework used to develop the review objective and scope of the review, and inclusion/exclusion criteria for an integrative review on patient and family perspectives on telepalliative care. 18
Information sources and search strategy
We searched MEDLINE, EMBASE, PsycINFO and CINAHL in March 2022, updated in February 2023, and hand-searched reference lists of included studies and systematic reviews. A health librarian qualified search methods. Search strategies included; keywords (palliative care, telehealth, telepalliative care, family), synonyms, subject headings, search terms identified in existing search strategies, Boolean operators, database specific syntaxes and a validated filter for mobile applications 25 (Supplemental Appendix 2).
Selection process
We employed Covidence to manage screening, selection and data extraction, which was piloted, and performed independently by the first and second authors with adjudication from the last author.
Quality appraisal
To determine appropriateness and sufficient quality of sources, we employed the Mixed Methods Approval Tool (MMAT) version 2018 used to appraise qualitative, quantitative RCTs, quantitative non-RCTs, quantitative descriptive, and mixed-methods designs containing two general and five design-specific questions that can be answered with Yes, No or Can’t Tell. 26 MMAT is described in more detail in the review protocol. 18 The first and second authors agreed on relevant indicators, independently appraised 10 studies, aligned understanding of the appraisal process, appraised remaining studies independently, and achieved consensus through discussion. 26 The last author appraised one study involving the first and second authors 27 and adjudicated in the event of disagreement.
Data extraction
We extracted the following information; author, year, country of origin, aim, design, method, theoretical approach, setting, type of palliative care, diagnoses group, number of patients and families, family constellation, technology type, intervention, perspective and key findings. The first and second authors piloted data extraction, established agreement, completed extraction independently, and achieved consensus through discussion. This process of data reduction was performed prior to further data analysis. 28 The last author performed data extraction on one study involving the first and second authors 29 and adjudicated in the event of disagreement.
Data analysis
We integrated quantitative data into the data matrix convergently at the point of data extraction by ‘qualitising’ quantitative results, extracting and coding data using the vocabulary of the original authors, as recommended when combining quantitative and qualitative data to perform a qualitative synthesis. 29 We performed a step-by-step thematic analysis; deductively in relation to predefined elements of the data matrix during extraction and reduction, and inductively and iteratively across and within the data matrix (Figure 1). 30 Included studies are described according to predefined extraction headings and results of the data analysis are presented thematically. 4
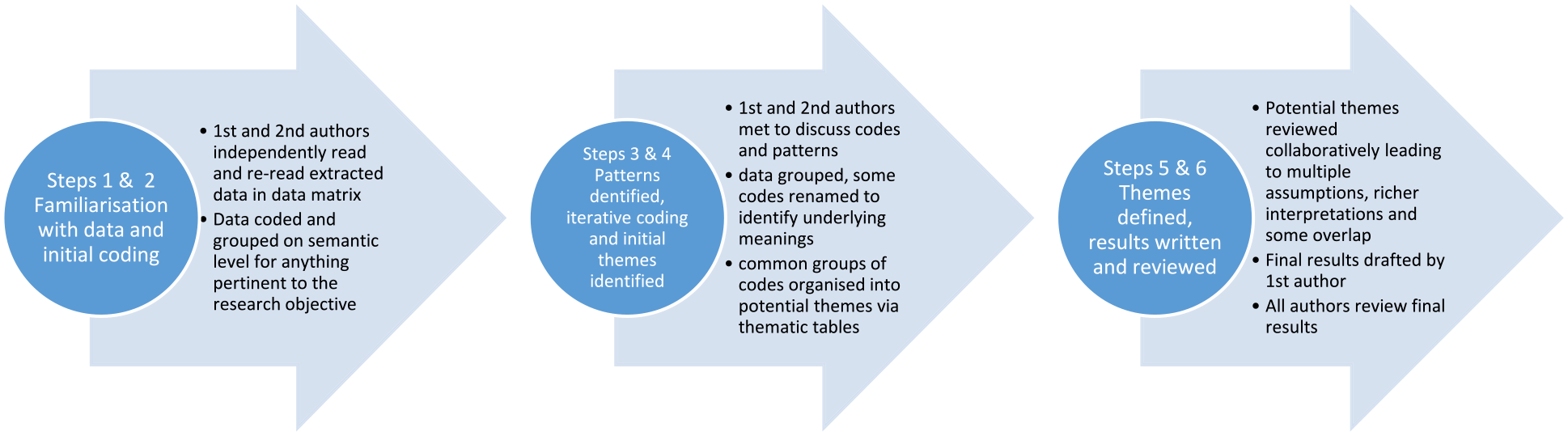
Steps followed in the thematic analysis of data extracted into a data matrix in a review of patients and families’ perspectives on telepalliative care.
