
Abstract
Background:
Older people living with multimorbidity are projected to become the main recipients of palliative care in the coming decades, yet there is limited evidence regarding their expressed palliative care needs to inform person-centred care.
Aim:
To understand the palliative care needs of community-dwelling people aged ⩾60 living with multimorbidity in the last 2 years of life.
Design:
A scoping review following Arksey and O’Malley.
Data sources:
Three international electronic databases (CINAHL, Ovid Medline, PsycINFO) were searched from March 2018 to December 2021. Reference lists were hand searched. Eligible papers were those reporting empirical data on older people’s needs.
Results:
From 985 potential papers, 28 studies were included, published between 2002 and 2020; sixteen quantitative, nine qualitative and three mixed methods. Data were extracted and presented under the holistic palliative care domains of need: physical, psychological, social, spiritual, and additionally practical needs. Different measurement tools (n = 29) were used, of which 20 were multidimensional. Primacy in reporting was given to physical needs, most commonly pain and function. Social and practical needs were often prioritised by older people themselves, including maintaining social connections and accessing and receiving individualised care.
Conclusion:
Identifying the palliative care needs that matter most to older people with multimorbidity requires the recognition of their concerns, as well as their symptoms, across a continuum of living and dying. Available evidence is superficial. Supporting end of life provision for this growing and underserved population necessitates a shift to tailored multidimensional tools and community focussed integrated care services.
What is already known about this topic?
Multimorbidity is increasing substantially worldwide, is associated with greater use of healthcare services, lower quality and quantity of life, and rises with age.
Older people with multimorbidity are expected to become the main recipients of palliative care in the coming decades; however, there is limited evidence of their specific needs.
Older people’s voices are vital to understanding their own palliative care needs and priorities, but these voices are hampered by structural inequities in service provision.
What this paper adds?
This is the first paper reporting on the expressed palliative care needs of community-dwelling older people with multimorbidity.
The most common palliative care needs identified across need domains were pain, function, unhappiness, staying socially connected, future planning, person-centred care and having meaning and purpose in life.
This paper highlights different priorities between the reported items in tools used to collect palliative care need and needs expressed by older people with multimorbidity.
Implications for practice, theory or policy?
Further evidence is required to understand need to support service changes required to provide accessible, person-centred care to this underserved population.
Multidimensional palliative care tools require refining to encompass complexity beyond the standard domains of palliative care.
Community palliative care provision should involve the integration of care across sectors and recognise the diversity of needs across the continuum of living and dying well for older people with multimorbidity.
Introduction
Multimorbidity is defined as the co-occurrence of at least two long-term conditions in the same individual. 1 Multimorbidity is associated with increased mortality, lower quality of life, and greater use of healthcare services, including unplanned hospital admissions. Globally multimorbidity is increasing, driven in part by worldwide ageing. 2 Predisposing factors include socio-economic status, certain ethnic backgrounds, being female, and the co-existence of physical and mental health needs. 3 Prevalence estimates vary, ranging from 13% to 72% of the population. 2 Recent estimates in England suggest more than half of people aged 65 and above 4 are living with multimorbidity. Older people living with multimorbidity are projected to become the main recipients of palliative care in the coming decades. 5 However, little is known about their palliative care needs and they are currently underserved by palliative care services for diverse reasons (1) frailty and non-malignant conditions contribute to an unpredictable dying trajectory that makes identifying palliative care needs and the start of the end-of-life phase challenging, (2) services have historically been single disease focussed,6,7 (3) age related structural inequalities impede access to care. 8
This paper focusses on the perceived palliative care needs of community-dwelling older people living with multimorbidity, and their proxies. Most people will live out their last years of life in the community, requiring integrated care addressing social as well as health needs. This paper also includes studies of those who transition between acute and community settings, a common experience for community-dwelling older people as they near the end of life. Within this review Bradshaw’s taxonomy of need, either an ‘expressed’ or ‘normative’ need, is utilised.9,10 An expressed need is ‘what an individual demands’, defined in this paper as what an older person themselves articulates as a need, while a normative need is ‘what a professional or family members think an individual wants’. 10 Palliative care need is often conceptualised through four domains: physical, psychological, social and spiritual. 11 We also included a fifth domain, practical need, reported by Larkin and Hegarty as important for capturing essential aspects of managing daily living (e.g. finances). 12 Definitions for these five domains (Table 1) were agreed by the authors and a clinical reference group of palliative and geriatric clinicians.
