
Abstract
Background:
Team-based palliative care interventions have shown positive results for patients at the end of life in both hospital and community settings. However, evidence on the effectiveness of transmural, that is, spanning hospital and home, team-based palliative care collaborations is limited.
Aim:
To systematically review whether transmural team-based palliative care interventions can prevent hospital admissions and increase death at home.
Design:
Systematic review and meta-analysis.
Data sources:
MEDLINE (Ovid), Embase (Ovid), CINAHL (Ebsco), PsychINFO (Ovid), and Cochrane Library (Wiley) were systematically searched until January 2021. Studies incorporating teams in which hospital and community professionals co-managed patients, hospital-based teams with community follow-up, and case-management interventions led by palliative care teams were included. Data was extracted by two researchers independently.
Results:
About 19 studies were included involving 6614 patients, of whom 2202 received an intervention. The overall pooled odds ratio of at least one hospital (re)admissions was 0.46 (95% confidence interval (CI) 0.34–0.68) in favor of the intervention group. The highest reduction in admission was in the hospital-based teams with community follow-up: OR 0.21 (95% CI 0.07–0.66). The pooled effect on home deaths was 2.19 (95% CI 1.26–3.79), favoring the intervention, with also the highest in the hospital-based teams: OR 4.77 (95% CI 1.23–18.47). However, studies had high heterogeneity regarding intervention, study population, and follow-up time.
Conclusion:
Transmural team-based palliative care interventions, especially hospital-based teams that follow-up patients at home, show an overall effect on lowering hospital admissions and increasing the number of patients dying at home. However, broad clinical and statistical heterogeneity of included studies results in uncertainty about the effect size.
Keywords
Both home-based and hospital-based palliative care interventions reduce hospital readmissions and increase home deaths.
Transmural team-based palliative care interventions can improve important outcomes for patients at the end of life.
Hospital-based teams that follow patients at home seem to have the largest impact on patient outcomes.
Since quality of the studies was low to moderate and heterogeneity was high, further research to draw stronger conclusions is needed.
Introduction
Palliative care is an approach to improving the quality of life for patients and their relatives facing life-threatening illness. 1 Palliative care traditionally focused on patients with an oncological diagnosis; however, the number of patients living with and dying from multiple chronic conditions is increasing, emphasizing the need for well-organized palliative care. 2 Although most patients at the end of life wish to be cared for and die at home, care transitions to the hospital, and consequently hospital deaths, are common in the last phase of life.3–6 Continuity of care, collaboration, and information sharing between care settings are important aspects of palliative care.7,8 However, collaboration between professionals from different care settings is suboptimal and can lead to negative patient outcomes.9,10
The organization of palliative care is highly dependent on country and setting. Whereas in some countries, palliative care specialists provide most of the palliative care, in many European countries, generalists such as the general practitioner provide most of the palliative care, and specialists have a consulting function. Studies have shown interventions incorporating multidisciplinary care teams are the most effective in improving patient outcomes. 11 These multidisciplinary care teams function either within the hospital or in the community setting and do not follow patients while they move from one setting to another. For continuity of care, structured collaboration between home and hospital, information sharing, and providing care at the desired place are important. Transmural palliative teams are teams that provide continuous care for patients at the end of life while the patient moves between settings. Whereas research has found both home-based and hospital-based palliative care interventions reduce hospital readmissions and increase home deaths,12–14 evidence on the effectiveness of structured transmural team-based palliative care collaborations is limited. Hence, whether transmural team-based collaborations in which patients are followed throughout care settings reduce hospital admissions and increase home deaths is unknown.
The aim of this study is thus to systematically review and summarize all evidence on effectiveness of transmural team-based collaborations between hospital and primary care professionals in palliative care on hospital admissions and home deaths. We include three models of care: (1) collaborative teams in which hospital and community-based professionals closely collaborate, (2) hospital-based teams that follow patients in the community setting, and (3) case management coordinated by a hospital-based team.
Methods
A systematic review was performed and results are presented in descriptive manner. For eligible studies a meta-analysis was performed with the aim to answer our research question: can transmural team-based collaborations decrease hospital admissions and increase home deaths. The updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. 15 The study was not registered. The study protocol is available on request.
Inclusion criteria
We included interventions of team-based collaboration between primary and secondary care. We defined transmural team-based palliative care as teams that provide continuous care for patients at the end of life while the patient moves between settings. Teams had to provide at least face-to-face consultations at home or in the hospital. We defined three organizational models for the teams:
Collaborative teams: These teams involve structural collaboration between professionals from both the hospital and community. They follow patients transitioning between care settings. They can provide medical care and symptom control at home.
Hospital-based teams: These teams provide care for patients in the hospital and community setting (through home visits), without structural collaboration with primary care professionals. These teams are mostly responsible for all care and can treat patients at home.
Case management: Case managers collaborate with hospital-based multidisciplinary teams. The main focus is on advance care planning and not on providing treatment at home.
We did not consider interventions to be transmural team based when teams were solely hospital based, for example, when they followed patients in the outpatient setting or were community/hospice based with referrals from the hospital but no further or unclear collaboration with the hospital.
