
Abstract
Background:
The impact of assisted hydration on symptoms and survival at the end of life is unclear. Little is known about optimal strategies for communicating and decision-making about this ethically complex topic. Hydration near end of life is known to be an important topic for family members, but conversations about assisted hydration occur infrequently despite guidance suggesting these should occur with all dying people.
Aim:
To explore the views and experiences of doctors experienced in end-of-life care regarding communicating with patients and families and making decisions about assisted hydration at the end of life.
Design:
Qualitative study involving framework analysis of data from semi-structured interviews.
Setting/participants:
Sixteen UK-based Geriatrics and Palliative Medicine doctors were recruited from hospitals, hospices and community services from October 2019 to October 2020.
Results:
Participants reported clinical, practical and ethical challenges associated with this topic. The hospital setting provides barriers to high-quality communication with dying patients and their families about assisted hydration, which may contribute to the low incidence of documented assisted hydration-related conversations. Workplace culture in some hospices may make truly individualised decision-making about this topic more difficult. Lack of inclusion of patients in decision-making about assisted hydration appears to be common practice.
Conclusions:
Proactive, routine discussion with dying people about hydration-related issues is indicated in all cases. There is room for debate regarding the limits of shared decision-making and the benefits of routine discussion of assisted hydration with all dying people. Clinicians have to navigate multiple barriers as they strive to provide individualised care.
The impact of assisted hydration on symptoms or survival in the last days of life is unclear.
Hydration-related conversations near the end of life are important, but the frequency of such conversations appears to be low.
Some studies have explored hydration-related communication strategies but few have examined decision-making processes and influences, or cultural considerations.
Several barriers exist to the effective individualisation of hydration-related practice at the end of life, including the formation of rigid workplace cultures.
This area of practice is challenging even for senior clinicians with experience in end of life care, given clinical uncertainties, discrepancies of opinion between patients, families and medical teams, and ethical quandaries.
Current practice may not be commensurate with shared decision-making principles.
A debate is required regarding the inclusion of dying people in conversations about hydration-related aspects of their care.
Education for undergraduate and postgraduate medical professionals could usefully address individualisation of care in practice as well as in theory.
Future research needs to examine the perspectives of dying people and their family carers on assisted hydration.
Introduction
There is at present a limited evidence base regarding the impact of clinically assisted hydration on symptoms or survival of people approaching the last days of life. 1 Despite this uncertainty, healthcare professionals are regularly faced with communicating with patients and those close to them and making decisions about this important and emotive area of clinical care. 2 The prevalence of provision of assisted hydration for people near to or in the last days of life varies considerably between countries 3 and between organisations such as hospitals and hospices, 4 indicating a lack of consensus about best practice.5,6 Factors such as organisational cultures and the beliefs and values of clinicians, patients and families may play important roles in decision-making.7–9
Given the lack of available evidence, few countries have produced guidelines with specific recommendations about the use of assisted hydration towards the end of life. In Japan, a clinical guideline gives detailed recommendations for the use of assisted hydration for patients with cancer experiencing a range of symptoms in the last weeks of life. 10 In the UK, National Institute for Health and Care Excellence (NICE) 11 guidelines avoid in-depth statements about benefits and risks, instead encouraging healthcare professionals to discuss issues relating to assisted hydration with all dying people and those close to them (henceforth ‘family’). However, UK audit data suggests that conversations about assisted hydration are only documented with dying people and families in 9% and 30% of cases respectively, well below the prevalence of other important conversations often held as death approaches. 12 It is not known why assisted hydration-related conversations occur so infrequently: the discrepancy between guidelines and practice suggests either that current practice is suboptimal, 13 or that existing guidelines are unrealistic or in need of revision. In the UK, the Review of the Liverpool Care Pathway made recommendations highlighting the need for training in the appropriate use of assisted hydration, how to discuss assisted hydration, and the need for specialist services to develop assisted hydration-related education and training, 14 which have not been actioned widely to date. This review, and the fallout accompanying the withdrawal of the Liverpool Care Pathway, demonstrated that the topic of hydration near the end of life is of great importance to families, and that poor communication or decision-making about hydration can result in drastically negative consequences.