Methods
Research question
This review asks: what are the perspectives of community-dwelling older people living with multimorbidity, and their proxies, on their palliative care needs?
Design
Arksey and O’Malley’s 13 scoping review method was selected. A scoping review is a form of research synthesis that allows literature in a particular area to be mapped, to identify the types of evidence available, gaps in the literature, and key concepts. A scoping review also permits collation and analysis of data from heterogeneous literature and post hoc development of inclusion/exclusion criteria, 14 to get an initial understanding of the breadth of the topic before restricting focus. This was important for a topic that has historically received limited research attention, where the evidence base has a dearth of literature indexed to multimorbidity, and where key search terms can be used differently across literature, making the identification of relevant evidence difficult (e.g. the conflation of multimorbidity and comorbidity, or synonymous terms, contributing to identifying papers focussing on single conditions).
Inclusion and exclusion criteria
Due to the lack of papers indexed as multimorbidity studies, we needed to keep our inclusion criteria broad (Table 2; see Supplemental Appendix 1 for more detailed information). Papers were included where a distinct, disaggregated sub-sample of older people living with multiple conditions were included within a larger total sample for a study among other populations for comparison. Papers that solely referred to a single disease, e.g. older people living with chronic obstructive pulmonary disease, were excluded. Papers were included where participants were living with two or more conditions, as per NICE guidance. 15
Inclusion criteria.
In seeking to examine evidence on end of life needs, palliative and end of life care items were included in the inclusion/exclusion criteria. Palliative care may be required long before the final weeks of life, while NICE include within their end of life definition those living with advanced, progressive, incurable conditions. 16 Those living with frailty were included as per Smith et al.’s strategy and clinical guidelines for using frailty as a proxy indicator for multimorbidity.1,15 However, papers were not excluded if no palliative or end of life information was provided, recognising that end of life can be hard to predict and may not be the primary focus of papers. Few studies were included on this basis, where for most studies limited or no information was available.
Proxies for older people were included with the understanding that older people will sometimes need support to express their needs and to better understand the state of current evidence as to how the needs of older people are currently being collected. However, the focus of the papers must be on older people’s needs, and consequently, papers focussing on professionals’ needs, service organisation, and delivery were excluded.
Search strategy
The search strategy (Supplemental Appendix 2) was informed by a previous review on the rise of multimorbidity in old age. 1 The strategy combines both generic terms for multiple, chronic conditions, such as ‘multimorbidity’ or ‘co-morbidity’ (group 1) AND terms for specific diagnoses, such as ‘COPD’, ‘diabetes’ or ‘dementia’ (group 2). This enables retrieval of papers that either use the term multimorbidity or include two or more terms for specific conditions. The list of conditions from Smith et al.’s strategy was adapted as appropriate for this review. Terms were excluded for chronic diseases with early on-set, which are less likely to be found in older populations, as well as terms such as alcohol or substance misuse, which identify specific sub-groups of people whose end of life care needs cannot be assumed to be representative of the broader population. MeSH terms for other concepts included ‘Aged’ (group 3) AND ‘End of Life Care’ or ‘Palliative Care’ (group 4) AND ‘Home-based’ OR ‘Community Health Care Services’ OR ‘Nursing Homes’ OR ‘Social Work’ (group 5). MeSH terms were identified on MEDLINE and adapted for searches on the other databases.
