
Abstract
Background:
Collaboration between parents and professional care providers is an essential part of pediatric palliative care. As children are embedded in family systems and many of the patients are not able to communicate verbally, their parents are the primary interaction partners for palliative care providers. International standards for pediatric palliative care in Europe state that parents should be supported, acknowledged as the primary carers and involved as partners in all care and decisions.
Aim:
To find out through which care practices pediatric palliative care teams shape collaboration with parents in everyday care.
Design:
Ethnographic method of participatory observations. Field notes were analyzed using thematic analysis.
Setting/participants:
Researchers accompanied three pediatric palliative care teams on home visits to eight different families caring for a child with life-limiting conditions.
Results:
Care practices of palliative care teams were characterized by familiarity, a resource-oriented attitude, empowerment of parents, shared decision-making and support for parents. Palliative care teams not only provided palliative medical treatment for the children, but also developed a trusting care partnership with parents. The teams employed a sensitive and multifaceted communication style in their collaboration with parents.
Conclusions:
Care practices in pediatric palliative care require time, communication skills, and a high level of psychosocial competence, to develop a trusting, collaborative relationship with parents. This should be taken into consideration when establishing pediatric palliative care structures, preparing guidelines, training staff, and deciding upon appropriate remuneration.
Pediatric palliative care consists of more than medical end-of-life care. It aims to enable patients to live as self-determined as possible, remain with their families, improve quality of life, alleviate symptoms, and avoid hospitalization.
Parents are the primary caregivers for children with life-limiting conditions and primary interaction partners for palliative care teams.
According to guidelines, palliative care teams should collaborate with parents in daily care.
Our analysis shows how specialized palliative care teams developed trusting care partnerships with parents in daily care.
Care practices of specialized outpatient pediatric palliative care teams were characterized by familiarity, a resource-oriented attitude, parent empowerment, shared decision-making, and support for parents.
These care practices were implemented in daily care by extensive communication.
Developing trusting collaboration with parents demands communication skills, psychosocial competence, and the time to treat each case individually.
Specialized outpatient pediatric palliative care requires specialized staff that have been extensively trained and have sufficient time and resources to provide such intensive care.
The importance of communication work should be taken into account when formulating guidelines, building palliative care structures, and deciding upon remuneration.
Introduction
“Parents are central to a child’s wellbeing. They should be present and involved in all aspects of their child’s care.” 1 This is one of the standards for pediatric palliative care formulated by the European Association of Palliative Care, emphasizing the important role of parents in pediatric palliative care. The provision of satisfactory care for children without involvement of their parents is unimaginable because children are deeply embedded in the family system.2,3 Many children and adolescents receiving palliative care have non-oncologic conditions, such as neuromuscular or neurodegenerative diseases. Such diseases which are often rare, have multiple and complex symptoms, and an uncertain prognosis.2,4–7 Thus the children and their families often need intermittent care in situations of crisis for several years. 8 As many of the young patients are not able to speak for themselves (because of neurological diseases, or their young age), parents act not only as caregivers, but also as representatives for their children.
International guidelines agree that for care to be appropriate, professional healthcare providers should acknowledge the importance of the parental role in pediatric palliative care by supporting parents and involving them in care and decision-making.1,9,10 Parents need to be empowered to make decisions, taught how to provide appropriate care, and to receive emotional support in coping with psychosocial issues.8,11 International research shows that parents of children with life-limiting conditions want care providers to take a sensitive approach that considers the entire family unit, while also addressing non-medical concerns.12–14 Narrative interviews we conducted with parents showed that parents wish for pediatric expertise, honesty, psychosocial support, an individualized approach, to experience self-efficacy and be recognized as experts in treating their children. 14
But how exactly can these goals and requirements be realized? The existing literature focuses on what parents wish and need, but not on how collaboration actually occurs through caregiving practices or professional strategies.12,14–16
In this article, we present the results of participatory observations in order to identify the care practices trough which palliative care teams work together with parents in the home care of their children.
Methods
Design
The presented data is part of the study “Evaluation of specialized outpatient palliative care in the German state of Hesse (ELSAH),” which aimed to explore the specific needs of children and adolescents receiving specialized outpatient pediatric palliative care and to make recommendations for the inclusion of their needs into the national rule of procedure on specialized outpatient palliative care. 17 As part of this project, we conducted participatory observations 18 with the three specialized outpatient pediatric palliative care teams in Hesse, Germany and accompanied them during home visits. In this paper, we present the findings of a thematic analysis and focus on professional strategies of the palliative care teams in interaction with parents. As ethnographic methods enable researchers to observe practices and recognize underlying knowledge through the immediate experience of social practices,18,19 we chose this method to present a thick description of the care practices of the palliative care teams in their everyday work with parents.
