
Abstract
Background:
Existing data on sedation at the end of life indicate challenges in the home care setting, leading to deviations from guidelines or non-provision of sedation.
Aim:
As part of the “SedPall” study, we aimed to explore circumstances in specialist palliative home care, which influence the practice of sedation.
Design:
Semi-structured qualitative interviews (n = 59) and two focus groups (n = 4, n = 5). Recruitment took place via contact persons. We thematically analyzed the transcripts with the Framework Approach, using MAXQDA 2018.2.
Setting/participants:
Physicians, nurses, and other members of the multiprofessional team from 10 palliative care units and seven home care teams.
Results:
Participants reported home care specific circumstances that can be categorized into three interrelated topics. (1) Lack of 24/7 on-site availability, (2) active involvement of the family, (3) challenges regarding teamwork and multidisciplinarity. Participants drew different conclusions from the reported circumstances regarding the feasibility of different types of sedation at home: While some reported to generally use all types of sedation, others stated that some types of sedation are not feasible in home care, for example deep sedation until death. Most participants questioned the applicability of existing sedation guidelines in the home care setting.
Conclusion:
Our data indicate that sedation practices might currently follow the healthcare professional’s attitude or service policy rather than the patient’s need. To avoid hospital admission in manageable cases and ensure that home care specific best practice standards are met, existing guideline recommendations have to be adapted and supplemented by additional supporting measures specific for the home care setting.
Previous studies on sedation at the end of life demonstrate challenges with the implementation of and deviations from specific guideline recommendations in the home care setting.
Additionally, the few existing data indicate that some palliative care specialists do not perform sedation at the end of life at home.
Home care specific circumstances influencing the practice of sedation in specialist palliative home care relate to a lack of 24/7 availability, active involvement of the family, and challenges with teamwork and multidisciplinarity.
Participants’ conclusions from the reported preconditions varied from using all types of sedation at home to restricting all or specific types to the hospital setting.
Three common guideline recommendations seem to be hardly implementable in the home care setting. (1) Continuous monitoring by qualified staff, (2) psychological evaluation in case of existential suffering as indication for sedation, and (3) dose reduction for re-evaluation of symptom burden.
Sedation practice should follow the patient’s need rather than the healthcare professional’s attitude or service policy.
Existing guidelines have to be adapted to the home care setting, and additional recommendations in addition to other supporting measures for all involved parties are necessary.
Introduction
Various terms have been used to refer to sedation at the end of life including “terminal sedation” or “palliative sedation”.1,2 To date, no common definition of these terms exists.3,4 Current terminology, which has been systematically constructed to clarify the concept of sedation, proposes the term “intentional sedation”.5,6 It defines sedation as “the result or process of inducing a state of reduced consciousness by medical means.” Intentional sedation is defined as sedation “as a means of achieving a previously defined treatment goal,” for example, the relief of suffering.5,6 The term “sedation” comprises different types of reducing the consciousness: it can vary from light to deep and can be applied temporarily or continuously until death. Despite intensive research, sedation at the end of life is still controversially discussed.1,7 Existing data indicate considerable variations in sedation practice and attitudes between countries and settings.8–10 Moreover, sedative drug administration poses several challenges for healthcare professionals, for example fears to hasten death, difficult decision-making processes, or concerns about the adequate depth.8,11,12 To meet these variations and challenges, European-wide as well as various country-specific guidelines have been developed, aiming to support healthcare professionals and set standards for best practice.4,13,14
These guidelines primarily focus on the inpatient setting.4,13,14 However, home is the preferred place of death in many countries.15,16 Existing data on the home care setting indicate difficulties with the implementation of specific guideline recommendations, for example continuous monitoring.17–19 Additionally, deviations from guidelines have been identified for the specialist as well as for the general palliative home care setting, for example regarding the decision-making process or opioid use.19–23 The few studies focusing on specialist palliative home care conclude that sedation at home may be used safely and efficaciously.18,23,24 Still, they demonstrate that some palliative home care specialists do not use sedation at home, for example because management is too complex or they lack facilities. 23 However, these studies do not provide information regarding the underlying circumstances leading to these perceived barriers in the home care setting.
