
Abstract
Background:
Individuals from minoritised ethnic backgrounds are less likely than individuals from the dominant ethnic group to access palliative care services and to have documented Advance Care Plans. They are more likely to be admitted to hospital in the last months of life.
Aim:
To use the Community Readiness Model to identify the barriers that influence how South Asian communities access and use two new palliative care services.
Design:
The Community Readiness Model is a validated tool that measures the readiness of a community. Key stakeholders were asked to: (i) complete a questionnaire to assess South Asian communities’ readiness to engage in advance care planning and, (ii) attend a focus group to explore their views on the communities’ understandings of palliative and end-of-life care.
Setting/participants:
Ten key stakeholders who held a variety of occupations within palliative and end-of-life care services were recruited from the community.
Findings:
The South Asian communities were found to be at the ‘pre-planning’ stage of readiness, despite initiatives to improve awareness. The readiness of the health system was found to be limited, with a narrow medical focus during advance care planning, poor integration of voluntary and community services and limited understanding of what people consider a ‘good’ death.
Conclusions:
The Community Readiness Model allowed insight into the South Asian communities’ awareness of and readiness (to use) palliative care services. Using the Community Readiness Model before service implementation allowed steps to be taken to avoid widening inequities in access and use of new services.
The degree to which individuals access and use palliative and end-of-life care services varies across communities and countries.
This study found that the South Asian community (in Bradford, UK) are currently not ready to engage with palliative and end-of-life care services despite local initiatives to improve awareness. They are at the “pre-planning stage” (see Table 1) about end-of-life care options and of the services that are available to them.
This study also found evidence that the services that aim to support people from minoritised ethnic communities at the end-of-life are not ready to address ethnic inequities.
Such services were found to have: (i) a narrow focus during advance care planning, (ii) poor integration of voluntary and community services (iii) and limited understanding of what a good death looks like for people from different cultural and religious backgrounds.
This study highlights the importance of assessing the degree to which both the community and the health and social care systems are ready to incorporate new initiatives so they are effective and successful in addressing (and not strengthening) existing inequities.
Introduction
Access to palliative and end-of-life care services varies across different demographic groups. 1 There is a recognition that services need to be modified to reflect different community characteristics and cultures, including family structures, prevailing faith orthodoxies and attitudes towards service providers. 2 There has been a particular concern to increase the use of advance care plans as a route to empower patients and their families in making choices about end-of-life care. 3 Work focussing on specific local communities has illustrated that when service offer and delivery can be aligned with prevailing beliefs and practices, take-up subsequently increases.4,5
