
Abstract
Background:
Sexual and gender minorities experience considerable health disparities across the life span. End of life presents unique challenges for this population, further exacerbating existing disparities.
Aim:
We aimed to identify applied patient-level palliative care interventions for sexual and gender minorities and describe how said interventions met the needs of these populations at end of life.
Design:
We conducted a scoping review in keeping with the updated Arksey and O’Malley Framework. All included reports were analyzed qualitatively to describe the intervention and summarize thematically how it met the needs of sexual and gender minorities at end of life.
Data sources:
We conducted searches in MEDLINE, EMBASE, PsychInfo, and CINAHL from 1946 to June 10, 2023. Reports were eligible for inclusion if they described a palliative care intervention delivered to sexual and gender minorities, and if the palliative care intervention responded to at least one specific need of the sexual and gender minority population(s) in question.
Results:
We included and summarized 27 reports. We identified three overarching themes describing how palliative care interventions responded to the needs of sexual and gender minorities at end of life.
Conclusions:
This review responds to a need to improve palliative care delivery for sexual and gender minorities. Recommendations derived from these interventions, including how to center and advocate for sexual and gender minorities at end of life, can be applied by any interdisciplinary palliative care provider.
Keywords
Sexual and gender minorities experience significant health care disparities and have unique needs at end of life. These communities continue to have difficulty accessing high quality palliative care. Existing literature focuses on summarizing the end of life needs and experiences of sexual and gender minorities and making recommendations for providing palliative care to this population.
This study provides a summary of documented palliative care interventions that respond to the needs of sexual and gender minorities. A qualitative review highlights central themes across interventions including that they were often delivered or conceptualized by members of the very community they served, that sexual and gender minorities were centered rather than merely included in care, and that providers of these interventions behaved as advocates for sexual and gender minorities.
Palliative care policy makers and providers from any interdisciplinary background can leverage the qualitative descriptions of these interventions as a practical guide for how to design or redesign end of life care interventions and improve access to high quality palliative care for these communities.
Background
Sexual and gender minorities include individuals and communities encompassed under the umbrella terms queer and 2SLGBTQIA+, as well as the various communities within this acronym, such as two-spirit, lesbian, gay, bisexual, transgender, non-binary, intersex, asexual, aromantic, gender-nonconforming, pansexual, and more. For the purposes of this article and to be inclusive of those who may not feel represented by the 2SLGBTQIA+ acronym, we will refer to these communities as sexual and gender minorities.
It is now well established that sexual and gender minorities experience significant health disparities compared to their heterosexual cisgender counterparts, including greater prevalence of certain cancers and cardiovascular disease, disproportionate rates of mental illness and substance use disorders, as well as higher rates of unstable housing and fewer educational opportunities.1–8 Beyond the health disparities experienced throughout the life course, sexual and gender minorities also have unique vulnerabilities at end of life. Many sexual and gender minority adults are at higher risk of isolation and social precarity at end of life as a result of having been ostracized by families of origin or of choosing to withdraw from family rather than disclose their sexual orientation or gender identity. 9 Others feel alienated by families of origin with whom they remain close but who downplay the importance of their sexual or gender identity. Although sexual and gender minorities often establish chosen family within their communities, they are less likely to have children, and chosen family members may also be frail, unwell, and unable to serve as a healthcare proxy or provide caregiving support at end of life.10–12 This is especially true of sexual and gender minorities who survive a generation of peers who died either prior to the availability of highly active antiretroviral therapy for HIV, or since, due to lack of access. Furthermore, sexual and gender minorities may mistrust the medical system, which creates additional barriers to end-of-life planning conversations with healthcare professionals.10,13–15 Sexual and gender minorities also describe needing to “re-enter the closet” and sacrifice identity expression when seeking end-of-life care in cis-heteronormative palliative care environments. 16 Finally, spirituality and sexuality are often closely linked for sexual and gender minorities. While hospice and palliative care professionals are skilled in exploring the spiritual realm, they are less comfortable when discussing sexuality, which may limit opportunities for sexual and gender minorities to explore important parts of their identity at end of life. 17
Each of these vulnerabilities creates unique needs for sexual and gender minorities at end of life. When palliative care teams fail to recognize these unique needs they reduce this population’s access to high quality goal-concordant care. In a recent qualitative study by Valenti et al., 18 lesbian and bisexual older women whose spouses had died within the last 5 years reported avoidance of care planning discussions, a lack of knowledge about end-of-life care, and missing or unhelpful end-of-life conversations with clinicians. 18 With respect to appointment of a healthcare proxy, Dickson et al. 19 found that nearly 40% of older sexual and gender minority adults in the Southern United States do not have an appointed healthcare power attorney, and this was especially true of those who were more socially isolated, single, or who identify as transgender or gender non-binary. 19 Furthermore, when palliative care providers are uneducated about the unique needs of sexual and gender minorities at end-of-life or act on biased beliefs, their sexual and gender minority patients may experience discrimination. 20 In a study of sexual and gender minorities living in Zimbabwe, Hunt et al. 21 found that participants experienced difficulty accessing palliative care due to stigma amongst their communities and healthcare providers, ultimately leading to a lack of spiritual support and even painful and undignified deaths. 21
Several recent reviews have been published on the needs and preferences of as well as barriers faced by sexual and gender minorities at end of life.22–26 However, to our knowledge, there are no studies that review applied patient-level palliative care interventions for this population. Our study was designed to answer the question “what applied patient-level palliative care interventions for sexual and gender minorities have been described in the literature, and how do said interventions meet the needs of sexual and gender minorities at end of life?”. In asking this question, we sought to center the work of those who have served sexual and gender minorities at end of life, as well as highlight and learn from the ways in which palliative care has been designed and delivered to meet the needs of sexual and gender minorities. We therefore conducted a scoping review and qualitative content analysis of interventions described and provide recommendations for how palliative care providers can best care for sexual and gender minorities at end of life.
