
Abstract
Background:
Patient-reported outcome measures have the potential to improve outcomes, quality, and effectiveness of care. Digital use of patient-reported outcome measures could be an option to foster implementation in palliative care. The Palli-MONITOR study focused on developing and testing an electronic patient-reported outcome measure in specialised palliative home care. As part of this study, we examined setting-specific challenges for the development of the measure.
Aim:
We aimed to identify and explore challenges for the development of electronic patient-reported outcome measures as standardised assessment in specialised palliative home care.
Design:
Qualitative approach with semi-structured interviews and focus groups. Data were thematically analysed using the framework method.
Setting/Participants:
Patients and professionals from five German palliative home care teams.
Results:
Patients described potential problems in using electronic questionnaires due to their deteriorating health. Answering the electronic questionnaire encouraged patients to reflect on their current palliative situation, which was partly perceived as burdensome. Identified concerns and questions regarding the future roll-out of electronic patient-reported outcome measurement addressed the process of receiving and using the provided information in clinical care routine. Challenging factors on organisational and structural level were the potential undermining of the established 24-h emergency call system and the potential use for patients.
Conclusions:
Our results provide a multifaceted picture of challenges developing electronic systems for patient-reported outcome measurement in palliative home care on the individual and organisational level. The study underpins the benefit of stakeholder involvement creating digital health innovations and emphasises the importance to therefore mind setting specific culture.
Use of patient-reported outcome measurement in routine care has potential to enhance patients’ outcomes, as well as quality and effectiveness of care
Implementation of electronic patient-reported outcome measurement in palliative care is challenging and development requires integration of field specific aspects
German specialised palliative home care varies broadly regarding clinical care routines and organisational structures
At the patient level, challenges for the use of electronic patient-reported outcome measurement were identified in terms of patients’ current health status, their familiarity in using internet-enabled devices and the design of the electronic patient-reported outcome measurement instrument.
To implement the use of electronic patient-reported outcome measurement in palliative home care, it is necessary to understand in which way health care professionals are able to receive and react to the information received via electronic patient-reported outcome measurements.
Developing an electronic patient-reported outcome measurement tool for palliative home care requires a concept that supports existing organisational structures.
The development of digital health interventions such as electronic patient-reported outcome measurement must take the specific cultures of each setting into account.
This study underpins the importance of including stakeholders as experts of their life-worlds in the development of new health technologies.
Background
The use of patient-reported outcome measures (PROMs) may have the potential to enhance effectiveness and quality of care by improving communication between patient and health care professionals, symptom monitoring, identification of unknown palliative needs and patient empowerment.1–5 Despite official recommendations, the routine use of PROMs in palliative care is still insufficient.4,6 A challenge for successful implementation of PROMs is to develop the tool according to setting specific requirements and conditions. 7 Additional barriers are health care professionals’ concerns of being assessed by using the measures or their resistance against change. 7 It is known from previous studies in German specialised palliative home care and from other clinical disciplines that a digital realisation of PROMs (ePROMs) is an option to overcome health care professionals’ fear of additional workload due to PROM implementation.8,9 However, health care professionals suspect digital and standardised PROMs to cause a loss of personal contact as well as an inadequate/insufficient and one-dimensional symptom assessment. 10 Nevertheless, digital PROMs are increasingly researched and integrated in the development of care models. The European MyPal project is currently developing a digital patient-reported outcome system to support palliative care for paediatric and adult patients with blood cancer. 11 In Germany, the project MySUPPORT aims to implement PROMs in different palliative care settings via a web-based application. 10 However, little is known about the use of ePROMs in the community setting and in patients with complex symptom burden in home care. The project Palli-MONITOR focuses on the development and feasibility of an ePROM/electronic version of the Integrated Palliative Care Outcome Scale (eIPOS) in German specialised palliative home care. 12 For the suitability of ePROMs in this setting, user friendliness on the patient-level is paramount as they have to deal with illness-related limitations. 5 The decentral structures and high heterogeneity of German specialised palliative home care may include even more unrecognised challenges regarding the development of an ePROM for this setting. 13 In addition to the challenges on the structural and organisational level, the perspectives of stakeholders must also be considered for a sustainable implementation of ePROMs. 14 Therefore, the aim of this study was to identify and explore challenges in developing a feasible ePROM in the particular setting of specialised palliative home care prior to the roll-out.