A recent literature review included studies that explored some potential hydration-related communication strategies and acknowledged the multiple meanings that hydration may hold.15,16 A small number of studies have examined healthcare professionals’ decision-making processes and influences.17–19 However, there is little understanding of the optimum timing of such discussions; the extent to which shared decision-making is practiced; and the extent to which hydration is incorporated into advance care planning discussions. This research has been designed to develop a more comprehensive understanding of assisted hydration-related communication and decision-making. This is needed to support healthcare professionals in challenging situations, 13 and to understand the antecedents of current practice, in order that future education and interventions may be effectively designed.
Aims
Regarding doctors experienced in the provision of end of life care, this study aims to gain greater understanding of their views and experiences of:
- Providing or withholding assisted hydration
- Communicating with dying patients and families about assisted hydration
- Decision-making about assisted hydration
Methods
Design
This research is situated within a constructivist paradigm, that is, the researchers take the position that reality is socially constructed and that knowledge is co-created between interviewer and participant. 20 This position led to the choice of a semi-structured interview approach for this study, which allows for a dialectic between interviewer and participant, and for the generation of rich insights into participants’ subjective experiences.
Setting
Interviewees were drawn from two tertiary hospitals, one district general hospital and six hospices/community palliative care services serving a wide geographical area and socio-economically diverse populations.
Population
Participants were doctors working as speciality trainees, staff grade doctors or consultants in the fields of Palliative Medicine and Medicine for Older People. Doctors working in these two specialties were chosen as they are frequently involved in end-of-life hydration decisions and discussions. Restrictions imposed by the COVID-19 pandemic limited our ability to include a wider range of participants including general practitioners, non-specialist providers of palliative care and nursing colleagues. We plan to undertake future research with these groups. Full eligibility criteria are outlined in Box 1.
Eligibility criteria for study recruitment.
Sampling
Interviewees were purposively selected on parameters of age, gender, ethnicity, level of seniority and site of work, to ensure a diverse sample of participants and to maximise variety and depth of insight.
Recruitment
Study information was sent to administrators at participating sites for dissemination to potentially eligible participants. Those who wished to take part contacted AK; thus, no data are available concerning numbers who did not wish to participate. If the sample had been less representative, we would have selected participants from under-represented groups; however, this was not necessary and all who showed interest were interviewed. Demographic data were collected and written consent was gained at interview onset. Participants were made aware of the availability of counselling services should the interview cause any distress. There were no inducements for participation. No participants withdrew having showed initial interest.
Data collection
AK, at the time working as an Academic Clinical Fellow and Specialty Trainee in Palliative Medicine, conducted semi-structured interviews with participants. Interviews lasted up to 1 h (range 35–59 min). From October to December 2019, interviews 1–10 were conducted in person at the participant’s place of work; interviews 11–16 were conducted via video call from July to October 2020. The hiatus, and altered approach to data collection, relate to the effects of the COVID-19 pandemic.
The interview schedule (Supplemental Appendix 1) was developed by the research team and was piloted by AK before interviews commenced (no changes made following pilot). Topics included: an invitation to recall recent or memorable cases that had involved assisted hydration; questions about participants’ experiences and usual approaches to communication and decision-making; and participants’ perceptions of current practice and how it may be improved. Interviews were audio-recorded, then transcribed verbatim by a confidential professional service. Transcripts were checked and anonymised by AK.
Data analysis
Analysis was inductive and undertaken concurrently with data collection to permit investigation of emergent issues in subsequent interviews, using a framework analysis approach as described by Gale et al. 21 After familiarisation with the transcripts, AK and BA dual-coded the first five interviews using NVivo-12 software. At this point, initial coding was discussed (no a priori codes were used) and a working analytical framework developed. AK coded the remaining interviews, iteratively updating the analytical framework as the study progressed. Following coding of all transcripts, the framework was finalised and data were analysed within and across cases, resulting in inductive development of themes and subthemes. AK kept a reflexive research diary throughout this process. COREQ criteria were utilised during manuscript preparation. 22
Data saturation was judged to have been reached after eight interviews with primarily hospice-based professionals, using Guest et al.’s 23 thematic saturation assessment method; two additional interviews were conducted in this setting, then six additional interviews were conducted with hospital-based professionals in anticipation of new information from this group. Complementing this approach, the concept of ‘information power’ was also utilised in determination of optimal sample size, taking into consideration principles suggested by Malterud et al 24 such as this work’s dense sample specificity and strong interview dialogues.