Methods
We conducted a scoping review with a qualitative content analysis to answer the research question “what applied patient-level palliative care interventions for sexual and gender minorities have been described in the literature. and how do said interventions meet the needs of sexual and gender minorities at end of life.” This scoping review adheres to the updated Arksey and O’Malley methodology for scoping reviews and we reported our findings in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)—Extension for Scoping Reviews.27,28
Search strategy
We designed our text word search and use of MeSH headings to reflect the diversity of sexual and gender minority communities (Table 1). To increase the sensitivity of our search we searched for reports pertaining palliative care or HIV/AIDS given the disproportionate impacts of the HIV/AIDS crisis on sexual and gender minority communities. Throughout its history, HIV/AIDS has been referred to by different terms, which were represented within our text words. With respect to palliative care, we included terms that are often used to describe the discipline including supportive care, end-of-life care, and death and dying, as well as environments where palliative care may be delivered, namely hospice. We did not include “intervention” as a concept given a lack of standardization in the definition of a healthcare intervention and in the interest of making our search as sensitive as possible.
Concept map for database search pertaining to patient-level palliative care interventions for sexual and gender minorities.
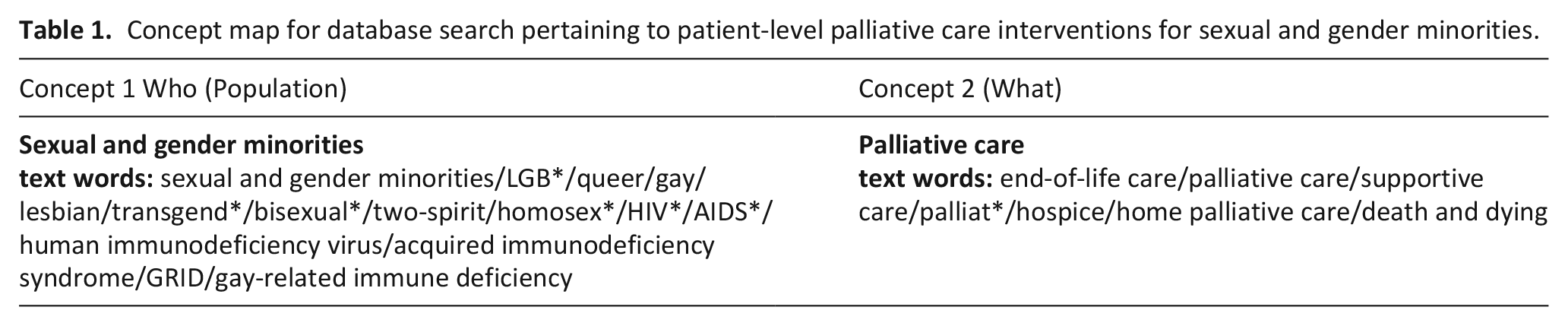
We searched four databases, including MEDLINE, EMBASE, PsychInfo, and CINAHL, on June 10, 2023, using a combination of MeSH headings and keywords. The primary author designed all search strategies with the help of a university librarian. We did not apply timeframe restrictions. Complete search strategies and results are included in the Supplementary Materials (Supplemental Table 1A-D). To enhance the literature review, we conducted a hand-search of studies cited within reports subject to full text review.
Eligibility criteria
Eligibility criteria were discussed prior to and iteratively throughout article review. We considered reports to be eligible for inclusion if they described an applied palliative care intervention for patient(s) of any age with any terminal illness; if the described palliative care intervention was delivered by any interdisciplinary team member(s); and if the intervention was described as addressing at least one unique need of one or more sexual and gender minority population(s). The authors did not predefine the unique needs of this population, rather needs were identified as any population-specific care requirement to which the intervention was intended to respond. These unique needs are detailed in the results section. Interventions carried out in any country were eligible for inclusion. Reports of any methodological type were eligible for inclusion so long as a full text was available. Reports were excluded if the target population did not include a sexual and gender minority patient or patient population, if there was no description of a patient-level palliative care intervention—including if there was a recommended intervention but no description of its application—if the applied patient-level palliative care intervention did not respond directly to at least one need of the sexual and gender minority population(s) receiving care, and if the reference was not an original publication, a full text work, or if it was not available in the English language.
Study selection
All citations were imported into Covidence. Both authors independently reviewed all citations by title and abstract. Citations for which the title was promising but there was no available abstract were included for full text review, and we subsequently excluded them if no full text could be located. Any disagreements regarding citations to include for full text review were discussed. Each author reviewed all full text reports independently to avoid bias. Decisions on full text reports were then compared. Any disagreements were discussed until both authors agreed. We considered citations “not retrieved” if no publication was found after searching the University of Toronto online Libraries, Google Scholar, and Google, as well as visiting the University of Toronto Gerstein Stacks, in three instances.
Analysis
For each of the included reports we extracted type, year, and country of publication, the patient population in question, where palliative care was delivered, the type of patient-level palliative care intervention described, and the methodologies used within each publication. Together, both authors reviewed all included reports to generate a concise description of each intervention. To thematically summarize the data and describe how the included interventions met the needs of sexual and gender minorities at end of life, we conducted a conventional qualitative content analysis of all included reports. 29 Content was open coded manually by each author, and a deductive codebook was created as each article was reviewed. Deductive open codes were compared to triangulate findings, and any divergence was discussed. Together both authors sorted open codes into sub-themes and then into overarching themes through an iterative process to ensure familiarity with the content.
