
Abstract
Background:
People with an advanced progressive illness and their caregivers frequently experience anxiety, uncertainty and anticipatory grief. Traditional approaches to address psychological concerns aim to modify dysfunctional thinking; however, this is limited in palliative care, as often concerns area valid and thought modification is unrealistic. Acceptance and Commitment Therapy is a mindfulness-based behavioural therapy aimed at promoting acceptance and valued living even in difficult circumstances. Evidence on its value in palliative care is emerging.
Aims:
To scope the evidence regarding Acceptance and Commitment Therapy for people with advanced progressive illness, their caregivers and staff involved in their care.
Design:
Systematic scoping review using four databases (Medline, PsychInfo, CINAHL and AMED), with relevant MeSH terms and keywords from January 1999 to May 2023.
Results:
1,373 papers were identified and 26 were eligible for inclusion. These involved people with advanced progressive illness (n = 14), informal caregivers (n = 4), palliative care staff (n = 3), bereaved carers (n = 3), and mixed groups (n = 2). Intervention studies (n = 15) showed that Acceptance and Commitment Therapy is acceptable and may have positive effects on anxiety, depression, distress, and sleep in palliative care populations. Observational studies (n = 11) revealed positive relationships between acceptance and adjustment to loss and physical function.
Conclusion:
Acceptance and Commitment Therapy is acceptable and feasible in palliative care, and may improve anxiety, depression, and distress. Full scale mixed-method evaluation studies are now needed to demonstrate effectiveness and cost-effectiveness amongst patients; while further intervention development and feasibility studies are warranted to explore its value for bereaved carers and staff.
Keywords
There is a rapidly growing evidence base for the use of Acceptance and Commitment Therapy in the management of psychiatric disorders, chronic conditions and stress.
Evidence on the use of Acceptance and Commitment Therapy for people with advanced cancer, concluded that it may be beneficial in improving psychological symptoms.
Acceptance and Commitment Therapy interventions are feasible and acceptable for people with advanced progressive illness; and may improve anxiety, depression, distress, sleep, and quality of life.
Evidence on Acceptance and Commitment Therapy for people with advanced progressive diseases other than cancer is lacking; and there are very few studies on its use or value for bereavement support.
Acceptance and Commitment Therapy has the potential to help manage psychological concerns in palliative care settings, though further evidence of effectiveness is warranted.
Training for palliative care staff in the principles of Acceptance and Commitment Therapy could increase access to evidence-based psychological support for people with advanced progressive illness.
Introduction
Palliative care is an approach that aims to improve the quality of life of people who are facing problems associated with advanced progressive illness, and their families. 1 Existential distress is frequently a concern for people with an advanced progressive illness, irrespective of culture or type of disease. 1 Anxiety, worry, uncertainty, loss of control and social role are common.2–5 Some people find it hard to engage in meaningful activities and relationships, may lose hope, and experience anticipatory grief .6,7 Regrets can occur where there is discrepancy between how people want things to happen and how they actually happen. These include regrets due to unfinished role responsibilities and broken relationships.4,6
Caregivers of people with an advanced progressive illness can also experience depression, anticipatory grief, loneliness, and a disturbance in their sense of meaning and purpose. 8 Increases in psychological symptoms such as anxiety and depression, as well as physical symptoms such as fatigue and pain due to their caregiver role is also common. 9 Up to 40% of caregivers are at moderate or high risk of prolonged grief disorder following bereavement. 10 Bereavement support needs increased during the COVID-19 pandemic, with many people reporting severe grief and difficulties accessing support.11,12 Evidence based interventions that help patients and caregivers recognise and manage psychological distress in the context of deteriorating health and bereavement are vital for high quality palliative care.4,13
Staff caring for people with an advanced progressive illness are at risk of stress, distress and burnout. This is partly due to the typical demands associated with working in healthcare such as unmanageable workloads and staff shortages, but also because of regular exposure to death, grief and loss.14–19 Over one-third of palliative care physicians met the criteria for burnout during the COVID-19 pandemic, further highlighting the need for interventions to support mental wellbeing amongst staff. 20
Acceptance and Commitment Therapy (ACT) is a form of Cognitive Behavioural Therapy that has its roots in radical behaviourism and emphasises how we respond to thoughts and feelings, rather than trying to alter the meaning of the situation as in traditional cognitive therapy. 21 It supports people to identify what is important to them, and to take action to enable them to live a life of meaning and value. 22 Instead of focussing on emotion regulation and symptom reduction, Acceptance and Commitment Therapy promotes acceptance of difficult thoughts and feelings, and acting in ways that are aligned with meaningful and valued living, even in the presence of difficult thoughts, feelings and circumstances. 23 This different focus gives Acceptance and Commitment Therapy a clear rationale and potential to improve wellbeing and quality of life of those impacted by advanced progressive illness, including caregivers and staff.
The Acceptance and Commitment Therapy model consists of six interdependent and overlapping processes. These processes are: (1) Acceptance – making space for challenging thoughts and emotions versus suppression or avoidance; (2) Defusion – stepping back from unhelpful thoughts and emotions to reduce their influence; (3) Contact with the present moment – maintaining flexible awareness of the present versus being overly influenced by concerns about the past or future); (4) Self as context – flexible perspective taking on our own self narratives versus being dominated by a rigidly held set of beliefs about who we are; (5) Values – identification of personal qualities and behaviours for a meaningful life versus dominance by expectations; (6) Committed Action – effective actions guided by values versus inaction or impulsivity. 24
There is a rapidly growing evidence base for the efficacy of Acceptance and Commitment Therapy in the treatment of a broad range of disorders and conditions, with recent systematic reviews describing its potential value for people with mood disorders, anxiety disorders, chronic illness, cancer survivorship, audiological problems, eating disorders, neurodevelopmental disorders, autism, sleep disorders as well as student wellbeing.25–36 Acceptance and Commitment Therapy can also be effective in improving general and work-related distress amongst health care professionals, 37 and for improving depression and quality of life amongst caregivers. 28 However, despite the emerging evidence base for the effectiveness of Acceptance and Commitment Therapy across a range of populations and contexts, we identified only three reviews focused specifically on advanced progressive illness or bereavement.38 –40 Two of these reviews concluded that Acceptance and Commitment Therapy may be beneficial in improving quality of life and alleviating symptoms of anxiety and distress amongst patients with advanced cancer38,39 However, both reviews excluded studies of people with advanced illnesses other than cancer, and considered evidence based on RCTs or quasi-experimental studies only. 38 Neither review sought to explore the potential value of Acceptance and Commitment Therapy for caregivers or staff involved in the care of people with advanced progressive illness. Consequently, given the emerging use of Acceptance and Commitment Therapy in palliative care 41 and its potential to improve outcomes for patients, caregivers and staff, we sought to determine the scope of the literature on Acceptance and Commitment Therapy for a broadly defined palliative care population. We were keen to report on all types of evidence that might address and inform clinical practice, explore how research has been conducted, identify characteristics related to delivering Acceptance and Commitment Therapy in this field, examine the outcomes that have been evaluated, impacts reported and identify evidence gaps.