Inclusion and exclusion criteria were calibrated by two team members (CN and SC) independently screening a sample of references (30–100) from each database. Titles and abstracts were screened for each paper by two team members (SC and CN) using inclusion/exclusion criteria (Supplemental Appendix 1) to assess eligibility. Papers that passed screening were reviewed in full and key information from the paper was extracted by the authors. Quality assessment is not required for a scoping review 17 but the Mixed Methods Appraisal Tool 18 was used to understand the state of the evidence for included studies (Supplemental Appendix 3). Papers were included on the basis that they addressed the aim of the review rather than based on a quality score. Figure 1 below shows the overall paper selection process. 19
PRISMA flow diagram. 19
Data extraction
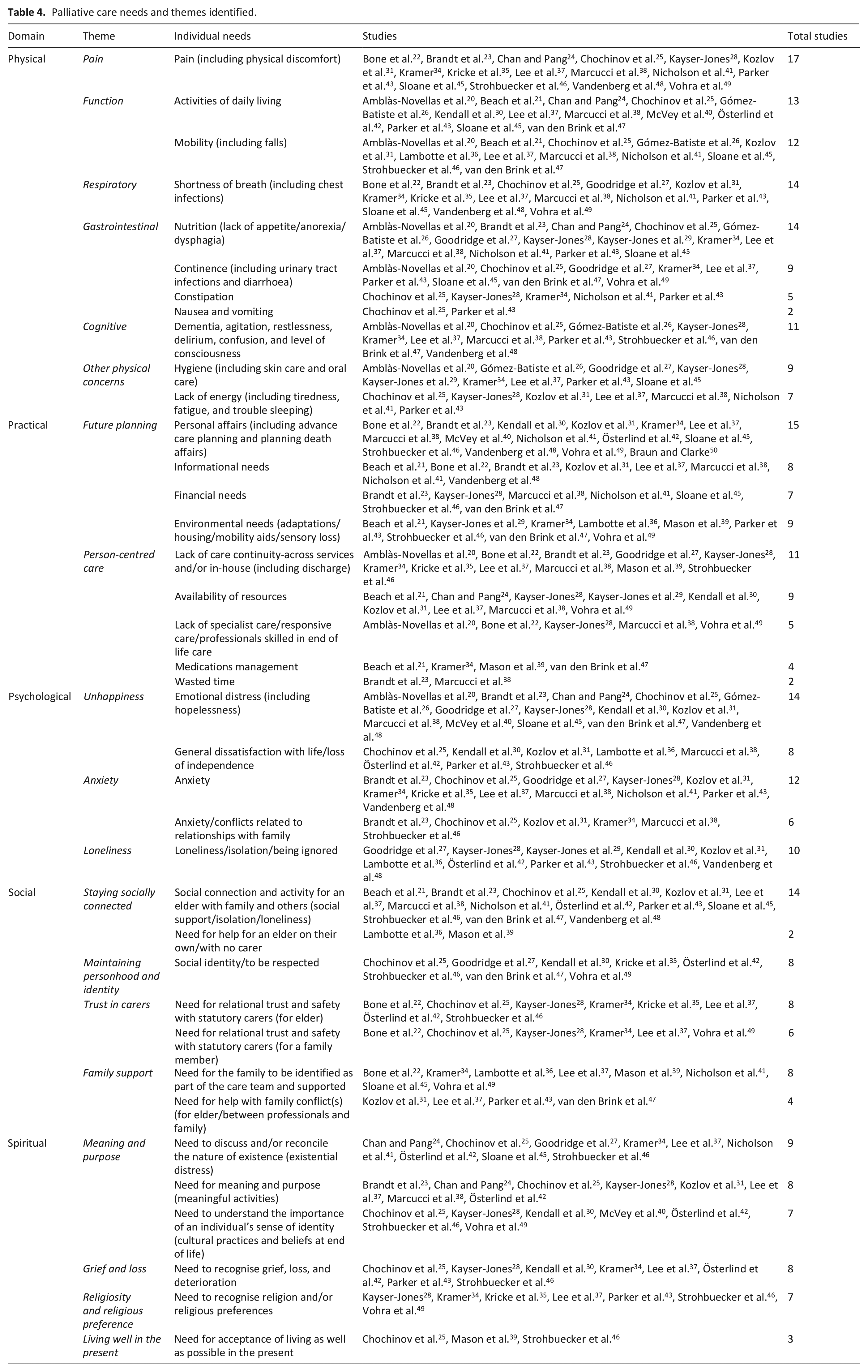
Following Arksey and O’Malley, 13 data were sorted by key themes using the palliative care need domains (Table 1) as a broad analytical framework. Relevant data were recorded in Excel spreadsheets and included author(s), title, year, country, study setting, aim, design, sample, intervention, result(s), measures used, need(s), how the need was reported (self-expressed or by proxy), practice/policy/research implications, and study limitations (Table 3). Within domains, themes and sub-themes were independently identified, then discussed and agreed by two people. Themes are grouped areas of high-level need (e.g. function) and sub-themes are more granular (e.g. ‘activities of daily living’ and ‘mobility’). In the physical domain, a sub-theme of ‘other physical concerns’ collated needs receiving scant attention attributed to hygiene and fatigue (Table 4). Where needs were identified as overlapping palliative domains these were discussed and agreed upon by the authors and clinical reference group covering palliative and geriatric medicine. Greater attention has been given to themes where more evidence has been available across studies. Collated results of the review are shown in the summary of findings related to need (Table 3) and thematic presentation of palliative care needs in the results below (each theme is highlighted in bold).
Included studies.
Palliative care needs and themes identified.
Findings
Figure 1 shows the PRISMA flow diagram for the scoping review that was conducted.
Study characteristics