Ethics
The study protocol was approved by the University of Cambridge Psychology Research Ethics Committee (PRE.2019.063, August 2019).
Results
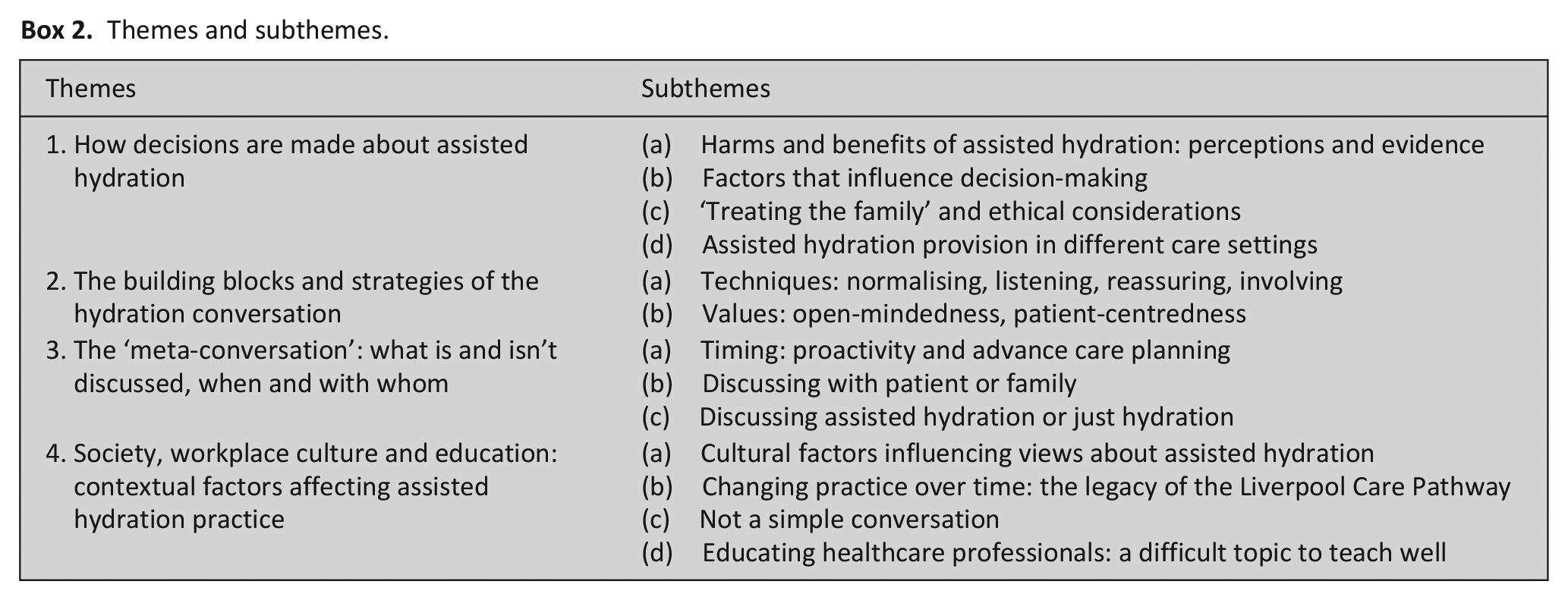
Analysis of the transcripts identified four main themes relating to doctors’ views and experiences of assisted hydration at the end of life (Box 2). Figure 1 demonstrates how themes interrelate. ‘Building blocks’ and communication strategies are influenced by contextual communication-related factors (the ‘meta-conversation’); these communication-related themes interact reciprocally with decision-making, and all these three are influenced broadly by wider contextual considerations including medical education, organisational cultures, and societal attitudes to hydration, death and dying. In the following account, ‘most participants’ refers to 50% or more; ‘many’ refers to five or more participants; ‘some’ refers to three or more participants.
Themes and subthemes.