Aim and research questions
Our aim was to map the evidence on Acceptance and Commitment Therapy for people with an advanced progressive illness, their caregivers (includes family members), and staff involved in their care. Specific research questions were:
What is the evidence for the feasibility, acceptability, and effectiveness of Acceptance and Commitment Therapy for people with a terminal or advanced progressive illness, their informal caregivers, including bereaved caregivers, and staff involved with their care?
How has Acceptance and Commitment Therapy has been delivered in palliative care settings (format, duration, mode of delivery, content, facilitation, barriers)?
What types of research designs have been undertaken and what outcomes have been measured?
Method
Design
A systematic scoping review was undertaken, guided by the Joanna Briggs Institute framework for scoping reviews. 42 This type of review allows diverse types of evidence to be mapped comprehensively to identify all evidence in an emerging field. 42 Scoping reviews are useful for examining broad areas to identify evidence gaps, clarify key concepts and report on evidence to address and inform progress in a topic area. The PRISMA-ScR guidelines were used to inform the reporting of the review. 43 The protocol was registered on the Open Science Framework registries: (https://osf.io/tpqax).
Eligibility criteria
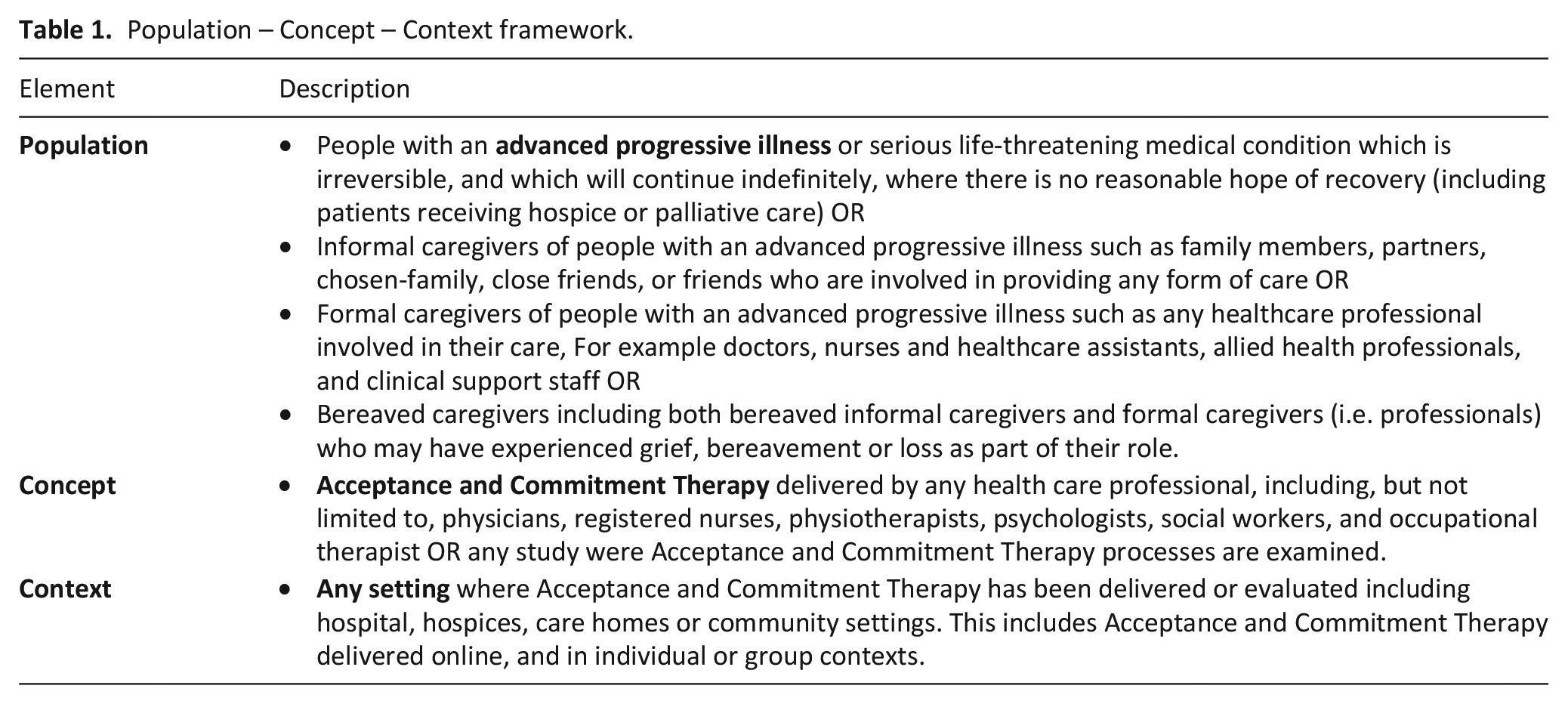
We included studies regarding the use of Acceptance and Commitment Therapy for people with an advanced progressive illness, their caregivers or staff involved in their care (Table 1).
Population – Concept – Context framework.
Types of sources
We considered empirical research studies published after 1999 (when Acceptance and Commitment Therapy was first described in detail). 23 This includes quantitative, qualitative, and mixed method studies; studies carried out in the English language. We excluded reviews, editorials, commentaries, case studies and dissertations below doctoral level; any studies which did not specify clearly whether a majority (>50%) of the population had an advanced progressive illness; any studies where the Acceptance and Commitment Therapy based intervention focused only on one component of Acceptance and Commitment Therapy (e.g. mindfulness); and any studies where Acceptance and Commitment Therapy was not a major component (<50%).