Methods
Research question
This study aims to explore home care specific circumstances in specialist palliative home care, which influence the practice of sedation.
Design
This qualitative study (semi-structured interviews and focus groups) was conducted as part of the consortium project “SedPall.” We used Framework Analysis to explore a wide range of different perspectives and experiences regarding sedation in specialist palliative care. Framework Analysis allows to analyze a high amount of data and to compare data within categories as well as within cases, enabling us to gain understanding of a wider variety of viewpoints regarding sedation. Framework Analysis is not aligned with a particular epistemology or ontology. In accordance with the aim of the study, we adopted a constructivist epistemology and idealism ontology. We utilized this explorative approach since qualitative data on sedation practice in Germany are scarce.25,26
Setting
Ten palliative care units and seven specialist palliative home care teams, which were located in twelve cities in Germany.
Population
Physicians and nurses
Additionally, other members of the multiprofessional team participated in the interviews. Inclusion criteria were involvement in at least one case where sedation was applied and sufficient German language skills. In addition, focus group participants needed to have work experience in the home care setting. Interview participants were also allowed to attend the focus groups.
Sampling
Purposeful sampling was used to ensure variation of the sample regarding profession and position, and, as far as possible, regarding age and gender.
Recruitment
Recruitment took place in the participating palliative care units and specialist palliative home care teams for the interviews and in the same seven home care teams for the focus groups. In each participating center, a contact person was involved to inform eligible staff about the study. Interested healthcare professionals were contacted via email or telephone to schedule an interview appointment.
Data collection
We conducted semi-structured interviews and subsequent focus groups. For the interviews, we developed an interview guide based on the literature and own clinical experiences of the consortium. We discussed it with other experienced qualitative researchers in the department and with a qualitative expert group at the LMU University (Supplemental Appendix A).8,27 It covered five main topics with adaptions for the respective profession: Experiences with different types of sedation and understanding of the concept in specialist palliative care, indications and intentions, decision-making process and consent, challenges and opportunities, dying under sedation. The interview guide was piloted in six interviews. Two trained researchers (VH, JB) conducted the interviews in the professionals’ workplaces between July 2018 and September 2019. Field notes were written after each interview. Parallel to the interviews, the research team constantly discussed whether new and important themes emerged. Interviews were conducted until data saturation was achieved.
After indexing the interview material (see data analysis), the influence of home care specific circumstances on sedation emerged as an important theme. The focus group guide was informed by relevant interview categories as well as questions arising in the consortium’s development of recommendations for sedation in palliative care. We discussed the guide additionally with other experienced qualitative researchers in the department (Supplemental Appendix B). It comprised three main aspects: opinions on the feasibility of different types of sedation in the home care setting, necessity of home care specific guideline recommendations, and suggestions regarding specific guideline recommendations. Each focus group was led by a facilitator and co-facilitator, respectively (JG, JB). Due to the COVID-19 pandemic, we conducted the focus groups via video call in September 2020. Digital field notes were written immediately afterward.
We collected data on sociodemographic and professional background of the participants using a questionnaire.
Data analysis
We thematically analyzed the qualitative interviews as well as the focus groups following the Framework approach, using MAXQDA version 2018.2. 25 After familiarization with parts of the interview material, we developed an initial analytical framework, with categories derived both inductively and deductively (close collaboration of VH and JB, with support of ES). The analytical framework was continuously refined while indexing all interviews (JB, VH, SM). The final framework consisted of 12 categories with 0–10 sub-categories, respectively (JB, SM, JG). Subsequently, we used the same procedure for the focus group material. The analytical framework for the focus groups consisted of seven categories without any sub-categories. Key messages of the indexed interview and focus group data relevant to the research question were summarized. We transferred the summaries to an overall thematic sheet with interview/focus group participants in rows and nine themes in columns: (1) Role of the family, (2) Teamwork and multidisciplinarity, (3) Availability, (4) Monitoring, (5) Documentation, (6) Guidelines, (7) Experience with different types of sedation, (8) Link to a palliative care unit, (9) Other general circumstances.