Results
Results of selection process
Six thousand one hundred eighty-five records were identified in the database searches. Duplicates (n = 1848) were removed. Following title and abstract screening (n = 5297), 127 records were retrieved for full text screening. Forty-four studies were eligible for inclusion. Supplementary searching and updated searches rendered no further studies for inclusion. The outcome of the searches, screening, and selection processes are illustrated in a PRISMA flow diagram (Figure 2). 16
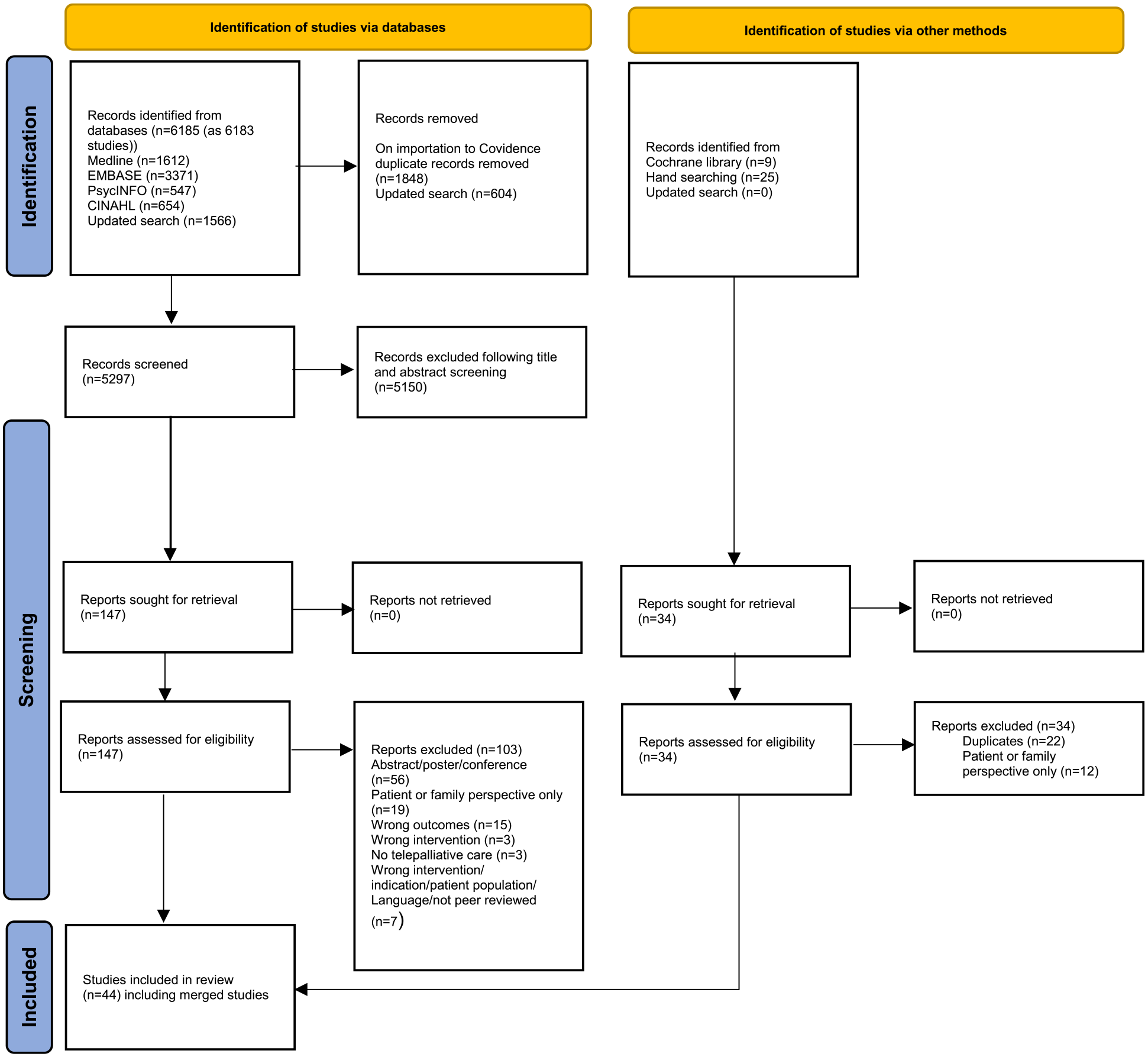
PRISMA 2020 flow diagram of studies included in an integrative review on patient and families’ perspectives on telepalliative care.
Results of quality appraisal
Quality appraisal scores ranged from 1* to 5*. All qualitative studies (n = 19) met the quality criteria with the majority (n = 16) scoring 5*. Quantitative studies (n = 5) comprised of randomised controlled design (n = 2), non-randomised controlled design (n = 1) and descriptive designs (n = 2) and ranged in score from 2* to 5*. Mixed-methods studies (n = 20) scored lowest ranging from 1* to 5* mainly due to lack of integration of quantitative and qualitative data results and lack of transparency of qualitative data collection and/or analysis methods employed. As recommended, no study was excluded following appraisal. 31 Low-scoring studies did not change the overall outcome (Supplemental File 1).
Description of included studies
The included studies (n = 44) comprised of 19 qualitative,3,4,27,32 –47 5 quantitative48 –52 and 20 mixed-methods studies,53 –74 spanning 18 countries in; North America,4,39 –41,46–48,50,53–56,58,59,61–63,65,66,68 –74 South America, 51 Europe,3,27,33–38,49,52,57,60 Africa,32,44 Asia45,67 and Australia. 64 The palliative care context was broad including; specialised palliative care in hospital and home settings (n = 19),3,27,41,42,45,49–55,58,59,61,63,66,67,74 general palliative care (n = 7),4,32,39,57,69,72 specialised and general palliative care (n = 12),33,35,36,38,43,44,46–48,62,64,70, peer support (n = 1), 37 early palliative care (n = 3)34,40,68 and Advance Care Planning (ACP) (n = 4).56,65,71,73 Patients’ diagnoses consisted mainly of cancer (n = 19),34,35,37 –39,42,44 –46,48–50,52,53,55,60,61,69,75 non-cancer (n = 8)40,41,43,56,65,68,72,73 and combinations of cancer and non-cancer diagnoses (n = 15).3,4,32,33,36,47,51,57–59,62,63,67,70,71 Family members, where specified, were mainly patients and spouses, but also patients and; adult children, siblings, parents, friends or neighbours or other family members.3,27,32,34,35,38,39,43,44,46–49,53–55,57 –59,61,64,67,68,71,73 Video consultations accounted for the most frequently used technology solution, alone (n = 11),35,36,43,46,51,62 –64,67,70,71 and in combination with other technologies; video consultations and telephone (n = 4),47,52,53,57 video consultations, websites and online forums (n = 3),38,58,59 video consultations, emails, applications (apps), and remote monitoring (n = 2),4,72 video consultations, telephone, apps, and/or e-mail (n = 2),3,69 and video consultations and apps (n = 1). 49 One study described use of various technologies to deliver palliative care; video consultations, telephone, website, online forums and social media forums, but not necessarily in combination with one another. 44 Telephone interventions were well represented, alone (n = 5)32,39,40,45,48 and in combination with other technologies. Several studies used websites alone (n = 7)34,42,56,60,61,65,73 and in combination with other technologies; website, e-mail, and online forum (n = 2)54,55 and website, online forum and social media forums (n = 1). 37 Apps used alone accounted for one study. 50 One study used remote monitoring alone. 74 Three studies pertained to perceived opinions and expectations to telepalliative care and therefore, technology was not categorised.27,33,41 Characteristics of included studies are available in Supplemental File 2.