Setting
To address the special and challenging situation of a terminally ill child and to provide family-centered care, children in Germany with life-limiting conditions involving a high burden of illness, complex symptoms and extensive care needs are eligible for specialized outpatient pediatric palliative care as a special form of palliative care that is delivered at home. 20 It is provided by an interprofessional team consisting of physicians, palliative care nurses and, in some cases, psychologists and social workers. It comprises palliative medical and nursing care, a 24/7 on-call service, psychosocial support, and coordination of care with local health care providers.
Population
In Hesse, there are three specialized outpatient pediatric palliative care teams, which focus solely on the home care of children with life-limiting conditions. Each team consists of about 10 team members. All teams participated in our study. The only formal exclusion criterion for teams and families was the absence of a signed consent form.
Sampling approach
Our aim was to observe the work of all three Hessian teams and to create a sample of families that reflects the daily work of the teams. Since there are only a limited number of children in active care at any one time and it was important to us to be considerate of the families’ current situation, we used convenience sampling.
Recruitment
We asked the three Hessian specialized outpatient pediatric palliative care teams whether they would allow us to join them during home visits. All teams agreed to participate and recruited families they currently care for and for whom they felt the researchers’ accompaniment was reasonable. They informed families verbally about the project and handed them study information and a written informed consent form. The family members first agreed verbally and at the latest on the day of the visit we received their written informed consent.
Data collection
Data collection and analysis were conducted by a team consisting of researchers from the fields of sociology, public health, psychology and medicine, all of whom had been trained in the use of qualitative methods. The researchers had prior contact with the specialized outpatient pediatric palliative care teams through the study and in some cases already met individual team members. In March and April 2019, we accompanied the three Hessian teams on eight home visits. Of these, four visits were accompanied by two researchers, and four by one. During the visits, we took field notes to document:
The travel time, duration of the visit, and the participants.
Information on the child, including age, diagnosis, medical history, state of health, duration of and access to specialized outpatient pediatric palliative care (observed and/or reported by the palliative care team members during or between the visits).
Observations made during the visit (in particular: observations on welcome situations, an outline of the care situation and the arrangement of persons in the room, interaction between palliative care team members, parents and the child, language and decision-making).
Afterwards we developed observation protocols 18 from our notes on each case. When two researchers were present, they combined their notes and agreed on one report.
Data analysis
Two researchers used thematic analysis 21 to analyze the observation protocols inductively in terms of the care practices employed by specialized outpatient pediatric palliative care team members in their collaboration with parents. The researchers discussed their codes, and agreed on a final coding system, which was then used to code all observation protocols using MAXQDA18 software. During the analysis, we developed codes to describe the actions of the palliative care teams and sub-codes to specify those actions empirically. Afterwards, the analysis was re-focused and the codes were sorted into themes, which are presented in the results section.
Ethical consideration
The ethics committee of Goethe University Frankfurt/Main, approved the study on April 10, 2017 (ID: 142/17). All participants (families and specialized outpatient pediatric palliative care team members) received information on the study, data anonymity and their right to terminate participation at any time and provided their written informed consent. All obtained data were pseudonymized. To take into account the vulnerability of the families, we had the palliative care teams assess which families were suitable to participate in the study.
Results
We were present at eight home visits (four visits accompanying one specialized outpatient pediatric palliative care team, and two accompanying each of the other two teams). All visits were conducted by a physician and a palliative care nurse. The visits lasted from 45 to 90 min, and averaged 60 min. On average, the teams had to drive 34 min to travel from one family to another. The characteristics of the visits are described in Table 1. All visits were planned visits and no acute life-threatening crisis situations. However, the care always took place because the child’s health status was not stable.
Characteristics of accompanied home visits.