Constant exchange within the project team as well as regular involvement of the PPI group ensured rigor and integrity of analysis. Finally, we presented our results on a final conference, where healthcare professionals, including study participants, could provide feedback.
Ethical issues and approvals
All participants gave their written informed consent. Interviews as well as focus groups were audio-recorded and transcribed verbatim, including anonymization. The study was approved by the Research Ethics Committee of the Medical Faculty at Ludwig-Maximilians-University Munich (reference number 17-792).
Results
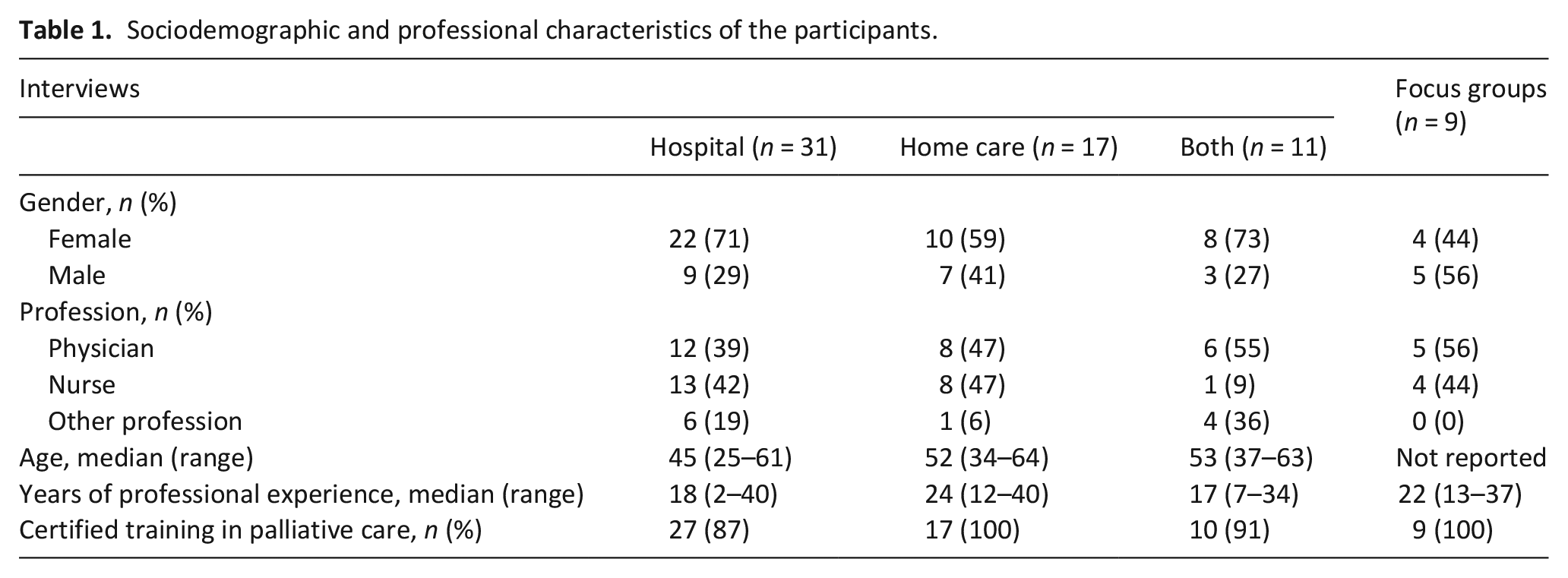
As part of the SedPall study, we conducted 59 interviews and two focus groups (with n = 4, and n = 5 participants). In the interviews, 22 nurses, 26 physicians, and 11 other members of the multiprofessional team participated. The focus groups consisted of four nurses and five physicians. Characteristics of the participants are summarized in Table 1. Only results addressing home care specific aspects will be reported in the following. Results of the interviews pertaining to other research questions of the SedPall study will be reported elsewhere.
Sociodemographic and professional characteristics of the participants.
By exploring home care specific circumstances in specialist palliative home care, which influence the practice of sedation, we additionally identified implications on the feasibility of different types of sedation as well as on the applicability of existing sedation guidelines.