This research used the Community Readiness Model 6 to understand the readiness that South Asian communities have to engage with new end-of-life services and in particular to undertake advance care planning. The model also provided insight into how far health and care service providers were planning innovations that were consistent with community knowledge and beliefs.
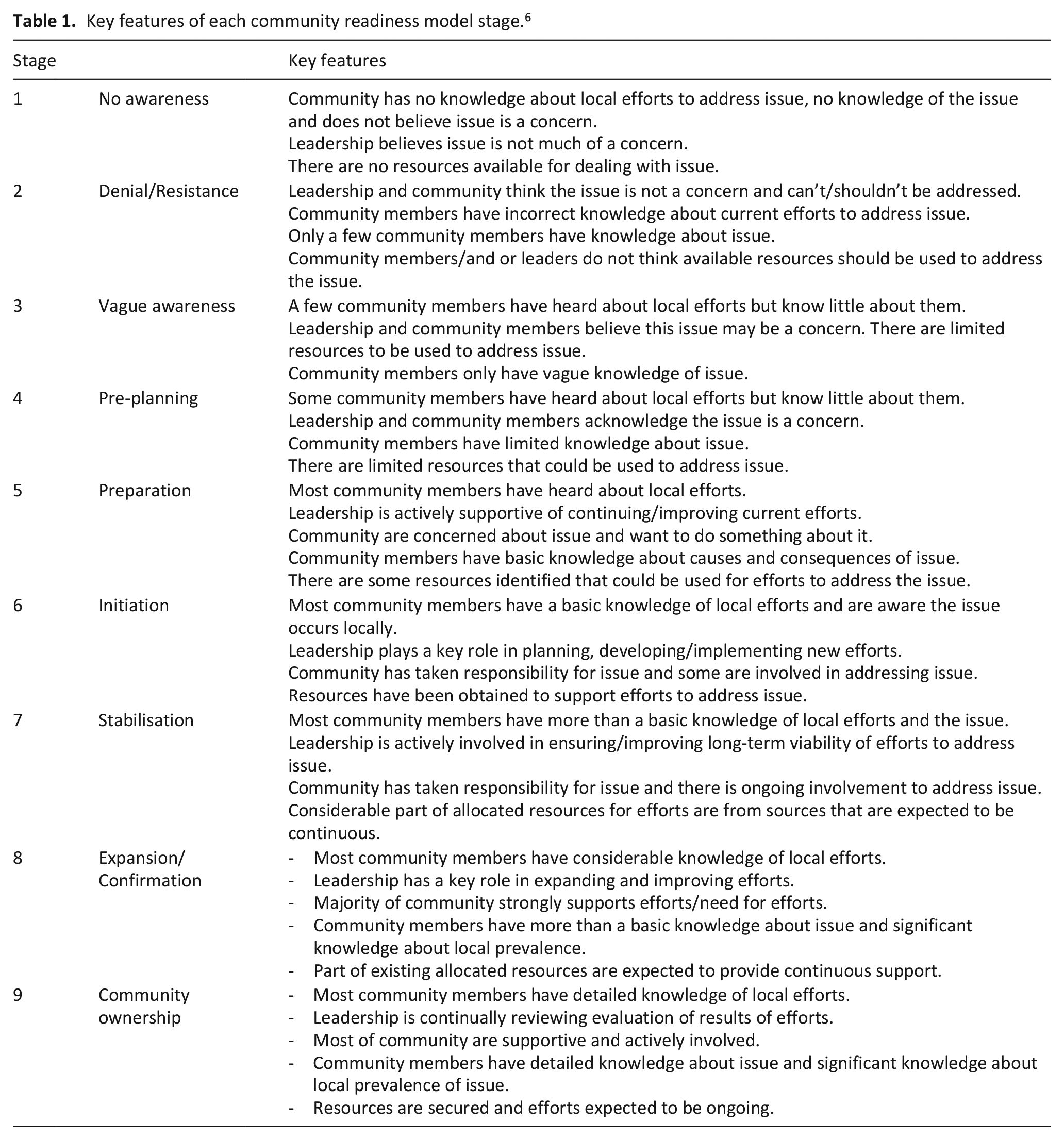
The Community Readiness Model places a community in one of nine possible states ranging from ‘no readiness’ to ‘community ownership’ (see Table 1). Understanding a community’s stage of readiness can assist with service design and with the preparation needed before the introduction of a new service. Findings from the Community Readiness Model can guide action to increase the likelihood of successful uptake of a service. It is an approach that has been used successfully in relation to other areas of health need,7,8 but such an approach has not been previously used to explore the palliative care within South Asian communities.
Key features of each community readiness model stage. 6
Whilst previous work has explored community readiness in relation to end-of-life care,9,10 this is the first study to utilise the model to explore readiness in South Asian communities to engage in end-of-life care services and it adds to the current literature that explores the end-of-life and palliative care for people of South Asian heritage.11,12 In comparison to previous literature (that focused on understanding the perspectives of South Asian individuals 12 and providing suitable community-based culturally appropriate end-of-life care 11 ), this study focuses on exploring the way in which South Asian communities view new end-of-life services.
Method
Study context
In 2019, Bradford NHS Clinical Commissioning Group explored levels of engagement (using focus groups and surveys) in relation to the way in which people think and feel about the end-of-life period within this community. It was noted in an internally circulated report, that Advance Care Plans were not discussed.
Seeking to improve the knowledge of, and to reduce inequities in the take-up of end-of-life care in the inner City of Bradford and in the use of Advanced Care Plans, the area’s Clinical Commissioning Group planned two specialist support initiatives: (i) a social prescribing and befriending service called ‘Choices’ to assist those approaching the end-of-life and, (ii) a Proactive Care Team of palliative care nurses to support individuals at the end-of-life.
Study design
The Community Readiness Model is a mixed methods approach that incorporates readiness scores and focus groups. Six dimensions help to ascertain the level of readiness within a community: community efforts, community knowledge of the efforts, leadership, community climate, community knowledge of the issue and resources for prevention (of the issue). The Community Readiness Model can be adapted to meet local circumstances.13,14 Consistent with this, we used a mixed methods approach, a self-completed questionnaire (to generate readiness scores), followed by online focus groups (to explore the self-completed questionnaire scores in more depth).
Study setting
Bradford is a city in the north of England with high levels of socioeconomic deprivation and ethnic diversity. There are a large number of South Asian people (9.9%), predominantly of Pakistani heritage (7.7%). 15 The Community Readiness Model was used to aid plans for the introduction of two specialist support services (see Study Context) so that possible inequities in regards to the access and use of such services could be reduced.