Themes
Five themes are presented below and summarised in Table 3. Patients and families’ perspectives on the effect of the Covid-19 pandemic illustrate contextual issues related to telepalliative care. The four remaining themes illustrate patients and families’ perspectives on value-adding attributes of telepalliative care, how various technologies are employed in telepalliative care, the need for the integration of services and the importance of timing and tailoring telepalliative care to patients and families’ individual needs.
Themes, sub-themes, and summary of findings from an integrative review on patients and families’ perspectives on telepalliative care.
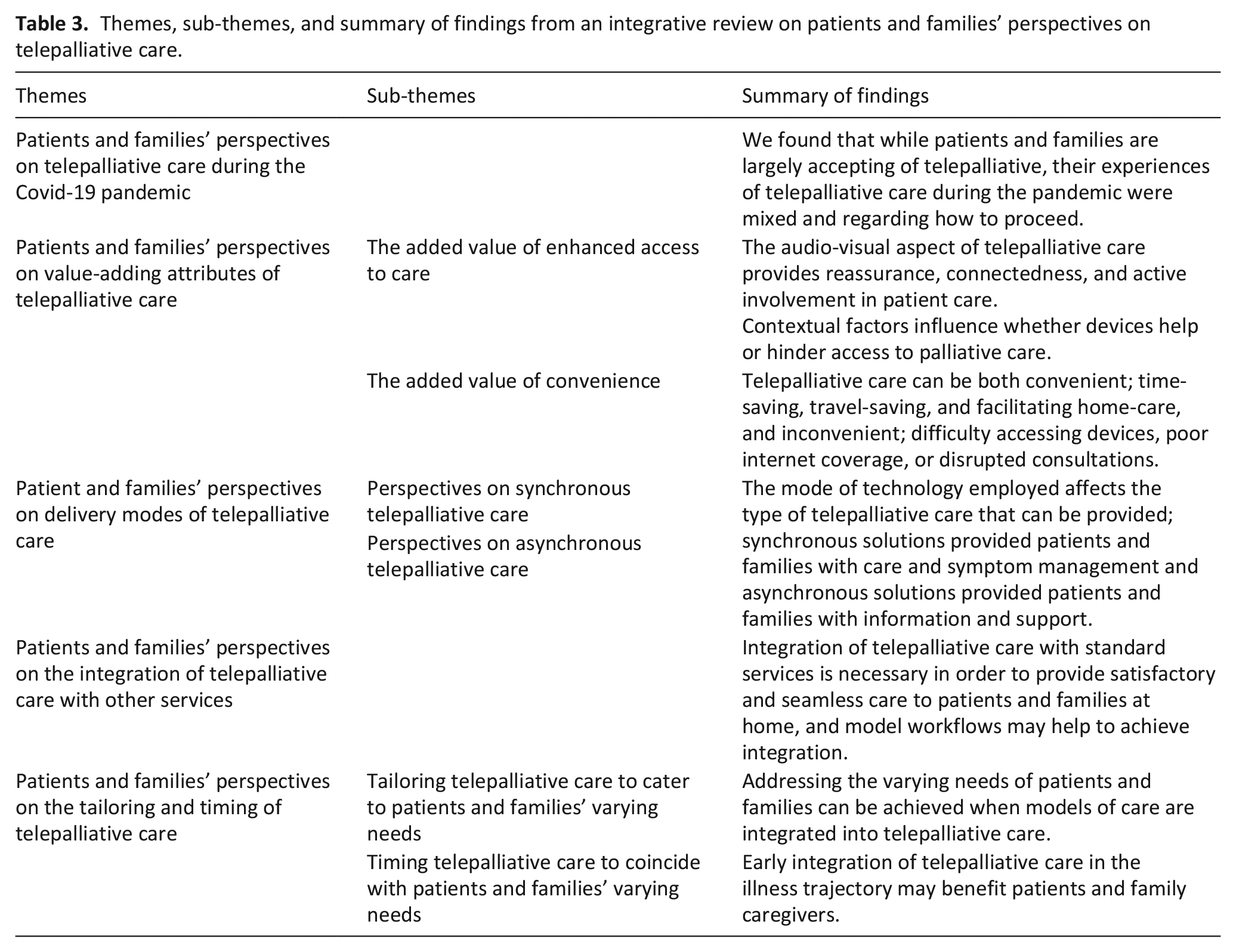
Patients and families’ perspectives on telepalliative care during the Covid-19 pandemic
Increased uptake and rapid adaption to telepalliative care is evident in the later studies in this review. Family conferences, 67 outpatient visits,43,52 community palliative care 47 and, hospital-centred spiritual and psychological care 51 were examples of telepalliative care during the Covid-19 pandemic. Common for all, was that telepalliative care was acceptable during the pandemic.43,47,51,52,67 However, when compared to face-to-face care, many considered telepalliative care as subpar and not a long-term solution.43,67 Reasons for this were unclear. Furthermore, technology in the context of isolating during the pandemic, was insufficient for providing social stimulation. 43 In contrast, some patients and families were highly satisfied with telepalliative care, would use it beyond the pandemic,51,52 agreed that it helped them to cope better with their illness, and would recommend it to others. 51 Others suggested a blended model in the future. 47
Patients and families’ perspectives on value-adding attributes of telepalliative care
Enhanced access to care and convenience were highly valued attributes of telepalliative care alongside added value in comparison to standard care, easy to use and not an added burden.33,38,41
The added value of enhanced access to care
Patients and families consider video-based telepalliative care in particular a major value-adding benefit.3,4,27,33,35 –37,40,44,53,57,62,63,70 The visual aspect led to pre-emptive symptom-management, which was highly valued by patients and families alike.3,35,70 While some found that the audio-visual aspect provided the opportunity to both see and hear anguish and distress,35,44,70 others preferred face-to-face contact to explain concerns or distress. 44 The visual aspect was explained as an exclusive digital connectedness possible only in the virtual context to provide information not otherwise available which, in turn, increased the value of the provided care.36,57,62 That said, some patients and families experienced difficulty building relationships, required technical help and real-time support. 63 Out-of-hours video consultation services, as an existing or potential service, were also highly valued.27,33,44,49,53 57 While some frequently used out-of-hours services for symptom management and psychological support,33,44,49 others did not, or seldom availed of them.44,53,57 Some patients and families were hesitant about disturbing providers 44 and other patients and families felt reassured through the availability of the service - its value lay simply in knowing that it existed. 57 Patients rely heavily on family to provide care and, therefore, enhancing access for families via telepalliative care in hospital and home settings is highly valued;41,53,62 families felt supported, actively involved, and updated in the care of patients.3,4,42,58,59,62,70 For in-patients and families, bedside access to hospital-provided technologies was highly valued for keeping in touch leading to enhanced-wellbeing.58,59 Contextual factors such as geographical location and income influence perceptions on the added value of enhanced access, as noted in studies from LMIC, where mobile phones enhanced and facilitated telepalliative care to support families.32,44 Initially, mobile phone usage in Africa, was hailed a low-cost method with the potential to deliver palliative care to people in poor communities. 32 By 2019, over half of Sub-Saharan Africans owned mobile phones. 44 Despite this, concerns over privacy, confidentiality, theft, power cuts, cost and lack of access to devices prevails. 44
The added value of convenience
Another value-adding benefit found is convenience35,39,40,48,52,63 expressed as accommodating personal presence over distance, facilitating family conferences, complex decision-making in the terminal phase3,35,48,62,64 and revealed as travelling- and time-saving36,52,62 and being in the comfort of one’s own home.36,46,63 Technological convenience may also explain why some preferred telephone-based telepalliative care, such as ENABLE telephone-based interventions,39,40,45,68 although, some patients and families were open to video/internet use.39,40 Some patients found video consultations too intense, 3 and fluctuations in one’s condition could dictate what the most convenient form of technology was.3,58,59 As illness progressed, stationary equipment presented a problem for patients; it was of limited use and reminded them of their approaching death, in contrast to portable and easy-to-use tablets.37,54 Despite possessing necessary technology and know-how, participation in telepalliative care services was not always convenient; difficulty accessing mobile phones during working hours, in public places or scheduling time away from work highlighted inconveniences.44,48 Inconvenience was also caused by interruptions to the virtual space; from uninvited persons, telephone calls accepted during consultations, 36 speaking over each other, many participants, 46 and unreliable internet coverage.36,51,57,64,70