Home care specific circumstances influencing the practice of sedation at home
Participants reported home care specific circumstances that can be categorized into three interrelated topics: (1) Lack of 24/7 on-site availability, (2) active involvement of the family, and (3) challenges regarding teamwork and multidisciplinarity.
Lack of 24/7 on-site availability
Lack of 24/7 on-site availability and limited staff were the predominantly mentioned home care specific aspects. Participants reported that patients can usually be visited once to twice a day, with additional telephone consultations if needed. In case of difficulties with a sedated patient, the structures hardly allow staying with the patient for a longer period. Especially weekends, nights, and times when additional emergencies of other patients emerged were reported to be challenging for the team. Due to the lack of 24/7 on-site availability, continuous monitoring of sedated patients by qualified staff is impossible. Thus, monitoring is predominantly carried out by the family or other services such as nursing services.
“[. . .] so, on the ward you can just look in every half-hour or leave the door open and you have a constant supervision. While one is at home, of course, you leave the relatives and patients to themselves and simply no longer control the situation.” (Participant, focus group 2)
Additionally, the home care setting was described as a rather slowly-reacting system as it takes some time until a team member can be on-site. Fast treatment adjustments are not possible and qualified staff is not present in case of emergencies. As a result, many participants reported difficulties with titration of sedatives. They described a risk of administering higher doses than actually needed due to the missing opportunity of quick dose adjustments. Conversely, they perceived also a risk of insufficient depth of sedation as they usually start with low doses and the family might be too cautious regarding additional as-needed doses.
“[. . .] that one is more inclined to perhaps, I’ll say now, knock-out some patients, even though it may not be necessary at that moment. [. . .] Because then there is also the other side, overdosing and underdosing. If you say that there is something being administered continuously, you [the relatives] are more restrained with extra doses or additions and the patient can be underdosed as well as overdosed.” (Interview participant 1, physician)
However, some participants also mentioned a positive aspect of this slowly reacting system: It allows the patient more opportunities for changes in wishes and decisions.
“But the advantage, I just remembered, of a sluggish home care system at the beginning of palliative sedation is of course that the patient can still decide. I remember one, a medical colleague [. . .] he wanted very deep sedation, really wanted to sleep through it, so to speak, but now the midazolam did not take effect as desired and was much slower and, yes, he reached a state where he could simply give us to understand through eye contact that the sedation is enough for me, that was incredibly impressive. [. . .] I think in an inpatient setting we would have sedated him faster, deeper possibly or started differently than we did at home.” (Participant, focus group 2)
Active involvement of the family
Participants reported that in the home care setting the family is actively involved in the medical care of the patient, while they have a predominantly observing role in the hospital setting. The accounts illustrated that treatment is heavily based on the families’ monitoring. In addition, relatives are often responsible for drug administration. Their active involvement was perceived to be a relief for relatives during the dying process as well as for the grieving process.
“It is an opportunity to really make an active contribution [. . .] and I experience this again and again, this deep gratitude and then also in the grieving processes this feeling, yes, I was able to make it possible for him that he was really at home until the end. [. . .] and I have become a part of achieving this and . . . that doesn’t apply to everyone, but for some people it is a very, very strong element.” (Participant, focus group 1)
However, some participants acknowledged that this amount of responsibility can also be a burden. They particularly emphasized the risk that relatives might feel responsible either for the patient’s death because of their drug administration or for the necessity to induce a deep sedation. Moreover, participants described as-needed doses administered by relatives to be problematic as they often struggle to assess the patient’s actual need. The necessity to delegate that amount of responsibility to the family was partially described as burdensome for the team.
“[. . .] and then we tell the relatives, well, if he were a bit restless now, then they could turn this dial [of the syringe driver] a bit, and that was always ‘whew’ for me, so then I thought, my God, what am I asking of someone? What do I expect of the wife or the husband or the daughter or the son, that they should somehow adjust dosages themselves? So, that’s quite different from being on the ward.” (Participant, focus group 2)
According to the participants, the duty of a specialist palliative home care team to care not only for the patient but also for the family is therefore particularly important in the context of sedation. Initially, the team has to clearly state the responsibilities, determine the relatives’ scope regarding drug administration and provide guidance. It is the team’s responsibility to recognize to what extent a family is able to take over the required tasks and when they might be overstrained, in order to protect the family as well as the patient. In addition, participants described a risk of decisions reflecting more the family’s suffering than the patient’s, as the patient is only rarely seen alone. Participants’ accounts revealed that extensive communication is necessary to meet these demands.