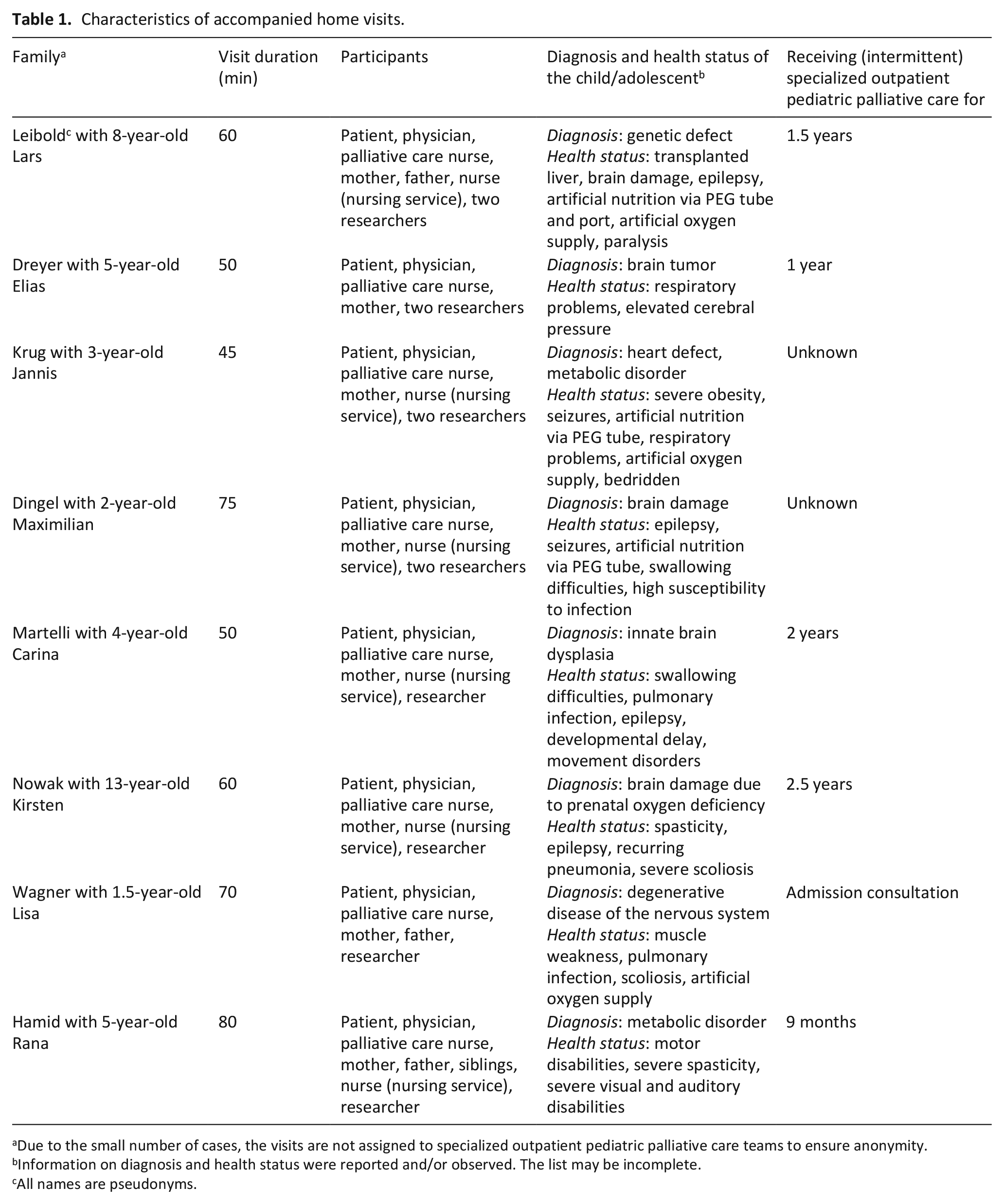
Due to the small number of cases, the visits are not assigned to specialized outpatient pediatric palliative care teams to ensure anonymity.
Information on diagnosis and health status were reported and/or observed. The list may be incomplete.
All names are pseudonyms.
In the following section, we describe the care practices of the specialized outpatient pediatric palliative care teams. Because physicians and nurses worked very equally and on eye-level during all visits, we decided not to distinguish between the professional groups in the analysis, but refer to both as “team.” We provide excerpts from observation protocols to show examples of situations experienced during the home-visits. Since the strategies of the three teams turned out to be very similar, differences between the teams are not discussed.