Search strategy
An electronic search was carried out in Ovid MEDLINE, PsychInfo, AMED and CINAHL covering the period of January 1999 to 12th May 2023.The search was undertaken using a combination of Medical Subject Headings (MeSH) and free text search terms for palliative care, Acceptance and Commitment Therapy and a range of terms for advanced progressive illnesses (See Supplemental File for Ovid MEDLINE search strategy). The terms used to retrieve the relevant papers were based on prior reviews and guidance from the research team’s expertise in psychological therapies and palliative care. The terms were adapted following pilot searches and varied slightly depending on the requirements of the database. ProQuest, ISRCTN and ICTRP registries were searched to identify further relevant papers. The reference lists of included papers and the reviews identified were hand-searched. Finally, all citations were exported to Endnote and duplicates were removed.
Data screening
Titles and abstracts were screened by one reviewer (TGW) and a sub-sample (25%) were independently reviewed by a second reviewer (AF) to check consistency as the searching progressed. Full texts were reviewed by one co-author (TGW) and a sub-sample (50%) were independently reviewed by a second (AF). Any queries were discussed by the full team to determine a definite list of studies.
Data extraction
Data were extracted by one reviewer (TGW) using a data extraction protocol developed for the purpose of the study. 44 A second reviewer (AF) reviewed a sub-sample (five papers) to help to ensure the accuracy and congruency in the data extraction process. The extracted data was tabulated on an Excel spreadsheet according to the following: author(s), title, author(s) origin, year of publication, journal, study type, population, setting, methodology, intervention format, healthcare professional level and outcomes. Any uncertainty with data categorisation was reviewed by all co-authors. Due to the wide range of study methodologies and heterogeneous nature of data, and in keeping with the aims of a scoping review, quality appraisal was not carried out. 42
Data analysis and synthesis
Based on our interest in scoping evidence on Acceptance and Commitment Therapy relevant to patients, caregivers and staff, we decided on a broadly deductive approach in order to map evidence for these groups. However, during the review process, it became clear that evidence could be usefully categorised as pertaining to interventions using Acceptance and Commitment Therapy; or observation studies describing relationships between Acceptance and Commitment Therapy components and outcomes commonly assessed in palliative care. Consequently, we decided to separately report intervention and observational studies. Consequently. For intervention studies we reported data on key characteristics such as setting, mode of intervention delivery, intervention format, outcomes assessed, enrolment and retention rates as well as findings. For observational studies we reported data on study aim, methods, outcomes and key findings. To support integration, quantitative data were tabulated and analysed descriptively in MS Excel. All studies were imported into NVivo so any qualitative data could be analysed and synthesised descriptively guided by the review aims (e.g. evidence on intervention acceptability).
Results
Study selection
A total of 17,638 records were identified from the electronic searches of databases, registries and hand searching reference lists. Duplicates were removed using Endnote resulting in 1,373 citations, a further 1,271 irrelevant records were excluded after screening. A total of 102 articles were selected for full text review. Overall, 26 studies were included (See Figure 1).
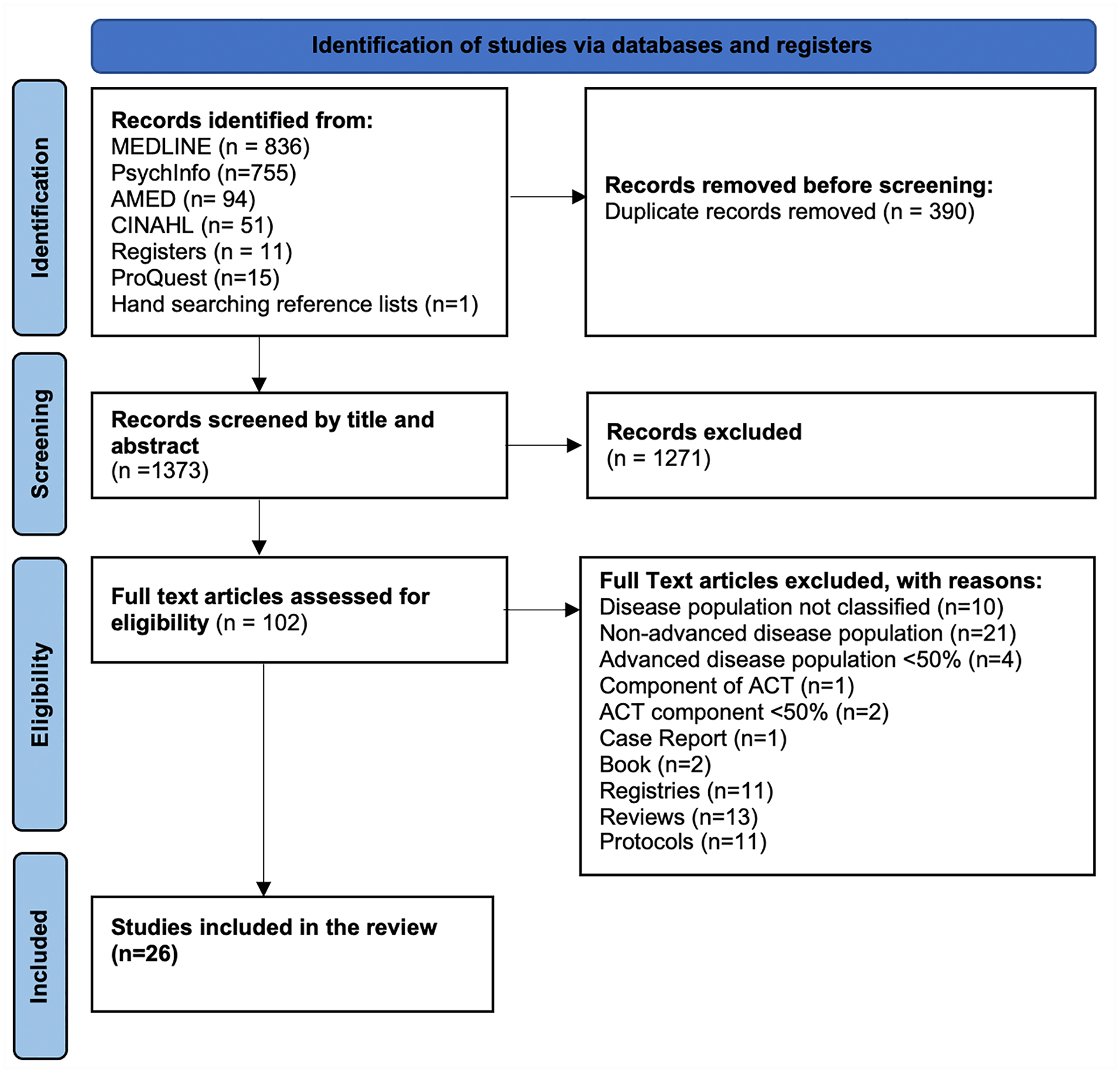
PRISMA flow chart highlighting the search strategy.