Findings
Search results
We retrieved 13,472 citations from MEDLINE, EMBASE, PsychINFO, and CINAHL. A total of 8743 non-duplicate citations were screened by title and abstract, and 259 reports were sought for retrieval. Of these, 45 could not be retrieved. A total of 214 reports were included for full-text review. Reasons for exclusion and the number of reports excluded for each reason are found in the PRISMA flow diagram (Figure 1). We included a total of 27 reports for data extraction and content analysis (Table 2).30 –56
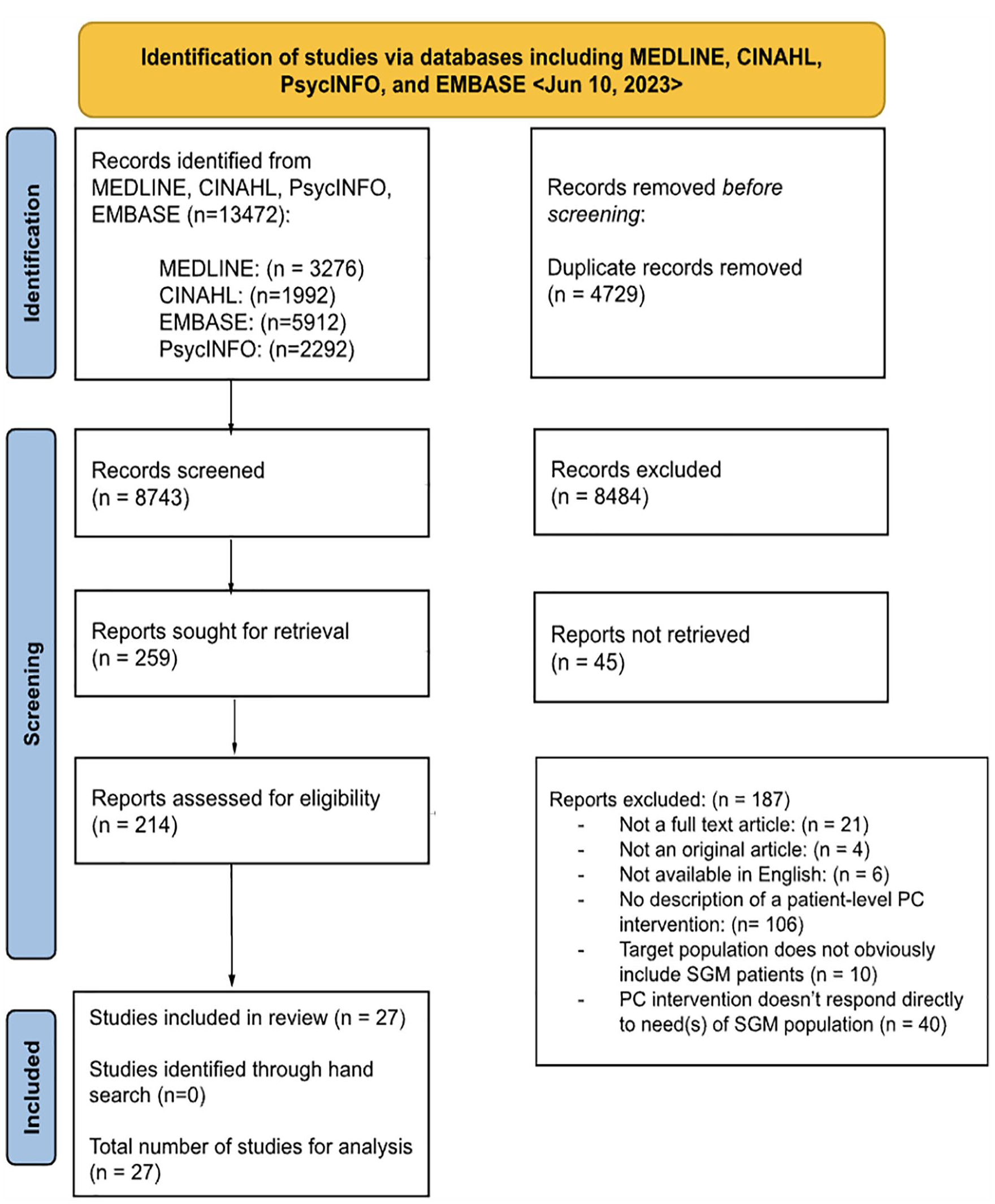
PRISMA flow diagram for scoping review of applied patient-level palliative care interventions for sexual and gender minorities.
Publication features and qualitative themes identified in 27 reports included in a scoping review of applied patient-level palliative care interventions designed to meet the needs of sexual and gender minorities.
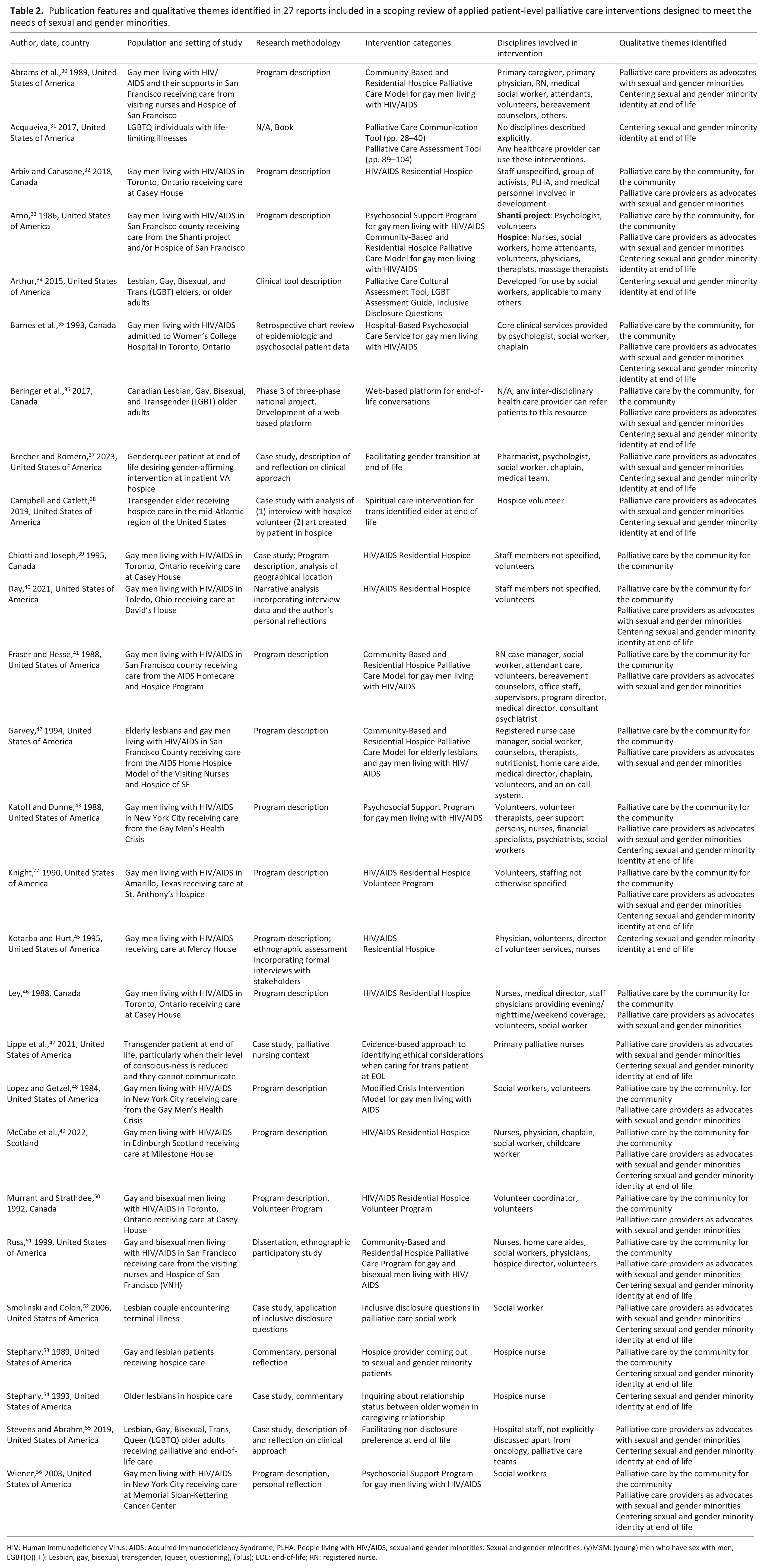
HIV: Human Immunodeficiency Virus; AIDS: Acquired Immunodeficiency Syndrome; PLHA: People living with HIV/AIDS; sexual and gender minorities: Sexual and gender minorities; (y)MSM: (young) men who have sex with men; LGBT(Q)(+): Lesbian, gay, bisexual, transgender, (queer, questioning), (plus); EOL: end-of-life; RN: registered nurse.