We used the following additional inclusion criteria for studies:
(1) Study participants, or i.e., patients, were 18 years or older.
(2) Studies defined their participants as being in need of palliative care.
(3) Studies used an independent control group: randomized controlled trials (RCTs), non-RCTs (e.g. before-and-after study, interrupted time series), and observational studies (e.g. cohort study and case-control study). Control groups were (historical) care as usual, which could either be palliative care provided in one setting, or no palliative care.
(4) Studies used one of the following outcomes: (re)-hospitalizations and/or days of hospital admissions or home death and/or (preferred) place of death. These outcomes can be seen as synonyms for good symptom control by reducing the need for unplanned hospitalizations and reflect organization of care to fulfill a patient’s wish to spend time and die at home.
(5) Studies had to be in English or Dutch.
Search strategy
MEDLINE (Ovid), Embase (Ovid), CINAHL (Ebsco), PsychINFO (Ovid), and Cochrane Library (Wiley) were systematically searched from onset until January 2021. We drafted a customized search strategy with the help of a clinical librarian (FJ). To validate the search strategy, we formulated a reference set of articles through a scoping search (IF). The search contained the following key concepts: “palliative care,” “transmural care,” “hospitalization,” and “place of death.” The full search strategy is displayed in Supplement 1.
Study selection and quality assessment
All titles and abstracts were screened independently by two of four researchers (IF, EG, MP, and SB) for eligibility for full-text assessment. The researchers discussed discrepancies between selection, which occurred in 3.9% of the abstracts, until reaching consensus, and, if necessary, consulted a third researcher (BB). Covidence software was used throughout the screening process. 16 References were screened for additional articles. IF and EG read the selected full text and assessed eligibility for data extraction independently. BB was consulted for the final selection of studies for this review.