Overview of studies
Nearly half of the 26 studies included were conducted in the USA (n = 11; 42%),45 –55 around a quarter in the UK (n = 6; 23%)56 –61 and a quarter in Australia (n = 6; 23%).62 –67 Articles identified were published from 2012 to 2023 (see Supplemental File: Figure 1). The publication rate accelerated during that time, with the highest number being published in 2020 (n = 5). Of the 26 papers included, 15 were interventions studies16,46,48,49,52 –55,57,60–63,66,68 while 11 were observational studies (eight quantitative, two qualitative and one mixed) (see Supplemental File: Figure 3).45,47,50,51,56,58,59,64,65,67,69 Intervention papers included randomised controlled trials (n = 3; 20%),54,63,66 pilot randomised controlled trials (n = 5; 33%),48,49,53,55,60 single-arm intervention pilot trials (n = 6; 40%)16,46,52,57,61,62 and qualitative intervention studies (n = 1; 6%). 68
Study populations
The majority of articles examined Acceptance and Commitment Therapy for patients (n = 15; 58%).16,47 –50,52 –54,57,58,60,65,67,69 Of these, 10 papers were focused on people with advanced cancer.16,47,49,50,52 –54,57,58,60 Four were focused on Acceptance and Commitment Therapy for families or caregivers62,63,66,68, two a mix of both patients and caregivers.48,55 Three were focused on staff45,56,61 and a further three involved people who had been bereaved.46,51,64 One study involved a mix of both staff and bereaved caregivers. 59 See Supplemental File: Figure 4.
Intervention studies
Fifteen papers evaluated an intervention.16,46,48,49,52 –55,57,60–63,66,68 Details of the interventions can be found in Tables 2 to 4. Of these, seven involved patients16,49,52–54,57,60; four involved caregivers 62,63,66,68; two involved patients and carers 48,55; one involved bereaved and staff 46 and one staff. 61
Details of intervention studies (N = 15 papers).
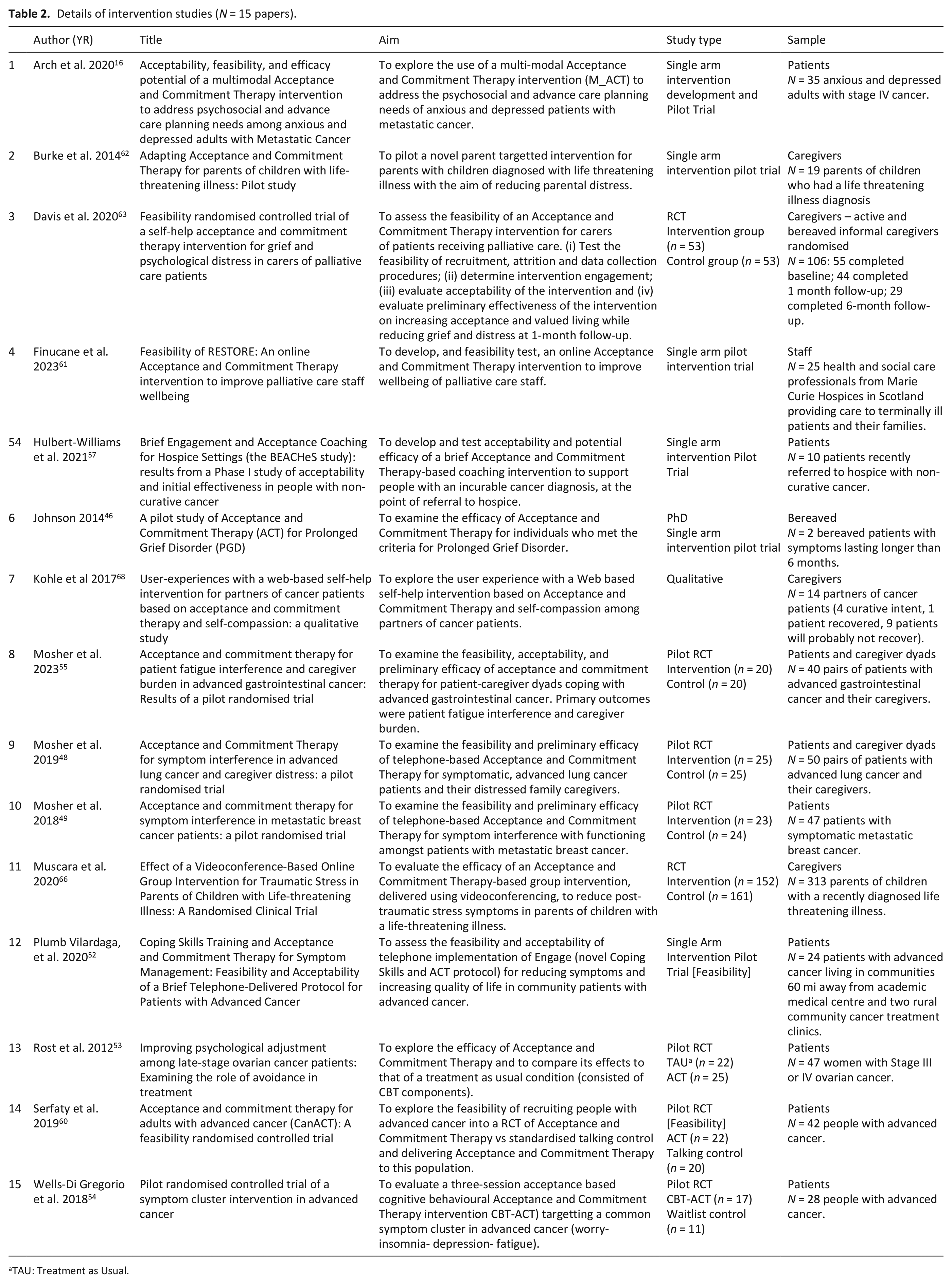
TAU: Treatment as Usual.