Study characteristics
Reports were published between the years of 1984 and 2023. Fifteen reports were published between the years of 1986 and 1999, representing reports released during the early years of the HIV/AIDS crisis. Twenty reports were written about palliative care interventions in the United States of America, six in Canada, and one in Scotland. Of the six Canadian reports, four pertained to a single residential hospice, Casey House, for people living with HIV/AIDS in Toronto, Ontario. Of reports written in the United States of America, five pertained to the AIDS Homecare and Hospice Program in San Francisco, California. Publication types included 23 journal articles, 2 books, 1 PhD dissertation, and 1 commentary. Few reports (n = 5) featured measurable outcomes with corresponding results (Supplemental Table 3).
With respect to the patient population of study, 16 of 27 reports pertained to gay and bisexual men; whether men were cis or transgender was not specified. Other target sexual and gender minority populations included exclusively transgender or gender nonconforming individuals (n = 3), lesbian, gay, bisexual, transgender, or queer individuals living with a terminal illness (n = 2), lesbian patients and their spouses (n = 2), and lesbian, gay, bisexual, transgender, or queer older adults (n = 4). All 27 reports addressed adult populations. With respect to the category of intervention, seven reports described a residential hospice palliative care program, five described a psychosocial support program for people living with HIV/AIDS, another five described an intervention consisting of both community-based and residential hospice palliative care delivery, two described volunteer programs, two describe the use of inclusive disclosure questions. The following were described in one report each: a web-based platform for LGBT adults to navigate end-of-life planning, a spiritual care intervention for a trans identified elder at end of life, an evidence-based approach to identifying ethical considerations when caring for transgender people at end of life, an example of coming out to one’s sexual and gender minority patients, a cultural assessment tool, an approach to facilitating non-disclosure preference at end-of-life, an example of facilitating gender-affirming intervention at end of life, and a palliative care assessment and communication tool for providers to use with LGBTQ adults. Some papers described more than one type of intervention, and therefore the total number of interventions listed (n = 30) exceeds the number of included reports.
In terms of the disciplines involved in delivering the described palliative care interventions to sexual and gender minorities, 12 reports described interdisciplinary teams, 5 reports described only volunteer service providers, 3 reports described an intervention delivered solely by social workers, 3 by palliative nurses, and a total of 4 reports did not describe the disciplines involved in the delivery of care. Across all 27 reports, a diverse array of disciplines were involved in the delivery of patient-level palliative care interventions to sexual and gender minorities (Table 2).
Thematic representation of sexual and gender minorities’ palliative care needs met by described interventions
All 27 reports were analyzed carefully by the authors, both of whom are queer-identified palliative care providers, to determine how the described interventions responded directly to the needs of the sexual and gender minority population(s) in question. We identified several emerging themes and subthemes that captured the overarching ways in which the included interventions responded to the needs of the sexual and gender minority population(s) to which they were providing care (Figure 2). A more detailed desc-riptive content analysis is available in Supplemental Table 2.