Challenges regarding teamwork and multidisciplinarity
Participants reported that teamwork processes differ significantly from the hospital setting. Different team members are not as easily available for discussion, which is particularly challenging when quick decisions are necessary. Multidisciplinarity differs from the hospital setting regarding two aspects. Involving further disciplines to help in the decision-making process, for example psychologists or ethics consultants, is either more time-consuming than in the hospital setting or impossible. Furthermore, third parties have to be included in the decision-making and treatment process, in particular, the patients’ general practitioners and home care nursing teams. Reaching joint decisions was reported to be challenging sometimes due to very different professional backgrounds and working processes. Participants mentioned that home care nursing teams often struggle with the care of deeply sedated patients, requiring additional instructions and support from the specialist palliative home care team.
Feasibility of different types of sedation at home and implications for practice
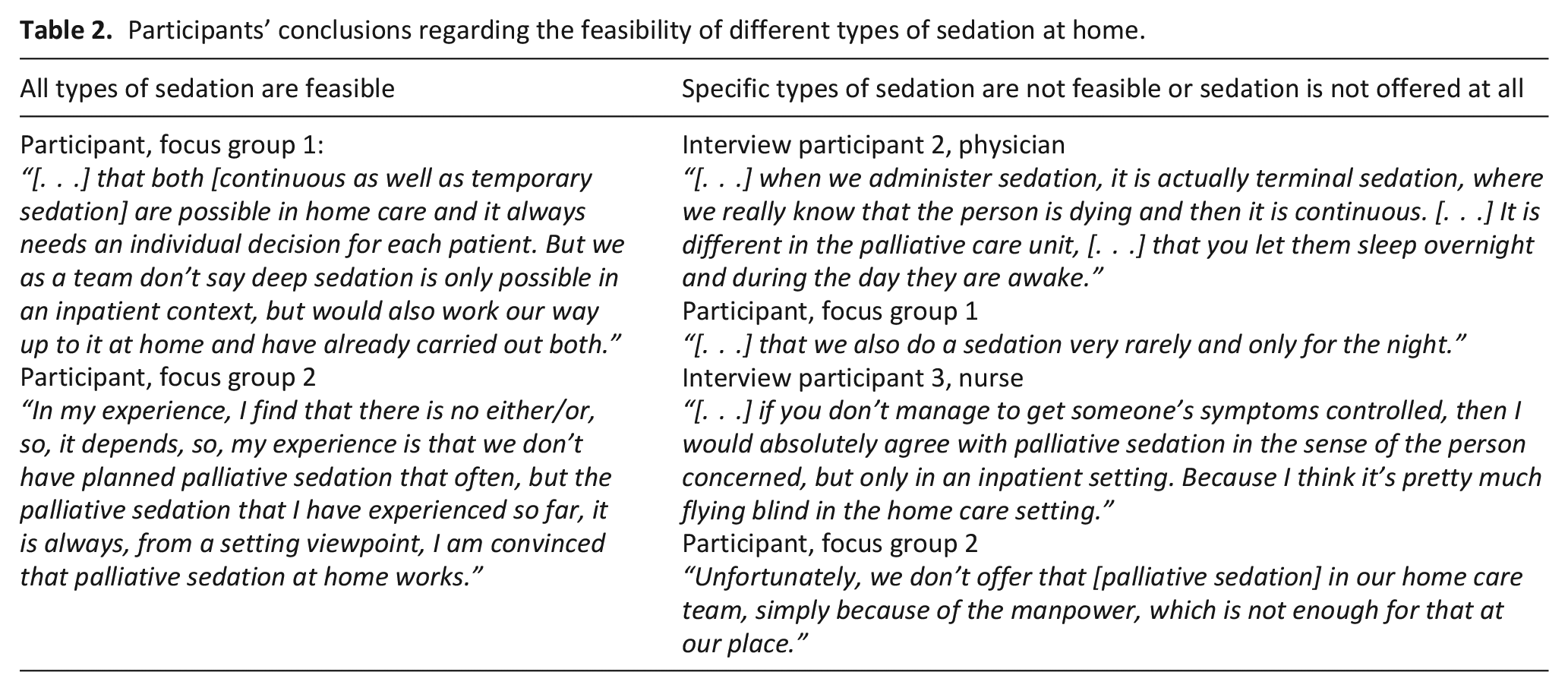
Participants draw very different conclusions from the reported home care specific circumstances regarding the feasibility of different types of sedation at home (Table 2). Some participants stated that deep sedation until death is not feasible in the home care setting, others refused to use temporary sedation. Main reasons for both opinions were the described lack of continuous monitoring by qualified staff and limited availability of a multi-professional team. Especially if no home care nursing team was involved, participants refused to use deep sedation at home. In contrast, other participants reported that, always depending on the individual family, they are able to use all types of sedation. Some perceived the limited multi-professionalism as reduction of “medical noise” and concluded that deep sedation until death is feasible even best in the home care setting. Regarding limited 24/7 on-site availability, they argued that situations in which deep sedation is needed are very rare and last only a limited period of time. These exceptional situations can be managed with adequate preparation and willingness of the whole team. Focus group discussion indicated that the general decision whether to offer different types of sedation at home is not dependant on the employee-patient-ratio.
Participants’ conclusions regarding the feasibility of different types of sedation at home.
Some participants regretted not being able to offer patients the opportunity of sedation at home and described hospital admission in these cases as burdensome. Additionally, patients sometimes had to be hospitalized after the decision to start sedation at home was made, for example due to overburdening of the family. In these situations, the start of sedation was postponed as the hospital healthcare professionals had to reassess the patient’s situation, leading to dissatisfaction for all parties involved: Patients and their families expected a prompt start, as they have already gone through the entire decision-making process and are suffering. The home care team could not keep the promise to start sedation promptly, and the hospital team was faced with a demanding patient and home care team.