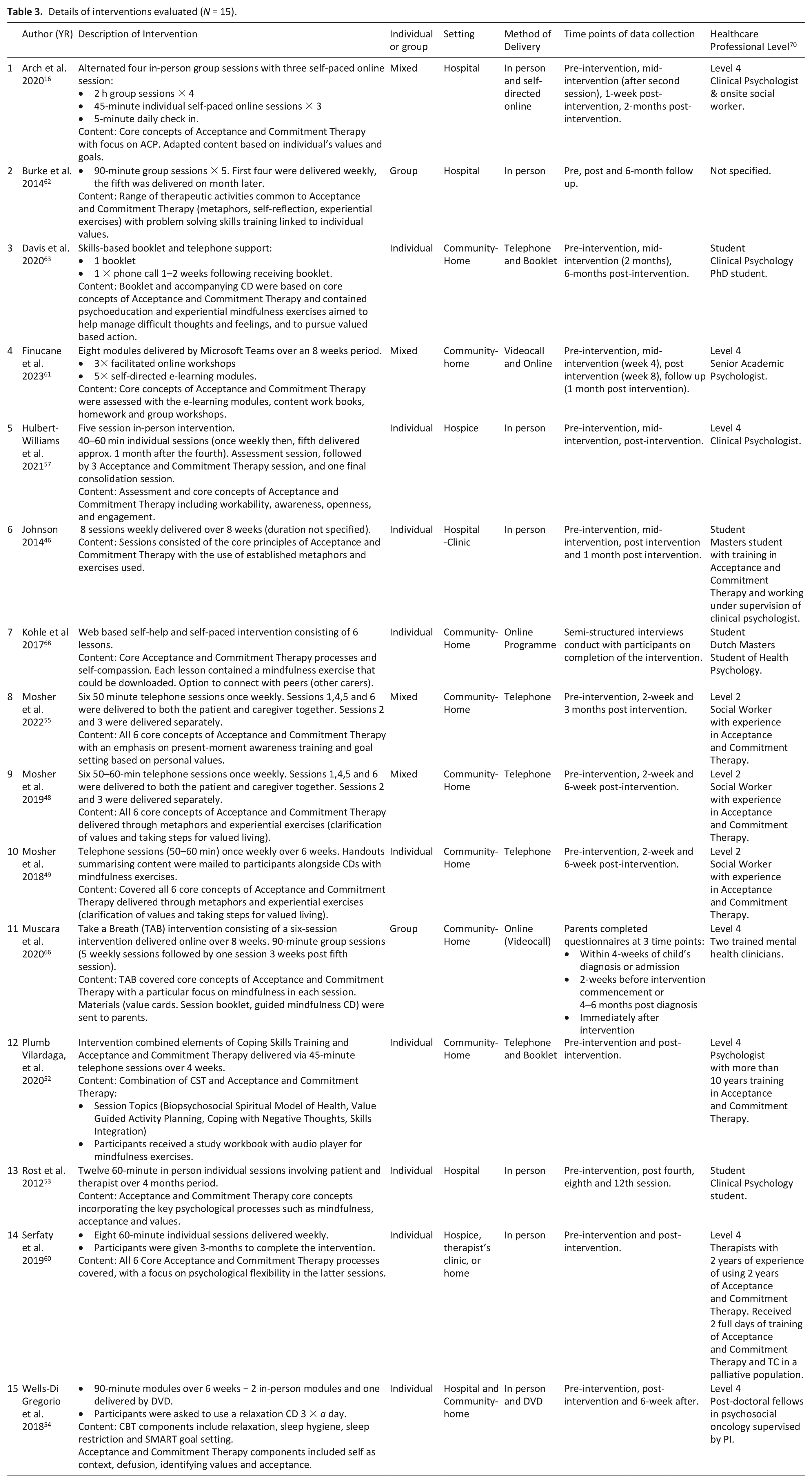
Details of interventions evaluated (N = 15).
Outcomes and findings of Acceptance and Commitment Therapy Intervention studies (N = 15).
AAQ-II: Acceptance and Action Questionnaire II.
PG: Prolonged Grief.
PROMIS: Patient Reported Outcomes Measurement Information System.
TAU: Treatment as Usual.
Settings
Four of the 15 intervention studies (27%) described interventions in hospitals16,53,62,63, eight (53%) described interventions in home settings.46,48,49,52,55,61,66,68 One intervention was delivered in both the hospital and community (7%) 54 and one was hospice-based (7%). 57 One paper described an intervention delivered in a hospice, therapist’s clinic or home (7%). 60 See Supplemental File: Figure 5.
Intervention mode of delivery
Most interventions evaluated were individual focused (n = 8; 53%)46,49,52 –54,60,63,68; three were group57,62,66, four were mixed (see Supplemental File: Figure 6).16,48,55,61 Interventions were most commonly delivered in person (n = 5, 33%),46,53,57,60,62 or by telephone (n = 5; 33%)48,49,52,55,68 (see Supplemental File: Figure 7).
Types of professionals delivering acceptance and commitment therapy interventions
Nearly half of the evaluated interventions (7/15; 47%) were delivered by specialists such as clinical psychologists.16,52 –54,57,60,61,63,66,68 A further three (20%) were delivered by social workers,48,49,55, three (20%) were delivered by clinical psychology students.53,63,68 One was delivered by an MSc student and supervised by a clinical psychologist (7%) 46 (see Supplemental File: Table 2).
Intervention content
All interventions incorporated the six core Acceptance and Commitment Therapy processes. Four combined Acceptance and Commitment Therapy with another intervention – traditional CBT, 54 Coping Skills Training, 52 Problem-solving Skills Training. 62 The studies used a variety of media, with five studies providing homework in the form of audiobooks,52,66 online modules,16,61 DVDs 54 and booklets52,63,66 (Table 3).