Twenty-eight studies were included. Sample size ranged from 6 to 12,481 and presented evidence from 12 countries (Table 3). Study designs included cross-sectional (N = 12), qualitative interviews (N = 6), mixed or multiple qualitative methods (N = 3), mixed (convergent design, qualitative and quantitative) methods (N = 3), surveys (N = 3) and case control (N = 1). Study care settings were described as nursing care homes (N = 10), residential care homes (N = 5), domiciliary care (N = 5), mixed community settings (N = 4), and mixed community and acute settings (N = 4). Needs were reported by individuals and proxy respondents as follows: older people with multimorbidity (N = 7), care professionals (N = 6), family members (N = 3), older people and family members (N = 1), older people and care professionals (N = 3), family members and care professionals (N = 4), and all groups (N = 4).
Data synthesis
Physical needs
Physical needs were reported in all studies. Pain and mobility difficulties were reported most often. Themes for physical needs were ‘pain’, ‘function’, ‘shortness of breath’, ‘gastrointestinal’, and ‘other physical concerns’.
“I have a lot of pain [. . .] I just have to get along with it and make the best of it.”
46
In one study, pain was found not to be assessed, monitored, and managed adequately for observed care home residents, with 40% experiencing severe pain most of the time. 28
“Every day the pain just keeps getting worse. They don’t want to give me anything for pain here. I don’t understand. I’m going to die anyway.”
28
No significant differences in pain reporting between those living with multimorbidity and other groups with life-limiting conditions were found in one study, 25 while another reported that older people living with multimorbidity receiving palliative care reported pain less frequently compared with standard palliative care patients, although pain was evident in both cohorts. 41 Pain was frequently cited as the most distressing problem in the final days of life for nursing home residents by family members and nursing home staff. 27 Another study found uncontrolled pain to contribute to emergency department attendance at the end of life. 22
Practical needs
Practical needs were identified in 25 papers and themes were ‘future planning’ and ‘person-centred care’.
“I was given very little notice about his discharge. A doctor told him he could be discharged when he was clearly not well enough to go home.”
22
Disconnected services can lead to perceptions of inconsistent and impersonal care. 39 Access to specialist services for long-term care residents was challenging in one study, as services would not provide home visits, and older people living with multimorbidity were unable to travel to access these services. 46
Inadequate resource and staffing posed challenges to the quality of care received, with adverse outcomes for long-term care residents’ experiences of death,28,29 as the following account illustrates:
“During the last week of life, Mrs. Lee’s left arm and hand became edematous; the hospice nurse asked the nursing staff to assist Mrs. Lee with meals, but no one helped her.”