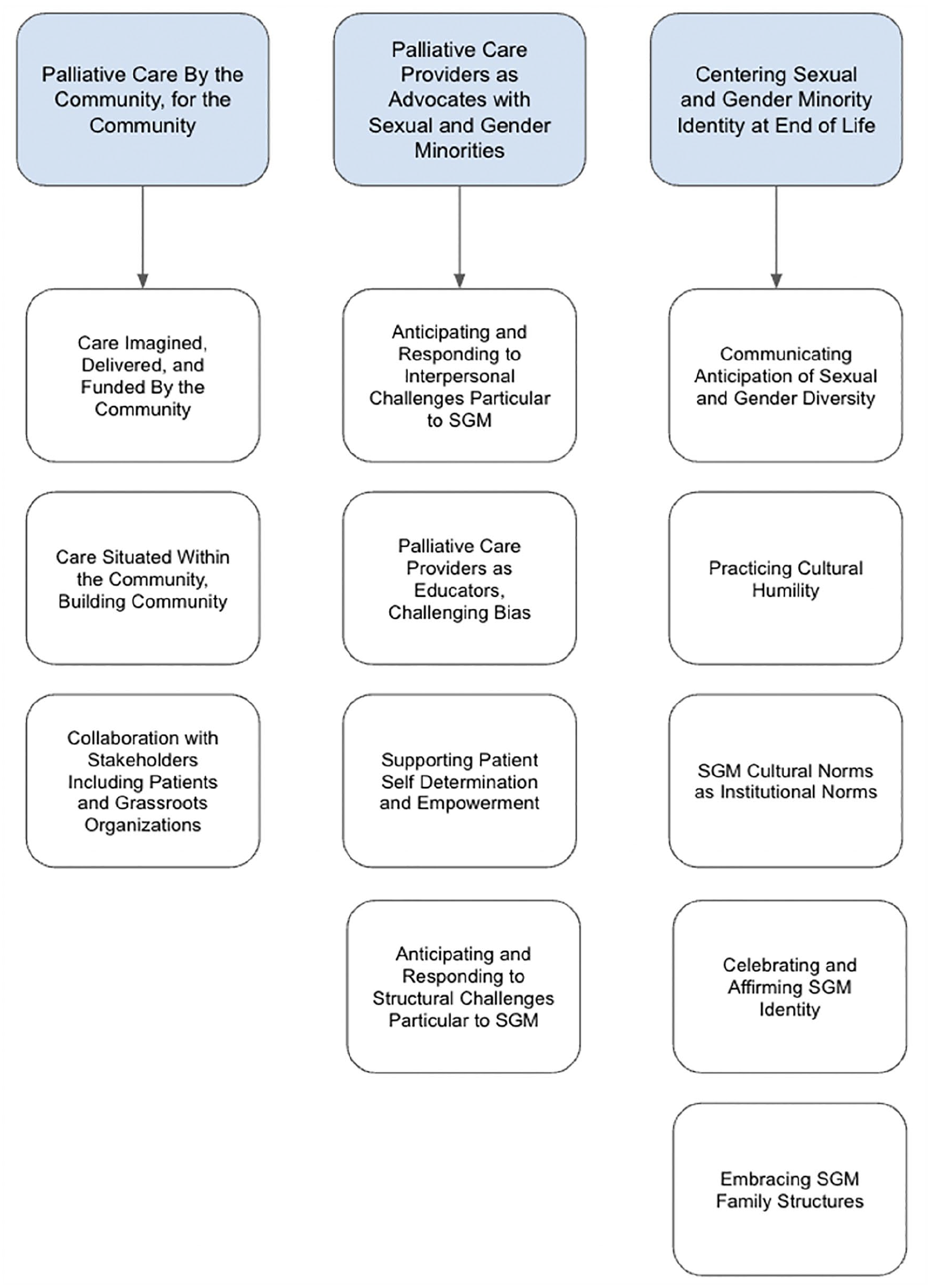
All 27 reports containing descriptions of patient-level palliative care interventions for sexual and gender minorities were subjected to a qualitative analysis. Reports were open coded by each author to identify the way that the needs of sexual and gender minorities were considered and/or met by each intervention. Open codes from all 27 reports were organized into subthemes and then into overarching themes to provide a qualitative description of how the palliative care interventions identified through this scoping review responded to the needs of sexual and gender minority populations at end of life. Three major themes were identified, including (1) palliative care by the community, for the community (2) palliative care providers as advocates with sexual and gender minorities, and (3) centering sexual and gender minority identity at end of life. Each theme had at least three subthemes, seen above in white boxes below each corresponding overarching theme.
Theme I: Palliative care by the community, for the community
Of the 27 reports, 17 made reference to being delivered by and for sexual and gender minority communities.32,33,35,36,39–44,46,48–51,53,56 We observed this in three key ways (Figure 2).
IA: Care imagined, delivered, and funded by the community
This observation was most applicable to hospice-based interventions for sexual and gender minorities living with HIV/AIDS. For instance, David’s House, an HIV/AIDS hospice in Toledo, Ohio, was a grassroots organization led by radical queers and activists, and they acquired funding through local drag shows, all of which was directed toward personal care and functional supports for hospice residents. 40 Day wrote about David’s House that it served as a model of citizenship based on “vulnerability, receptivity, and physical susceptibility” and therefore reflected queer organizing ethos. 40 Similarly, many hospice staff at Coming Home Hospice in San Francisco were themselves gay men, therefore creating a sense of community and safety; this was also true of the volunteer programs described, as many volunteers were drawn from the gay and lesbian communities in particular.33,39–41,43–45,48,50
IB: Care situated within the community, building community
Palliative care interventions described were often situated geographically within sexual and gender minority communities. Examples of this include Casey House, an HIV/AIDS hospice in Toronto, Canada, which was established mere blocks away from Toronto’s gay village; David’s House in Toledo where 12 gay bars were located at the time; and Coming Home Hospice in the Castro District, a predominantly gay male community in San Francisco.40,41,46,50,52 In their analysis, Chiotti and Joseph 39 suggest that by situating Casey House within the gay community, the hospice offered “a symbolic place which embodies the gay community’s defiance against AIDS and its empowerment to deal with an issue hitherto marginalized by the state.” Some palliative care interventions also facilitated new communities. For instance, a web-based platform for LGBT older adults seeking end-of-life resources included a forum and discussion board where terminally ill LGBT adults and their loved ones could share experiences and form connections. 36
IC: Collaboration with stakeholders including patients and grassroots organizations
A total of 14 palliative care interventions for sexual and gender minorities were developed in collaboration and/or consultation with stakeholders,32,33,35,36,39–44,46,48,49,51 including either patients themselves or grassroots organizations like Gay Men’s Health Crisis or AIDS Committee of Toronto.35,43,48 For instance, the aforementioned web-based platform for LGBT older adults was designed in consultation with anticipated sexual and gender minority users of the platform, 36 and the Hospice of San Francisco was developed in collaboration with the San Francisco AIDS Foundation, which was an all-volunteer grassroots organization composed mainly of gay community leaders and physicians. 33
Theme II: Palliative care providers as advocates with sexual and gender minorities
Within the included reports, we observed four ways that interdisciplinary palliative care providers and teams behaved as advocates with their sexual and gender minority patients at end of life (Figure 2).