The Cochrane risk-of-bias tool 17 was used for quality assessment of RCTs and the Robins-I tool was used for non-RCTs. Because the blinding of transmural team-based palliative care interventions is essentially impossible, studies where participants and professionals were not blinded were not automatically assessed as high risk. Furthermore, the outcomes for hospitalization and place of death are unlikely to be influenced by a lack of blinding and will therefore be treated as “low risk-of-bias” even if blinding was unsuccessful.
Data extraction
Two researchers (IF and EG) independently used a standardized data-extraction form for data extraction. Data were collected on study characteristics (author, publication year, country, type of study), intervention characteristics (aim of study, description and components of intervention, recruitment place, comparator, team members), patient characteristics (mean age, gender, disease characteristics), and outcomes (hospitalization, place of death, preferred place of death).
Data analysis
Studies were synthesized in a descriptive summary. Odds ratios and 95% confidence intervals were constructed per study and for each outcome. If these data were not available from the main manuscript, authors were contacted to provide these data. We used the Mantel-Haenszel estimator to perform a random-effects meta-analysis with studies that reported event data on the outcomes for hospital admissions and/or home deaths. If studies reported different endpoints for hospital admissions, for example, admissions 1 month before death and 6 months before death, we included data from the longest timeframe. In the analysis of home deaths, we additionally used the Peto odds method because one of the studies had zero events. Pooled odds ratios were converted to absolute risk reduction and number needed to treat.
We used the chi-square test and I² statistic to assess the statistical heterogeneity. We defined several sources of clinical and methodological heterogeneity and used subgroup analyses to explore their influence on the pooled effect estimates. First, we hypothesized that the effect would be different for the three types of interventions. Second, we investigated whether risk-of-bias influenced the effect estimates. We did not construct funnel plots, because the sample of included studies per outcome was less than 10.
Results
