
Abstract
Background:
People who use drugs with life-limiting illnesses experience substantial barriers to accessing palliative care. Demand for palliative care is expected to increase during communicable disease epidemics and pandemics. Understanding how epidemics and pandemics affect palliative care for people who use drugs is important from a service delivery perspective and for reducing population health inequities.
Aim:
To explore what is known about communicable disease epidemics and pandemics, palliative care, and people who use drugs.
Design:
Scoping review.
Data sources:
We searched six bibliographic databases from inception to April 2021 as well as the grey literature. We included English and French records about palliative care access, programs, and policies and guidelines for people ⩾18 years old who use drugs during communicable disease epidemics and pandemics.
Results:
Forty-four articles were included in our analysis. We identified limited knowledge about palliative care for people who use drugs during epidemics and pandemics other than HIV/AIDS. Through our thematic synthesis of the records, we generated the following themes: enablers and barriers to access, organizational barriers, structural inequity, access to opioids and other psychoactive substances, and stigma.
Conclusions:
Our findings underscore the need for further research about how best to provide palliative care for people who use drugs during epidemics and pandemics. We suggest four ways that health systems can be better prepared to help alleviate the structural barriers that limit access as well as support the provision of high-quality palliative care during future epidemics and pandemics.
Keywords
Communicable disease epidemics and pandemics, such as the COVID-19 pandemic, intensify the healthcare inequities encountered by people who use drugs.
Pandemics are expected to increase the demand for palliative care resources.
People who use drugs with life-limiting illnesses experience inequities in access to palliative care.
There is limited evidence beyond the HIV/AIDS context to guide decision-makers on the provision of palliative care for people who use drugs during communicable disease epidemics and pandemics.
This paper demonstrates that there is limited knowledge about how to provide palliative care for people who use drugs during epidemics and pandemics other than HIV/AIDS.
We identified enablers and barriers to equitable palliative care access, which include organizational barriers, issues related to stigma and structural inequity, and access to opioids and other substances
Our findings build on past research that seeks to integrate the premises of health equity within palliative care so health systems can be better prepared for future epidemics and pandemics.
The findings from our scoping review provides accessible and relevant evidence for healthcare professionals and decision-makers (e.g. policy makers, administrators) that can be applied to the COVID-19 pandemic response efforts and potentially future epidemics and pandemics.
More research is needed about palliative care access, policies, and programs for people who use drugs during communicable disease epidemics and pandemic beyond the HIV/AIDS context.
Introduction
People who use drugs have an elevated risk of death compared to the general population. 1 People who use drugs refer to people who use(d) drugs such as alcohol, tobacco, cannabis, heroin, fentanyl, and may have experienced non-iatrogenic harm (e.g. psychological, physical, legal, and policy-related) associated with their drug consumption. 2 They are also at high risk of life-limiting illnesses such as Acquired Immunodeficiency Syndrome (AIDS), cancers, pulmonary diseases, and liver cirrhosis, 3 and can benefit from palliative care. 4 Previous research has identified how palliative care tends to deprioritize the needs of populations who are “doubly vulnerable”—people who require palliative care and are disadvantaged in terms of the social determinants of health. 5 Many people who use drugs have unique end-of-life care needs, and encounter barriers in having these needs addressed. Barriers include the influence of structural inequities such as poverty and homelessness, stigma, and systemic racism, resulting in fewer social support and financial resources. 6 Healthcare professionals also face difficulties in identifying members of this population who would benefit from palliative care. 7 Delivery of community-based palliative care may be limited for this population due to concerns that settings, such as shelters, are unsafe. 8 Zero-tolerance policies toward non-medical use of substances also restrict access to many palliative care units and hospices.8,9
COVID-19, substance use, and palliative care
Communicable disease epidemics and pandemics intensify the healthcare inequities encountered by people who use drugs. 1 The novel coronavirus pandemic (COVID-19) has increased the risks associated with substance use, and vice-versa.6,10 Loss of in-person clinical and support interventions is exacerbating substance use and leading to worse health outcomes, particularly for those who are structurally disadvantaged. 11 An analysis of United States electronic health records found that people diagnosed with substance use disorder were at an increased risk for COVID-19 because of their high prevalence of life-limiting illness and social inequalities. 12 Concurrently, the COVID-19 pandemic is worsening the overdose crisis, and resulting in a higher rate of overdose deaths than pre-COVID-19.13,14
In response to the high transmissibility and mortality of COVID-19, healthcare was limited early in the pandemic to essential services. 10 These included addictions treatment and outreach, but many programs, including harm reduction services, closed or had reduced hours creating service access issues and treatment disruptions.15–17 While demand for palliative care increased during the COVID-19 pandemic,18–20 palliative care professionals were considered essential but many were required to transition to virtual care to reduce in-person encounters. 21 However, people may not have access to the necessary technologies to receive virtual care (e.g. smartphones, internet), especially those who live with severe mental disorders, poor health literacy, and experience homelessness.15,22 These public health interventions were necessary to minimize the SARS-CoV-2 transmission but had negative consequences for many people who use drugs. 23 Restricted access to mental health and substance use services likely increased the risk of relapse and overdoses through increased physical isolation and reduced connections to social support systems.15,22Physical distancing is often not possible for people experiencing homelessness, such as those who live in congregate settings (e.g. shelters), or those who depend on an (unreliable) illegal supply of drugs and need to leave their homes in order to obtain them. 24
Rationale
Given the structural inequities experienced by many people who use drugs, it is important to understand the impact of communicable disease epidemics and pandemics on this population to help compress the systemic inequities in receiving high quality palliative care. Recent knowledge syntheses suggest there is limited evidence to provide guidance for providing palliative care for this population, but these reviews did not account for epidemics and pandemics.4,25 To address this gap, we conducted a scoping review to identify and map available and emerging evidence in this area.
Review objective
This paper is part of a larger knowledge synthesis project focused on palliative care for people who use drugs during epidemics and pandemics.26,27 We conducted a preliminary search of the PubMed and Web of Science databases in May 2020 and we did not identify any reviews addressing palliative care needs for people who use substances during communicable disease outbreaks (e.g. Ebola, H1N1). Our primary objective is to answer the question, “what is known about communicable disease epidemics and pandemics, palliative care, and people who use substances?” The objective of the present manuscript is a focused analysis on findings related to equitable access, policies, and programs in palliative care for people who use drugs.