For treatment integrity, four of the intervention studies (27%) assessed intervention fidelity with developed checklists to ensure adherence to the treatment protocol48,49,55,66, four other studies carried out informal fidelity checks.52,54,57,61 Three of the papers stated that in future research they would develop fidelity checklists.46,60,61
Duration and frequency of interventions
Total duration of the interventions varied from 15 min to 12 h (Table 3). The longest intervention consisted of 12 weeks of 1 h in-person sessions delivered in hospital to people with advanced cancer. 53 The shortest duration was a one-off individual phone call (15–60 min) for informal caregivers. 68 Intervention sessions ranged from 15 to 120 min: in-person based sessions (60–90 min) and technology-based sessions (45–120 min). Group-based sessions lasted longer than the individual-based sessions. Two of the papers did not specify the duration of their intervention sessions (13%).46,63
The frequency of the interventions ranged from one-off63,68 to 12 sessions. 53 The 12-session study adopted an individual in-person mode of delivery. 53 Two thirds of the papers delivered weekly sessions (n = 10)46,48,49,54,55,57,60 –62,66 with three delivering booster sessions a month after the last session.57,62,66
Data collection points during interventions
Most intervention studies (n = 14/15) collected outcome data pre and post intervention.16,46,48,49,52 –55,57,60 –63,66 Ten of these further assessed their outcomes 1–12 months after the intervention was delivered.16,46,48,49,53–55,61–63
Outcome measures reported in intervention studies
A range of physical and psychological outcome measures were assessed (see Supplemental File: Figure 8/9). Psychological flexibility was assessed in nearly all papers (n = 12; 80%),46,48,52,53,55,57,60 –63,66,68, four of these used the AAQ-II to assess psychological flexibility.55,60,63,66 Other key outcomes assessed included anxiety (n = 6),16,52–54,63,66 depression (n = 6),16,52–54,63,66 distress (n = 7),48,52–54,57,60,62 valued living (n = 7)46,52,55,60,63,66,68 and pain interference (n = 5).16,46,48,49,52
Feasibility and acceptability of acceptance and commitment therapy
Six of the 15 intervention studies examined feasibility and acceptability as one of their stated outcomes.16,52,55,60,61,63 Enrolment rates varied from 19-82%. The studies reporting the lowest levels of recruitment involved participants recently referred to a hospice service in the UK (19% of those eligible consented), 57 and an intervention involving parents with elevated stress symptoms with a child admitted to hospital for a life-threatening illness or injury (25% consented). Recruitment was highest (82%) in a study involving patients with Stage III or Stage IV ovarian cancer, in which eligible patients were informed about the study during their routine clinic, and the intervention was scheduled to take place alongside their routine appointments to minimise travel and time requirements. 53 Across all interventions studies, retention rates ranged from 26-88%. Retention was highest (88%) for a study which used an individual telephone based intervention with sessions lasting 45 min, removing barriers of in-person intervention such as illness and travel. 52 It lowest for a study involving six-session online group intervention for in parents of children with a life-limiting illness. 62 Detailed data on enrolment and retention data can be found organised by participant population in Table 4 in Supplemental File 1.
Twelve studies (80%) reported patient satisfaction rates with their interventions16,49,52–54,57,60 –63,66,68; and interventions were generally acceptable to participants in all studies. Detailed data on satisfaction rates organised into population group in Table 5 in the Supplemental File 1.
Details of observational studies (N = 11).
PROMIS: Patient Reported Outcomes Measurement Information System.
Effectiveness of acceptance and commitment therapy interventions
Intervention studies reported on a wide range of outcome measures, broadly suggesting that Acceptance and Commitment Therapy results in improvements in a range of outcomes, though some improvements were not statistically significant (Supplemental File: Table 3). No studies identified negative or adverse impacts of Acceptance and Commitment Therapy.
Psychological flexibility
Nine studies reported improvements in psychological flexibility, though only two RCTs reported statistically significant improvements.53,66 The remaining studies showed improvements that were not significant: pre/post study designs (n = 5)46,52,57,61,62 and RCTs (n = 3).48,55,63 The qualitative study reported comments of participants showing increased psychological flexibility. 68
Anxiety
All of the studies which measured anxiety showed improvements (n = 6), although only two RCTs reported statistically significant improvements.53,54 The other studies showed improvements that were not significant, pre/post designs (n = 2)16,52 and RCTs (n=2).63,66
Depression
All of the studies (n = 6) which measured depression showed improvements, only two RCTs showed statistically significant improvements.53,54 Two pre/post studies16,52, two RCTs63,66 showed improvements that were not significant.
Distress
Six studies showed improvements in distress, with three RCTs showing statistically significant improvements53,54,60, three pre/post studies showing not statistically significant improvements.52,57,62
Valued living
Six studies showed improvements in valued living post intervention,46,52,60,63,66 although only one RCT showed statistically significant improvements. 66 Two pre/post studies46,52, two RCTs showed non statistically significant improvements.60,63 The qualitative study showed that a number of participants post intervention had an increased awareness of values in life and were living in accordance with personal values. 68 One study showed no improvements in valued living post intervention. 55
Pain interference
Only two of five of the studies examining pain interference showed improvements (40%), one pre/post study 52 and one RCT 16 showed improvements that were not significant. Three studies found no change; two RCTs48,49, one pre/post study. 46
Fatigue interference
Four studies reported improvements in fatigue interference, of these only one RCT showed statistically significant improvements. 49 The remaining three studies, two RCTs54,55, one pre/post design 52 described improvements that were not statistically significant.
Sleep interference
Three studies showed improvement in sleep interference, two RCTs reporting statistically significant improvements.49,54 One study did not show any improvements with sleep interference post intervention. 49
Quality of life
Three studies showed improvements in quality of life add53,55,57, one study reported significant improvements. 53 and one pre/post study 57 and one RCT 55 described improvements that were not significant. One pre/post study showed minimal change to quality of life post intervention. 61
Other outcome measures
Two studies described improvements in grief and anticipatory grief post intervention,46,63 though these were not statistically significant, and one was a PhD study involving only two participants. One pre/post study reported improvements that were not significant in mindfulness post intervention, but this was not statistically significant. 62
There was heterogeneity in outcome measures throughout the studies, many outcome measures were only reported in one study (Supplemental File: Figure 2). Four studies described statistically significant improvements in outcomes post intervention; emotional control, 53 thought suppression, 53 post-traumatic stress symptoms 66 and worry. 54
Qualitative evidence exploring the effectiveness of Acceptance and Commitment Therapy showed that caregivers found the intervention helped them to cope with negative emotions and thoughts. 68 Also, the intervention helped the caregivers become more aware of their personal values. 68 The caregivers expressed ambivalent feelings towards the peer support and content of feedback from the counsellor.