The database searches yielded 11,217 records, and manual searches identified an additional 35 records (Figure 1 19 ). We screened 8566 abstracts for inclusion and exclusion criteria, after which we assessed 275 full texts for eligibility. Nineteen articles were included in this review. For two studies, three separate articles were published that looked at different outcomes, and these studies will be described as one study by Benthien et al.20–22 and by Rogers et al. 23–25
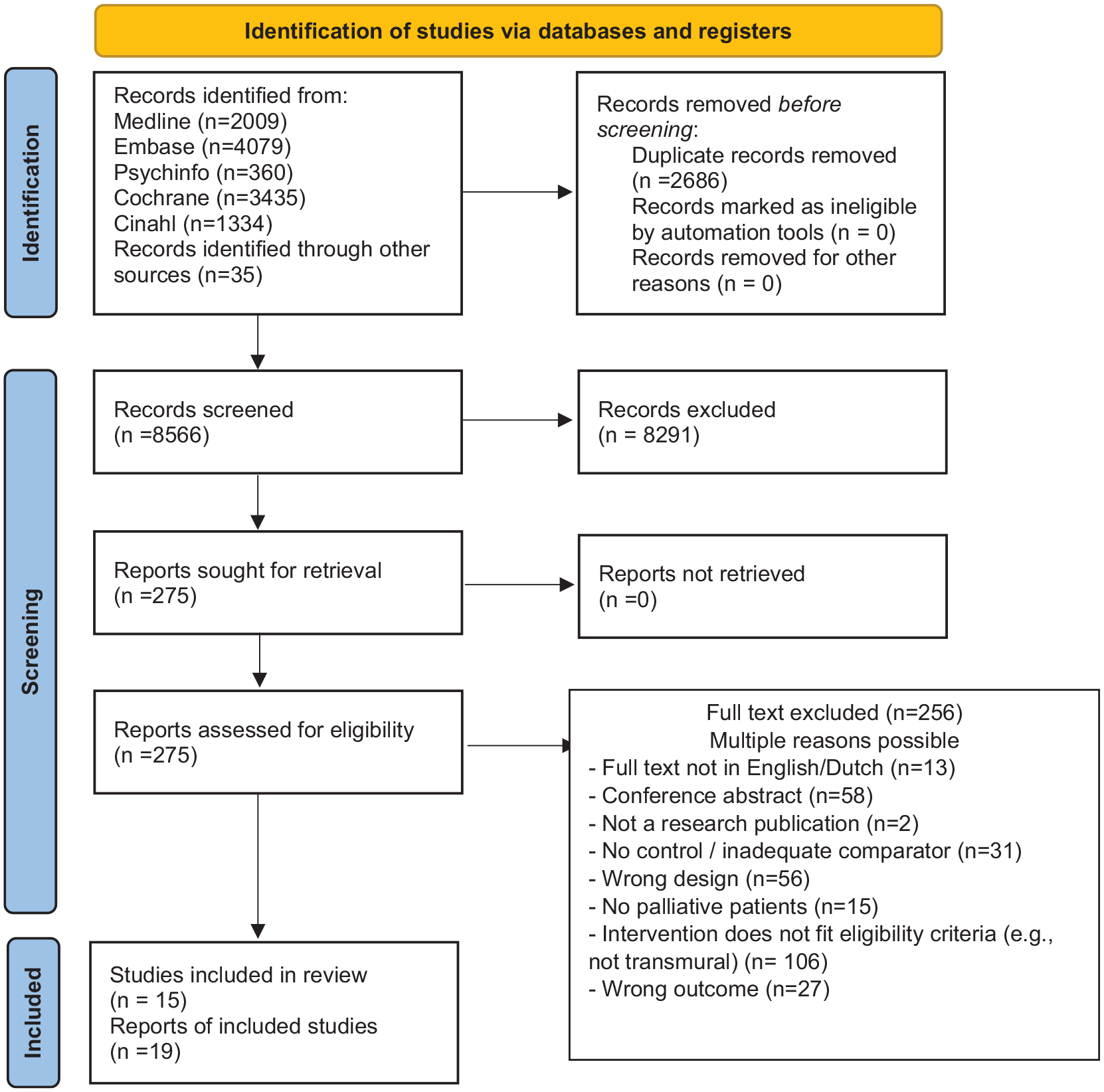
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
Description of studies
Table 1 and Supplement 2 summarizes the included studies and outcomes. Seven studies were RCTs20,21,23–30 or a cluster RCT, 31 two were prospective non-randomized studies,32,33 one was a prospective quasi-experimental study, 34 four were retrospective before–after studies,35–38 and one was clustered, partially controlled before–after study. 39 Of these, three studies were pilot studies.29,33,35
Study characteristics. Collaborative team hospital and primary care.
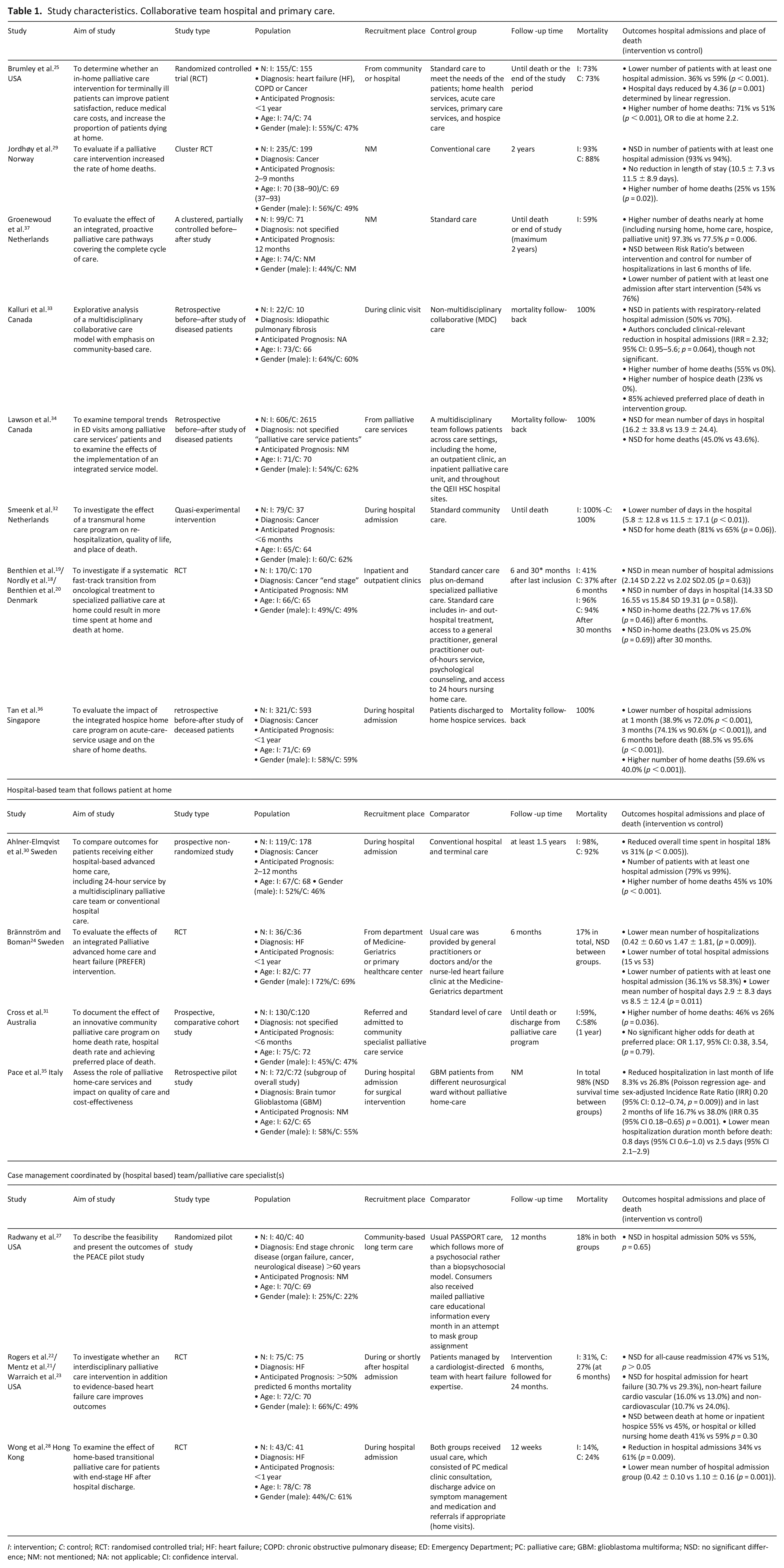
I: intervention; C: control; RCT: randomised controlled trial; HF: heart failure; COPD: chronic obstructive pulmonary disease; ED: Emergency Department; PC: palliative care; GBM: glioblastoma multiforma; NSD: no significant difference; NM: not mentioned; NA: not applicable; CI: confidence interval.
Overall, the studies included 6614 patients, 2202 of whom were in the intervention groups. Eight studies assessed collaborative teams with hospital and primary care professionals, though none of the interventions were exactly the same.21,27,29,34–36,38,39 The effect of hospital-based teams that followed patients in the community setting was assessed in four studies.26,32,33,37 In three studies, case management was the primary focus of intervention.24,29,30
In four studies, the intervention was compared with non-transmural palliative care,30,35,36,38 whereas in the other studies, the usual care did not include palliative care, although in some cases, usual-care patients did receive hospice or terminal care on demand.
For eight studies, hospital admissions were (one of) the primary outcomes,27,28–32,34,35,37,38 whereas it was a secondary outcome for four studies. Cross et al. 33 solely looked at place of death.
Risk assessment