Familiarity
Care was characterized by a familiarity between the specialized outpatient pediatric palliative care teams and parents. Establishing trust and familiarity was the cornerstone of collaboration. Familiarity was visible in routine tasks that took place as a matter of course and required no further explanation. These routines showed that the palliative care teams knew the specifics of every family and had become adapted to them. While traveling to each individual family, the team members were able to describe each case from memory. When we arrived at the families’ homes, for example, the teams always knew whether to take off their shoes or leave them on:
We arrive at the family’s house and ring the bell. Mr. Wagner opens the door and invites us to come in. While we are still standing in the hallway, he has already disappeared into the living room. The palliative care-team members take off their shoes without being asked and follow Mr. Wagner into the living room. (Observation protocol Wagner)
This comportment showed exemplarily that the teams entered the family home respectfully and followed the rules that applied there. In one case, when visiting the Hamid family, the team took the time to stay, eat some cake and drink coffee. The physician later explained that they always eat cake and drink coffee when visiting the Hamids because it is the way the family expresses gratitude and the moment when family members speak openly:
It is exactly over this one cup of coffee that the parents report problems, and not when they are asked directly, the palliative care nurse remarks after the visit. (Observation protocol Hamid)
Overall, the teams moved very comfortably around the families’ homes. They knew their way around and were allowed to move freely. Sometimes, communication between parents and the palliative care team was so fast and performed so routinely that the researchers were unable to follow everything. It showed that their shared experiences had enabled them to become familiar with one another and to develop into a well-coordinated team. Furthermore, parents and team members also talked about private matters concerning the parents such as a mother’s pregnancy, vacations, house renovations, careers, weekend trips, and siblings’ hobbies.
Resource-oriented attitude
We also observed that no matter how limited a child’s abilities were, the teams never behaved as though nothing more could be done, but displayed a resource-oriented attitude in their care practices. For example, when visiting the Leibold family:
The physician asks Ms. Leibold to tell us what her son is able to do, whereupon the mother tells us that he can breathe autonomously, manage bowel movements independently, cough alone and is dry at night ‘like a big boy.’ (Observation protocol Leibold)
This observation showed that mother and physician assessed the child’s development in the same terms. Such behaviors are regarded as “normal” in 8-year old children, but in the present context, age was irrelevant to the interpretation of the condition. Both mother and physician focused on his capacities and skills, regardless of age.
The specialized outpatient pediatric palliative care teams took an interest in what the parents thought about their children and not only talked about illness and symptoms, but about what the child can do, how well it is developing, whether it laughs etc.
Empowering parents to care for their children
Specialized outpatient pediatric palliative care teams empowered parents to care for their children themselves by providing knowledge and guidance. They gave general information on the effectiveness of drugs and the origin of symptoms, and provided detailed instructions to parents on, for example, how to administer medications and nurse their children:
As some people react a little sensitively to eucalyptus, she [the mother] is encouraged to try the cream on a small area first to see whether Kirsten can tolerate it. Then she shows the mother on her own back (that of the doctor) exactly where she should apply it. (Observation protocol Nowak)
This parent empowerment created a basis for shared decision-making.
Shared decision-making
We observed that by sharing knowledge, specialized outpatient pediatric palliative care teams and parents could weigh up and evaluate information in order to reach a common decision. The first thing the teams did at the beginning of the visits was to ask the parents for their opinion on their child’s current condition.
The physician asks the mother whether the change in the inhalation from dry to moist has helped, and what she thinks about it. She answers that with infections the damp inhalation is better, otherwise dry, which the physician immediately confirms. (Observation protocol Krug)
They first asked about symptoms, drug compatibility, side effects, physical comfort etc., and then based their subsequent work on the information and assessments the parents had given them. We observed many situations in which parents decided what was relevant. Either the parents said directly what was important to them during a visit, and the team members conducted themselves accordingly, or the palliative care team asked what they wanted.
Afterwards, the physician asks the mother: “Is there anything else that is important to you?” The mother then describes a conversation with several hospital doctors about a planned change in Lars’ medication. (Observation protocol Leibold)
Even minor concerns, such as small skin rashes, were treated as important and not dismissed as mere trifles. The team members asked parents about their treatment preferences. In the case of the Nowak family, for example, mother and physician talked about suppositories and tablets for the stomach that Kirsten, the child, receives. The physician asked the mother which she would prefer to reduce first, whereupon the mother answered that she would rather reduce the suppositories. The specialized outpatient pediatric palliative care team recorded the decision and decided to come back after 2 or 3 days to see how it had worked out.