Methods
We conducted a scoping review using the Levac et al.’s six-stage framework, 28 which builds on the contributions of Arksey and O’Malley, 29 Joanna Briggs Institute, 30 and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting guidelines. 31 We published the scoping review protocol on 27 October, 2021. 26
Inclusion criteria
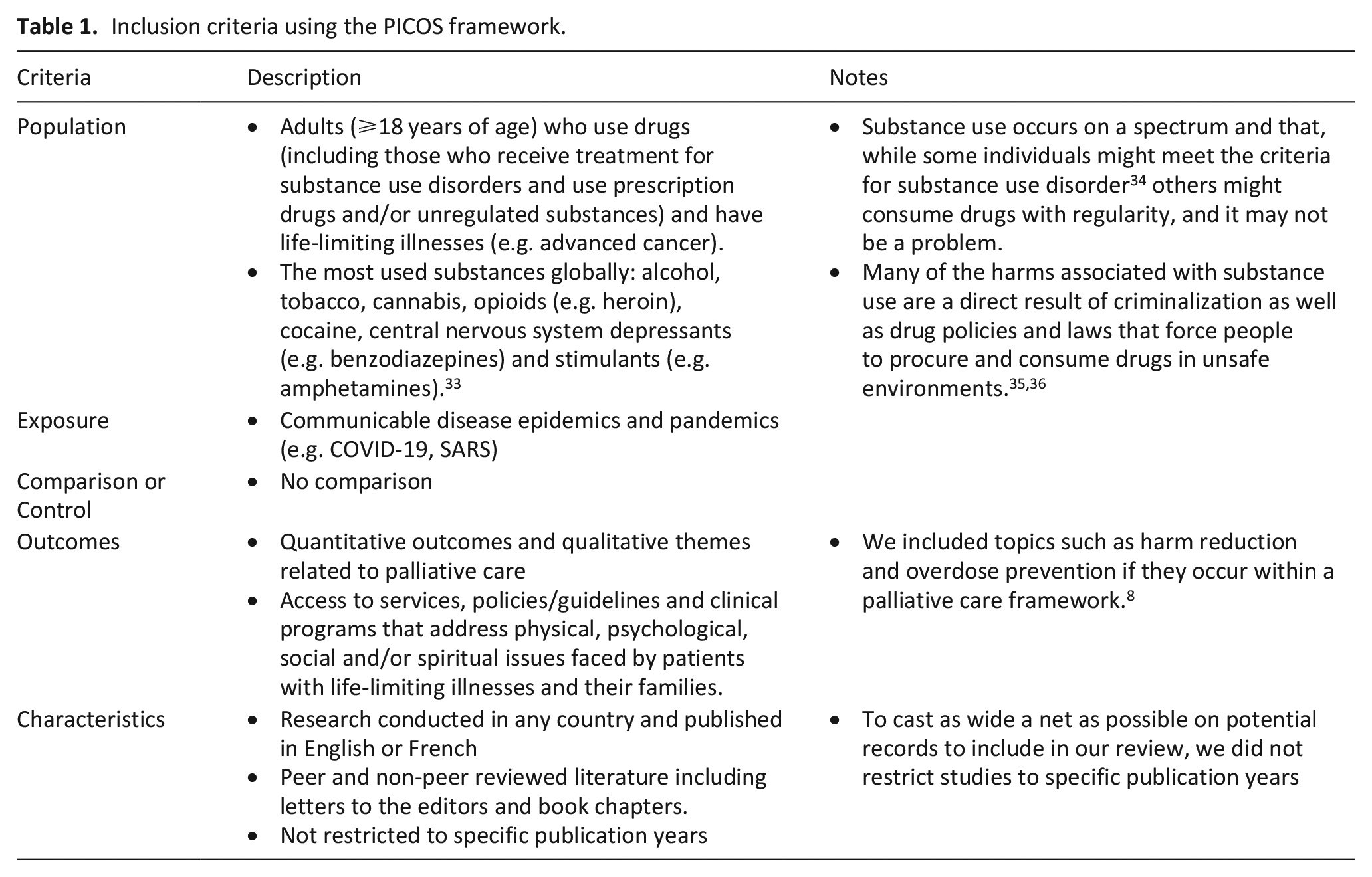
We applied the PECOS (Population, Exposure, Comparison or Control, Outcomes, and Characteristics) framework 32 to structure our eligibility criteria. Please see Table 1.
Inclusion criteria using the PICOS framework.
Information sources and search strategy
An information specialist (RF), in collaboration with our team of technical and subject matter experts, developed a comprehensive search strategy to identify studies in the following bibliographic databases: Medline ALL (Medline and Epub Ahead of Print and In-Process and Other Non-Indexed Citations), Embase Classic +Embase, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trial, PsycInfo all from the OvidSP platform, and Scopus from Elsevier, from their inception to April 2021. Each search strategy comprised a combination of controlled vocabulary terms and text words, adapting the database-specific search syntax. Where available, we used both controlled vocabulary terms and text words in the subject block structure, such as but not limited to palliative, hospice, terminal, and alternative terms in one block, communicable disease, pandemic, disaster planning and relevant synonyms in the third block. The terms in each block were combined using Boolean Operator “OR.” and three subject blocks were combined using Boolean Operator “AND.” Where applicable, we restricted the search to human studies, adults ⩾18, and English and French languages. We stored the results from the database searches in EndNote X9. 37
We conducted grey literature searches over the same timespan to identify published literature that was not indexed in the bibliographic databases. The search strategies were customized based on available searching features for each grey literature resource. We searched the following grey literature resources: TRIP medical database, Google, prominent health organizations websites (e.g. Centres for Disease Control and Prevention, Centre of Addiction and Mental Health), associations of palliative care, and public health (communicable disease). A list of the grey literature websites is shown in Supplemental Appendix 2. To identify additional relevant studies, we used reverse snowballing to screen the reference list of the included studies.
Selection of sources of evidence
We imported the records into Covidence, a web-based literature review software, which we used to detect and remove duplicates. 38 Two independent reviewers (PQD, SL) screened the title and abstracts of the remaining records according to the eligibility criteria, and then applied the same process to the full text articles. Disagreements were resolved by consulting a third reviewer (DZB or JL). We screened records with no abstract based on their title. If there were conference proceedings or abstracts without full text, we excluded these due to the limited available information. Three main reasons counted toward exclusion: wrong population (e.g. people with curative diagnoses), wrong exposure (e.g. non-communicable disease public health emergencies) and wrong outcomes (e.g. not related to palliative care). We applied the same process to the full text articles.
We imported the results identified in the grey literature searches into Google Sheets. We manually assessed the eligibility of each record by applying our PECOS framework criteria. If there were disagreements between the two reviewers, they consulted a third reviewer.
Data charting process
We developed a standardized data charting form using Google Sheets to extract the following variables: author/organization, publication year, journal, country of the corresponding author, article type (commentary/opinion article, conference/workshop, guideline, news article, program report, other), publication language, countries and settings in which studies were conducted (acute care, inpatient palliative care, long-term care, community, home care, infectious diseases clinic, palliative care clinic), populations (life-limiting diagnoses, substances used, sex and gender, age, ethnicities), target audiences (healthcare professionals, researchers, policy makers, governments), communicable diseases, and palliative care outcomes (interventions, access to services, policies/guidelines, and clinical programs).