Table 2 shows the risk-of-bias scores. Out of the seven RCTs, none received a low risk for all five bias points. All studies either received some concern or high risk-of-bias score due to deviations from intended interventions, because information on adherence to the intervention was missing. Jordhøy et al. 31 received a high risk-of-bias score on the randomization process because it was a cluster RCT.
Risk of bias.
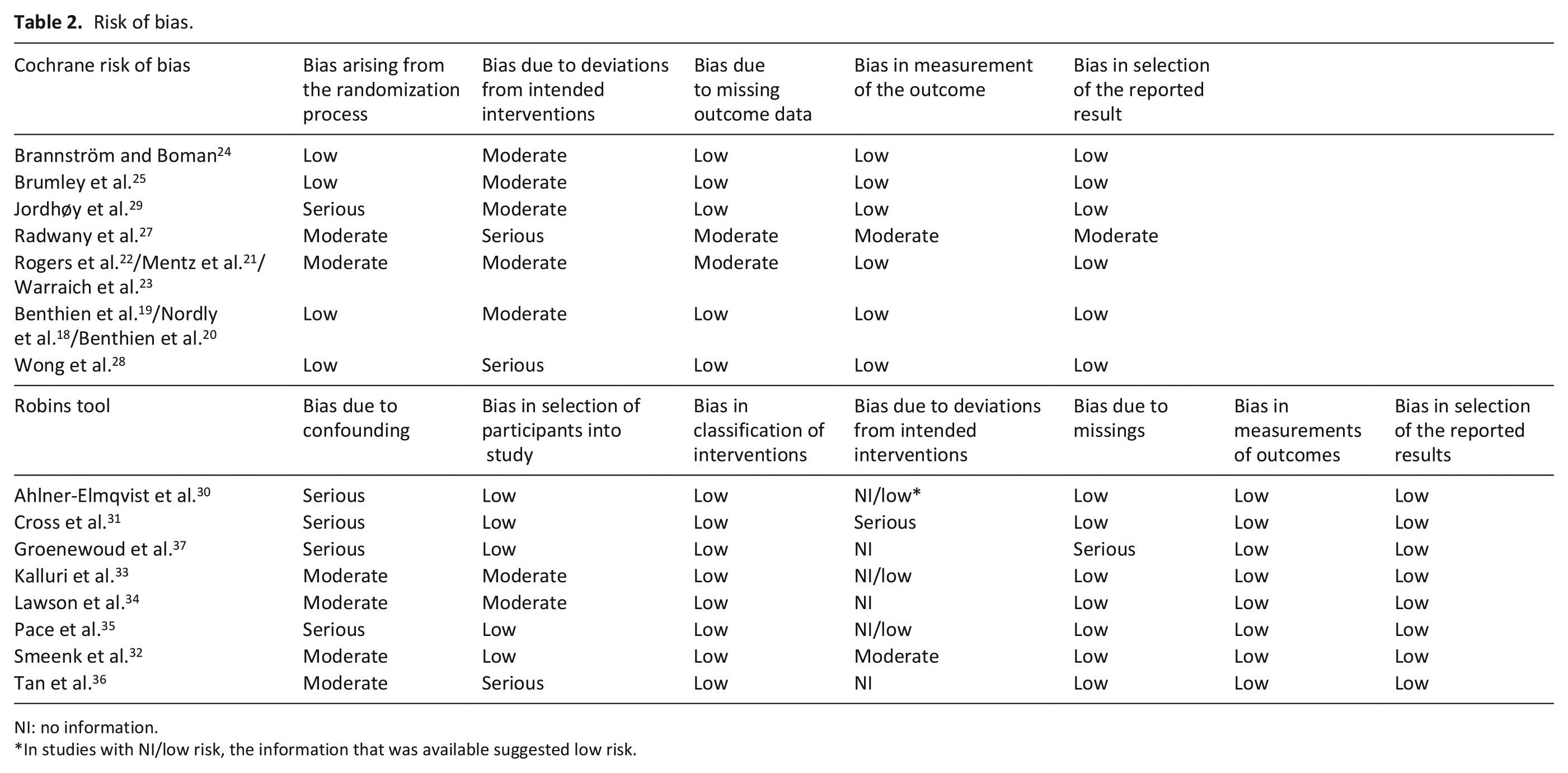
NI: no information.
In studies with NI/low risk, the information that was available suggested low risk.
For the non-RCTs, all studies received at least moderate risk in the confounding section. Also, moderate to serious risk-of-bias was found due to deviations from intended interventions or insufficient information to fully judge this section.
Meta-analysis
Twelve studies were included in the analysis on hospital admission (see Figure 2). Overall, the odds of hospital admission was significantly reduced. The pooled odds ratio was 0.48 (95% CI 0.34–0.68). The overall absolute risk difference was −0.13 (95% CI −0.16, −0.10), and equals a number needed to treat of 7.55 (95% CI 6.11–9.87). However, considerable heterogeneity exists (I² = 60%), and relevant subgroup differences were detected. Interventions with collaborative teams and hospital-based teams resulted in fewer hospital admissions, but this effect was not observed in case-management interventions. For collaborative teams, the absolute risk difference was −0.10 (95% CI −0.13 to 0.07) with a NNT of 10.13 (95% CI 7.57–15.31). For the hospital-based teams the absolute risk difference was −0.26 (95% CI −0.34, −0.18), with a NNT of 3.86 (95% CI 2.94–5.61). However, the residual heterogeneity for outcome was high within the three subgroups (I² 31%−74%), suggesting the differences in outcomes cannot be fully explained by the differences in intervention. For the sensitivity analysis for risk-of-bias, we selected studies that received a moderate risk-of-bias score on no more than two domains as the “higher”-quality studies, because none of the studies received an low risk-of-bias on all domains. These analyses could not be performed for the subgroups, due to the low number of studies. Looking at the pooled effect, the decreased odds for hospital admission remained (OR 0.52, 95% CI 0.33–0.81) (Supplement 3).