IIA: Anticipating and responding to interpersonal challenges particular to sexual and gender minorities
A number of reports described an awareness of interpersonal issues that sexual and gender minority populations may face at end of life such as approaching death without traditional familial supports, a desire to reconcile with families, coming out to care providers, and the need to prepare for disability and death at a young age, especially for those dying of AIDS-related illness.35,36,41,43,44,48,50,51,56 Some interventions responded to these issues through implementation of peer volunteer presence and psychosocial support programs.36,43,44,48 In addition, at least two interventions recognized and responded to the unique experience of sexual and gender minority grieving as a collective and complex process in the context of mass deaths, predominantly of gay and bisexual men with AIDS, particularly prior to the availability of highly-active antiretroviral therapy.41,56
IIB: Anticipating and responding to structural challenges particular to sexual and gender minorities
End of life teams also anticipated and responded to systemic challenges particular to their sexual and gender minority patients. A case study by Lippe et al. 47 reflects on the systemic barriers encountered when providing care to a transgender person at end of life including anti-trans attitudes and violence within healthcare that affect both the transgender individual and their loved ones. In response, Lippe et al. 47 describe having applied a structured approach to anticipating ethical questions and reflecting on one’s biases in this circumstance. Lopez and Getzel highlight how the Gay Men’s Health Crisis responded to abuse, neglect, and prejudice encountered by gay men living with AIDS when accessing the healthcare system and social service organizations, and how they integrated advocacy into their service approach. 48
IIC: Supporting patient self-determination and empowerment
Care providers were also advocates when supporting the self-determination and empowerment of their sexual and gender minority patients at end of life. For instance, a volunteer-based intervention at St. Anthony’s Hospice in Amarillo, Texas was designed in response to an understanding of sexual and gender minorities’ spirituality as a key means of exercising self-determination. Volunteers worked with sexual and gender minority patients to facilitate artistic production and experiential transcendence in what Knight describes as a “mode of immortality” and a means for sexual and gender minorities to leave a legacy and grieve at end of life. 44
IID: Palliative care providers as educators challenging bias
Across the interventions we examined, it was common for palliative care providers to engage in formal or informal education both within and outside of their organizations to challenge bias and stigma directed against sexual and gender minority communities. For instance, Stevens and Abrahm 55 describe a case wherein they facilitated non-disclosure of their patient’s sex assigned at birth in order to uphold their expressed wishes regarding privacy at end of life. Informal education of hospital staff was key to sustaining this practice and was achieved through debriefing the ethical complexities of non-disclosure to highlight non-normative cultural priorities and the importance of ascertaining and upholding them for sexual and gender minority patients. 55
Theme III: Centering sexual and gender minority identity at end of life
As an alternative to providing inclusive care, health care teams can design and deliver care that centers a given population or set of populations with shared needs. Many of the included reports effectively centered sexual and gender minority patients and their identities in the design and delivery of end-of-life care. Palliative care teams and interdisciplinary providers practiced centering in five key ways (Figure 2).
IIIA: Communicating anticipation of sexual and gender diversity
Communicating anticipation of sexual and gender diversity was best exemplified by two interventions involving the use of inclusive disclosure questions.52,54 Smolinski and Colon 52 anticipated and welcomed lesbian identity at end of life by using an inclusive set of questions when inquiring about a patient’s relationship status with their same-sex companion. In doing so they modeled for other team members how to use verbal and non-verbal cues to express anticipation of and comfort with lesbian patients, rather than assuming cis-heteronormative identity. 52 Similarly, Stephany—herself a lesbian—used open-ended questions to understand the nature of a connection between two older women in caregiving relationship. 54 Stephany emphasizes the importance of recognizing generational differences in terminology, highlighting the impact of the institutionally sanctioned anti-lesbian violence of “the pre-Stonewall days” on the language used by older lesbians to describe their relationships in a healthcare context.
IIIB: Practicing cultural humility
Here, cultural humility refers to the ways in which palliative care providers sought to identify and intervene upon their own biases about sexual and gender minority communities, as well as appreciate and meet the diverse needs of their sexual and gender minority patients. Garvey describes how the AIDS Homecare and Hospice Model of the Visiting Nurses and Hospice of San Francisco delivered palliative care to elderly lesbians and gay men living with HIV/AIDS. They articulate the unique challenges faced by gay and lesbian seniors such as years of being closeted and concerns regarding stigmatization when accessing contemporary resources, but also highlight the strengths of elder gay and lesbian patients, such as high sexual health literacy and well-established self-help strategies. 42
IIIC: Sexual and gender minority cultural norms as institutional norms
Several palliative care interventions stood out for how their institutional practices reflected the cultural norms of their sexual and gender minority patients. These interventions included David’s House, Mercy House, Milestone House, and Coming Home Hospice—all residential hospice programs for gay and bisexual men living with HIV/AIDS—as well as the psychosocial support program at Memorial Sloan-Kettering Cancer Centre.40,45,49,51,56 These interventions adopted sexual and gender minority cultural norms through an emphasis on touch as an expression of spirituality and means of healing from the notion of being untouchable, the recognition of relationship as a critical part of healing and specifically the relationship between staff and patient as reciprocal and mutually beneficial, and the use of culturally relevant language and gender-vague pronouns by those being cared for and those providing care.45,51,56 As Kotarba writes about AIDS hospice, “this culture allows for the mixing and melding of medicine, alternative healing, gay politics, government funding, and spirituality, as well as the unprecedented expansion of nurse and patient autonomy.” 45
IIID–E: Celebrating and affirming sexual and gender minority identities; embracing sexual and gender minority family structures
Multiple interventions were notable for celebrating and affirming the various identities of their sexual and gender minority patients, and/or for embracing non-normative sexual and gender minority family structures. Campbell and Catlett describe a volunteer’s interaction with a transgender woman receiving hospice care; through the collaborative compilation of a multimedia book about her life experiences, this patient met a spiritual need for connection and personal expression at end of life that is often disallowed to trans people in healthcare settings. 38 Brecher and Romero 37 describe the case of a genderqueer veteran admitted to an inpatient VA hospice, who desired gender-affirming treatments in their final 6 months of life. Although hospice staff were initially unfamiliar with how best to support this patient, they educated themselves, helped the veteran access gender-affirming hormone treatment, and normalized gender-affirming expression such as applying nail polish and wearing feminine clothing. 37 Finally, Stephany provides an example of how sexual and gender minority palliative care providers can offer a distinct type of affirmation to their sexual and gender minority patients by coming out to them, and makes a strong argument for the importance of sexual and gender minority representation in palliative care environments. 5
Discussion
Main findings
We identified 27 reports published between the years of 1984 and 2023 describing applied palliative care interventions that respond to the needs of sexual and gender minorities living with a terminal illness. We qualitatively analyzed each report and identified three unifying themes including (1) palliative care by the community, for the community, (2) palliative care providers as advocates with sexual and gender minorities, and (3) centering sexual and gender minority identity at end of life.