Patients and families’ perspectives on delivery modes of telepalliative care
Perspectives on synchronous telepalliative care
Synchronous solutions, such as telephone or video consultations account for well over half of the solutions in this review. Several studies demonstrated how patients and families found it possible to develop relationships with providers in which they felt engaged.3,35,36,57,64 Entering a virtual room, which was neither in the hospital nor in the home, was referred to as ‘transcending institutional walls’. 36 Through digital connectedness, patients and families experienced empathetic relationships with specialists and were comfortable talking about sensitive topics.36,46,51,62 Providers’ abilities to develop close and trusting relationships with patients and families, was indicative of the success of video-based telepalliative care. 57 While some patients and families reported difficulty building relationships,52,63 others described that communication of sensitive topics was easier if there was a pre-existing relationship with a provider. 34 Video consultations carried the advantage of providing clearer communication due to the visual aspect,62,66 avoiding misunderstandings previously experienced in telephone consultations. 3 One of the biggest advantages of video consultations was the possibility for active family participation.3,4,35,36,41,66 As illness progressed, patients gradually participated less in video consultations.35,36 Technical concerns relating to screen size, portability of equipment, internet coverage and audio-visual quality existed,33,36,53,62,64,67 but were less evident in later studies. While video consultations were favourable, telephone interventions remained popular39,40,45,48 as a means of employing methods already available and familiar, thus avoiding over-burdening patients and families.3,41,48,57
Perspectives on asynchronous telepalliative care
Several studies explored asynchronous solutions, such as apps, websites, patient portal systems, social media platforms and online forums, which could be provider or non-provider led.33,34,37,38,42,50,54 –56,60,61,65,72 –74 Some patients and families felt well supported by traditional services, families and friends, whereas others availed of online communities to avoid burdening loved ones, or found traditional services unavailable. 37 Online forums and social media provided unique and alternative resources for people who wished to connect with others,33,38,44 or sought support in ‘navigating the cancer experience’. 37 While palliative care is less explicit, factual information and psychological and social support empowered patients and families in encounters with clinicians, navigating the healthcare system and accepting a new identity as a cancer patient.33,37,44 Provider-led websites for information-seeking and self-reporting were desired and plentiful, and covered psychological support interventions, factual information on cancer and treatment options, patient and family portal systems, symptom self-management or reporting apps and ACP websites.34,41,42,50,54–56,60,61,65,71–74 While some lacked flexibility due to restricted functions, or were useful but considered arduous and lacked technical support,34,42 others were found easy to use, empowering and helpful, provided several functions at once61,71,72,74 and strengthened patient-family relationships. 75 Websites that actively engaged older adults and families in ACP were beneficial despite challenges 65 Families could complete the tool at home with patients 56 and families experienced increased knowledge and self-efficacy. 65 Some found testimonials helpful and relatable where others found that encountering unexpected graphic illness-related content caused anguish, or was overwhelming.56,60,69,73 Provider-led websites offering professional support were well visited from within and outside USA; reading others’ posts was helpful but posting queries, and receiving qualified answers was extremely helpful, and several paid multiple visits.54,55 Queries pertained mainly to psychological and physical aspects.
Patients and families’ perspectives on the integration of telepalliative care with other services
As early as 2012, patients and families proposed that telehealth services should be designed to supplement, rather than replace, standard palliative care. 33 Lack of integration between specialised telepalliative care and community care caused frustration and confusion among patients, families and providers.53,57,69 Telepalliative care well integrated with standard care led to seamless transitions of care in the terminal phase.35,57 A study that demonstrated higher satisfaction and well-being among patients and families who received community-integrated specialised telepalliative care in comparison to those who received usual care, employed a model workflow 64 which may be key to successful integration of services. Early integration of telepalliative care into illness trajectories may also contribute to increased integration, 27 as reflected in recruitment strategies of patients recently referred or not previously palliative care patients. 64
Patients and families perspectives on tailoring and timing telepalliative care
Tailoring telepalliative care to cater to patients and families’ varying needs