Methods
Study design
We conducted a multi-centre qualitative interview and focus group study. According to social constructivist theory, we understand the world to be dynamic and socially constructed. As individuals’ perspective of reality is shaped by their experiences and views, we consider the interpretative paradigm as an appropriate philosophical base exploring challenges developing health care interventions.14,15 Reporting of this study is based on the COREQ Checklist. 16
Intervention
The study is part of the project Palli-MONITOR, a multicentre, sequential mixed-methods, two-phase development and feasibility study (following the MRC framework: MRC-phase I), aiming to pilot the implementation of an ePROM system in five participating palliative home care teams (trial registration: ClinicalTrials.gov NCT03879668). 12 IPOS is an internationally tested and widely used patient and proxy questionnaire for measuring palliative symptom burden and concerns of patients with advanced disease, asking in 17 items about the impact of physical, emotional, spiritual and practical issues on patients and their families. 17 The electronic version used in this study (eIPOS) was provided via an existing app/web-app for ePROM. During an introductory visit, the patients learned how to use eIPOS on their own web-enabled device, supported by the researcher (IBF), if necessary. Patients received patient-individual codes, and instructed to visit a website for the eIPOS, completing it 1–2 times a week for at least 2 weeks. They could choose between an overview version of the whole questionnaire or presentation of single questions (one question displayed per slide). As the objective of this sub-study was to understand stakeholder perspectives on the planned ePROM procedure, the electronic system was not set up to forward data in patient records and entered values were not forwarded to the clinical team at that time. Patients were repeatedly and at the end of each completed eIPOS made aware that the specialist palliative home care team will not receive the entered information.
Setting
The study was conducted in five specialised palliative home care teams in Bavaria, Germany. Two of the teams were located in an urban and two in rural regions, one team was located in a mixed urban-rural region. None of the teams used PROMs as standardised assessment at the time of data collection.
Population
Patient interviews: Inclusion criteria were (i) currently receiving palliative home care by one of the participating teams, (ii) not too distressed or ill to participate in the study (assessed by the clinical team), (iii) sufficiently fluent in German, and (iv) the use of an own web-enabled device.
Focus Groups with health care professionals: Participation was possible for (i) physicians and nurses working in the participating teams and (ii) being sufficiently fluent in German.
Recruitment and sampling
Patient interviews: Patients were recruited from the participating teams and purposively sampled according to the following criteria: age (−60/ 60–75/ 75+), sex (f/m/d), region (urban/urban-rural/rural), technical experience (beginner/advanced; assessed by the recruiting health care professionals).
Focus Groups with health care professionals: Participants were recruited in the participating teams, purposively sampled with the following criteria: profession (nurse/physician), sex, and region of their home care team.
All participants provided written informed consent.
Data collection
Patient Interviews: Impressions from the introductory visit regarding participants’ use of internet-based devices or first reactions on the eIPOS were captured in field notes. Participants completed eIPOS repeatedly in a 1–2 weeks test phase and afterwards reported their experiences in a semi-structured interview. Interviews were conducted face-to-face (by IBF) in the participants’ home. To avoid response bias, the patient and the interviewer were preferably alone. However, considering the potential vulnerability of the interviewee, the participant could also choose a family carer to be present during the interview.
The interview guide covered questions on patients’ experiences testing the eIPOS regarding preferred frequency of eIPOS-use, technical challenges, handling of the device in relation to the patient’s condition; impact of completing eIPOS on patients’ emotional state, and opinion about the current design of eIPOS. Discussions with health care professionals from the participating teams and researchers’ impressions (IBF, AB) from field observations during their site visits supported the development of the interview guide. Additional methodological experts/researchers and a patient and public involvement (PPI) group supported its further development. We assumed to reach data saturation with 20 interviews, as this number would allow covering the scope of our purposeful sampling, considering criteria of age and sex of the participants, as well as the region (urban/rural) of the responsible SHPC-team.
Focus Groups with health care professionals: Due to geographical distances between some of the teams, we planned to conduct two focus groups in two different regions. One site was chosen to ensure short travel for health care professionals of the urban teams, the other focus group was located to be reached easily for health care professionals of the rural teams.
As the participants did not have any own experience with eIPOS at the time of the focus groups, a short input illustrated the basic idea of eIPOS and its conceivable implementation in clinical practice. The focus group guide covered questions on possible challenges, potentials, and acceptance of electronic monitoring of patient reported palliative care needs in specialised palliative home care.
Interviews and focus groups were audio-recorded and transcribed verbatim using anonymisation by a professional transcription office. Additionally, the researcher (IBF) noted for each interview and focus group impressions of the recorded situation and relevant information expressed outside the audio recording in postscripts.