Findings from observational studies (n=11)
Eleven observational papers were identified.45,47,50,51,56,58,59,64,65,67,69 The most frequently assessed outcomes were acceptance (n = 6)45,47,50,58,64,65 and valued living47,50,51,64,67,69 both assessed in six studies (see Table 5).
Acceptance
Several papers found that higher acceptance was associated with statistically significant improvements in anticipatory grief,64,65 anxiety, 65 depression, 65 physical function 58 and low levels of burnout and stress. 56 There was also an association between higher acceptance scores and greater levels of work engagement, job satisfaction and wellbeing in staff. 56 A cross-sectional questionnaire study of people approaching end of life in an inpatient palliative care unit reported that acceptance was a significant predictor of reduced anticipatory grief over and above depression and anxiety, suggesting that acceptance-based interventions could play an important role in ameliorating suffering relating to anticipatory grief. 65 A doctoral thesis reported that therapists used acceptance and commitment therapy and positive adjustment in their practice for patients following bereavement. 59
Valued living
Statistically significant interactions were found between mindfulness, committed action and self-care behaviours. 69 One study found that avoidance and low importance of values in bereaved populations was correlated with bereavement difficulties. 51 Unexpectedly, in one study higher scores of valued action were significantly correlated with higher scores of physical pain and death attitudes. 67
Grief and anticipatory grief
Higher acceptance was statistically significantly associated with lower anticipatory grief. 65 Also, increased acceptance and valued living was statistically significantly associated with improvements in adjustment to loss amongst bereaved university students. 64
Discussion
This is the first review to comprehensively map the evidence on Acceptance and Commitment Therapy for people with an advanced progressive illness and their formal and informal caregivers. To date, most research has been conducted in the U.S, most studies have involved patients, and most interventions have been community-based, and delivered in-person or via telephone. Our findings suggest that Acceptance and Commitment Therapy is acceptable to people with an advanced progressive illness and those involved in their care. Across all studies, Acceptance and Commitment Therapy interventions were feasible to evaluate, at least in the short term. Nearly all intervention studies described improvements in distress, anxiety, depression, and psychological flexibility, though not all improvements were statistically significant, often due to underpowered studies. No negative impacts of Acceptance and Commitment Therapy were reported in any intervention study. Observational studies described significant associations between core Acceptance and Commitment Therapy processes such as acceptance and key psychological outcomes including adjustment to loss.
Overall, recruitment to Acceptance and Commitment Therapy intervention studies generally appeared feasible, with most studies reporting recruitment rates of at least one-third of those eligible. Challenges associated with recruitment and retention of participants in palliative care studies are widely recognised, with factors such as deteriorating health, feelings of being overwhelmed, and fatigue, all contributing to low levels of recruitment and retention.71,72 Gatekeeping is also an issue with ‘fear of burdening vulnerable patients’ the most reported reason for gatekeeping among healthcare professionals. 73 In this scoping review, recruitment was lowest in an intervention study recruiting participants during the period in which they had just been referred for hospice care 57 – a time during which patients can feel heightened levels of distress, while professionals may be more likely to gatekeep as they focus on clinical care. In contrast, recruitment was highest where the intervention took place alongside routine appointments, minimising the need to travel and reducing overall research burden. 53 Strategies to improve recruitment include having research staff on-site, limiting burden by running intervention alongside routine care, offering flexibility around location and timing of participation, engaging patient representatives in the design of recruitment strategies, and working closely with healthcare professionals and leaders to promote research engagement.71–73
This review provides strong evidence that Acceptance and Commitment Therapy is acceptable in palliative care settings. In most intervention studies, attrition was low during intervention delivery, with most studies reporting retention rates of 75% or higher. Evidence regarding acceptability resonates with findings from a recent UK national survey which reported that 41% of hospice psychological support teams use Acceptance and Commitment Therapy to support patients and families. 41 This suggests that even though evidence is still emerging, practitioners find Acceptance and Commitment Therapy a valuable psychological approach in palliative care. This could be due to its logical fit with the needs of patients with advanced progressive illness, or the strength of evidence for Acceptance and Commitment Therapy in other health populations, or it could be due to the finding that training in Acceptance and Commitment Therapy has benefits for both therapeutic skills and for personal wellbeing.74–76
We found preliminary evidence that Acceptance and Commitment Therapy is effective in improving key psychological outcomes for patients, carers and palliative care staff. Following Acceptance and Commitment Therapy, participants in most studies reported improvements in psychological flexibility,46,52,53,55,57,61–63,66,68 anxiety,16,52–54,63,66 and depression.16,52–54,63,66 Although preliminary, these findings reflect the benefits of Acceptance and Commitment Therapy reported for other populations, including people with mental health problems and chronic pain.26,77 Evidence for benefits of Acceptance and Commitment Therapy on physical outcomes such as fatigue, sleep and pain was limited. Weak effects for pain interference were found, with half of the papers assessing pain showed no change post intervention.16,48,49 Findings in palliative care populations broadly align with findings from a review of Acceptance and Commitment Therapy for chronic pain, which found significant effects of Acceptance and Commitment Therapy on pain acceptance, but no impact on pain severity. 77 Overall, given the small sample sizes, focus on feasibility and acceptability over efficacy and effectiveness in many studies, and use of pre-post designs, further research examining the effectiveness of Acceptance and Commitment Therapy on key psychological and physical outcomes in palliative care populations is warranted.