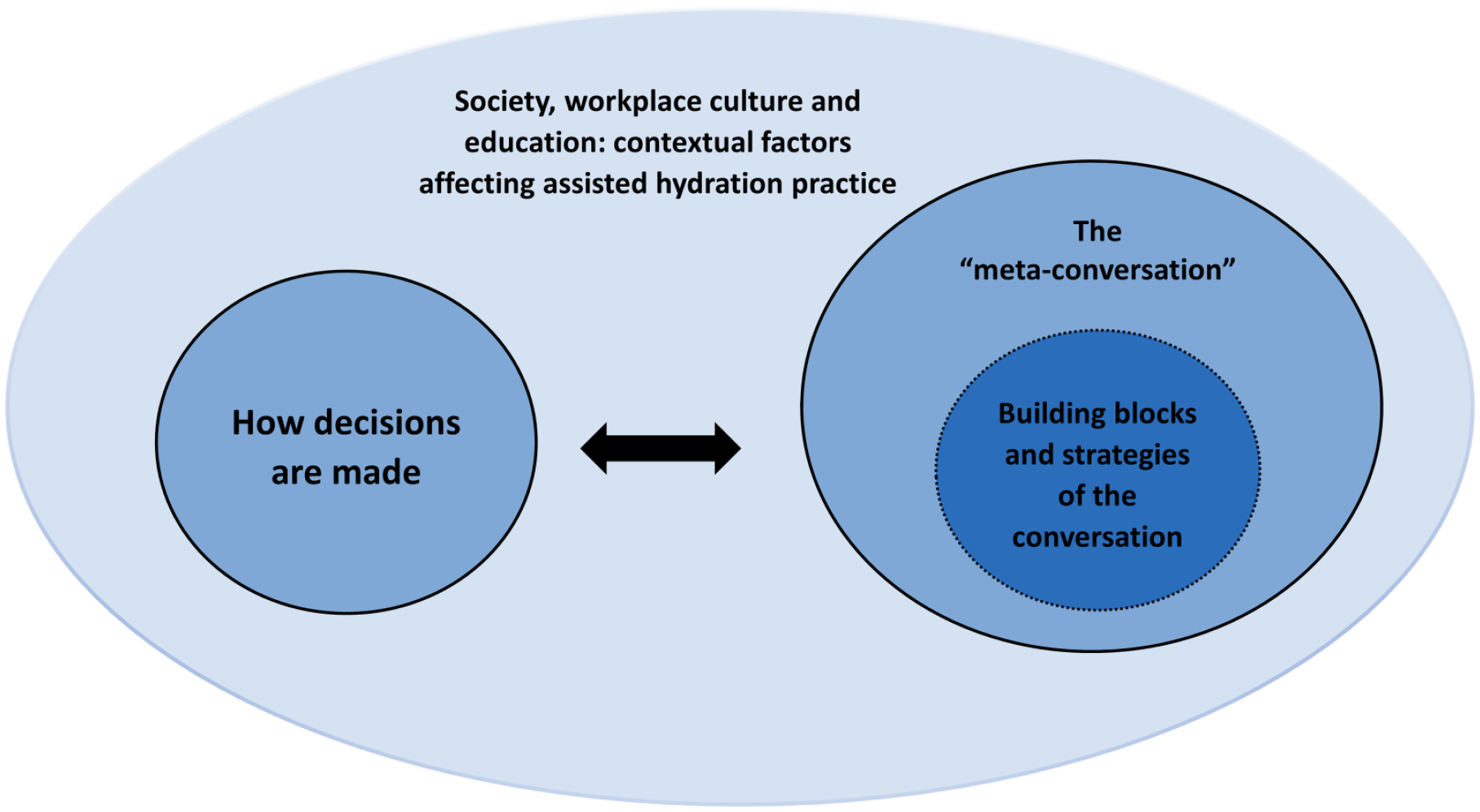
The relationships between the four themes.