Data analysis
The data corpus included the transcripts of interviews and focus groups, postscripts, and field notes covering the introductory patient’s visit. We conducted thematic analysis using the framework approach. 18 Our framework was developed following a deductive-inductive approach. Initial categories based on former knowledge and the research question were deductively applied to the data corpus, followed by an inductive identification of additional categories and subthemes. 19 Two researchers (IBF, AB) tested the primary matrix considering inter-coder-reliability and subsequently adapted the structure of the framework. Each step of the analysis process was accompanied by regular multidisciplinary team meetings. MAXQDA® v.2018.2 was used for data management.
Ethics
Ethical approval was obtained from the Research Ethics Committee of the Ludwig-Maximilians-University Munich (Ref: 18-815). With respect to the partly very vulnerable sample (interviews with patients), we considered ethical aspects regularly, also jointly with the participating teams. To avoid unreasonable burden, voluntary nature of participation was repeatedly emphasised throughout the research process and participants were encouraged to leave the study if they showed signs of distress. 20
Results
Patient interviews
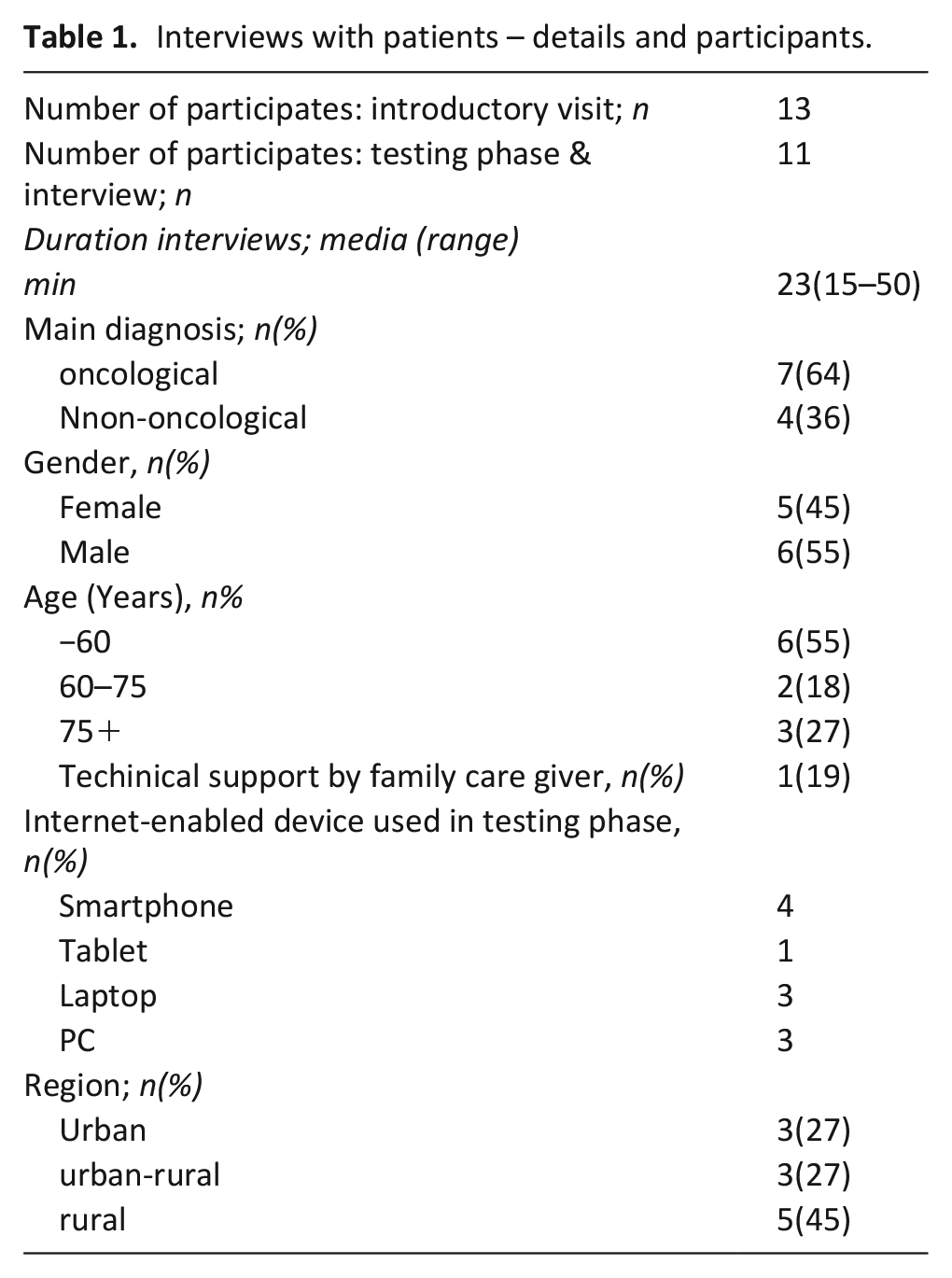
From March to October 2019, we recruited 21 patients for the study. Seven patients declined the introductory visit due to deterioration. The introductory visit was conducted with 14 patients. Afterwards, two patients decided not to participate in the interview and testing phase because their health deteriorated, and one patient declined to participate after reading the eIPOS questions. Eleven patients completed the testing phase of eIPOS and were interviewed subsequently. Additionally, two patients refused to participate in the testing phase and interview but allowed the researcher (IBF) to use the field notes from their introductory visit. For participants’ details see Table 1.