There is existing evidence that acceptance is an important element for a good death and a facilitator in the provision of end-of-life care. 78 Findings from observational studies in this scoping review supports the view that acceptance is a key process in palliative care. Acceptance was associated with improved anxiety, 65 depression, 65 death acceptance, 64 lower anticipatory grief64,65 and mobility. 58 Greater acceptance was also linked with higher levels of work engagement, job satisfaction and wellbeing in palliative care staff. 56 In Acceptance and Commitment Therapy, acceptance describes a willingness to open-up and make room for difficult thoughts and emotions, when this helps the person accomplish something they care about. It is viewed as an active choice that involves decreasing the effort that one exerts to control or regulate inner experience, and actively experience things as they are.52 –54,57,60,62 For instance, acceptance may involve a willingness to experience difficult thoughts and feelings associated with an advanced progressive illness in the service of communicating preferences regarding future care and plans. This contrasts with experiential avoidance which might involve attempts to reduce or avoid unwanted inner experiences when doing so has a negative impact on functioning, or may get in the way of doing what is important and most valued. Promoting acceptance amongst people with an advanced progressive illness, and their carers, may support better communication and clarity around future care preferences. Recent evidence from a feasibility study points to the acceptability of Acceptance and Commitment Therapy to address advance care planning needs of depressed and anxious adults with advanced cancer. 16 Further research on this relationship is warranted
In this scoping review, short or flexibly delivered interventions resulted in greater participant retention.16,48,49 Brief psychosocial interventions have been found to be effective in improving clinically relevant outcomes for people receiving palliative care.38,79 Illness stage is also an important consideration, with shorter, flexible intervention formats being essential for those using hospice services and closer to the end of life. We identified two hospice-based interventions studies in this review. In one study, 4 of 10 participants recruited died during the study 57 in the other, only 8 of 20 (40%) allocated to the 8-week intervention condition completed the 1.5 month follow-up due to death, feeling too unwell, feeling overburdened and related reasons. 60 Given deteriorating physical health, earlier intervention is important for people with an advanced progressive illness, and where this is not feasible, brief and flexible interventions, which do not overburden the person, need to be prioritised.
Strengths and limitations
This is the first comprehensive review focused on Acceptance and Commitment Therapy in palliative care settings, synthesising evidence for people with any advanced progressive illness, their caregivers, and staff involved in their care. This review, which draws on data from 26 research studies, extends the findings from a systematic review in this area, which summarised findings from six studies involving people with advanced cancer. 38 Given the rapid growth in Acceptance and Commitment Therapy as an effective psychological intervention for people with a range of conditions, 29 this review is timely.
A number of limitations are noted. First, a high degree of heterogeneity in relation to study populations, aims, intervention designs and format made some comparisons difficult. Secondly, the lack of control group in most studies limited the strength of evidence, such that only preliminary evidence on effectiveness could be described. Thirdly, as most intervention studies focused on people with advanced cancer, conclusions regarding the use of Acceptance and Commitment Therapy for other populations was limited. As this was a scoping review, we focused on mapping the broad field rather than critically appraising papers, and quality appraisal was not undertaken. Choices regarding study inclusion were pragmatic, and papers in languages other than English were excluded; therefore, findings may be limited in the extent to which they apply across cultures.
Directions for future research
Of the 26 studies reviewed, only three focused on Acceptance and Commitment Therapy for bereavement support. The dearth of evidence on Acceptance and Commitment Therapy for bereavement was also recently noted in a systematic review on managing grief, which only identified two studies. 40 Future research is needed to explore the acceptability and value of Acceptance and Commitment Therapy for people who have been bereaved. Similarly, only two studies involving palliative care staff were identified,45,56 however given the effectiveness of Acceptance and Commitment Therapy in promoting wellbeing in other occupational settings, 37 further research examining Acceptance and Commitment Therapy for palliative care staff wellbeing is warranted. Most patient studies involved people with cancer, so research involving people with other advanced progressive or life-limiting illnesses is needed.
Interventions need to be scalable and cost-effective to implement, so future feasibility testing of interventions needs to incorporate preliminary economic evaluation. Similarly, models of intervention delivery which rely on highly specialist staff such as clinical psychologists for delivery may not be scalable, so research is needed to adapt interventions so that Acceptance and Commitment Therapy can be delivered by a wider range of professionals. There is now emerging evidence for the value of Acceptance and Commitment Therapy delivered online in other settings, 26 so given the potential for online interventions to increase access to psychological support, future evaluation of online Acceptance and Commitment Therapy for palliative care is timely. Greater consideration of the acceptability and effectiveness of Acceptance and Commitment Therapy for diverse groups and cultures is also recommended.
In terms of research design, efficacy, effectiveness and implementation studies involving patients and carers need to be prioritised. Few full-scale evaluations of Acceptance and Commitment Therapy to support patient, carers and staff wellbeing in palliative care settings have been conducted, so evidence regarding effectiveness remains uncertain. Mixed method evaluation studies, with larger sample sizes and comparison conditions are needed. Hybrid effectiveness-implementation studies are also recommended to explore how delivery of the intervention can be scaled up, and delivered in health and social care contexts.80,81
Implications for clinical practice
Whilst this field of research and practice is still early in its development, practitioners can be reassured that Acceptance and Commitment Therapy has a relatively robust evidence base in many related areas of practice, such as organisational stress, caregiver stress, chronic and mental ill health. This review provides evidence that Acceptance and Commitment Therapy interventions for people with advanced progressive illness are likely to be acceptable, and feasible to deliver, with preliminary evidence of efficacy. There is also evidence from pre-trial cross-sectional studies that the processes targetted in the Acceptance and Commitment Therapy model are related to wellbeing in people with advanced illness and therefore are logical intervention targets. Given the early stage of development of this field, it may be valuable for clinicians to routinely evaluate practice and identify unusual or boundary cases that could be written up as case studies to inform intervention development. Given the heterogeneity of delivery seen in this review, clinicians should be encouraged to explore and evaluate delivery methods in routine practice, in parallel with further research. In particular, training non psychologists / non psychotherapist to deliver elements of Acceptance and Commitment Therapy may be useful to address the relative scarcity of those professional groups, relative to others.
Conclusion
Acceptance and Commitment Therapy is acceptable and feasible to deliver in palliative care settings. There is preliminary evidence that Acceptance and Commitment Therapy improves anxiety, depression and distress amongst those with advanced progressive illness, as well as their caregivers. Full scale mixed method evaluation studies involving larger samples and a comparison group are now needed to demonstrate efficacy, effectiveness and cost-effectiveness. Further intervention development and feasibility studies involving staff and bereaved carer populations are warranted.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231183101 – Supplemental material for Acceptance and Commitment Therapy (ACT) for people with advanced progressive illness, their caregivers and staff involved in their care: A scoping review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231183101 for Acceptance and Commitment Therapy (ACT) for people with advanced progressive illness, their caregivers and staff involved in their care: A scoping review by Tilly Gibson Watt, David Gillanders, Juliet A Spiller and Anne M Finucane in Palliative Medicine
Footnotes
Acknowledgements
We are very grateful to Ruth Jenkins at the University of Edinburgh for advice on literature searching. Thank you also to Jean Lugton and Anne Canny for proof-reading and providing helpful comments on a draft version of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Anne Finucane is funded by a Marie Curie Senior Research Fellowship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.