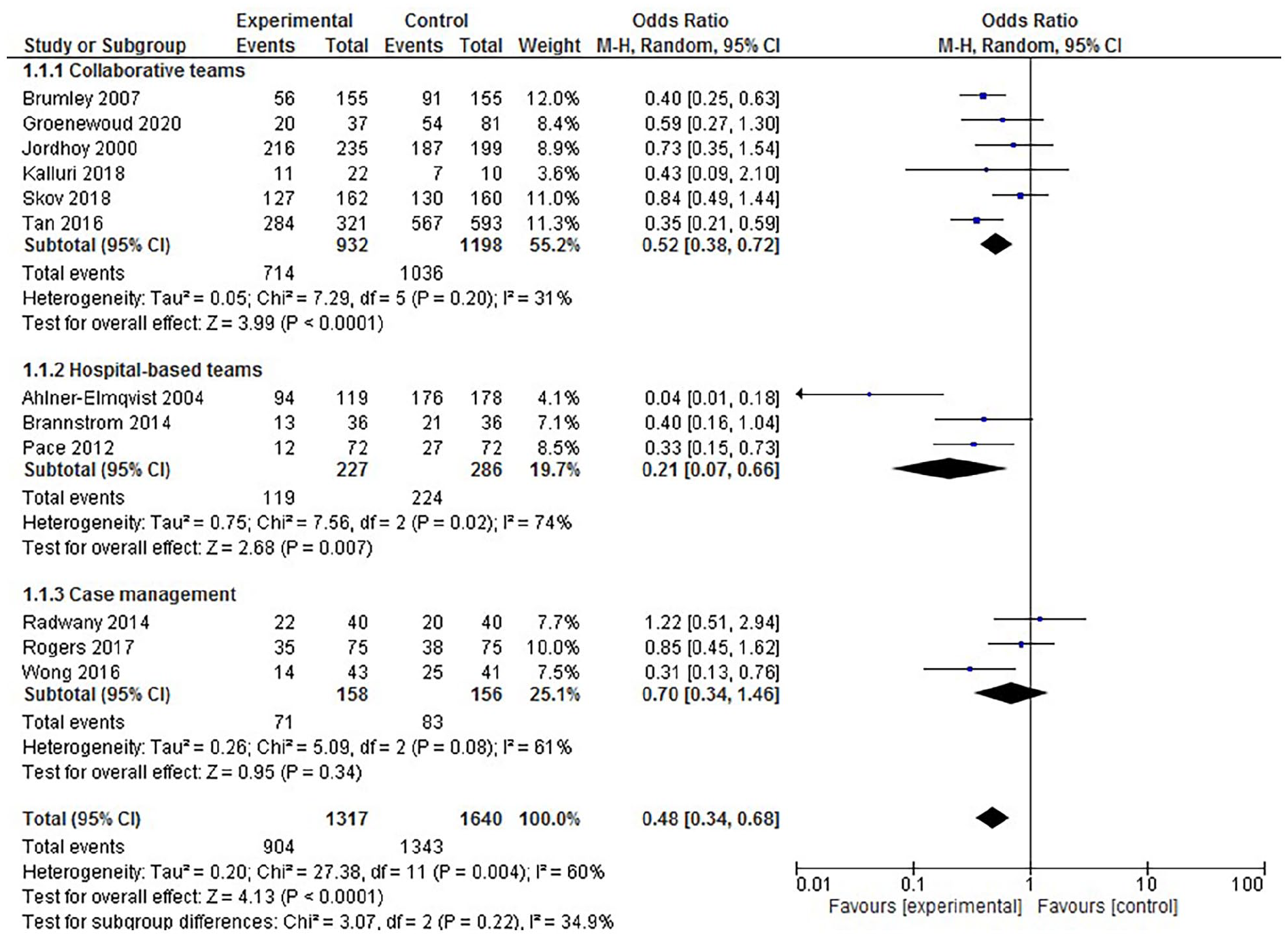
Meta-analysis on hospital admission forest plot.
Nine studies reported the percentage of patients with home deaths (Figure 3). We excluded one study from the random-effects modeling, because in the control group, zero events occurred. 35 The pooled effect indicate more home deaths (OR 2.19, 95% CI 1.26–3.79) with an absolute risk difference of 0.07 (95% CI 0.04–0.10) and an NNT of 14.7 (95% CI 10.4–25.3). The effect was larger in hospital-based teams (OR 4.77, 95% CI 1.23–18.47) than in collaborative teams (OR 1.73, 95% CI 0.98–3.04). However, the residual heterogeneity for outcome was very high within the two subgroups (I² 86%−92%).
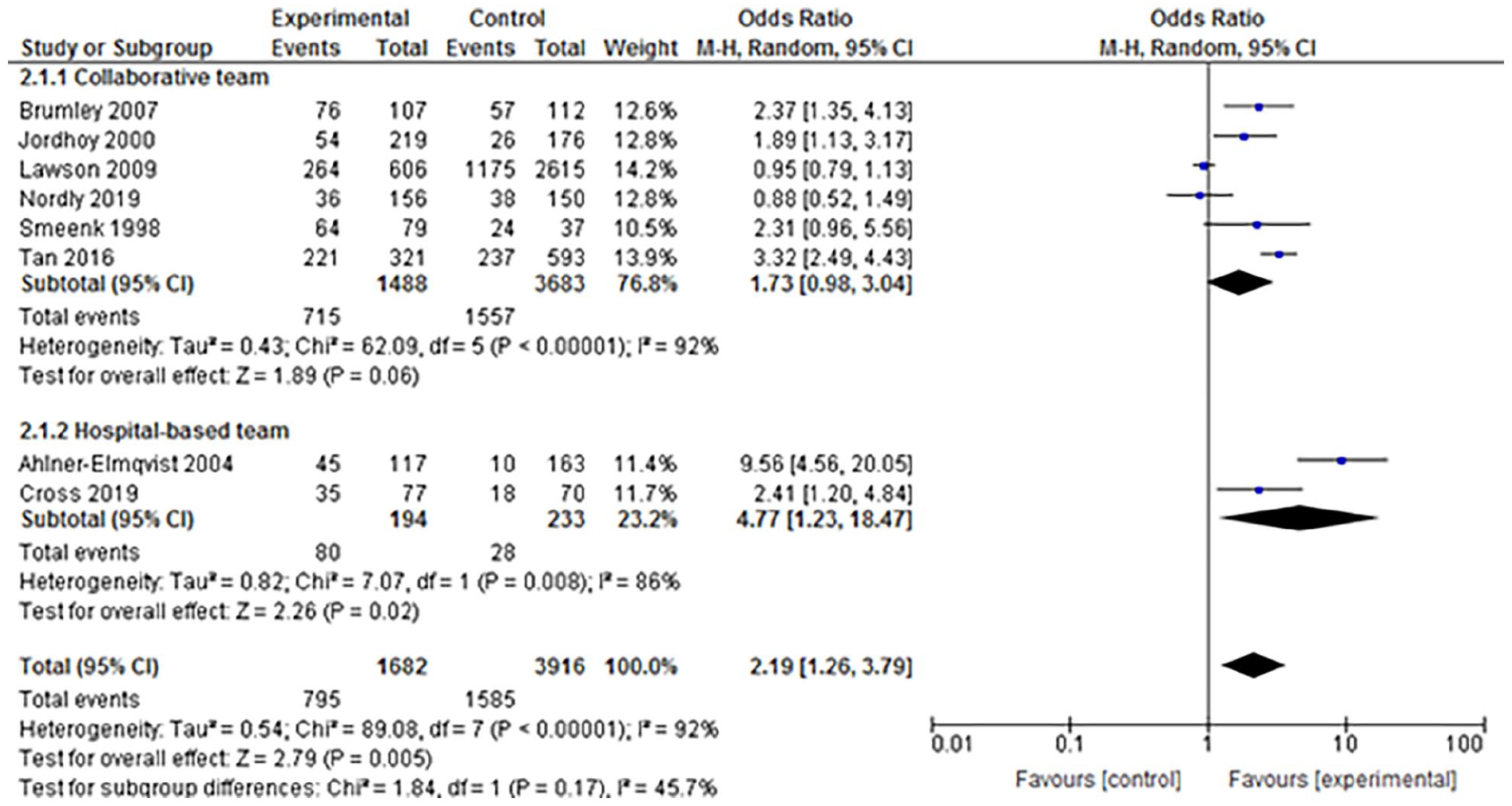
Meta-analysis on home death forest plot.
We found similar effects toward more home deaths in the sensitivity analysis with Peto odds, including the study with zero events (OR 1.57 95% CI 1.38–1.78), as well as within the sensitivity analysis for risk-of-bias (OR 1.63, 95% CI 0.81–3.31); see Supplement 3.
Additional outcomes
Two studies provided the mean number of admissions days. Lawson et al. 36 found no significant differences between intervention and control (16.2 ± 33.8 vs 13.9 ± 24.4). Smeenk et al. 34 did find a lower mean number of admissions days in the intervention group (5.8 ± 12.8 vs 11.5 ± 17.1 (p < 0.01)).
In two studies, the percentage of home deaths was combined with inpatient hospice deaths. Whereas Groenewoud et al. 39 found a significantly higher number of patients dying at home/hospice, Warraich et al. 25 did not find a significant difference. Two studies mentioned the preferred place of death: Kalluri et al. 35 reported that 85% of patients in the intervention group died at their preferred place of death; however, no number for the control group was mentioned. Cross et al. 33 found no increase in death at place of preference (odd ratio 1.17, 95% CI: 0.38, 3.54, (p = 0.79)).
Discussion