Interviews with patients – details and participants.
Focus groups with health care professionals
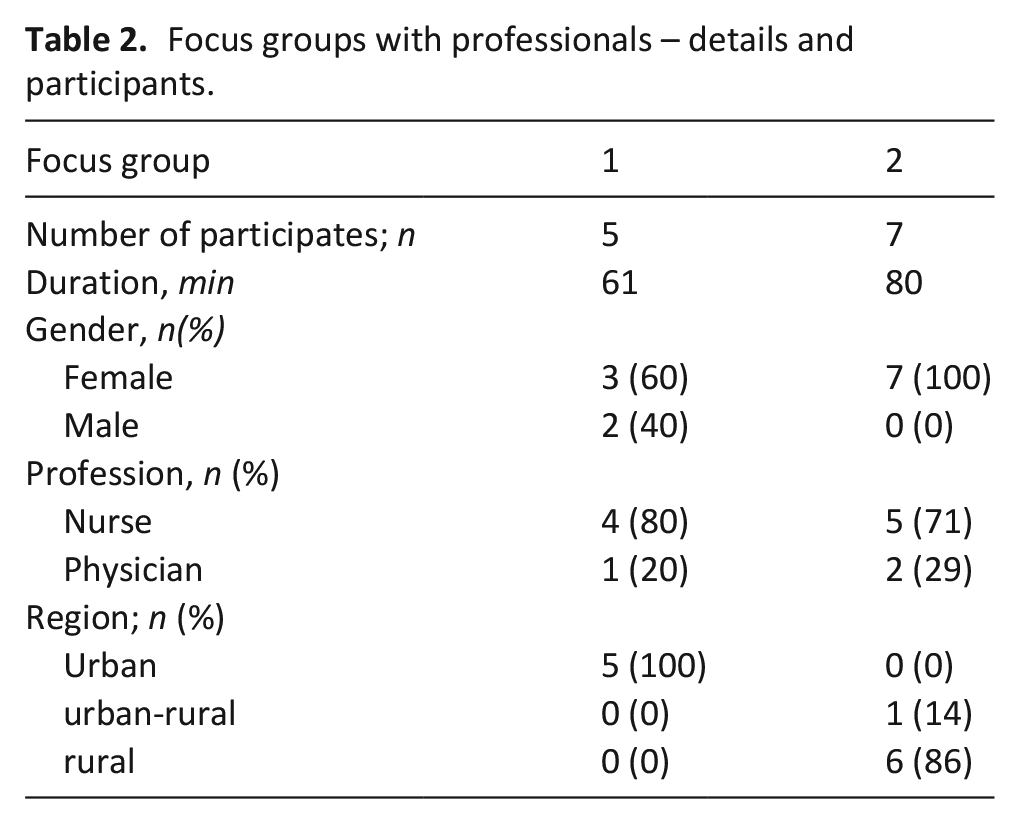
In summer 2019, we conducted two focus groups. Twelve health care professionals from the five participating teams involved in the overall project participated (see Table 2). Details of health care professionals are not further specified due to risk of identification.
Focus groups with professionals – details and participants.
Our framework organised the inherent information from the data corpus in seven deductively developed categories (see Figure 1).