What this article adds?
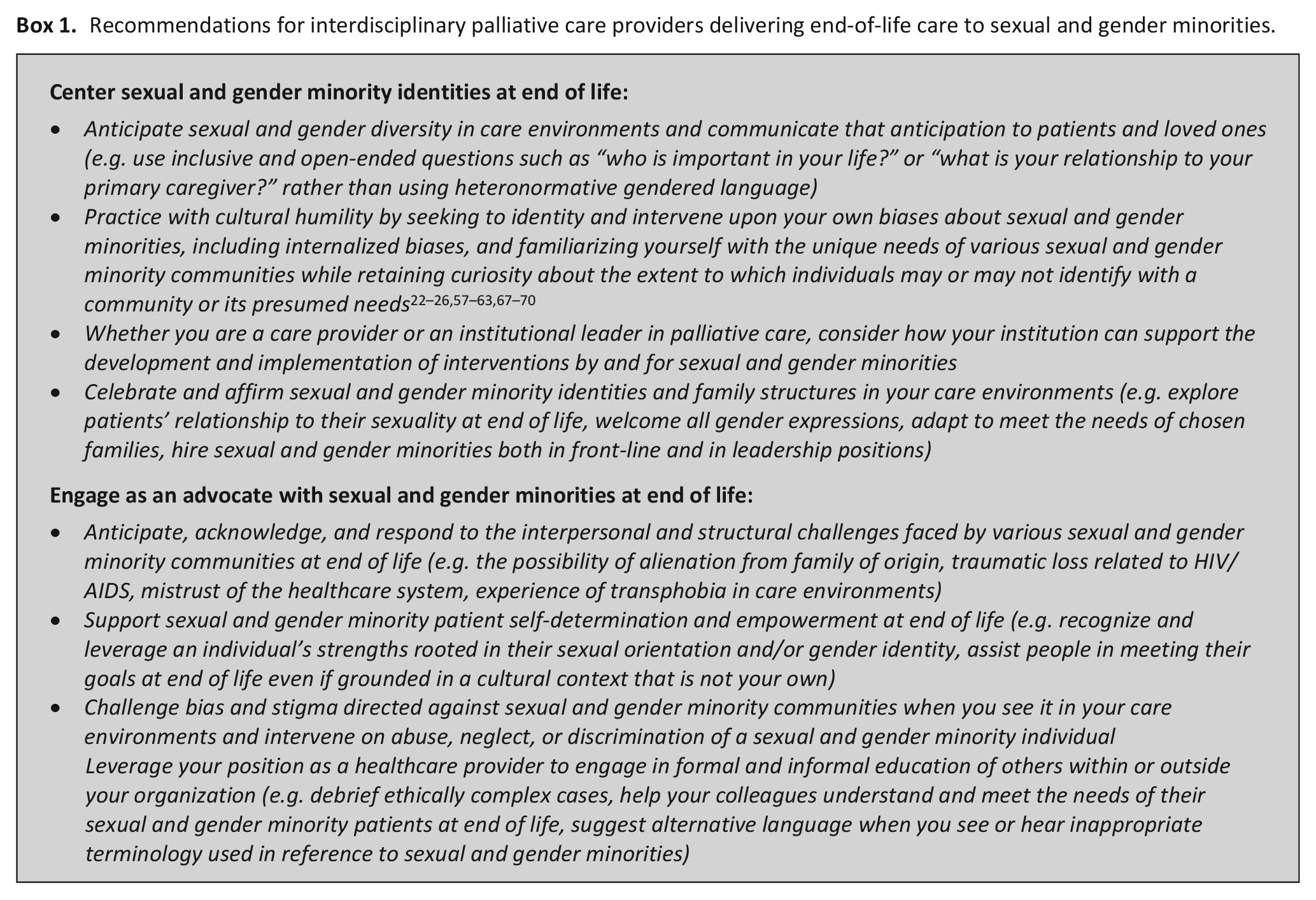
To our knowledge, this is the first scoping review of applied patient-level palliative care interventions for sexual and gender minorities, and the first study to provide a qualitative description of how applied palliative care interventions meet the needs of sexual and gender minority patients at end of life. Existing reviews pertaining to end-of-life care for sexual and gender minority populations summarize the needs of the community, 22 the experiences and preferences of sexual and gender minorities with serious illness,23,26 palliative and end-of-life care for sexual and gender minorities in the context of cancer, 24 and barriers to providing palliative care to members of this population with cancer. 25 In contrast, our review provides a summary of past and present real-life examples of end-of-life care interventions that meet the needs of sexual and gender minority populations. We also offer a set of recommendations grounded in our thematic findings, for how palliative care providers can better serve their sexual and gender minority patients (Box 1).
Recommendations for interdisciplinary palliative care providers delivering end-of-life care to sexual and gender minorities.
While there is a body of primary research on interventions designed to improve end-of-life care for sexual and gender minority populations, those interventions are largely targeted at the level of healthcare education rather than patient-level care.57,58 For example, Chidiac et al. 58 developed an education program for palliative care teams and were successful in increasing knowledge, confidence, and comfort with the unique issues and needs of sexual and gender minority patients in the palliative care setting. Others have recommended affirmative strategies including the collection of sexual or gender identity status at intake, demonstrating sensitivity, referring to culturally competent teams and community resources, creating a safe and inclusive environment by displaying markers of inclusion in clinical spaces, affirming relationships, and engaging in reflection to understand bias, however the implementation of these recommendations is not desc-ribed in the literature.59 –63
Many publications document the impact of the early HIV/AIDS crisis on the delivery of hospice services. These publications focus primarily on the challenges existing hospice organizations faced in accommodating a younger population with needs, lifestyles, and family structures that were previously uncommon in their institutions.64–66 In contrast, our review includes a subset of articles on this topic that describe interventions that went beyond accommodation and responded directly to the needs of sexual and gender minorities living with HIV/AIDS. About 16 of the 27 reports we analyzed described palliative care interventions for gay and bisexual men living with HIV/AIDS in the 1980s–1990s, of which 14 were notable for having been in some way delivered or conceptualized by members of sexual and gender minority communities. This subset of publications represents a proliferation of formalized end-of-life care interventions designed specifically for and by sexual and gender minorities. Interventions from this era, such as the various hospice programs we include, and the programs delivered by the Gay Men’s Health Crisis are born directly from the cultural needs and strengths of sexual and gender minorities. In both their number and qualitative richness, these articles illustrate that much of our understanding of how to provide end-of-life care to sexual and gender minority communities is grounded in the early work of those affected by HIV/AIDS.