While some needs are met through interventions targeting the family unit,66,67 others go unmet, leading some families to request individual consultations. 48 Reasons include the need to discuss sensitive topics that are uncomfortable discussing in joint sessions, to develop caregiving skills, and for scheduling convenience. 48 Dealing with anticipatory grief and bereavement are aspects that speak in favour of one-to-one sessions. 41 Patients, on the other hand, are concerned about the burden their illness places on the family, practically and financially, 45 and patients and families appreciate providers’ interests in family wellbeing.36,41 Telepalliative care interventions are shown to reduce anxiety, depression and caregiver burden in patients and families compared to standard care.48,49 Despite lower acceptance among older patients and those with low digital literacy,46,50,52 the health and wellbeing of the family unit can be addressed through individual and joint family consultations, 46 and with technical support, older patients and families with low digital literacy, are willing and able to participate in telepalliative care.41,46 One telepalliative care intervention that demonstrated high satisfaction was based on a model that incorporated shared decision-making (SDM) and the value, acknowledge, listen, understand and elicit (VALUE) approach into family conferences. 67 Prior to the conference, platforms and devices were chosen according to patients and families’ wishes. 67 A telehealth workflow provided structure, and SDM principles and the VALUE approach elicited preferences and helped achieve consensus on care goals. 67 Attention to individual needs in asynchronous telepalliative care requires broad, flexible designs that accommodate the needs of various groups. Examples of the same are the ACP websites designed for cognitively impaired adults and their families,65,71,73 or interventions that also cater for the hard of hearing and visually impaired.60,71 While studies showed that ACP websites are highly acceptable, families find themselves in dual roles as facilitators and participants, 65 and appreciate professional support. 71 Others websites tailor to specific disease groups.54,55 Common for these, are targeting the needs of specific populations. Personalising interventions takes tailoring a step further in providing meaningful telepalliative care, which was a desired feature for some patients and families.41,42,46 It is noteworthy that patients and families were particularly satisfied with solutions that successfully combined synchronous and asynchronous methods to deliver personalised telepalliative care.4,49,57,69 Confidence in the service increased use and thereto resulting benefits. 49 TapCloud designed for pain and symptom management of older rural palliative care populations and BOLSTER, designed for patients with gynaecologic-associated palliative care combined remote patient monitoring and video consultations tailored to patients’ specific conditions, symptoms and medications, and resulted in improved symptom burden and well-being among patients and families.4,69
Timing telepalliative care to coincide with patients and families’ varying needs
Patients and families had differing opinions on when it was appropriate to introduce telepalliative care; some perceived it less feasible as illness progressed, and others, that it started too late, or that they were too old or ill to acquire skills necessary for participating in telepalliative care.3,27 Support is particularly necessary at the time of diagnosis, progression of illness and towards the end of treatment. 34 Initially telepalliative care supports and empowers patients and families and, as illness progresses, it supports families in caring for patients. 53 Periodic reassessment can ensure that patients and families have adequate support to access interventions that are simple and flexible, using devices that match their preferences.34,39 Families preferred face-to-face consultations for first visits, receiving bad news, discussing ACP, and future expectations, whereas some patients preferred face-to-face consultations for receiving bad news, and others were comfortable having all visits via video. 63 Participants in early telepalliative care interventions, found them acceptable and very helpful for building caregiving skills, health literacy and reducing distress,39,40,36,46,48,68 but some recommend in-between session contact, flexibility in frequency and duration, incorporating ACP and starting earlier.40,45,46,68
Discussion
Summary of main findings
We found that while patients and families are largely accepting of telepalliative, their experiences of telepalliative care during the pandemic were mixed regarding how to proceed. Patients and families highly valued enhanced access to care via the audio-visual aspect of telepalliative care for providing reassurance, connectedness and active involvement of families in patient-care. They also valued the convenience of telepalliative care for time-saving, travel-saving, and facilitating homecare, but also, telepalliative care could lead to inconveniencies; difficulty accessing devices, poor internet coverage or disrupted consultations. In order to provide satisfactory and seamless care at home, integration of telepalliative care with standard services is necessary and early integration into the illness trajectory may benefit patients and families. Model workflows may help to achieve integration and models of telepalliative care may help to address the varying needs of patients and families. From a technology viewpoint, devices could help or hinder access to palliative care depending on the needs and context of patients and families. In addition, the mode of technology employed affects the type of telepalliative care that can be provided; care and symptom management via synchronous telepalliative care, information and support via asynchronous telepalliative care, or preferably, a mixture of both.