Synthesis of results
We developed a PRISMA-ScR flow diagram to map out the review process (see Figure 1). We analyzed the quantitative data (e.g. study characteristics) using descriptive statistics and summarized them in tables and graphs. Through comparative analysis of the extracted data, we summarized the results, and then according to each palliative care outcome as described above.
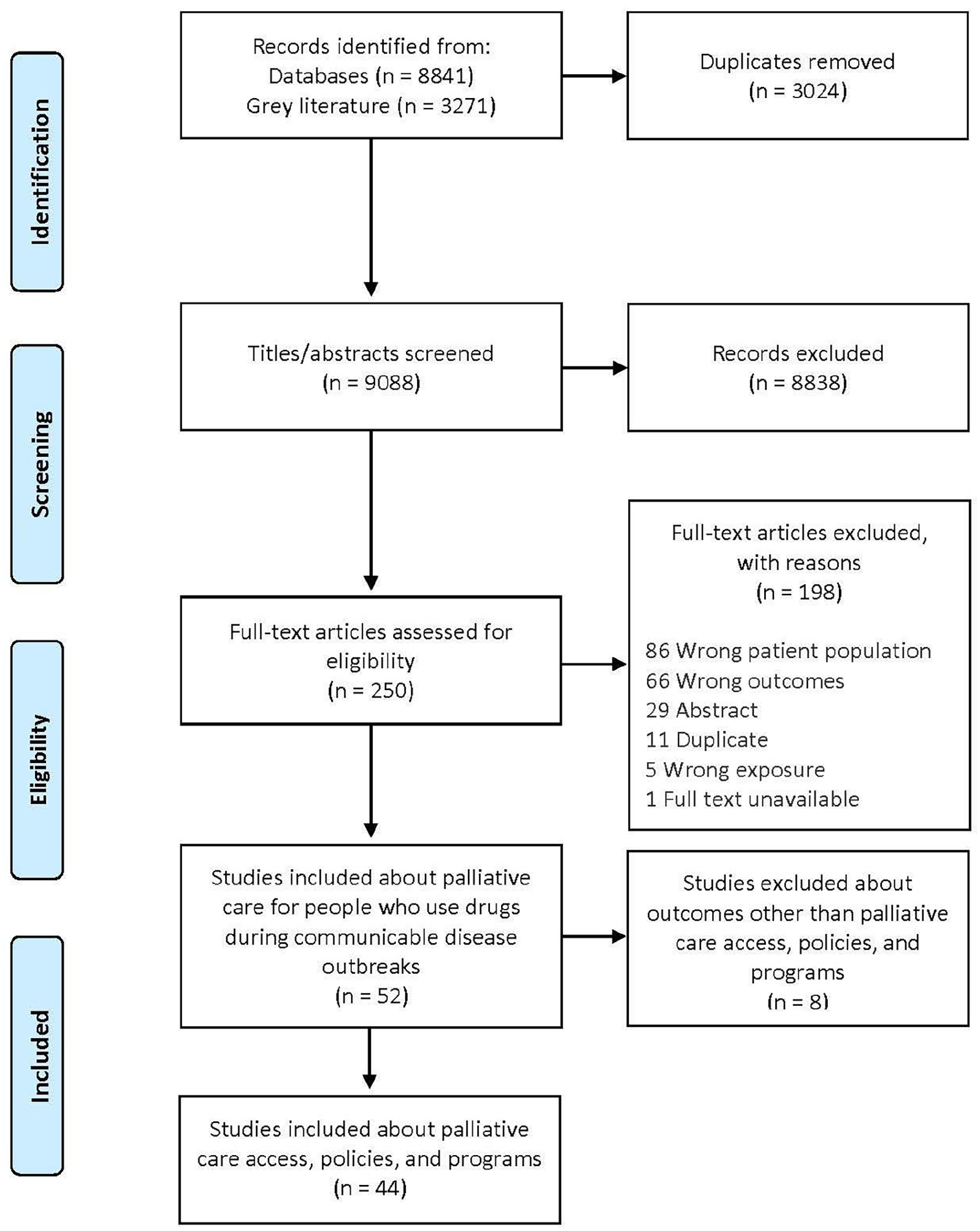
PRISMA-ScR flow diagram.
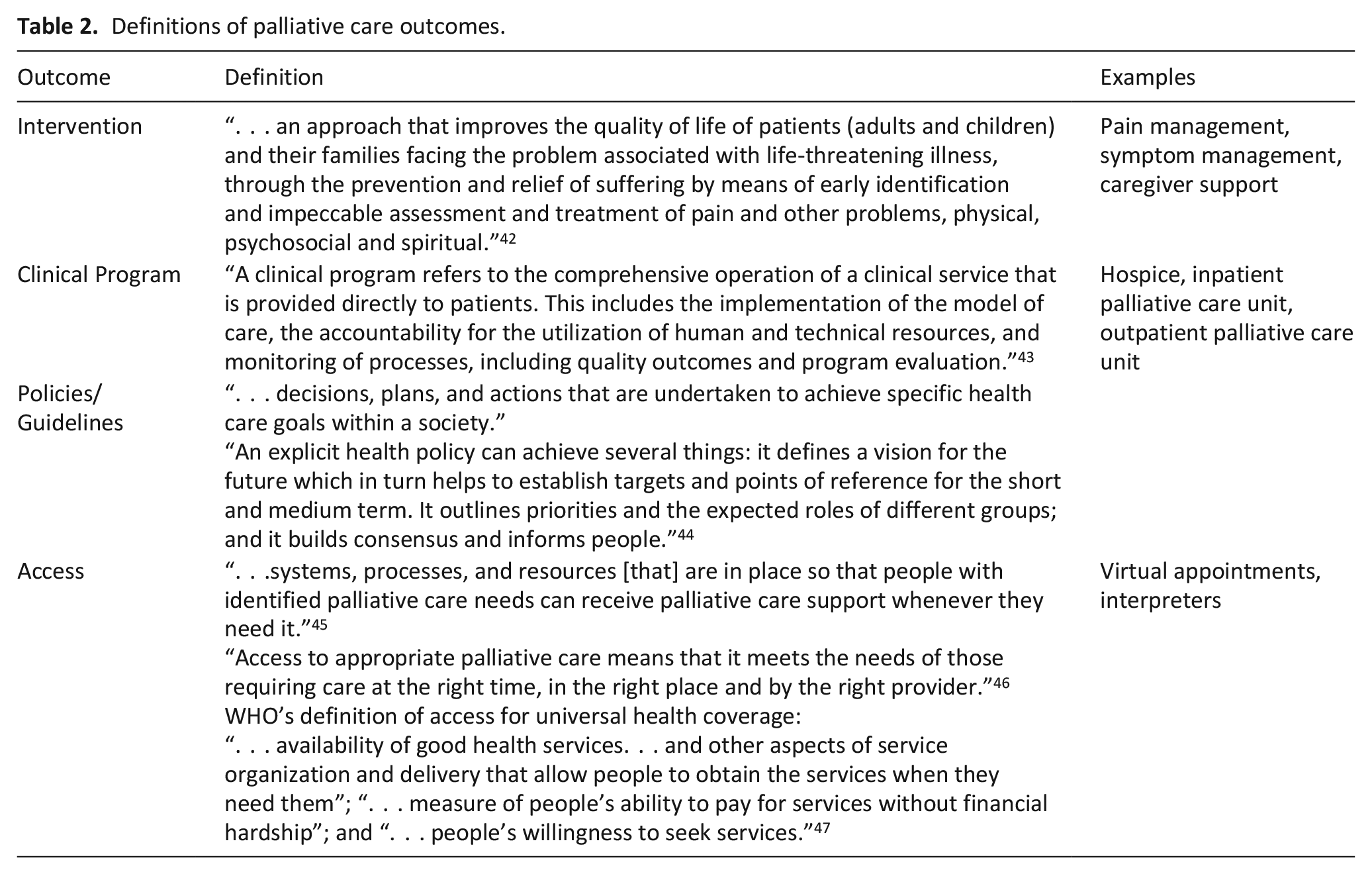
We analyzed the qualitative data thematically using a hybrid process of inductive and deductive analysis. 39 Based on the priorities of the team’s knowledge users, we developed a codebook with the following four a priori palliative care-related codes that were applied to our findings (please see Table 2). We coded each record in duplicate using the codebook and the qualitative analysis software, NVivo. 40 We used the constant comparative method 41 to inductively identify additional codes that capture common themes, sub-themes where relevant, and differences within and between the records. The sub-themes were not identified a priori.