Participants, who offer sedation at home, drew two main conclusions from the home care specific conditions for the practice of sedation in this setting. First, documentation was perceived to be of great importance. Shared documentation enables the involvement of all relevant parties and creates a sense of common responsibility. However, the participants emphasized that there are no common standards for documentation, leading to differences in handling between the teams. Second, compared to the hospital setting, further preparative considerations are necessary: for example evaluation of family factors, additional parties to be involved, availability of equipment.
“[. . .] especially in the home care setting, where different documentation systems are in place - the nursing service has its own documentation system - and if you find a common paper there, which you can deposit with the patient, that always remains there on site, of course, then everyone has the possibility to view the information. Even the relatives are allowed to see and read it and there are also things that they enter there themselves. So, everyone is on board and everyone is responsible, of course. The paper can also be a connecting element.” (Participant, focus group 2)
Applicability of sedation guidelines in the home care setting
Most participants expressed critical views on the applicability of existing sedation guidelines in the home care setting. They mostly referred to three guideline recommendations from the EAPC framework, which were described to be hardly implementable or not reasonable 28 : (1) Continuous monitoring by qualified staff, especially regular monitoring of vital signs, (2) psychological evaluation in case of existential suffering as indication for sedation, and (3) dose reduction for re-evaluation of symptom burden. In addition, participants reported that precise specifications for this highly individual care situation can cause difficulties in the home care setting, as the home care team has to justify decisions to third parties. They criticized that in case of accusations after the death of the sedated patient, lawyers can only refer to existing guidelines, but some recommendations are not applicable in the home care setting.
“[. . .] we are still always happy when we are allowed to do the post-mortem examinations and no KV [Association of Statutory Health Insurance Physicians] doctor is called and asks questions – how high was the dosage?” (Participant, focus group 1)
Some participants stated a need for guidelines, which comprise the requirements a home care team has to fulfil to be able to offer different types of sedation at home. Additionally, it was mentioned that guidelines should include recommendations regarding the home care specific aspects of interaction and further preparative considerations. According to the participants, such guidelines could support the process of clarification, whether and under which circumstances sedation can be offered, and help home care teams gain confidence to offer sedation.