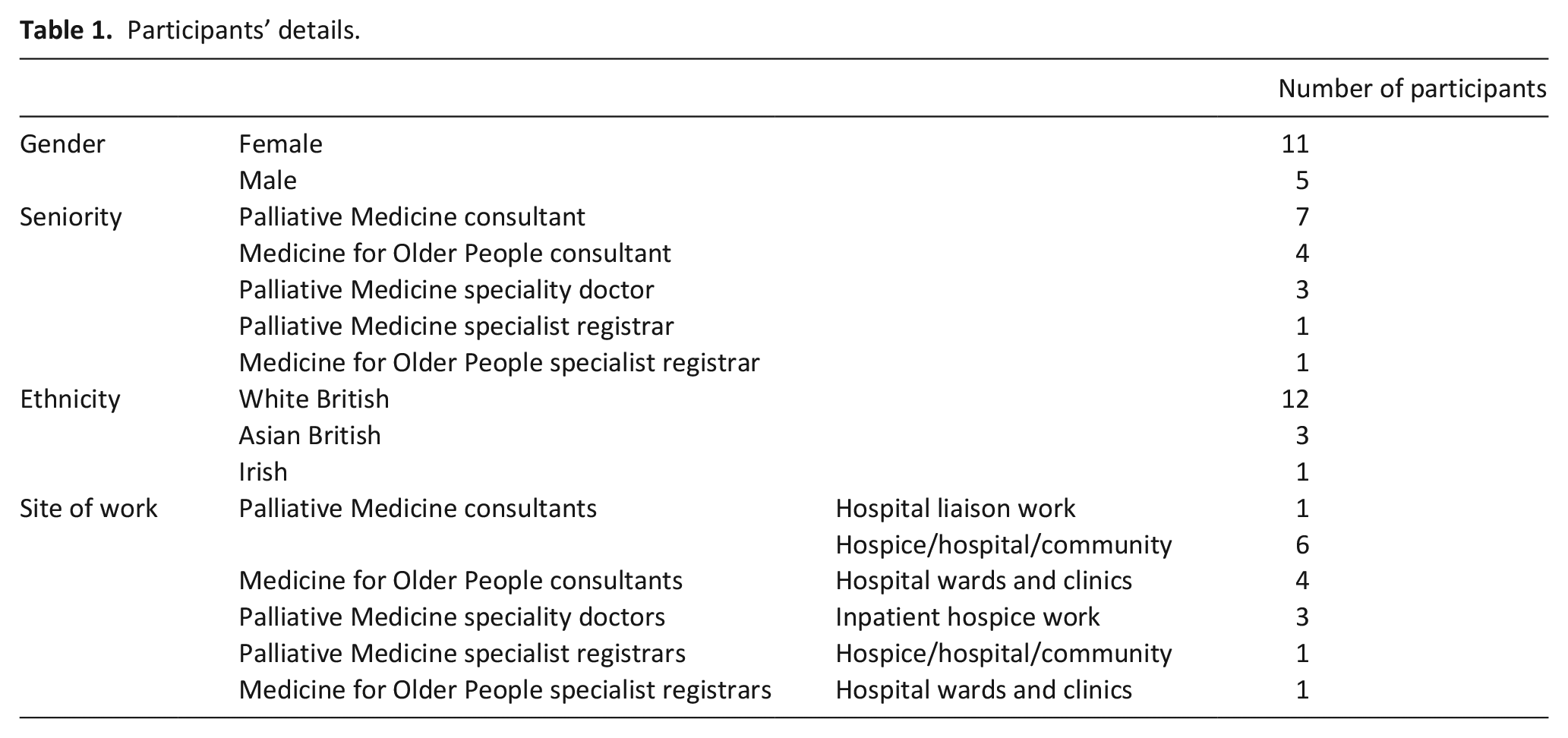
Participants were mostly consultant grade with a median of 9 years’ experience in their current speciality (range 2–16 years), principally working in an inpatient setting. Demographic details of the sixteen participants are displayed in Table 1.
Participants’ details.
Theme 1: How decisions are made about assisted hydration
Harms and benefits of assisted hydration: Perceptions and evidence
Participants perceived more potential harms of assisted hydration than benefits. Participants expressed concerns about the development of oedema, respiratory distress and secretions, prolongation of dying, and the ‘burden’ of the intervention (P8). By comparison, some thought assisted hydration might ameliorate thirst on occasion, while others felt it ‘makes them feel someone is doing something’ (P2). Some participants referenced specific recent studies that had influenced their practice; many stated that they knew of little firm evidence. There were discrepancies of opinion regarding specific side effects.
Factors that influence decision making
A large number of factors that impact on decision-making were discussed by participants, summarised in Table 2.
Factors participants discussed as influencing whether assisted hydration is used in the last days of life.