Definitions of palliative care outcomes.
Results
From our database search from inception to April 2021, we imported 9088 records (5817 from electronic databases and 3271 from grey literature) obtained from the database searches. Forty-four records met our inclusion criteria. Some records were counted in more than one theme. The most common records were research articles (n = 16; 36.4%) and guidelines (n = 16; 36.4%). Healthcare professionals represented 84.1% (n = 37) of the target audience, and 18 (40.9%) of the records came from the United States. HIV (n = 36; 81.8%) was the most common communicable disease, followed by hepatitis (n = 10; 22.7%), COVID-19 (n = 9; 20.5%), and tuberculosis (TB) (n = 9; 20.5%). The community (including home; n = 14 (31.8%) and palliative care unit n = 14 (31.8%) were the most common settings, followed by a clinic (not infectious disease or palliative; n = 13; 29.5%), and acute care (n = 12; 27.3%). The most common life-limiting illness was AIDS (n = 36; 81.8%). Injection drug use was identified in 22 (50.0%) of the articles, followed by alcohol (n = 19; 43.2%) and opioids (n = 19; 43.2%). The most documented racial category of patients was Black (n = 16; 36.4%). For a complete summary of characteristics of records included in our study see Table 3. For the complete list of included records, please see Table 4.
Summary of characteristics of included studies (n = 44).
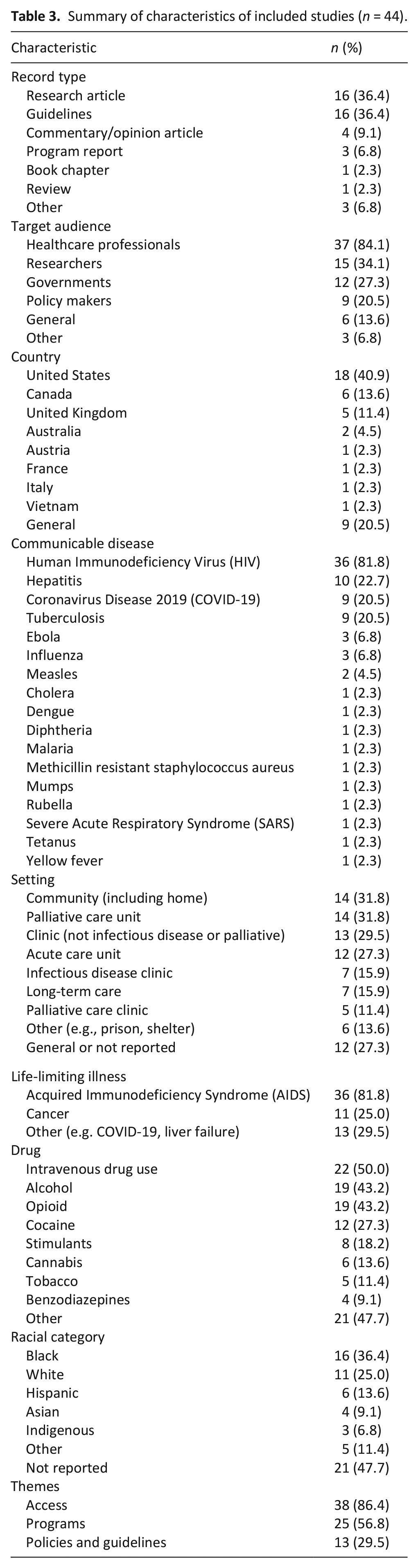
Table of included records.