Discussion
Main findings
This qualitative study identified home care specific circumstances influencing the practice of sedation at home. Circumstances were categorized into three interrelated topics: (1) Lack of 24/7 availability, (2) active involvement of the family, (3) challenges regarding teamwork and multidisciplinarity. Some participants restricted all or specific types of sedation to the inpatient setting due to the reported circumstances. Others reported to generally use all types of sedation at home, emphasizing that it is always case-specific. Moreover, participants reported challenges with hospital transfer in the context of sedation and expressed a critical view regarding existing sedation guidelines.
What this study adds
A previous quantitative study on sedation practice at home has shown that part of palliative home care physicians preferred to refer patients to the hospital for “palliative sedation” or did not administer “palliative sedation” at home. 23 Different authors assumed that the decision to sedate a patient at home might reflect the provider’s attitude or service policy rather than the patient’s preferences or needs.29,30 Our results revealed that although all participating specialist palliative home care teams are faced with the same home care specific circumstances, they draw very different conclusions regarding the feasibility of different types of sedation. As sedation is an important end of life measure, the opportunity to receive it should not depend on the respective specialist palliative home care team. Porzio et al. 31 for example defined in their study criteria for the eligibility for deep continuous sedation at home, including absence of any other sources of suffering in the family and residing no farther than 20 min away from the hospital. Ineligible patients were admitted to an inpatient palliative care unit. 31 Similarly, our participants wished for guidelines comprising requirements that have to be fulfilled to be able to offer different types of sedation at home. Uniform criteria can help to generate confidence for the home care teams and therefore help to make best practice sedation at home available for all patients who fulfil these criteria. This means that patients not meeting the respective criteria for different types of sedation have to be admitted to hospital to receive sedation. Our interviewees described hospital admission in these circumstances as challenging for the whole system, confirming the results of a previous study where 31% of the specialist palliative home care teams evaluated hospital admission as “very to extraordinarily burdensome”. 32 To reduce this burden as far as possible for all parties involved, the interface between specialist palliative home care and inpatient care needs to be enhanced.
Conversely, home care teams need to be supported to avoid admission to the hospital for sedation in manageable cases. Our results demonstrate that existing sedation guidelines have to be adapted for the home care setting. Although various authors have repeatedly called for adapted guidelines, recommendations are still predominantly focused on the inpatient setting.4,13,14,18,29,30 According to our interviewees, especially guideline recommendations regarding continuous monitoring by qualified staff, psychological evaluation in case of existential suffering, and dose reduction for re-evaluation of symptom burden are hardly or not implementable in the home care setting. These results have informed the recommendations on sedation in specialist palliative care which our SedPall study group has developed. 5 We have formulated recommendations regarding these aspects in a way, which defines basic criteria to uphold crucial standards irrespective of general applicability in all settings, but leaves room for highly individual decisions in the home care setting. Finally, our results demonstrate the need to add best practice criteria regarding home care specific aspects to existing recommendations. Specifically, steps to assess the home care situation and to improve the quality of involvement of the family as well as other professionals such as general practitioners and home care nursing teams, have to be taken. A previous study among home care nurses assumed communication problems as important cause for refusal of “palliative sedation” by the caring nurse. 21 Both family and other professionals require respective information and training by the specialist palliative home care team. In Germany, lay carers are allowed to administer medication as prescribed by health professionals. However, our results indicate different challenges. Assessing the need regarding as-needed doses may be difficult for lay carers due to lack of experience, and the responsibility associated with such monitoring and drug administration may be burdensome for some relatives. Trainings for lay carers, for example for subcutaneous as-needed doses, may reportedly play a key role in achieving adequately symptom controlled home deaths. 33 Additionally, previous studies have suggested educational training as well as simulation programs for professionals, especially regarding types of sedation that are only rarely performed.21,34 In accordance with a previous study, our participants also stressed the value of shared documentation involving all relevant parties. 21 Recommendations and practice protocols should specify these home care specific preparative tasks, and should be supplemented by further supporting measures, for example standard documentation tools for all parties involved and information leaflets regarding sedation at the end of life for family and other professionals.