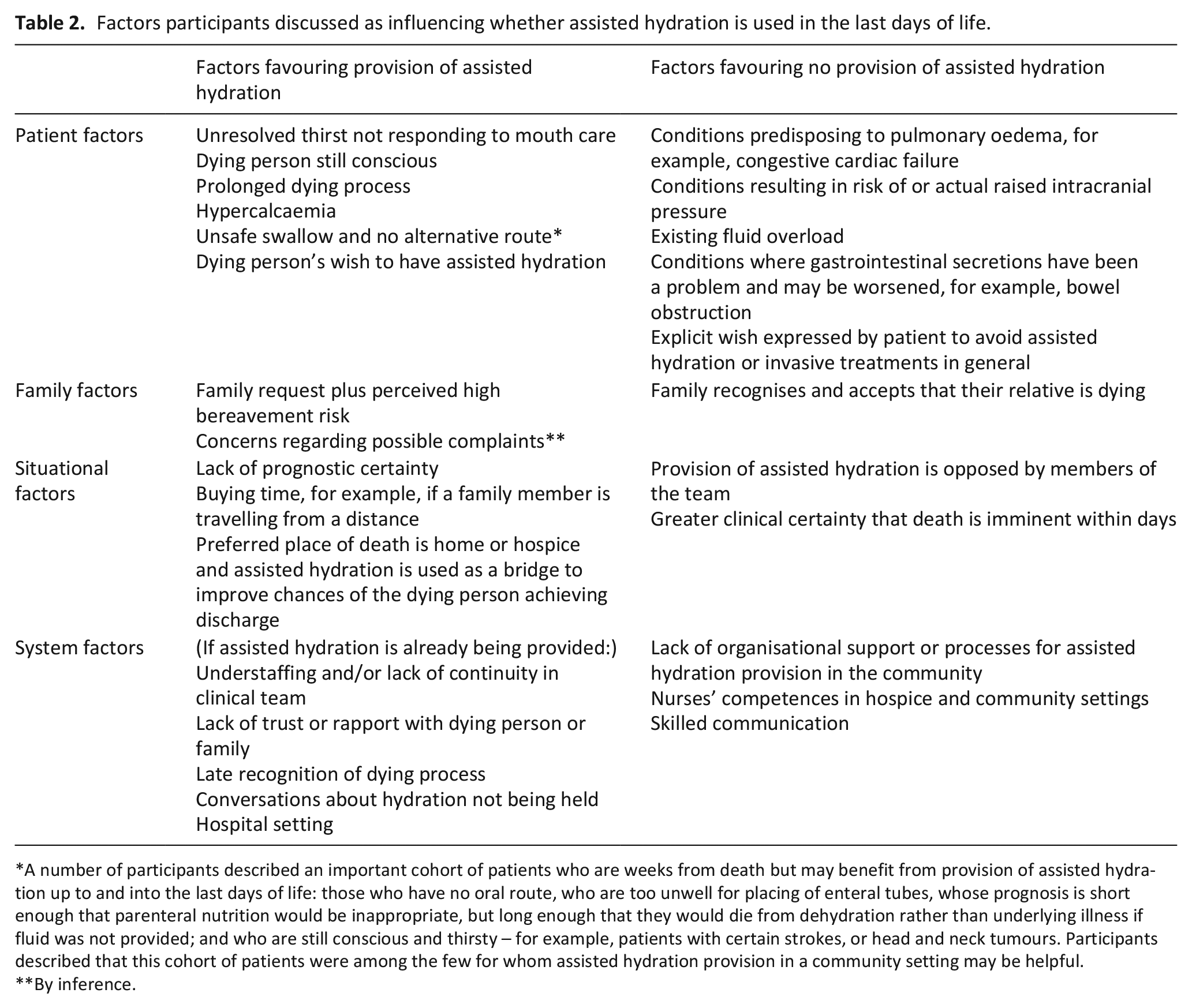
A number of participants described an important cohort of patients who are weeks from death but may benefit from provision of assisted hydration up to and into the last days of life: those who have no oral route, who are too unwell for placing of enteral tubes, whose prognosis is short enough that parenteral nutrition would be inappropriate, but long enough that they would die from dehydration rather than underlying illness if fluid was not provided; and who are still conscious and thirsty – for example, patients with certain strokes, or head and neck tumours. Participants described that this cohort of patients were among the few for whom assisted hydration provision in a community setting may be helpful.
By inference.
‘Treating the family’ and ethical considerations
All participants had encountered situations in which family requested assisted hydration provision, but where participants felt clinical benefit from assisted hydration was unlikely. All but one described that unless they had concerns regarding particular risk of specific harms, and if family were implacable, they would commence a trial of assisted hydration, with careful communication about monitoring and cessation of the trial if no improvement was seen, as expected by participants. Some expressed that this use of assisted hydration ‘buys time’ (P15) for adjustment to the dying process.