Another example involving the Wagner family demonstrated shared decision-making in the treatment of an infection:
The physician asks Ms. Wagner whether she would prefer to begin an antibiotic therapy early or whether she would rather wait a little. The physician and Ms. Wagner then jointly weigh up the pros and cons. Finally, both agree that the signs indicate a viral infection. [. . .] Ms. Wagner says that she prefers to administer drugs without delay. The physician nods. Both agree that an additional bacterial infection should be avoided. (Observation protocol Wagner)
At the same time, the teams also advised the parents to do certain things, or explained that a specific treatment or medication was more suitable or important in the current situation. With their medical and nursing expertise, they set a framework within which the parents could decide. In doing so, the professionals treated the parents as experts and demonstrated confidence in their ability to make the right decisions.
Caring for parents and their concerns
Team members not only treated the patients but also addressed and provided psychosocial support for the whole family. In several cases, the palliative care teams focused on the parents as individuals, not only as intermediaries between themselves and the children, and inquired about their resources. They did this by creating room for parents to talk about their concerns and uncertainty. For example, Mr. Hamid told the team members that he found it extremely difficult to enter his daughter’s bedroom because it upset him to see her in her current condition. After leaving the Hamid household, the palliative care nurse and the physician described how important it was for Mr. Hamid that they take some time to sit down and talk to him about his fears and problems. When we visited the Dingel family, Ms. Dingel, who is pregnant, spoke to the team about problems with her older son, who clings to her because he fears she will return to hospital for a long period, as was the case when her sick son was born. When visiting the Dreyers the mother talked about disagreements with her husband on how to deal with Elias and his symptoms.
In such situations, specialized outpatient pediatric palliative care team members took the time to listen to parents’ concerns, demonstrated empathy and pointed out support options where possible. When visiting the Nowak family, for example, Ms. Nowak and the team talked about a planned conversation on the contingency measures that should be adopted in case of an emergency:
Mrs. Nowak says her husband is terribly afraid of the conversation. She says it is terrible for him to talk about it, or even to think about Kirsten dying. He says he can’t think about anything other than that meeting. The palliative care nurse asks if there is anything they can do to perhaps make it a little easier for her husband. Thereupon the physician suggests bringing forward the appointment so that it does not take place on the last day of Mr. Nowak’s vacation. She says he would certainly enjoy his vacation more if he had the conversation behind him. (Observation protocol Nowak)
We could observe that teams showed parents their appreciation of their care efforts. They mentioned the multiple burdens and the energy needed to deal with it, and did not take it for granted. If they felt that parents needed further support, the teams suggested relief services, such as respite-care, hospice stays or treatments at home. It became clear that the palliative care teams also considered the well-being of parents as their area of responsibility and acted accordingly.
Discussion
Our analysis showed that the care practices of specialized outpatient pediatric palliative care teams were characterized by familiarity, a resource-oriented attitude, parent empowerment, shared decision-making, and support for the parents. Through extensive communication, the teams formed collaborative relationships and provided family-centered care that actively involved parents. By doing so they succeeded in meeting the requirements of the international standards for pediatric palliative care 1 as well as the needs of parents for support and empowerment.12,13,22,23
The care practices described above enabled the specialized outpatient pediatric palliative care teams to meet the needs that we previously identified in a series of narrative interviews. 14 Parents wished for pediatric expertise, honesty, psychosocial support, and an individualized approach, while at the same time experiencing self-efficacy and being recognized as experts in the care of their children. 14 The observed familiarity demonstrated the individualized approach the teams took to each case. By empowering parents, the palliative care teams addressed the parental need for self-efficacy, while shared decision-making showed the extent to which they respected parents as experts in the care of their children. At the same time, they supported and advised them as pediatric experts. By considering parents’ concerns, acting in an appreciative manner and offering support options, the specialized outpatient pediatric palliative care teams provided psychosocial support and built up trusting relationships. Even the physical examination of the child took place in constant exchange and communication with the parents. Such resource-oriented attitudes clearly show how the palliative idea of non-abandonment can be implemented in daily practice. 24 Building collaborative relationships demands far-reaching communication and the time to treat each case individually. Several studies have shown that solid relationships with professionals make periods of uncertainty easier for parents to deal with, while unsatisfactory relationships complicate their struggles.15,16,25–27 Especially in hospitals, fulfilling the requirements for good collaboration in pediatric palliative care might be challenging. This may be due to constant change in care providers and limited time per patient. In Germany, only two pediatric palliative care units exist, which means that a large proportion of children and adolescents with life-limiting illnesses must be cared for in curative wards.8,25 Every year more than four million people die with serious health related suffering in Europe, with estimated 138,913 of them being children. 28 To provide care for these children, three main types of service exist: inpatient hospices, hospital programs and home care programs. While most European countries offer at least one type of pediatric palliative care, only 12 countries provide all three. 28