Discussion in relation to core elements of complex interventions
Given the complexity and number of components involved, telepalliative care interventions can be defined as complex interventions. 20 Few of the included studies describe use of recommendations for developing and evaluating complex interventions,40,44,68 despite recommendations for the same in palliative and end-of-life care research, 75 as supported by previous findings on patient perspectives on telepalliative home-care. 76 Therefore, the results are discussed in relation to; context, programme theory and stakeholders, which are core elements of the framework for developing and evaluating complex interventions, 20 as illustrated in Figure 3.
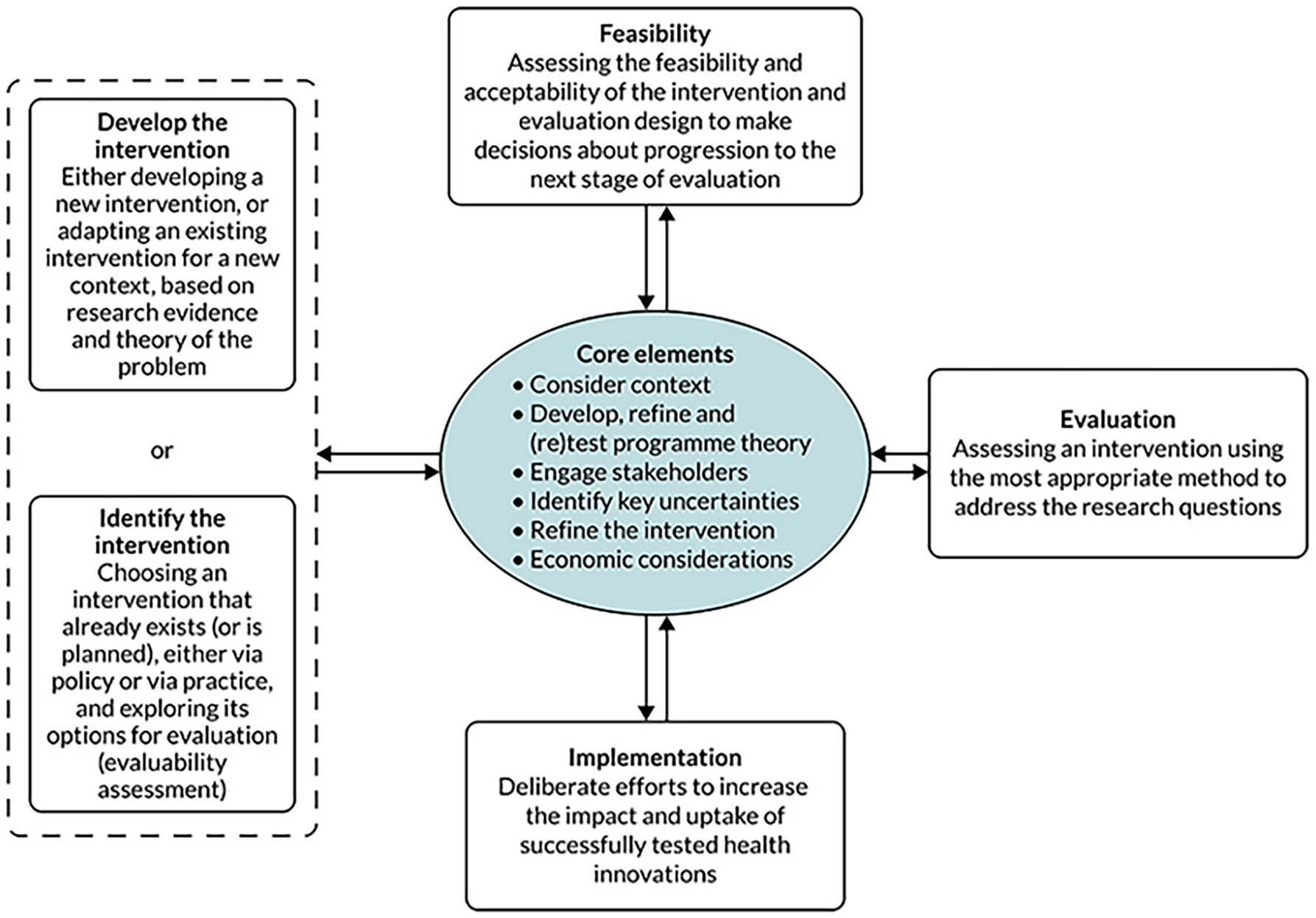
Main phases and core elements of complex intervention research. The diagram illustrates the non-linear, iterative pathway through the research process. The core elements should be repeatedly considered and may lead to further work at the same phase or movement to another phase. 20
Context
Evaluating how telepalliative care interventions interact with the context in which they are implemented can lead to greater focus on usefulness in real-world settings, in how they bring about change leading to desired or undesired outcomes, and transferability across contexts. 20 We found that depending on context, telepalliative care increased convenience such as time saving, comfort of home and technically simple solutions,35,36,48,63 or led to inconveniences such as difficulty scheduling or attending consultations, or interruptions during consultations.36,44,48 Thus, depending on context, telepalliative care could increase families’ role in patient care,3,41 or impede it. 44 As illustrated, possessing know-how and technology do not automatically equate with participation in telepalliative care interventions, as other contextual factors prohibited participation. Therefore, examining context iteratively in the context in which interventions are situated may ensure that patients and families receive necessary support and chosen devices match their needs, are clinically feasible, and fit into their everyday lives. Furthermore, key dimensions regarding context whether they are physical, social, cultural or financial need to be considered to ensure that responses brought about by the intervention are desired outcomes. 20 As demonstrated in the included studies, patients and families also found telepalliative care useful and acceptable during the Covid-19 pandemic.43,47,51,52,67 However, most would prefer face-to-face care in the future.43,47,67 Recent studies examining patients’ preferences for telehealth during the pandemic and the initial post-pandemic phase presented similar findings.77,78 Reasons for this are unclear. However, understanding that context can be multidimensional and dynamic 20 and considering the spatial context of Covid-19, where interventions were rolled out alongside sheltering-in-place directives and consequent social isolation, one could argue that some patients and families were negatively impacted by their context, while others were not. A recent study on telepsychiatry suggests that cumulative mental fatigue among providers from participation in video consultations may affect patients and families’ perspectives negatively. 79 In contrast, telepalliative care interventions can also increase efficiency, professional development and job satisfaction among professionals. 80 Nonetheless, acknowledging that technological mediation can place a mental strain on providers and affect their ability to build rapport with patients and families is a contextual factor worth addressing in future telepalliative care interventions. Furthermore, the financial context; whether or not participation in telehealth incurs a financial burden, may also affect patient and families’ preferences for telehealth in a post-pandemic context. 78 A review of exemplar telepalliative care projects draw attention to several contextual factors that could affect the sustainability of telepalliative care in the aftermath of the Covid-19 pandemic, where training, appropriate equipment, and physical environment are important aspects to consider alongside organisational aspects such as reimbursement issues and internet access. 81
Programme theory