Participants
Population and inclusion criteria
The Community Readiness Model uses key stakeholders. In this study, the inclusion criteria consisted of individuals who were familiar with palliative and end-of-life care services and with the views of South Asian communities (current patients, carers and relatives were not included).
Sampling approach
Key stakeholders were identified and invited to join the study by the Clinical Commissioning Group. Key stakeholders are expected to provide understanding about ‘the community in an esoteric way’.8,16,17
Recruitment
A total of 10 stakeholders took part and each completed a questionnaire and participated in a focus group. Stakeholders came from a variety of different ethnic groups (specific participant demographic details were not collected because this information was not deemed essential).
Data collection
The mixed methods approach was carried out sequentially, with a five-item questionnaire administered in advance of the focus group sessions. The average readiness scores ascertained from the questionnaires were used to: (i) inform the best way for the research team to introduce each focus group session, (ii) to explore variability between participants’ views in advance of group discussion and, (iii) give direction for in-depth exploration of key issues during focus groups.
Pre-focus group questionnaire
A five-item questionnaire was created specifically for use in this study by our research team. We generated questions that were closely related to the six Community Readiness Model dimensions with options to score each from 1 to 9 based on their perception of the readiness of the community (see Supplemental File 1). Participants’ response scores were averaged to generate a total readiness score (the lower the score the less ‘readiness’ the community demonstrates). This questionnaire provided an initial idea as to the level of readiness key stakeholders believed was present and also ascertained individual perceptions without peer influence.
Focus group sessions
Participants then took part in one of two focus group sessions in July 2021. A pre-generated topic guide (see Supplemental File 2) was used to question stakeholders about their knowledge of the communities’ awareness of, and readiness to take-up, palliative and end-of-life care services. Focus groups were used to give further depth and context to the scores that stakeholders gave in the pre-focus group questionnaire.
Ethics
Health Research Authority ethical approval was obtained on 26.04.2021 (reference: 292954).
Data analysis
Descriptive statistics were used to identify the median and range scores of the questionnaire. After the focus groups were transcribed, reflexive thematic analysis was undertaken by two researchers (RM, NS). 18 Each focus group was analysed separately using the main interview questions (see Supplemental File 2) to identify the main themes. Similarities and differences between individuals responses were noted to help identify the prominent themes across both focus groups. Findings were then pooled to identify similarities between groups. The wider research team explored these and developed conclusions and recommendations.
Findings
A total of 10 stakeholders took part, including clinical staff, end-of-life Choices Co-Ordinators, Clinical Commissioning Group members and Voluntary and Community Sector workers. In the pre-focus group questionnaire, the median score was 4.1 (range: 3.6–4.8) which indicates that key stakeholders felt that the South Asian communities were at the ‘pre-planning’ stage (stage 4, see Table 1).
However, in the focus groups, key stakeholders gave responses that suggested the South Asian communities had only a ‘vague awareness’ of palliative and end-of-life care services (stage 3) (i.e. showing less ‘readiness’ than in their pre-focus group questionnaires). This discrepancy between the mean pre-focus group questionnaire score and the focus group score was discussed by the research team. After weighing the range and strength of opinions identified in the focus groups themes against the scores from the pre-focus group questionnaires, it was concluded that the communities as a whole were at the ‘pre-planning’ stage (stage 4).
A summary of the overarching themes identified are summarised below:
1. Continued lack of awareness of palliative and end-of-life care services in the communities – despite efforts to increase engagement.
Stakeholders described a lack of awareness about palliative and end-of-life care (along with associated services) in the South Asian communities. This is despite significant initiatives to support better awareness and knowledge within these communities, including moving the hospice from the outskirts of Bradford to the more ethnically diverse inner city and the employment of a South Asian ethnic liaison worker. When discussing death, post death concerns including funerals and the wish for a prompt burial took precedence. Unless care has been provided to a relative or experienced first-hand, many were unaware that professional end-of-life support exists. There was support for introducing end-of-life care earlier in the illness trajectory for suitable individuals and a recognition that understanding community needs takes time and requires both good relationships and trust.
There was also consensus across both focus groups that the lack of awareness surrounding palliative care and end-of-life care services seen in Bradford was a reflection of a wider reluctance to discuss death.
‘Prior to the pandemic we interviewed 256 residents across Bradford districts and Craven, and I think two people mentioned the term advanced care planning, out of 256’.
‘. . .it hasn’t got in the community, definitely not got into the South Asian community. . . I don’t think I’ve ever come across this [the end-of-life care initiatives]’.
‘as a society we don’t talk about death, generally, in the same way that we will dedicate our time to preparing for the arrival of a new birth in the family or in the community. . .’