This systematic review and meta-analysis assessed the effect of transmural team-based collaborations between hospital and primary care professionals on hospital admissions and home deaths. We included 19 studies that incorporated collaborative teams, hospital-based teams, or case management. Meta-analysis demonstrated overall a lower number of patients with hospital admissions, and more home deaths. However, observing a precise effect estimate was impossible because of the heterogeneity. Subgroup analysis only partially explained the between-study variance but indicated hospital-based teams were the most effective. Furthermore, not all studies were of high quality; however, when we only included higher-quality studies, the overall reduction in hospital admissions and increase in home deaths remained.
Comparison with literature
Previous reviews have focussed on palliative care interventions in either the hospital setting or home care settings, with some positive results in reducing hospital admissions and increasing the rate of home deaths.13,14 Our review is novel in that it specifically focused on studies that span both the hospital and home setting. Overall, hospital-based teams that follow patients at home seem to have the largest effect on reducing hospital admissions and increasing the rate of home deaths, whereas case-management interventions showed limited effects. One explanation could be that in the included studies, the hospital-based teams were often fully in charge of the patient, and thus, continuity of care was achieved. However, earlier in the disease trajectory it might be more appropriate to provide palliative care alongside regular care. Additionally some patients might wish to continue seeing their general practitioner in addition to palliative care specialists. In these cases, collaborative teams in which palliative care specialists and generalists work together might be more desirable. This preference is also in line with the generalist-plus-specialist care model first described by Quill and Abernethy, 40 and fits well with the early palliative care model whereby palliative care is provided alongside disease-modifying treatment. Another explanation for the large effect of the hospital-based intervention could be that care as usual was non-palliative care in these interventions, whereas in the collaborative-team interventions, the usual care of the control group often already contained palliative care components.