Strengths and weaknesses
The main strength of this study is the inclusion of physicians, nurses, and other members of the multiprofessional teams from palliative care units as well as home care teams from different sites in Germany. We included participants of different professions, age, gender, and positions. Moreover, we conducted in-depth interviews as well as focus group discussions. By this, we were able to obtain detailed and comprehensive insights of home care specific circumstances. Using the Framework approach produced highly structured outputs, which facilitated a holistic overview of the entire data. The study results must be considered in the context of the following weaknesses: As we did not receive any information on reasons for non-participation, some perspectives may not be fully taken into account. Furthermore, sedation at the end of life is a sensitive issue, entailing the risk of social desirability bias. The research team was aware of the risk and tried to minimize it by sufficient information, the interview guide, training of the interviewers, and the two data sources (individual interviews and focus groups).
Implications for clinical practice and policy
This study provides important insights on the necessity to adapt existing sedation guidelines to the home care setting. Moreover, it highlights that there is a need for additional recommendations, especially regarding eligibility criteria, multiprofessional teamwork, and involvement of the family. Appropriate guideline recommendations together with additional supporting measures for all involved parties can help to ensure that sedation practice follows the patient’s need rather than the healthcare professionals’ attitude or service policy. Development and implementation of these measures should be rigorously evaluated.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221128938 – Supplemental material for “It’s pretty much flying blind in the home care setting”: A qualitative study on the influence of home care specific circumstances on sedation in specialist palliative home care
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221128938 for “It’s pretty much flying blind in the home care setting”: A qualitative study on the influence of home care specific circumstances on sedation in specialist palliative home care by Sophie Meesters, Jeremias Bazata, Violet Handtke, Jan Gehrmann, Sandra Kurkowski, Carsten Klein, Claudia Bausewein and Eva Schildmann in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163221128938 – Supplemental material for “It’s pretty much flying blind in the home care setting”: A qualitative study on the influence of home care specific circumstances on sedation in specialist palliative home care
Supplemental material, sj-pdf-2-pmj-10.1177_02692163221128938 for “It’s pretty much flying blind in the home care setting”: A qualitative study on the influence of home care specific circumstances on sedation in specialist palliative home care by Sophie Meesters, Jeremias Bazata, Violet Handtke, Jan Gehrmann, Sandra Kurkowski, Carsten Klein, Claudia Bausewein and Eva Schildmann in Palliative Medicine
Footnotes
Acknowledgements
We thank all the nurses and physicians who shared their experiences and views in the interviews and focus groups. In addition, we thank the contact persons at the participating centers for supporting the recruitment of participants. Finally, we thank Philip Saunders (Language Service) for translating the quotes as well as our Patient and Public Involvement group (D Bein, C Doennhoefer, I Flemmer, I Hellwig, K-H Kurz, EK Niesmann, M Wein) for continuing support of this project and discussion of emerging results.
Authorship
Study concept and design: Eva Schildmann, Jeremias Bazata, Violet Handtke, Jan Gehrmann, Sophie Meesters, with support of Claudia Bausewein. Acquisition of data: Jeremias Bazata, Violet Handtke, Jan Gehrmann, Sophie Meesters, Sandra Kurkowski, Carsten Klein. Analysis of data: Sophie Meesters with support of Jeremias Bazata, Violet Handtke, Jan Gehrmann, and Eva Schildmann. Interpretation of data: all authors. Drafting of the manuscript: Sophie Meesters. Critical revision of the manuscript for important intellectual content: all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the Bundesministerium für Bildung und Forschung (Federal Ministry of Education & Research), 01GY1702B (SedPall).
Research ethics and consents
All participants gave their written informed consent.
Data management and sharing
Transcripts as well as central and thematic charts are available from the authors upon request, under the provision that the research ethics committee of the Medical Faculty at Ludwig-Maximilians-University Munich agrees.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.