Programme theory describes key components, mechanisms and features of an intervention and how, and under what conditions, the intervention will lead to desired outcomes. 20 We found that patient and family-centric models that are needs-based, anchored in the community and introduced early in the illness trajectory may increase the potential for improved integration of telepalliative care with other services.35,39,45,64,67 Furthermore, incorporating models of care into interventions that combine synchronous and asynchronous solutions may increase the possibility of providing tailored and personalised telepalliative care to patients and families.4,67 Ensuring that these features are included in the programme theory of telepalliative care interventions requires theorising policies, evidence, research, and the involvement of key stakeholders. 20 Programme theory can be further refined based on feasibility testing, as evident in the APNPC website.54,55 Regarding measuring desired outcomes, several included feasibility studies use predefined outcome measures and gathered data via validated questionnaires. While complying with recommendations in The MOREcare Statement on good practice in evaluating interventions in end-of-life care, 75 it is necessary to develop outcome measures that are psychometrically robust, but also clinically responsive. 82 Tools to report patient-reported experiences, though few, and family caregiver-reported experiences exist in palliative care. 83 However, suitable tools to report patient and family-reported experiences of telepalliative care have yet to be developed, 84 also highlighted in a recent systematic meta-review where evidence relating to physical and psychological symptoms and quality of life were either lacking or inconclusive. 85 While the current review indicates some value-adding attributes, there is a gap in relation to identifying attributes that can contribute to tool development to evaluate telepalliative care interventions in populations where fluctuations, progression of illness, and subsequent attrition are anticipated.
Stakeholders
Complex intervention research requires strong and early engagement with key stakeholders such as patients, practitioners, and policymakers. 20 While this review provides important perspectives on telepalliative care interventions from a patient and family perspective, it also raises questions such as: How to ensure that interventions add value to patients and families’ lives? What type of technology is appropriate to ensure desired outcomes and fit into patients and families lives? And how to tailor an intervention to patients and families’ specific needs? According to the guidelines for complex interventions, key stakeholder engagement should be targeted, but also broad and occur at each phase of the development of an intervention. 20 We found that while video consultations offer unique benefits to patients and families, not all can, or are willing to participate in video consultations, and telephones remain a familiar and useful method of communicating for some.3,39 Furthermore, we found that preferable options are multifunctional, flexible, and offer peer or provider support.4,57 Therefore, early engagement with patients and families to conceptualise and refine intervention requirements, in collaboration with stakeholder feedback throughout intervention development, may help to improve outcomes. 20 We also found that patients and families have varying needs for support and information; some prefer traditional healthcare services, while others choose to seek information and support among like-minded peer-led online communities or dedicated provider-led websites, and furthermore, needs change throughout the illness trajectory.34,37,54,55 While reiterating reasons for stakeholder engagement in developing complex interventions, this also highlights the importance of considering reasons for stakeholder priorities and awareness of conflicts of interest among stakeholders. 20 Patients and families appreciated dyadic sessions, but would also prefer some single sessions 48 indicating the necessity of taking varying needs into account and redesigning interventions, as illustrated in a recent ENABLE intervention adapted for patients with lung disease. 68 Furthermore, patients and families are particularly vulnerable at the time of diagnosis, fluctuations in symptoms, and towards the end of treatment, 34 illustrating the importance of being attuned to changing needs and involving patients and families as stakeholders in intervention design.