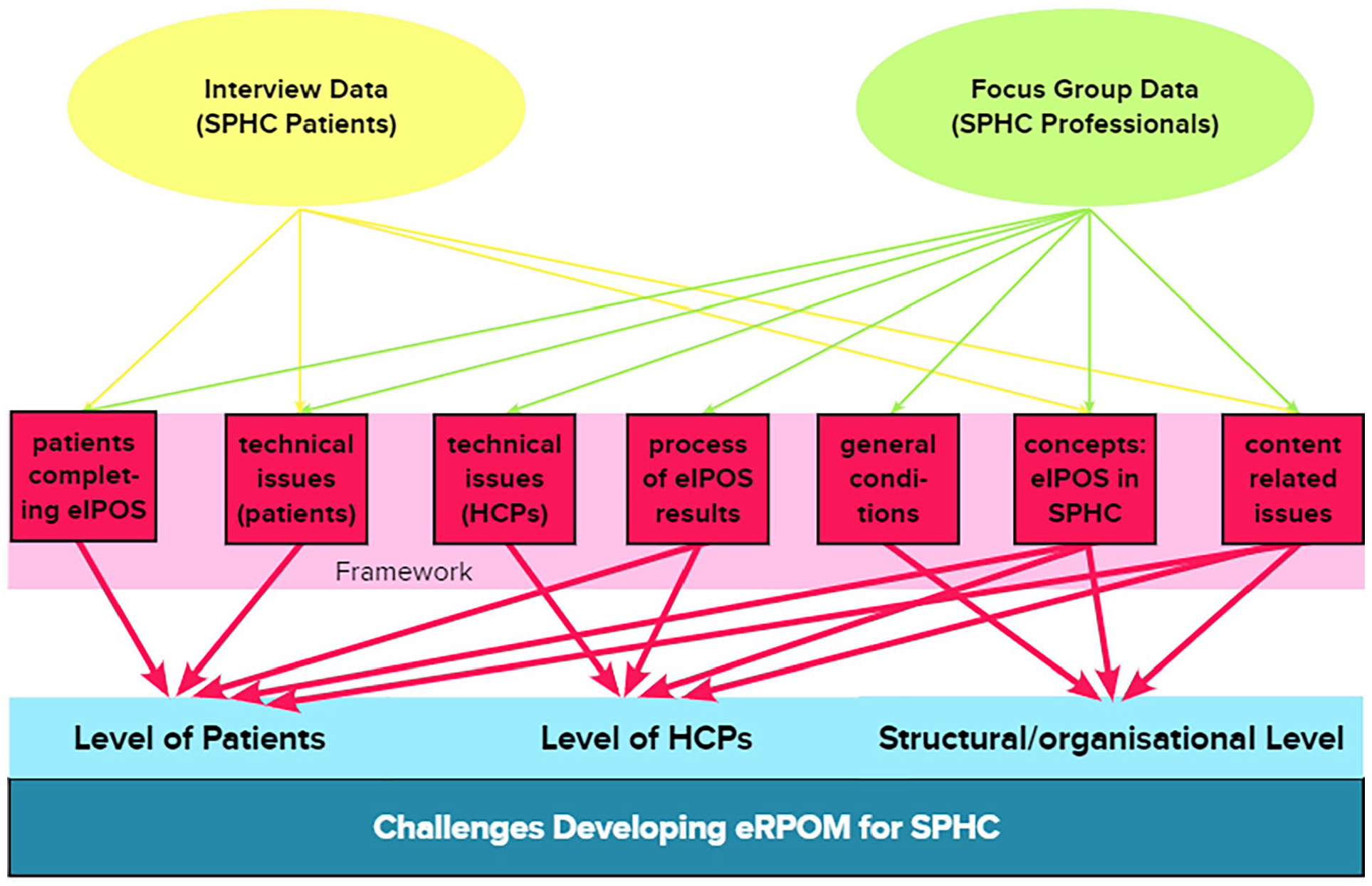
Data base, framework and structured reporting of challenges developing ePROM for SPHC.
In a further step we systematised our findings and present them as challenges in developing an ePROM from the perspectives of patients or health care professionals. These are complemented by challenges related to basic organisation and structure of the home care teams (see Figure 1).
Challenges at patient level
Identified challenges at patient level in all categories are reported below.
ePROM-use depending on current condition: health care professionals expressed concerns that many of their patients might not be able to use eIPOS on their own, due to high symptom burden very poor general condition or other illness-related limitations.
Now when I take a closer look, I find it difficult to find patients who are able [to use eIPOS]. There are many who are no longer able to do this.
(Health care professional 1)
Health care professionals’ concerns that patients’ condition might not allow independent ePROM use were mirrored in the difficult recruitment process for the patient-interviews. In the focus groups, a repeatedly proposed solution to this challenge was to involve relatives in the use of eIPOS. Patients indicated that the actual act of completing eIPOS depends on their current health state. One patient described that he completed eIPOS especially when he felt unwell to document or communicate this. Other patients tended only to use eIPOS on ‘good days’, everything else would mean too much burden in situations where they are confronted with, for example, intense pain, severe vomiting, or psychological problems. Patients in a more stable condition and/or with non-oncological diseases preferred a lower frequency of eIPOS use, because they felt that noteworthy changes were not as frequent.