28
In addition to the above example, care home staff and residents spoke different languages and staff could not respond to residents’ articulated needs. Furthermore, food provision was not culturally appropriate and had an impact on residents’ weight.28,29
Psychological needs
Psychological needs were identified in 24 papers. Themes were ‘unhappiness’, ‘loneliness’, ‘anxiety’, and ‘depression’.
Having choices and independence was identified as important by older people living with multimorbidity.
43
Progressive loss of independence caused frustration
30
and fear,
46
but dissatisfaction could be tempered by acceptance:
“I’m not really happy here. You just have to accept the situation, after all I get help here . . .”
42
Social needs
Social needs were identified in 22 papers. Themes were ‘staying socially connected’, ‘maintaining personhood and identity’, ‘trust in carers’, and ‘family support’.
“The [LTC facility] nurtured not only [the resident] but us as a family. They facilitated all sorts of special arrangements for us so that we could do what [the resident) loved.”
49
“There’s very little personal rapport here. There’s nothing personal about the way they talk to you.”
46
“. . .Most of the dying patients come to the point where they don’t trust people; they don’t trust the nurses. And the nurses don’t have much time; there are just an awful lot of patients for the nurses.”
28
Spiritual needs
Spiritual needs were identified in 19 papers and themes were ‘meaning and purpose (meaningful activities)’, ‘grief and loss’, ‘religiosity and religious preference’, and ‘living well in the present’.
“I’m going to die. Nobody cares for me anymore.”
28
In contrast, value of life was defined, in one study, as the least desirable quality of life concern for older people living with multimorbidity at end-of-life.
24
Meaning and purpose were also linked to meaningful activities in life, such as older people being provided with activities they might enjoy,
42
as the following quote illustrates:
“She wanted to fill her life with more activities and meaning.”
42
Meaningful activities could also refer to activities that maintain a sense of dignity, such as enabling older people to walk to the toilet rather than insisting on pads 28 for as long as possible. 39
Discussion
Main findings
This paper aims to establish the perspectives of community-dwelling older people living with multimorbidity regarding their palliative care needs. The most identified palliative care needs across domains were pain, function, unhappiness, staying socially connected, future planning, having accessible and tailored care, and having meaning and purpose in life. While palliative care needs were identified across all domains, only 25% of papers drew from research where older people living with multimorbidity themselves solely reported their needs. The remaining 75% of papers reported needs through a proxy (care professionals and/or family), sometimes jointly with older people living with multimorbidity, but most frequently without. Physical needs received the most attention in the reporting of findings; one-third of the tools identified in this review primarily or exclusively reported needs related to physical function. Conversely, expressed physical needs received comparatively less attention in the qualitative accounts of need elicited from older people living with multimorbidity. Explanations for this variance may be (1) physical needs are being met and are therefore no longer of concern, (2) a consequence of non-physical needs being outside the sphere of care professionals’ control, (3) implementation of tools may be driven by the preoccupations of the specific service. Needs reported by older people themselves focussed on psychological symptoms, existential questions, maintaining social connections, being informed about care, and practical issues regarding accessing and receiving timely and trustworthy care tailored to their individual needs and circumstances.
What this study adds
This is the first paper of which we are aware reporting on the expressed palliative care needs of community-dwelling older people with multimorbidity. The findings highlight the different priorities between the reported items in multidimensional tools used to capture palliative care needs and the needs expressed by older people themselves. Older people living with multimorbidity evidently reported needs that go across domains of need, for example depression, which has a strong correlation with physical function. 51 Kendall et al. 30 note the progressive loss of function of people with advanced frailty compared to other advanced disease (cancer and organ failure) and that gradual loss of function, cognitive decline and fear of institutionalisation are more salient needs than needs related to dying. The link between mental and physical health is well established in multimorbidity, 52 however in this review, cognition is primarily considered as a component of multidimensional tools. There is minimal discussion of the interplay between needs, which illustrates the challenge of whether or not needs are viewed as interconnected.