Our results underpin the need to expand palliative care structures for children and their families to meet the requirements of good palliative care such as parent-provider collaboration. Home care provided by specialized teams offers children the opportunity of a self-determined best possible death while spending the final weeks, months, or years of their lives with their families. This form of palliative care permits the provision of high-quality family-centered care, with the family home remaining at the center of care. 29 Our results underline how important it is that every family should have access to a multidisciplinary, holistic pediatric palliative care team at home.29,30 As the EAPC Atlas of Palliative Care in Europe reports, 29 European countries have home care programs specifically dedicated to palliative care for children, while 19 out of 34 countries also reported the existence of specific standards or norms guiding the provision of pediatric palliative care. 28
Strengths and limitations
Specialized outpatient pediatric palliative care teams supported the recruitment of parents. Therefore, those with a good relationship to their palliative care team may be overrepresented. However, as the team members were able to assess the condition of the families, this recruitment method allowed us to ensure that ethical considerations regarding the suitability of families for study participation could be taken into account. We took care to intervene in the situations as little as possible. It can never be ruled out that the presence of the researchers could have led to participants not addressing certain topics, or changing their behavior in some way. However, a strong change in behavior would probably have led to irritation on the part of other interaction partners. It can be assumed that established strategies and behaviors will prevail even when researchers are present.
Our sample included parents of children of differing age and health status. As very young children were involved, as well as children that were not able to communicate their expectations and preferences on their own, their parents had to speak for them. Cases involving, for example, oncologic diseases in older children, may involve other aspects of complexity because the children can then fully interact with the teams. Our article focuses on direct interaction between parents and the specialized outpatient pediatric palliative care teams. Communication of palliative care teams with children is a further important aspect in the provision of specialized outpatient pediatric palliative care, but one that could not be explored in this article due to its complexity.
It should be noted that our observations cover a limited period of time (one visit per family, two/four visits per team). With only one visit, it is more difficult to assess routines in the interaction and the impact of the researchers on the participants. Nevertheless, themes and professional strategies could be clearly identified across the visits of each team and across the teams. The use of participatory observations gave us a direct view of the interaction of specialized outpatient pediatric palliative care teams with parents. It generated results that go beyond the narration of experiences and showed the practice of care in a real world setting and in real time.
Conclusion and implications
The daily care practice of specialized outpatient pediatric palliative care teams is highly complex and requires specialized training as children are “not just little adults.” 31 Pediatric palliative care encompasses not only medical treatment, but also collaboration with and care for parents. Building a trusting relationship with parents demands time, communication skills and psychosocial competence. These special requirements of palliative care for children and their families and the high communication share should be taken into account when establishing inpatient and outpatient palliative care structures, preparing guidelines, training staff and deciding upon appropriate remuneration. It is to be hoped that home-based palliative care continues to expand in Europe and throughout the world, so that more families have the opportunity to receive good, comprehensive palliative care in their own home environment.
Footnotes
Acknowledgements
We would like to thank all families and specialized outpatient pediatric palliative care team members that participated in our study. We also thank Meike Gerber, who supported recruitment and data collection and Phillip Elliott, who edited the manuscript.
Author contributions
DS, JE, CP collected, analyzed, and interpreted the data. DS and JE were the principal authors and responsible for drafting the manuscript, which was critically revised by all authors. MH, SB, FMG, and AE contributed toward designing the overall ELSAH study and applied for funding. DS, MA, HS, KK, and JE made substantial contributions to the conception of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is being funded by the innovation fund (“Innovationsfonds”) of the Federal Joint Committee in Germany (grant number: 01VSF16006). The funder has had and will have no role in study design, data collection, analysis, decision to publish, and the preparation of the manuscript.
Study registration
Data management and sharing
Our data protection protocol guarantees patients and providers that data will be analyzed and used only within the ELSAH project and by researchers of the study team. Therefore, we cannot provide any data.