‘Understanding what’s happening at a community level and what a community needs, takes time. . .’
‘. . .I think for me it comes back to again building that trust, to have these discussions, and the skillsets as healthcare professionals to have these discussions about faith and try to understand. . .’
2. Continued focus by healthcare professional on clinical elements of advance care planning – despite local and national initiatives.
Healthcare staff acknowledged that professionals continue to focus on end-of-life care arrangements (e.g. where people want to die) or on clinical aspects (e.g. do not resuscitate decisions) of advance care plans rather than taking a holistic approach. This is despite local and national initiatives and teaching to support the emotional, spiritual, cultural and social dimensions of end-of-life care. Participants felt it was unclear who was responsible for facilitating holistic discussions and did not feel that previous initiatives to engage communities had been effective.
‘. . .I’m also not convinced that doctors really do brilliant advanced care plans, they do ones that are medically good some of the time, so I get some helpful ones back about what medical things patients do or don’t want, but I don’t get a sense of who the patient is and what’s important to them. . .’
‘. . .we don’t really have a single definition of what an advanced care plan, is an advanced care plan a conversation, or is it the documents? Who should be having these discussions?’
‘. . .make sure this advanced care planning has all the MDT [multi-disciplinary team] round it’.
3. Poor integration of services – in particular with Voluntary and Community Sector services.
Stakeholders acknowledged difficulties amongst services to ‘Act as One’ – a key regional initiative to support more integrated service provision. In Bradford, while efforts have been made to encourage specialist and generalist palliative care services to work more closely together, participants highlighted the barriers for voluntary organisations caring for people at the end-of-life if they did not have access to patient notes.
‘. . .we as specialist services need to integrate, so those people who are accessing palliative care early on really get good services. . .’
‘. . .there’s been a real power dynamic between them as being voluntary service providers and healthcare providers, so they couldn’t get access to patient notes’
‘. . . hearing those stories about lack of connection and people not knowing and services not working closely together, I think there’s a real issue there about integration of care, from all sides’.
‘. . .this is about everybody and it’s about trying to be inclusive. . . communities within communities absolutely we should be working with’.
4. Understanding what good end-of-life care looks like for culturally diverse communities.
Stakeholders reported that service providers and commissioners needed to have a greater understanding of South Asian communities. It was felt that the prevalent view of what a ‘good death’ may be is based on a white British perspective, and it is not known what a ‘good death’ means to members of South Asian communities. This is despite work to discuss and engage community members, including employing a community liaison worker. Additionally, attention needs to be given to family structures which are characterised by extended family networks and multi-generational households.
‘. . .Because what does a good death look like, what is a good death from a South Asian patient point of view? We don’t know. All we know, what is a good death from a middle class, white Caucasian, . . . educated point of view’.
‘. . .no one can tell me what is a good death experience from the South Asian point of view, what does the community want or need?’
‘. . .there’s very little training about understanding faiths in a different way, yet where our speciality is all about, you know, we say we value spiritual care at the end-of-life as much as the physical symptoms but I don’t think our training necessarily reflects that’
‘. . .its institutional barriers that we haven’t taken down to enable these different communities to participate. . .’
5. Understanding what good end-of-life care looks like for different faith communities.
It was agreed that faith concerns needed specific attention. While the prevailing view was that faith communities shared many of the attitudes of wider society, including a reluctance to discuss death, there were some differences. It was suggested that the South Asian communities may have different ‘social constructs’, perhaps linked with a belief that Islam ‘requires’ that one does everything possible to preserve life and that end-of-life care planning may be perceived as hastening death. However, it was acknowledged that some Islamic scholars (including local ones), offered an alternative viewpoint which centred on quality of life.
‘. . .they are from Muslim faith, and it’s widely held that you have to do everything to save life till the very end. Whether it’s right or not. . .’
‘. . . you mentioned the South Asian community for example, our social constructs might be very different to the general take on things’.
‘. . .what do the different faiths want after death, there’s very little training about understanding faiths in a different way. . .’
Discussion
There was evidence of limited awareness about end of life services. However, most findings for each of the individual themes points towards limitations in the healthcare system to adequately achieve an improved level of community readiness rather than some inherent deficiency or resistance on the part of the community. There was limited engagement in advance care plans by healthcare professionals, and there was a focus on a narrow medical view. There was poor integration of voluntary and community sector services to support early identification of end-of-life care needs, and to offer education and support for those with multiple barriers to accessing services. In addition, there was limited understanding of what a ‘good’ advance care plan and a ‘good’ death means for people from different cultures and faith communities. Despite initiatives to address ethnic inequities for people from the South Asian community, many persist.