Limitations
This scoping review focused only on articles that were published in English. Also, 25 of the studies came from high-income countries; the remaining three were from middle-income countries. A key challenge for this review was to identify relevant papers that focused on the concept of multimorbidity. Historically, multimorbidity has received limited attention in academic literature and has synonymous terms (e.g. co-morbidity) that vary in meaning across different clinical and geographical spaces. Using a published multimorbidity search strategy alongside the scoping review method allowed for development of inclusion/exclusion criteria better to identify the limited evidence available.
Alongside conceptualising multimorbidity, challenges in analysis arose when evidence spanned domains of need, for example the concept of dignity. The flexibility of a scoping review design has enabled development of an analytical framework to encompass diverse data. Further, and crucially for a review focussing on the needs of older people living with multimorbidity from their own perspectives, many of the included papers relied on the ‘normative’ needs, 10 as reported by proxy respondents.
The review also highlights the limits of the available evidence to understand need and thus develop appropriate end of life provision for older people with multimorbidity. Most papers reported using a tool that counted the prevalence of need but gave little detail on the extent or consequences of the need for daily living. Few papers reported directly from older people and more work is required to understand the differences and similarities of needs reported by older people living with multimorbidity themselves and their proxy respondents. Most included papers focus on participants who were living in long-term care settings, with seven of the nine qualitative papers drawing exclusively from long-term care settings. Additional work is also required to understand the differing needs of older people living with multimorbidity in long-term care settings compared to living in other community domiciliary settings.
Implications for practice
Currently, older people living with multimorbidity are less likely to receive palliative care, and more likely to experience inappropriate, invasive, futile, and costly interventions in their last year of life. 41 Addressing this inequity includes: (1) new and refined multidimensional tools that reflect and enable identification of what matters most and (2) access to integrated care that spans health and social care provision, which crucially is wrapped around the person in their community to enable them to be an active participant, connected to people and places that are important to them. 53
Multidimensional patient-reported outcome measures are important in measuring change in health status, quality of life, 54 and the impact of care. A systematic mixed-methods review of studies evaluating person-centred tools around clinical uncertainty for a similar population highlights the benefits of tools measuring across need domains. 55 Tools targeting ‘comprehensive assessment and continuity of care’ were found to improve ‘outcomes of quality of death and dying, clinician’s global assessment, goal attainment and symptom burden’. 55 Any tools developed for older people with multimorbidity near the end of life must cover multiple, complex palliative care needs across domains of need. Further, tools must also measure what matters most to the patients with which they are being used to have validity. 56 A recent scoping review found that important outcome concepts for older palliative care patients and services were not widely represented within frequently used tools, 57 drawing attention to the task of correctly measuring the right outcomes. Co-design of tools can support this task, yet in practice this has not been widespread. 58 A trial of this process with an older population with advancing frailty found that maintaining involvement from older people was essentially dependent on having supportive relatives. 59 Despite potential barriers, any future tools developed to address the needs of older people with multimorbidity should incorporate co-design. Tools that sit within integrated models of care and incorporate both patient experience and outcomes may be more attuned to capturing and responding to this population’s needs. Older people’s medicine does not, compared with palliative care, have as well-developed tools for capturing multidimensional and patient-focussed needs and outcomes.
Access to end of life care for all people with life limiting conditions is recognised as important at the highest policy level. 60 However, this remains at odds with structural factors, including over reliance on acute services, dominance of the medical model of care, 61 ageist practices, 62 and the persistent view from some that palliative care has connotations with treatment withdrawal and imminent death. 63 The recent Lancet Commission on revaluing dying 64 argues that moving beyond the current imbalance and inequity in the experience of dying will require radical shifts including reframing dying as a relational and spiritual process, rather than simply being physiological, and the recognition of an individual’s social network, for example family, friends and communities in leading the support for the dying, rather than professionals. However, radical shifts require an acceptance of mortality, including in older age. Currently, within most discourse there is little, or no, mention of preparation for death as part of healthy ageing.