Patients’ challenges in eIPOS-use connected with internet familiarity and technical design: Patients also reported challenges using eIPOS on their own web-based device. Although the inclusion criteria stipulated the patients’ use of an internet-enabled device, participants reported problems with opening eIPOS, ticking the answers or electronically submitting the questionnaire. Some patients forgot how to open the internet browser on their device or did not find the field where to add the personal code for opening eIPOS. For submitting the completed questionnaire, patients had to use a specific button at the end of eIPOS. Participants often oversaw this button and consequently did not send the completed questionnaire. Another challenge using eIPOS on smartphones was that due to the small display size, some patients had difficulties in ticking the correct answer boxes on the touch screen.
Patients also commented on the design of the eIPOS and preferred an overview of the whole questionnaire rather than presentation of single questions (one question displayed per page). One reason for this was that using the single question version, some patients felt burdened by the length of the questionnaire. Furthermore, participants tended to be confused when seeing eIPOS for the first time during the introductory visit and/or had problems to understand the questions.
Personally, I find this overall version more useful because I can read through it straight away and then I have an overview. Then I know, aha, I can write that [symptom] in there, write that in here, write that in there.
(Patient 10, 55 years)
Another reason for preferring the overview-version was the desire to re-check the previous questions and answers or the following items to decide whether to quote a specific symptom burden or palliative need with this question or whether it might fit better in another place. Furthermore, some patients felt burdened by the list of potential symptoms, even not experiencing them.
Effects on patients: Already completing the eIPOS had an impact on patients - even without forwarding the results to the teams. Some patients perceived the regular use of the electronic questionnaire as a task they had to fulfil and as an additional activity they had to integrate into their daily routine characterised by the terminal situation. A patient described that she was annoyed by the regular task of completing the eIPOS. Further challenges for patients were the necessity of getting out of bed to sit in front of the computer for completing eIPOS if they did not use a smartphone or tablet. Also, participants felt it required a quiet and unescorted moment confronting themselves with the questions of eIPOS.
Completion of eIPOS focussing on physical, psychological, social, and spiritual dimensions requires patients to engage in a holistic process of reflection of their current situation. Some participants appreciated this effect, reporting that this reflection helped them to cope with the current symptom burden by focussing and noting it on eIPOS or by applying appropriate self-help measures afterwards:
‘Because then I also thought, man, how were the last three days, that I reflect a bit. I thought that was good. And somehow, I am a bit more precise with, uh, that I think about what was a main problem or a concern and what was a symptom. [. . .] I think this is good, because only through this can I somehow, yes, deal with it or, yes, heal, (laughs) no, not heal, but go into acceptance or see that I really do something. Heat pads or whatever’. (Patient 4, 58 years)
Other participants described how they tried to supress their current situation as much as possible in everyday life and that using eIPOS undermined this coping strategy. One potential participant refused the use after reading the questions of eIPOS in the introductory visit, pointing out that he was not willing to be ‘rudely’ directed regularly to his situation by the questionnaire.
Challenges of ePROM use in specialist palliative home care: health care professional level
In the focus groups, health care professionals discussed various challenges connected to the uncertainties regarding the actual implementation concept of eIPOS in concrete clinical practice. General concerns were that eIPOS might not bring any new information because of the close and intensive care relation between patients and health care professionals and that an electronic assessment system could not be used by many of their patients. Further challenges were linked thematically to the process of receiving the information electronically transmitted via eIPOS as well as to health care professionals’ potential use of eIPOS information.
Concerns and requirements of health care professionals receiving eIPOS: Focus group participants raised the questions which health care professionals from the multidisciplinary team is responsible to assess the eIPOS-reported symptom burden and concerns and when this should happen. Most of them would prefer to receive new eIPOS information in the morning when daily planning is organised. Nevertheless, health care professionals emphasised that time resources are scarce then and reading out a comprehensive list of patient-reported symptom burden and problems in eIPOS might be challenging. They suggested a distinction between relevant symptoms and others that do not require immediate reaction from the team. Symptoms and problems reported via eIPOS like ‘loss of appetite’, ‘feeling depressed’ or ‘practical problems’ were assessed as non-urgent for current daily planning. Furthermore, health care professionals generally mentioned the fear to miss out patients’ current need for support, if for some reason they do not check the documentation software for, for example, half a day:
But then the question is, do I notice it at all, am I on the computer or am I on a home visit?