Strengths and limitations
Rigour and transparency in execution, represent the main strengths of this review. Methodological rigour was achieved by performing the review in accordance with the outlined methodology. 15 A health librarian qualified the search strategies which were piloted and refined, and searches were performed and updated in multiple databases. To identify further sources, supplementary searches were performed. Screening and data extraction were piloted and performed independently. Analytical rigour was achieved by following the steps of thematic analysis; 30 the first and second authors coded data independently, discussed categories and themes with the last author, and a finally with the whole research group. The data set is available in the data extraction table (Supplemental File 2). To increase transparency, the review was prospectively reported to PROSPERSO, and a review protocol was published.
Notwithstanding every effort to do so, language limitations may have restricted identification of articles not found in the employed databases, or searches in databases in languages other than the languages listed inclusion criteria. The majority of included studies originate from HIC, illustrating an underrepresentation of studies from LMIC, as previously seen.2,86
Conclusion
Our objective was to synthesise evidence on telepalliative care from patients and families’ perspectives. We found that enhanced access to care and convenience, as attributes of telepalliative care, are highly valued. Patients and families have varying needs during the illness trajectory which may be addressed by early integration of telepalliative care based on models of care that are flexible and combine synchronous and asynchronous solutions. Integration with community care services could lead to further satisfaction with telepalliative care and seamless transitions of care. Patients and families experiences of telepalliative care during the Covid-19 pandemic resulted in many preferring face-to-face palliative care in a post-pandemic context. Recommendations for future research are; an exploration of how expansion during the Covid-19 pandemic is shaping telepalliative care, an examination of the use of models of care in telepalliative care, and the identification of outcome measures building on meaningful patient and family experiences as measurements of acceptance and feasibility of telepalliative care interventions. Furthermore, future research should address disparities in telepalliative care in LMIC.
Supplemental Material
sj-docx-2-pmj-10.1177_02692163231217146 – Supplemental material for Patient and families’ perspectives on telepalliative care: A systematic integrative review
Supplemental material, sj-docx-2-pmj-10.1177_02692163231217146 for Patient and families’ perspectives on telepalliative care: A systematic integrative review by Eithne Hayes Bauer, Anders Nikolai Ørsted Schultz, Frans Brandt, Anthony C Smith, Georg Bollig and Karin Brochstedt Dieperink in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_02692163231217146 – Supplemental material for Patient and families’ perspectives on telepalliative care: A systematic integrative review
Supplemental material, sj-docx-3-pmj-10.1177_02692163231217146 for Patient and families’ perspectives on telepalliative care: A systematic integrative review by Eithne Hayes Bauer, Anders Nikolai Ørsted Schultz, Frans Brandt, Anthony C Smith, Georg Bollig and Karin Brochstedt Dieperink in Palliative Medicine
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231217146 – Supplemental material for Patient and families’ perspectives on telepalliative care: A systematic integrative review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231217146 for Patient and families’ perspectives on telepalliative care: A systematic integrative review by Eithne Hayes Bauer, Anders Nikolai Ørsted Schultz, Frans Brandt, Anthony C Smith, Georg Bollig and Karin Brochstedt Dieperink in Palliative Medicine
Footnotes
Acknowledgements
Caroline Moos, Research Assistant, Department of Clinical Research, Hospital of Southern Jutland, Institute for Regional Health Research, 6000, Aabenraa, assisted with the development of the search strategies and data management in Covidence. Herdis Foverskov, Librarian, University Library, University of Southern Denmark, 5230, Odense, assisted with the development of the search strategies. Kathryn Skivington, on behalf of Skivington et al., 2021, provided permission to reproduce ![]() , main phases and core elements of complex interventions research.
, main phases and core elements of complex interventions research.
Authorship
All authors made substantial contributions to the development and design of this review. The first author developed the search strategy and performed systematic database searches. The first and second authors performed title and abstract screening, full text screening, data extraction, and critical quality appraisal of retrieved studies. The last author was involved in full text screening, data extraction, and critical quality appraisal of retrieved studies. The first and second authors performed data analysis and all authors participated in reviewing data analysis and main findings. All authors contributed to the development of the manuscript and approved the final version for publication.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anders Nikolai Ørsted Schultz reports personal fees from OpenTeleHealth aps. The remaining authors declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author discloses receipt of financial support for the publication of this article from: Knud and Edith Eriksens’ Memorial Trust (Knud og Edith Eriksens Mindefond), grant number: 62786-2022.
Research ethics and patient consent
Ethical approval and patient consent are not required for this study. The research group have strived for transparency through reflexive and rigorous adherence to methodology in conducting and reporting this review with respect for original authors’ results and conclusions.
Data management and sharing
All data retrieved for this review are secondary data retrievable on the named databases. Search strategies, critical quality appraisal, and table of results are all accessible in supplementary files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.