Importantly, one of the central themes we identified in our qualitative analysis of the interventions included in this review was “centering sexual and gender minority identity at end of life.” Centering sexual and gender minorities in the provision of palliative care both recognizes that one’s sexual orientation and gender identity are important parts of their life and does not presume what role these identities may or may not play in their end-of-life care. To effectively center each sexual and gender minority patient with terminal illness, there must also be palliative care interventions that intentionally serve to meet the needs of transgender and gender nonconforming people, sexual and gender minority people of color, Indigenous sexual and gender minorities, and sexual and gender minorities with other intersecting identities. Although not all reports included in this review referred to the racial or gender identities of those they served, those that did described a predominantly White cisgender gay male community. This observation likely represents a failure to document the true diversity of sexual and gender minority populations receiving palliative care interventions and highlights a gap in the literature. Similarly, the literature included in this review is almost exclusively North American despite having not limited our search geographically, suggesting that palliative care interventions for sexual and gender minorities outside North America may be essentially undocumented in the academic literature. This limits our insights into how to meet the needs of sexual and gender minorities at end of life to the sociocultural contexts of North America. To this end, although there were qualitative commonalities across described palliative care interventions, it bears remembering that sexual and gender minorities belong to a diverse array of communities and sub-communities, each of which has their own set of individual needs based on their socioeconomic contexts, geopolitical contexts, and intersecting identities.
Limitations of this article
This scoping review was limited to a search of the extant literature and did not incorporate a survey of palliative care providers or organizations. We are cognizant of patient-level palliative care interventions for sexual and gender minorities whose applications are not represented in the literature and therefore were not included in the present review. One such example is the Canadian Virtual Hospice Two-Spirit and LGBTQ+ Proud, Prepared, and Protected online resource. 67 Similarly, we searched four large databases, however we may have included additional publications had we searched others. It is possible that some excluded palliative care interventions did consider and respond to the needs of sexual and gender minorities, but if this was not clearly described in the article it was assumed to be of minimal importance to the development of the intervention and was therefore excluded. For example, while most HIV/AIDS services likely provided care to gay and bisexual men, publications referencing these were excluded if they did not explicitly describe members of their patient population as sexual and gender minorities or did not specify how they developed and delivered their intervention(s) to meet these communities’ unique needs.
Finally, most reports in this review did not include outcome measurements or results. This scoping review therefore serves primarily as a description and qualitative analysis of included reports and does not provide information about the efficacy of most palliative care interventions described.
Implications for policy and future research
This review provides a list of examples and recommendations for how palliative care providers and policy makers might best provide end-of-life care to sexual and gender minorities. However, there still exists a paucity of literature describing end-of-life care interventions for this population, particularly outside of North America. This review also highlights a gap in evaluation, with few of the included publications including measured outcomes and corresponding results; this represents an area for further research. Furthermore, we have commented on the lack of literature pertaining to palliative care interventions for sexual and gender minorities who also belong to intersecting minoritized and racialized communities. There is therefore a need for further program description and evaluation in this area, and likely for enhanced program development.
Recommendations for care
In the absence of an abundance of literature on applied patient-level palliative care interventions for sexual and gender minorities, we encourage palliative care providers and policy makers to identify and reach out to local sexual and gender minority-focused programs and experts with specific questions about how they can serve their patient populations. Providers should also refer to existing reviews on the needs and preferences of sexual and gender minorities at end of life, as well as those providing recommendations and best practices.22 –26,57–63 We recommend accessing specific palliative care resources for sexual and gender minorities including the Canadian Virtual Hospice Two-Spirit and LGBTQ+ Proud, Prepared, and Protected online resource 67 and the National Health Service’s guide on achieving quality for lesbian, gay, bisexual, and transgender people at end of life. 68 For general resources pertaining to healthcare for sexual and gender minorities we recommend educational resources offered by the National Resource Centre on LGBTQ+ Aging and Health 69 and Rainbow Health Ontario, 70 as well as Caring for LGBTQ2S People: A Clinical Guide, Second Edition. 71
Based on our qualitative analysis and knowledge of the literature, the authors make the following practical recommendations, and we challenge palliative care providers from all disciplines to begin implementing these strategies in their practice (Box 1). These recommendations are rooted in qualitative data as well as the authors’ expert opinions, and therefore are not assigned a grade.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231214123 – Supplemental material for Applied patient-level palliative care interventions designed to meet the needs of sexual and gender minorities: A scoping review and qualitative content analysis of how to support sexual and gender minorities at end of life
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231214123 for Applied patient-level palliative care interventions designed to meet the needs of sexual and gender minorities: A scoping review and qualitative content analysis of how to support sexual and gender minorities at end of life by Lilian Robinson and Cam Matamoros in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163231214123 – Supplemental material for Applied patient-level palliative care interventions designed to meet the needs of sexual and gender minorities: A scoping review and qualitative content analysis of how to support sexual and gender minorities at end of life
Supplemental material, sj-pdf-2-pmj-10.1177_02692163231214123 for Applied patient-level palliative care interventions designed to meet the needs of sexual and gender minorities: A scoping review and qualitative content analysis of how to support sexual and gender minorities at end of life by Lilian Robinson and Cam Matamoros in Palliative Medicine
Footnotes
Author contributions
Both authors made a substantial contribution to the design of this work as well as the acquisition, analysis, and interpretation of data. All authors either drafted or critically revised this article, approved the version to be published, and have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Consent and data sharing
No patient data was used and therefore no consent was obtained. Data extracted from included reports is available in Table 2 and the ![]() . Most reports included in this review are available through academic institutional access. Please contact the corresponding author if a report(s) cannot be obtained.
. Most reports included in this review are available through academic institutional access. Please contact the corresponding author if a report(s) cannot be obtained.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Research Ethics Board approval was not required for this work.
Registration and protocol
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.