(Health care professional 3)
To support reception process of eIPOS in the software itself, health care professionals expressed the need of a pop-up message indicating a new eIPOS. Moreover, most of the focus group participants asked for a warning signal in the software, highlighting patients with high values or deteriorating symptoms reported via eIPOS.
Another aspect is the interpretation of eIPOS information provided by the patients. Health care professionals mentioned a process of assessing the reported values in context of their knowledge about the patients:
Mr. [name patient], if he has a two [in the eIPOS-scale for self-assessing symptom burden; editors‘ note], then I know, okay, that’s a four. So, yes, you just know that, when you have visited him [. . .] several times and when you know him. (Health care professional 2)
Furthermore, health care professionals emphasised that the eIPOS values are only able to give a hint and mentioned the need of further assessment to valid reported values and understand underlying needs.
Challenges – use of eIPOS information: Participating health care professionals discussed challenges how to react on eIPOS-reported values. One crucial aspect was how to deal with the potential expectation of patients to receive a prompt reaction:
The question is: [. . .] Is it really meant in such a way that we have to react directly on a reporting in the system? That is quite relevant. And what if it occurs at 2 o’clock in the morning? And what if at the weekend? How is it communicated to the patient?
(Health care professional 9)
The question is, when do you have to react and how?
(Health care professional 7)
Some focus group participants were unsure whether the team would be able to respond appropriately to all aspects returned in the eIPOS because of limited team resources, for example, psychological or spiritual support.
Health care professional 3: And that means, I think, that we can’t or won’t take action about every single issue [eIPOS-reported symptom burden or problem; editors’ note], I don’t know, maybe it’s sometimes better to let sleeping dogs lie. Health care professional 2: That it is made clear that things are, um, inevitably, um, going down.
These results also highlight that it might be challenging if patients notice that there is no response from the health care professionals regarding the reported symptom burden or problems.
Developing ePROM for specialised palliative home care: Challenges on the organisational and structural level
Organisational challenges: In the focus groups and some interviews, specific procedures of using ePROM in the daily care routine of palliative home care were reflected. Uncertainties related to the actual implementation concept of eIPOS in concrete clinical practice and that the ePROM-tool might reduce personal contact to the patients and undermine the existing 24 h-emergency call system. Another aspect pointed to the 3-day period used in eIPOS whereas some participating teams had daily contact with their patients.
The questionnaire asks for the last three days. Which symptoms in the last three days. If he has severe pain on day one, how can I tell if day one with severe pain has already been treated? [. . .] There was already medication on demand. There was already a visit, etc. How can I differentiate that, so that I don’t have even more work to do?
(Health care professional 5)
Challenges related to structural preconditions: health care professionals emphasised that specialised palliative home care can only be provided for patients with complex symptom burden. Due to scarce resources teams give priority to patients in acute crisis and pause care for patients where the situations stabilise again:
But because we have become more of a crisis team, we are back to the point where we all say: Which patients are suitable for this [eIPOS, editors’ note]? Because if they are so stable that they can or want to deal with something like that, they are actually so stable that we pause with the care. (Health care professional 8)
Health care professionals suggested using ePROM in less intensive levels of care, which usually also mean less contact between the team and the patient: In this situation, eIPOS could serve as an indicator for increasing the intensity of care due to increasing symptom burden. Health care professionals recommended the shared use of ePROM across the different intensity level of palliative home care to support patients’ changes between the services.
Discussion
Main findings
We aimed to identify and explore challenges for developing an ePROM for standardised assessment in specialised palliative home care. Our results draw a comprehensive picture of these challenges on patients’ and health care professionals’ level as well as on the organisational and structural level. Main findings regarding the patients’ level are that the general use of ePROM in a status of deteriorating health is challenging, which was reflected in (i) the short time period patients are cared for by specialised palliative home care, (ii) insufficient equipment with own web-enabled devices, and (iii) challenging recruitment of interview partners due to poor general condition. The health status of only a very small proportion of patients from the participating teams allowed participation in the testing phase of the eIPOS with an own web-enabled device. This correlates with previous studies in palliative care indicating that some patients’ general condition might be too poor to use PROMs.21–23 Our results suggest that this could be overcome for the setting of palliative home care by family caregivers using ePROMs as proxies, as it is already recommended for the implementation of paper-based PROM use. 9
The poor health condition also hampered patients’ participation in the qualitative interviews. As no new aspect emerged in the last two interviews, we concluded that data saturation was reached after the 11th interview to avoid burdening further interview partners.