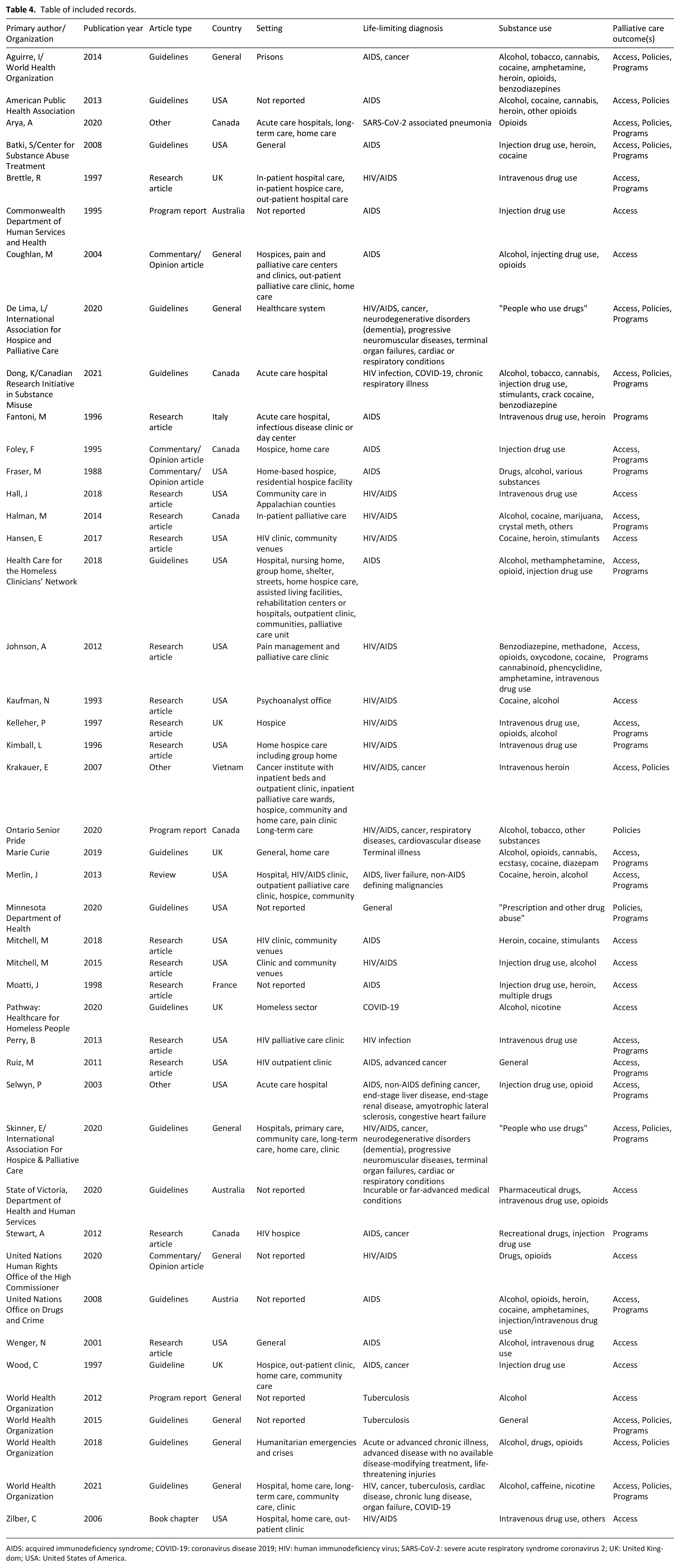
AIDS: acquired immunodeficiency syndrome; COVID-19: coronavirus disease 2019; HIV: human immunodeficiency virus; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2; UK: United Kingdom; USA: United States of America.
Theme 1: Access
Thirty-eight records (86.4%) described access to palliative care by people who use drugs during communicable disease outbreaks. We identified additional sub-themes of enablers and barriers to accessing palliative care.
Enablers (n = 8)
During communicable disease outbreaks, policies can be implemented to ensure that people who use drugs have access to palliative care in all settings, including shelters,22,48 and can follow public health measures implemented in response to outbreaks. For example, during the COVID-19 pandemic, physical distancing, and quarantine (or self-isolation) are key public health measures that can help reduce the spread of COVID-19. The Government of Canada released information about how to care for a person with COVID-19 at home, which was recommended to be applied to any location that people identify as “home.” 22 If people are unable to isolate themselves at home, safe accommodations should be provided. If this is not possible, people should at least be provided access to basic sanitary supplies for hygiene and infection prevention purposes (e.g. handwashing, masks, toilets). 49 Policies can also be established to increase prescriber access to controlled substances (e.g. opioids) for palliative care. In April 2020, the Australian government issued a public health emergency order that removed the requirement that medical practitioners, nurse practitioners and pharmacists need to check a prescription monitoring tool 50 before prescribing and supplying controlled substances for people with life-limiting illnesses. 51 Additionally as of April 2020, Australian physicians and nurse practitioners were no longer required to obtain a treatment permit to prescribe controlled substances to people who are “not drug dependent” and “drug-dependent” people who are confined (e.g. people who are incarcerated) or not personally managing their medications (e.g. hospital inpatient). 51
Specific interventions can be implemented to overcome structural barriers to accessing palliative care and other healthcare services. For people with life-limiting illnesses who experience homelessness, substance use, and mental illness, shelter-based palliative care can be effective and reduce overall healthcare costs. 52 During the COVID-19 pandemic, some countries allocated funding to buy tablets for hostels, shelters and shared houses. 49 These tablets are used by palliative care coordinators to liaise more efficiently and safely with services users and staff. 49
Barriers (n = 16)
Barriers that prevent people who use drugs from accessing palliative care were further subcategorized into the following sub-themes: stigma, structural inequity, restricted access to opioids and other psychoactive substances, and organizational barriers.
Stigma (n = 14)
Studies about TB 48 and HIV epidemics identified that stigma related to substance use prevents access to and delivery of healthcare,48,53–56 including management of pain57,58 and other symptoms. 59 Healthcare professionals, including caregivers for patients at home, 54 reported that pain management was challenging for people with substance use disorders because they were concerned about contributing to the patients’ substance use disorder, diversion, and serving as a “source” for unregulated substance use. 57 An article about palliative care for people living with HIV/AIDS in Asia identified that healthcare staff rarely inquired or assessed patients’ pain. If patients complained of pain, they were labeled as “difficult,” “demanding” or “drug seeking.” 53
Studies reported that HIV infections were often associated with assumptions about sexual behavior and substance use, specifically homosexuality and injection drug use, and people were often judged negatively and rejected by others.60–62 Due to fears of being stigmatized by healthcare professionals 59 and past traumatic medical experiences, 55 some people with HIV did not want to access healthcare. Structural stigma through policies, such as zero tolerance for drug and alcohol use, also deterred people from accessing health care during HIV epidemics. 59 These forms of stigma contribute to development of shame of living with HIV. 60 A Canadian study reported that people with HIV/AIDS traveled from their smaller communities of origin to a large city to receive medical care to conceal their HIV status. 56 The concerns about transmitting HIV by sex or substance use made many people with HIV and their families uncomfortable with disclosure to others. 56 These interacting forms of stigma result in challenges with advance care planning 63 and overall poor quality health care for people with HIV.