Key stakeholders agreed that increasing awareness of end-of-life care services and advance care planning needs to prioritise understanding community views, ideas and expectations. To help increase death awareness as a community issue, it would be imperative to facilitate discussion using public information and existing avenues for public and patient engagement. 19 This would include holding discussion spaces in community venues, led by community groups and having drop in sessions to allow for a safe space for individuals to ask questions. 20
More generally these findings mirror those from national and international evidence that illustrate the public (at large) have a limited knowledge of palliative-care services and that this can be part of death avoidance.21,22
Our findings support the need to combine a focus on assessing community readiness and community inclusion to foster a public health approach to palliative care service development.23,24 Simply informing ‘communities’ of services and assessing their readiness to use services, without understanding structural and systemic barriers to inclusion and wider issues within the health services such as integration 25 and embedment, will result in ongoing exclusion of minoritised groups.26,27 The COVID-19 pandemic has led to services being more cognisant of their lack of knowledge about what a ‘good death’ looks like for diverse ethnic communities28,29 with the wider literature suggesting significant crossover between different communities,30–33 in addition to intra and inter-community nuance. 34 Care providers need to enhance their knowledge and cultural competency and address structural barriers including representation of the workforce. 35 Care providers also need to practice cultural humility to support more inclusive service development and engagement that prioritises the needs of culturally diverse communities. 36 This is the groundwork necessary to build trust and promote equity and agency, which are all necessary to address ethnic disparities. 37
Our findings underline the importance of using validated methods (that have been used across a variety of domains) 8 to ascertain community knowledge and community views before detailed plans for new services are implemented. Having a better understanding of why individuals in the South Asian communities do not engage with discussing the end-of-life care period or why they do not avail themselves of advance care plans means that service providers can undertake a period of listening to communities and acting on their ideas and concerns to inform new services/approaches. When those services are then launched they will be introduced into a now more knowledgeable and receptive community.19,38 National guidelines in multicultural societies such as the UK now recognise the importance of community partnerships and commitment to equity to address inequities at the end of life – how to do this has not been clearly outlined. 39 Our findings suggest working on service providers readiness to listen and act on what is heard through an equity lens, is an essential first step.
Limitations
The Community Readiness Model approach uses a small sample, and asks key community leaders and stakeholders to discuss in-depth the levels of readiness of a community. The small sample size may have limited the themes identified as the findings represent the views of the selected stakeholders and may not represent the views of the wider community or community members themselves. The Community Readiness Model is designed to uncover gaps in understanding amongst both the lay-person and professional communities, and as such encourage further work to focus on addressing these gaps.
Our adapted Community Readiness Model methodology gave us several benefits. The pre-focus group questionnaire reduced the potential influence of peers and allowed stakeholders to begin to consider the areas of concern in advance of the focus group. This may have helped facilitate the free flowing discussions that took place. As researchers, having an idea of stakeholders’ opinions in advance of the focus group also enabled us to better prepare.
We acknowledge that this study provides us with just one perspective on the South Asian communities and other avenues of exploration would further the depth of understanding within these communities, most importantly speaking directly to members of these communities.
Conclusion
Assuming that services that work in some communities will work in all risks perpetuating inequities. Using the Community Readiness Model approach allows services to identify levels of community readiness and the steps needed to enhance engagement in new services and to ensure the cultural appropriateness of all services. However, services must also consider their readiness to hear the views of community members, change models of care and address inequity at the end-of-life. Wider engagement and integration of the health and social care system should be in place before new services are implemented to support access.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221146587 – Supplemental material for Applying the community readiness model to identify and address inequity in end-of-life care in South Asian communities
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221146587 for Applying the community readiness model to identify and address inequity in end-of-life care in South Asian communities by Rachael H Moss, Jamilla Hussain, Shahid Islam, Neil Small and Josie Dickerson in Palliative Medicine
Footnotes
Contributor statement
RM and JD obtained IRAS ethical approval for this study. RM, JH, SI, NS and JD designed and finalised the methodology, along with the interview topic guide and accompanying documentation. RM and NS conducted the focus groups within this study. RM and NS analysed the transcripts and once complete, discussed the findings with JH, SI and JD. Discussions amongst the team (RM, JH, SI, NS and JD) took place to decide final themes and recommendations. RM, JH, SI, NS and JD wrote this manuscript and all authors are willing to be accountable for it.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Bradford District and Craven Clinical Commissioning Group.
Patient and public involvement
Members of the community that were deemed to be key stakeholders (as described in the method) were involved in the focus group sessions that took place.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.