Furthermore, our findings recommend ePROM use already in earlier stages of palliative home care and its use across the different services. This idea goes in line with identified need of electronic patient record supporting the share and exchange of information across different palliative care settings. 24 Corresponding to other studies our results demonstrate that using eIPOS enables reflective processes on patients’ level.1,25 However, this could also be a barrier to ePROM use in case of evoking negative emotions when faced with current or potential symptom burden. A study of the feasibility of paper-based PROMs in German specialised palliative home care identified health care professionals’ concerns about burdening patients in this way. 9 In contrast, our results suggest that the use of ePROMs could also serve as a facilitator as it allows patients to better understand and express the perception of their illness.
Moreover, our findings illustrate how health care professionals in palliative home care imagine the process of receiving ePROM information and reacting to them. Corresponding to previous studies in specialised palliative care in the UK and various palliative care settings in Germany, we noticed a fear that ePROM-use could reduce personal interaction between patients and health care professionals.10,21 Our findings about the low acceptance of ePROM by health care professionals doubting the potential benefits provide another challenge in implementing ePROM in palliative home care.7,9,10
Furthermore, the technical implementation regarding, for example, the design of the patients’ questionnaire or the display of the ePROMs in the teams‘ documentation system, plays a crucial role for acceptance. 21 As the participating teams did not use standardised PROM assessment in daily care routine before, it might be possible that identified challenges relate generally to the routine use of standardised measurement of patient reported outcomes and not explicitly to its electronic realisation.
Beyond the individual or team level, our results confirm that digital innovations need to support, rather than undermine the existing organisation of clinical care and fit into structural preconditions, as shown in previous research. 26 In this regard, we consider the very divergent organisational structures in German specialised palliative home care as particularly challenging to develop a generally suitable ePROM system.
Strengths and weaknesses
Our qualitative approach supported explorative investigation of challenges for the development of a setting specific ePROM system. We managed to included later user groups in a participatory idea, as requested for studies focussing on digital health approaches. 27 As participants were recruited from five palliative home care teams, differing considerably regarding clinical care organisation, regional setting, and their collaboration with a network of complementary care structures, our results represent a broad spectrum of backgrounds and views.
Because the overall project followed the MRC framework 28 that recommends an exploratory study prior to implementing the intervention into clinical practice, only the patients had personal experience with eIPOS which could be seen as a weakness. Medical professionals had no experience with eIPOS at the time the focus groups were conducted. However, we attempted to mitigate this weakness by introducing the concept of eIPOS in the focus groups to bring all participants on the same level of knowledge. Furthermore, due to inclusion criteria the patient-related results represent only a (small) part of patients in the home care setting as only comparatively stable patients were included.
What this paper adds
This study provides stakeholder generated insights about challenges that should be faced when developing a field-specific electronic assessment system. This created the base for the following parts of the Palli-MONITOR-study following MRC phase 2 (feasibility/piloting) where the eIPOS-intervention was modelled based on the stakeholders‘ insights. Using the example of specialised palliative home care, our results demonstrate the need of an adaption of ePROM-tools to the setting – not only to the obvious structural conditions, but to something, what could be captured with the term of setting specific culture. 29
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221141487 – Supplemental material for Challenges developing an electronic patient-reported outcome measurement for palliative home care: A qualitative interview and focus group study
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221141487 for Challenges developing an electronic patient-reported outcome measurement for palliative home care: A qualitative interview and focus group study by Isabel Burner-Fritsch, Anna Bolzani, Katerina Hriskova, Stefanie Kolmhuber, Claudia Bausewein and Farina Hodiamont in Palliative Medicine
Footnotes
Acknowledgements
The authors are grateful to the patients and palliative care professionals participating in this study, enabling our research as well as further development of setting-sensitive use of digitalisation in palliative home care.
Author contributions
IBF: data collection, analysis, interpretation of data, led the writing process and drafted original article and reviewing for critically important content interpretation of data and reviewing for critically important content. AB: reviewing data for critically important content. KH: conceptualisation, supported the writing process. SK: conceptualisation, supported the writing process. FH: obtained funding, conceptualisation and design, supported the writing process, critical review of the final manuscript. CB: obtained funding, conceptualisation and design, supported the writing process, critical review of the final manuscript.
All authors take responsibility for appropriate portions of the content of this article.
Data sharing and management
Due to the high sensitivity of qualitative interview and focus group data, data is only available on reasonable request in German language.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Federal Joint Committee German Innovation Fund (Innovationsausschuss des Gemeinsamen Bundesausschuss), grant number 01VSF17014. The funder played no role in the collection, analysis and interpretation of data, in the writing of the report or in the decision to submit the article for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.