Structural inequity (n = 11)
People experience structural vulnerability when densely woven patterns of disadvantage prevent them from accessing healthcare, including palliative care,49,59,64,65 and increase their risk of negative health outcomes. This population comprises people who use drugs49,66 and other marginalized populations, such as sexual and gender minorities,49,66 people who are incarcerated 66 and those experiencing homelessness, 49 poverty,64,67 mental illnesses,49,68,69 language barriers,64,66 historical trauma, 64 and disabilities. 49 Sometimes these identities intersect and intensify the inequities. These populations are less likely to have social support59,70 and to self-advocate, 64 and can be disadvantaged when decisions are made about resource allocation. 64 During communicable disease outbreaks, strain on the healthcare system can worsen existing inequities. 64 Access to visits and support from healthcare and social care professionals can also be restricted during outbreaks, such as during the COVID-19 pandemic. 49 The literature suggests that palliative care professionals may not always have the tools and resources they need to offer better support to people experiencing structural vulnerability. 64
Criminalization of people who use drugs contributes to structural inequities and was a major driver of the HIV epidemic. 71 Fear of criminal penalties deterred people with HIV who used drugs from using health services and treatment, and increased their risk of violence, discrimination and serious illness. 71 Overuse of incarceration and pretrial detention of people who use drugs contributed to the high prevalence of HIV and hepatitis among those who were incarcerated. 71 Poor prison conditions and management along with lack of access to preventative, curative and palliative care resulted in increased risk of transmission of bloodborne infections. 72 Further, criminal prohibitions impeded the use of medications for research and prevented patients with HIV from accessing drugs for palliative care. 71
Restricted access to opioids and other psychoactive substances (n = 8)
Many countries have strict regulations on importing, manufacturing and licensing of opioids and psychoactive substances such as benzodiazepines due to the risks of addiction and drug diversion.53,73,74 During communicable disease outbreaks, the World Health Organization (WHO), United Nations and International Narcotic Control Board recommend that restrictions on export, transportation, storage and provision of controlled substances be removed to ensure that they are available for symptom management.6,67 A model guideline for simplified control procedures is available in the WHO guide, “Integrating palliative care and symptom relief into the response to humanitarian emergencies and crises.” 67 Further, the International Narcotic Control Board is mandated to support member states to ensure that controlled substances are available for medical and scientific purposes, including facilitating export and import of controlled substances for humanitarian emergencies.49,67
Organizational barriers (n = 3)
People who use drugs encounter unique challenges when trying to access palliative care in healthcare organizations, particularly if they have a comorbid mental disorder.55,69 When faced with end-of-life care decisions, people may resume their substance use, which can affect their capacity to participate in treatment plans.54,55 Some healthcare organizations do not permit substance use on the premises, which prevents access to services. 59 These organizations may not have the appropriate resources and staff to provide care for patients with complex medical and social conditions. 54 For example, a practice document described a case of a 48-year-old man with AIDS, alcohol, and methamphetamine use disorders and severe post-traumatic stress disorder and neurocognitive disorders. 55 After being admitted for only 6 h, a hospice discharged him to the street because they did not have the security or intensive one-on-one support needed to care for him after he became confused and “lashed out” at a volunteer. 55 Several days later, the man was admitted to an acute care hospital and died of an infection. 55
Theme 2: Programs
Twenty-five records (56.8%) described palliative care programs for our target population and context. Several records identified that the intersections of substance use, psychiatric disorders, and social inequities in health requires clinical programs to use a collaborative approach when providing palliative care to people with life-limiting illnesses, especially during communicable disease outbreaks.48,52,54,57,65,68,69,75,76 Injecting drugs in unsafe environments place those injecting at risk of acquiring blood-borne viruses (e.g. HIV) 59 and people experiencing structural vulnerability may not be able to implement public health measures in response to communicable disease outbreaks (e.g. physical distancing). 22 We identified practical strategies that programs can use to help reduce health inequities including service coordination, facilitating transitions in care and developing reasonable, feasible care plans that meet patients where they are situated.52,55,68 One document also suggested that emotional support and palliative care training should be provided for staff and organizations who provide care for people experiencing homelessness. 49
The literature suggests that community-based services, including hospices, can help loved ones remain together, avoid acute care hospitalization and, potentially, reduce healthcare costs.54,77 Homecare teams can provide access to nursing and services such as social work, physical therapy, occupational therapy, respiratory therapy, and home health aides. 54 However, patients may encounter challenges with receiving care at home. Homecare staff may have limited experience with managing mental health and substance use conditions. 54 Loss of income from either the patient or their caregiver can create challenges with housing, health insurance, nutrition, and medications. 54 Palliative care units are an alternative to remaining at home for patients with HIV at the end of their lives but they may not be compatible with the needs of structurally disadvantaged people living with HIV/AIDS. 54
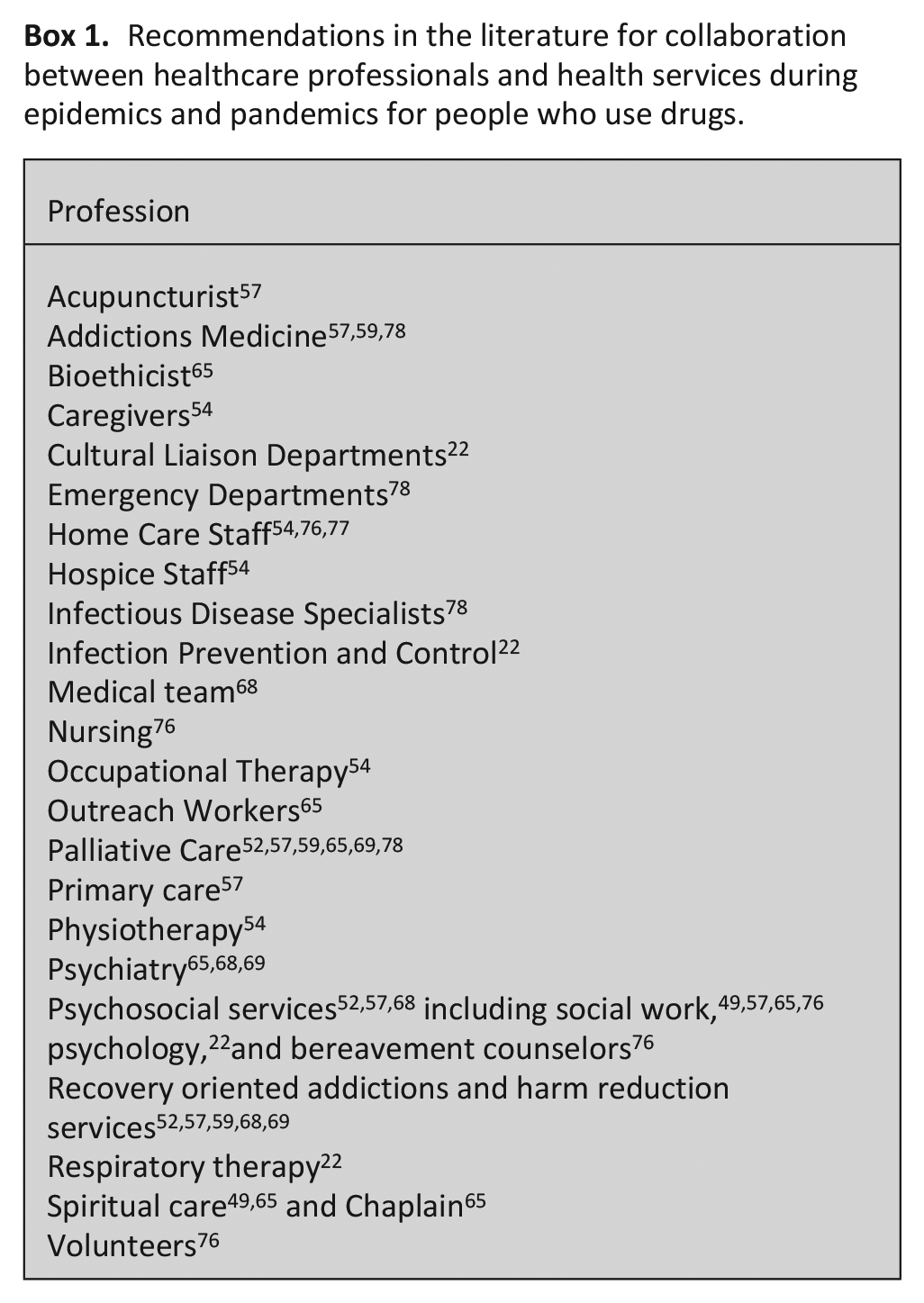
The literature suggests that interprofessional and inter-organizational collaboration is critical for providing equitable care for people who use drugs during epidemics and pandemics (see Box 1).54,65 We identified prior training and experience with HIV treatment, palliative care and substance use are important when establishing teams and providing care. 54 Senior leadership support can help establish the credibility of the program and assist with connections with other services.65,76 For patients on opioid agonist treatment, the literature suggests medical teams should collaborate with addictions medicine (ideally the patient’s opioid agonist prescriber) to determine whether the treatment can be modified to be dosed more frequently, changed to a different opioid or if other medications should be added. 22 For patients who are socially isolated, chaplaincy and social work involvement can help meet their psychosocial, spiritual, religious and existential needs. 49
Recommendations in the literature for collaboration between healthcare professionals and health services during epidemics and pandemics for people who use drugs.