Within the subgroup of case-management studies, the studies with longer follow-up showed no differences in readmissions, whereas the study by Wong et al. 30 did find positive effects of the intervention during the 12-week follow-up. Case management alone, even if in collaboration by a palliative team, might not be sufficient in the last months of life, when needs increase and more hands-on medical care is needed at home, to prevent hospital admissions. Furthermore, two of the case-management studies included patients with heart failure, and although the studies inclusion criteria stated end-stage heart failure, mortality rates were low, which could result from the difficulty in assessing prognosis in organ failure. 41 Case management’s limited effect on the reduction in hospital admissions in palliative settings is disappointing, especially compared with non-palliative settings. 42
Our meta-analysis also showed, on average, more home deaths in the intervention groups. The more intensive collaboration with primary care and the provision of medical and nursing care at home could have resulted in both patients and care professionals feeling confident that a “comfortable” death could be achieved at home. Furthermore, in many studies, advance care planning was part of the intervention, and open discussions about the preference to die at home could have increased home deaths.43,44 By choosing home deaths as an outcome, we did not incorporate patients who died in hospice, which is the second-most reported preferred place of death. 45 Preferably, the outcome measured would have been the preferred place of death; however, this outcome was only reported in two studies.33,35 This finding is not surprising, because the preferred place of death is often not known for all patients and is subject to change over time. 46 In the study with the largest effect on home deaths, patients in the intervention group explicitly chose home care, whereas the control group did not, and the incentive to continue care at home until death might therefore be high compared with other studies. 32
Limitations
The heterogeneity of the included studies was high, which is an important shortcoming in many reviews on palliative care. We aimed to improve the comparability of the effects in the included studies by using two outcome measures that were available for all patients, instead of more frequently used outcomes, such as quality of life, that can be measured with a wide variety of scales. Nonetheless, the interpretation of our findings, and especially the meta-analysis, should be considered within these limitations. In addition the small number of studies included within the analysis of the hospital-based teams and case-management intervention makes it difficult to draw meaningful conclusions. Furthermore, the quality of the included studies varied as well. Most studies were of moderate quality or showed at least some potential bias. Interestingly, although all interventions studied could be described as complex interventions, 47 almost none of the studies included adherence to protocol or reported on it in a separate study. 48 Jordhøy et al. 31 did describe failing implementations as important limitations in their study. Failures in implementation are not necessarily limitations if clearly reported. Understanding why implementation failed and how such failure could have affected the results is important so others can learn how to improve future studies and care programs.
Conclusion
This review and meta-analysis of transmural team-based collaborations between hospital and primary care professionals in palliative care showed the interventions lowered hospital admissions and increased the number of patients dying at home. Hospital-based teams that follow patients at home seem to have the largest impact on these outcomes; however, the heterogeneity of the included studies limited strong overall conclusions.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221135616 – Supplemental material for Effectiveness of transmural team-based palliative care in prevention of hospitalizations in patients at the end of life: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221135616 for Effectiveness of transmural team-based palliative care in prevention of hospitalizations in patients at the end of life: A systematic review and meta-analysis by Isabelle Flierman, Elske Gieteling, Marjon Van Rijn, Bastiaan Van Grootven, Iris van Doorne, Faridi S Jamaludin, Dick L Willems, Majon Muller and Bianca M Buurman in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163221135616 – Supplemental material for Effectiveness of transmural team-based palliative care in prevention of hospitalizations in patients at the end of life: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-pmj-10.1177_02692163221135616 for Effectiveness of transmural team-based palliative care in prevention of hospitalizations in patients at the end of life: A systematic review and meta-analysis by Isabelle Flierman, Elske Gieteling, Marjon Van Rijn, Bastiaan Van Grootven, Iris van Doorne, Faridi S Jamaludin, Dick L Willems, Majon Muller and Bianca M Buurman in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163221135616 – Supplemental material for Effectiveness of transmural team-based palliative care in prevention of hospitalizations in patients at the end of life: A systematic review and meta-analysis
Supplemental material, sj-pdf-3-pmj-10.1177_02692163221135616 for Effectiveness of transmural team-based palliative care in prevention of hospitalizations in patients at the end of life: A systematic review and meta-analysis by Isabelle Flierman, Elske Gieteling, Marjon Van Rijn, Bastiaan Van Grootven, Iris van Doorne, Faridi S Jamaludin, Dick L Willems, Majon Muller and Bianca M Buurman in Palliative Medicine
Footnotes
Availability of data
Protocol, template data collection forms, data extracted from included studies, data used for analyses, analytic code available from the corresponding author on reasonable request.
Authorship
The study was designed by IF, MvR, MM, and BB. Search strategy was designed by FJ. Titles and abstracts were screened by IF, EG, MP, and SB. Selection of studies was done by IF and EG and discussed with MvR, BB. Selection of studies after a search update was done by IF and IvD. Quality assessment and data analysis of included studies was done by IF, EG, and IvD. Statistical analysis was done by IF, EG, and BvG. IF, EG, and MvR wrote the first draft of the manuscript, which was critically reviewed by all authors. All authors approved this version to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMw (The Netherlands Organization for Health Research and Development), grant number 844001103. This study was a sub study of a larger research project.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.