Access to tailored end of life care for older people requires an interface between geriatric and palliative care and involves core components, including comprehensive assessment, future care planning, and skilled integrated working.65,66 Possible changes to clinical practice will vary by locality but can be guided by age-attuned principles of palliative care of relationality, inclusivity, individualisation, and integration, focussed on the needs and concerns of, and delivered in partnership with, older people and their family. 67 Integrated care for older people living with multimorbidity requires a political, societal, and professional will to invest in the concurrent work of dying and living well in older age. 61 With increased illness burden, older people living with multimorbidity are disadvantaged in lobbying for equitable care and in services as they are currently configured, which will continue to compound inequity for those living with multimorbidity in older age. Holding together living and dying 68 requires a recognition of palliative care needs across a complex adaptive system69,70 that encompasses dynamic, relational, and social systems, and that integrates and transcends palliative care domains.
Conclusion
Worldwide, multimorbidity is dramatically increasing, requiring a new and different clinical and service response including at end of life. 71 The response must begin with older people living with multimorbidity themselves, their understanding of their priorities and palliative care needs. While there is currently limited evidence, this review suggests there are diverging priorities between the dominant ways of identifying and capturing need and the needs that are most important to older people. Refined multidimensional tools and integrated care models are proposed to address unequal palliative care provision for the increasing number of older people living and dying with advancing multimorbidity.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221118230 – Supplemental material for Addressing inequity in palliative care provision for older people living with multimorbidity. Perspectives of community-dwelling older people on their palliative care needs: A scoping review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221118230 for Addressing inequity in palliative care provision for older people living with multimorbidity. Perspectives of community-dwelling older people on their palliative care needs: A scoping review by Caroline Jane Nicholson, Sarah Combes, Freda Mold, Helen King and Richard Green in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163221118230 – Supplemental material for Addressing inequity in palliative care provision for older people living with multimorbidity. Perspectives of community-dwelling older people on their palliative care needs: A scoping review
Supplemental material, sj-pdf-2-pmj-10.1177_02692163221118230 for Addressing inequity in palliative care provision for older people living with multimorbidity. Perspectives of community-dwelling older people on their palliative care needs: A scoping review by Caroline Jane Nicholson, Sarah Combes, Freda Mold, Helen King and Richard Green in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163221118230 – Supplemental material for Addressing inequity in palliative care provision for older people living with multimorbidity. Perspectives of community-dwelling older people on their palliative care needs: A scoping review
Supplemental material, sj-pdf-3-pmj-10.1177_02692163221118230 for Addressing inequity in palliative care provision for older people living with multimorbidity. Perspectives of community-dwelling older people on their palliative care needs: A scoping review by Caroline Jane Nicholson, Sarah Combes, Freda Mold, Helen King and Richard Green in Palliative Medicine
Footnotes
Acknowledgements
The authors thank the clinical reference group who supported and guided this work in the design of the scoping review and the defining of palliative care needs. The authors also thank Alessia Costa who helped in the initial thinking prior to the review and Faith Howard who helped in our thinking about multidimensional patient-reported outcome measures.
Authorship
The scoping review was conducted by the authors with participation at each stage by the cited member(s) of the team as described below. The search strategy was developed by CN, SC, FM, and HK. The original and subsequent searches at later time intervals were carried out by SC. Screening was carried out by CN, SC, FM, and HK. Data extraction was carried out by CN, SC, FM, HK, and RG. Quality appraisal was carried out by FM, SC, and RG. Need identification was carried out by CN, SC, FM, and HK. Analysis was caried out by CN, SC, FM, and RG. RG and SC drafted the manuscript. All authors took part in team discussions and critically revised the manuscript, making substantial contributions and approving the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Caroline Nicholson (ICA Senior Clinical Fellowship, ICA-SCL-2018-04-ST2-001) is funded by Health Education England (HEE) / National Institute for Health Research (NIHR) for this research project. The views expressed are those of the author and not necessarily those of the NIHR, HEE, NHS or the UK Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.