Theme 3: Policies and guidelines
We identified 13 records (29.5%) about palliative care policies and guidelines. Given the increased demand for palliative care during communicable disease outbreaks, the literature suggests palliative care should be integrated into public health response efforts.49,72,79 The literature recommends that people should have equitable access to palliative care in all settings including shelters, prisons and any location that patients identify as their homes.49,67,72,79 Healthcare professionals should create triage systems to determine which patients should receive in-person palliative care consultations and which ones can be seen virtually. 64 The literature suggests that frameworks be developed to guide decision making in situations where resuscitative or life-sustaining treatments may need to be stopped, with a focus on patients’ comfort, dignity and psychosocial, spiritual, and cultural needs. 54 One document suggested that patient requests for medical assistance in dying should not affect the palliative care they receive. 22
The literature recommends that healthcare professionals plan to ensure that they have adequate supplies of palliative care medications.64,79 Medication availability in prisons is often severely restricted and determined by prison wardens, rather than healthcare professionals or patient needs. 49 Stockpiling medications may be limited by storage and management constraints, and safeguards are needed to minimize risk of unregulated use and diversion. However, these medications are essential, and their distribution should be considered in crisis response planning to meet palliative care needs. 79
Several records indicated that healthcare policies for people with life-limiting illnesses who use drugs should be flexible, trauma-informed and patient-centered, and ensure that patients have low barrier access to resources and comprehensive services where they can form trusting relationships with healthcare professionals.48,49,68 The literature suggests that “culturally competent” systems of care be developed using strategies that minimize culture clashes between healthcare professionals and patients, such as expecting that there will be differences in beliefs about death and dying. 54 Efforts should also be made to include patients with multi-morbidity in research. Guidelines based on randomized control trials about healthier patients with communicable diseases (e.g. HIV) may not account for the complex care needs of the most vulnerable patients. 68
Discussion
Main findings of the study
The aim of our scoping review was to identify and map the evidence on palliative care for people who use drugs during communicable disease epidemics and pandemics. We identified 44 records related to palliative care access, programs, and policies and guidelines; we summarized major themes in this literature and provided some preliminary insights into key challenges for the delivery of equitable palliative care. Most records were from high income settings, such as the United States, Canada, and the United Kingdom, and focused on HIV/AIDS. A few records addressed pandemics caused by aerosol transmission such as COVID-19. Multi-level stigma remains quotidian for people who use drugs, which manifests in barriers to accessing care and worse health outcomes. 80 The importance of collaborative multidisciplinary care was a common thread throughout the included records, as mainstream healthcare and palliative care models are not necessarily designed to meet the unique palliative care needs of structurally vulnerable populations such as people who use drugs. 8
Our review found that there is a paucity of guidance for healthcare professionals and health policy on considerations for palliative care access, programs, and policies and guidelines in epidemics and pandemics beyond the HIV/AIDS context, although the COVID-19 pandemic has been a catalyst for some emerging guidance. The inequities faced by people who use drugs can be exacerbated in epidemics and pandemics when there is resource scarcity and restrictions are placed on accessing essential in-person services.
Our findings suggest that health systems consider proactively developing a “palliative care surge plan” 81 for during epidemic and pandemic planning that is inclusive of evidence-based substance use approaches. Arya et al. 64 and Downar and Seccareccia 81 propose four critical elements for pandemic palliative care: (1) Stuff (i.e. medication, equipment, (2) Staff (i.e. staff with palliative care expertise), (3) Space (i.e. hospitals and other healthcare centers should provide dedicated spaces for supportive care), and (4) Systems (i.e. triage system that identifies patients at greatest need of direct specialist care). These elements can be extended to people who use drugs, grounded in our review findings. In this context, “Stuff” refers to the essential medications required to provide palliative care to large numbers of patients, but it also refers to continuation with opioid agonist therapies, provision of safe supply of pharmaceutical grade drugs,24,82 and abandoning abstinence-only policies. 8 For “Staff,” this might mean a multi-disciplinary team with expertise in palliative care, harm reduction, and substance use, or seamless communication across teams. In pre-pandemic planning, this creates an opportunity for focused education, training, and capacity building for hospital- and community-based clinicians in providing high quality compassionate trauma-informed care 83 as well as building relationships within and across services and sectors.4,81 Regarding “Space,” proactive planning can include dedicated spaces that integrate harm reduction services such as supervised consumption sites within palliative care contexts. 84 In some cases, these spaces may need to be mobile to meet people who are receiving palliative care but not admitted to a structure like a hospice. Finally, for “Systems,” a triage framework that helps identify people who use drugs who are in greatest need of specialist palliative care can help improve equitable access as well as use limited public resources more efficiently and effectively.
Limitations of the study
We restricted our studies to English and French languages due to limited available resources and the rapidly evolving literature of our subject matter. This review does not include literature published in databases and grey literature after April 2021, so there were likely additional records published that our analysis did not capture. We addressed this limitation by integrating literature published after the search date within our Introductory and Discussion sections. Most records that met our inclusion criteria were published about people who use drugs in the context of the HIV epidemic in community and inpatient settings located in high-income countries. The main drugs consumed were alcohol and opioids. While 36.4% (n = 16) of our sample identified as Black, almost half of our sample (n = 21; 47.7%) did not report any racial category, which limits our understanding of the needs of specific racialized groups. The generalizability of our findings to other communicable diseases outbreaks, resource limited settings in low and middle-income countries, and drugs beyond opioids and alcohol should be approached with caution.
What this study adds
This is the first scoping review, to our knowledge, that explores palliative care for people who use drugs during communicable disease epidemics and pandemics with a focus on access, programs, and policies and guidelines. Our findings build on past research that seeks to integrate the premises of health equity within palliative care. The findings from our review provides accessible and relevant evidence for healthcare professionals and decision-makers (e.g. policy makers) that can be applied to the COVID-19 pandemic response efforts and help plan for future epidemics and pandemics.
Our findings point to parallels with other epidemics, such as HIV/AIDS. Similar to the HIV epidemic, COVID-19 disproportionately impacts communities who face profound structural disadvantages, such as people who use drugs, and are also highly stigmatized.85,86 Racism is a fundamental cause of inequities in health, 87 and Black populations experience a disproportionately higher burden from HIV/AIDS and COVID-19.88,89 Indeed, given the focus of our review, it is not surprising that the most frequently occurring racialized category of patients in our sample was Black.
Given that our findings point to how intersecting structural determinants of health intensify during epidemic and pandemic periods, there is much to learn from scholars who have applied syndemic theory to COVID-19 and HIV/AIDS research, including those focused on the complex ways in which structural and systemic factors and health conditions can intensify disease progression and social outcomes. 90 Indeed, syndemic thinking has been used to describe the COVID-19 pandemic and how COVID-19 clusters with chronic health inequities, exacerbates epidemics in enabling environments, and tracks social disadvantage.24,91 Applying a syndemic lens to palliative care for people who use drugs in epidemics and pandemics, may help generate new knowledge that can shift the policy focus on the delivery of palliative care services as a priority and instead on the densely woven patterns of disadvantage more broadly that limit access and create inequitable health outcomes for this population.
Conclusions
Health-related inequities are magnified when people who use drugs with life-limiting illnesses require high quality palliative care during epidemics and pandemics. Our findings can support decision-makers in helping to minimize inequities in palliative care access for this population and enhance population health outcomes, especially during times of health system strain and resource scarcity. Given the high morbidity and mortality associated with substance use disorders, the negative impacts of the social and structural determinants of health, and the resulting increased risk during communicable disease epidemics and pandemics, people who use drugs should be a priority population to receive palliative care. More research is needed about palliative care access, policies, and programs and guidelines for people who use drugs during communicable disease epidemics and pandemic beyond the HIV/AIDS context.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221143153 – Supplemental material for Palliative care for people who use drugs during communicable disease epidemics and pandemics: A scoping review on access, policies, and programs and guidelines
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221143153 for Palliative care for people who use drugs during communicable disease epidemics and pandemics: A scoping review on access, policies, and programs and guidelines by Daniel Z Buchman, Samantha Lo, Philip Ding, Naheed Dosani, Rouhi Fazelzad, Andrea D Furlan, Sarina R Isenberg, Sheryl Spithoff, Alissa Tedesco, Camilla Zimmermann and Jenny Lau in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163221143153 – Supplemental material for Palliative care for people who use drugs during communicable disease epidemics and pandemics: A scoping review on access, policies, and programs and guidelines
Supplemental material, sj-pdf-2-pmj-10.1177_02692163221143153 for Palliative care for people who use drugs during communicable disease epidemics and pandemics: A scoping review on access, policies, and programs and guidelines by Daniel Z Buchman, Samantha Lo, Philip Ding, Naheed Dosani, Rouhi Fazelzad, Andrea D Furlan, Sarina R Isenberg, Sheryl Spithoff, Alissa Tedesco, Camilla Zimmermann and Jenny Lau in Palliative Medicine
Footnotes
Acknowledgements
Thank you to Rebecca Bagnarol for helpful assistance with manuscript formatting.
Author contributions
Daniel Z Buchman: Made a substantial contribution to the design of the work, as well as acquisition, analysis, and interpretation of data; drafted the article; takes public responsibility for appropriate portions of the content; approved the version to be submitted for publication. Philip Q Ding: Contributed to acquisition, analysis, and interpretation of data; critically reviewed drafts of the article; approved the version to be submitted for publication. Naheed Dosani: Contributed to writing and review of drafts of the article, approved the final version submitted for publication, will be involved in dissemination of these findings to media and social media. Samantha Lo: Contributed to acquisition, analysis, and interpretation of data; critically reviewed drafts of the article; approved the version to be submitted for publication. Rouhi Fazelzad: Contributed to formulating the research question, designing and executing literature search strategies, writing the information sources and search strategy section, and approved the final version submitted for publication. Andrea D Furlan: Contributed to obtaining funds for this project, design, interpretation of data, takes public responsibility for appropriate portions of the content, approved the final version submitted for publication, and will be involved in dissemination of these findings to media and social media. Sarina R Isenberg: Contributed to study design, data acquisition and interpretation; critically reviewed drafts of the article. approved final version to be submitted for publication and take public responsibility for appropriate portions of the content. Sheryl Spithoff: Contributed to study design, data acquisition and interpretation; critically reviewed drafts of the article. approved final version to be submitted for publication and take public responsibility for appropriate portions of the content. Alissa Tedesco: Contributed to study interpretation, writing and critically reviewing drafts of the article, approved the final version submitted for publication, will be involved in dissemination of these findings. Camilla Zimmermann: Contributed to study design and data interpretation; critically reviewed drafts of the article; approved final version to be submitted for publication and takes public responsibility for appropriate portions of the content. Jenny Lau: Made a substantial contribution to the design of the work, as well as acquisition, analysis, and interpretation of data; drafted the article; takes public responsibility for appropriate portions of the content; approved the version to be submitted for publication.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrea Furlan receives an unrestricted educational grant to maintain the online Opioid self-assessment program from the Canadian Generic Pharmaceutical Association (CGPA). The funding organization had no role in the preparation, review approval, or data analyses of the course content. Dr. Furlan is the inventor of the App Opioid Manager. The App is owned by UHN, the hospital where Dr. Furlan works and Dr. Furlan does not receive any profits from the App sales. Dr. Furlan has a YouTube monetized channel and receives payment for advertisements on the channel. There are some videos related to opioids in her channel. All other authors report no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institute of Health Research grant number CMS – 171746, awarded to JL and DZB.
Research ethics and patient consent
Not required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.