One participant described using the smallest amount of fluid possible for fear of prolonging dying, and how in this setting assisted hydration is ‘for show. . . a trick from the medical profession’ (P13). While participants omitted mentioning fear of complaints as an influence on practice, almost all remembered challenging cases in which assisted hydration-related complaints occurred or were felt to be a risk. Several identified that it can be unhelpful to treat dying person and family separately in end-of-life decision-making.
Assisted hydration provision in different care settings
Decision-making is influenced by the setting and available resources. Use of assisted hydration in the community was described as exceptional; only few participants described having organised this, in highly unusual cases. Participants described barriers including access to equipment, lack of clarity about processes and medical responsibility, and concerns over monitoring; they thus tend to avoid proactive discussion about assisted hydration in community settings. Some expressed a view that while it may be rarely used, there are circumstances where it would be ideal to have assisted hydration in the community as an option. In a hospice setting, some described that logistical concerns could affect their willingness to use assisted hydration.
Theme 2: The building blocks and strategies of the hydration conversation
Techniques: normalising, listening, reassuring, involving
Many participants emphasised ‘making sure that everyone is on the same page’ (P8) (i.e. aware of the context of the patient’s declining health and the likelihood of further decline and death) before proceeding to discuss assisted hydration with dying people and/or families. Hospice-based participants discussed communicating the normalcy of diminishing oral intake towards end of life; this narrative was not prominent in hospital-based participants’ responses. This may relate to a greater diversity of trajectories and points of recognition of dying in a hospital setting.
Many discussed using the technique of normalising as reassurance, conveying the idea that most dying people appear comfortable without assisted hydration. Most discussed encouraging family involvement in mouth care. Participants discussed explaining [their perceptions of] harms and benefits of assisted hydration, typically focussing on harms. Some felt that hydration is an emotive topic, connected with symbolism of life, hope and caregiving, and discussed acknowledging this and the impulse to help a loved one to stay hydrated.
When reflecting on ‘difficult’ cases (signified by a discrepancy in preferred outcomes between medical team and patient or family), many felt that if families are disquieted by non-provision of assisted hydration, this may herald other unaddressed concerns. Some discussed needing to ‘unpick’ these concerns (P7); others were inclined to take requests for assisted hydration at face value. Some discussed encouraging patients to articulate their feelings with family present:
Values: Open-mindedness, patient-centredness, and individualised care
Many participants discussed using what they considered to be good general communication skills, including taking time to build rapport and trust, and listening rather than launching into prepared explanations. Many felt that remaining open-minded is important; as several participants had views about assisted hydration being unhelpful, the term ‘open-mindedness’ may refer to being prepared to consider the use of assisted hydration despite doubts about efficacy. Individualisation of care was seen as overwhelmingly important; most emphasised that while they feel assisted hydration is rarely clinically beneficial for dying people, blanket decisions must be avoided. The conversation is seen as one where there is ‘real potential to upset the person you’re talking to’ (P8).
Theme 3: The ‘meta-conversation’: what is and isn’t discussed, when and with whom
Timing: Proactivity and advance care planning
Participants agreed that proactively raising the topic of hydration or assisted hydration is helpful. Some felt that if eventual impaired swallowing is foreseeable, hydration should be discussed as part of advance care planning. Hospice-based doctors spoke about normalising ideas relating to reduced intake and reduced thirst while patients are still conscious, thus involving them, and preparing families to be more accepting of non-provision of assisted hydration later on. This strategy relies on early recognition of short prognosis.
Discussing with patient and/or family
Most stated they do not routinely discuss assisted hydration with dying people ahead of them losing capacity; the topic is commonly raised with family when the patient is obtunded and recognition of last days of life has occurred. Some were concerned about patients’ non-involvement in these decisions and advocated for more routine assisted hydration discussions with patients. Others defended this approach, feeling that decisions about assisted hydration are not suited to being planned in advance.
Discussing assisted hydration or just hydration
Many participants differentiated between discussing assisted hydration and discussing hydration in general terms, without mentioning parenteral fluids. For hospice-based participants whose patients rarely receive assisted hydration, the goal was described as achieving a shared understanding of a focus on comfort. Discussing assisted hydration was felt to be potentially undesirable in cases where it is clinically inappropriate, or where the discussion could be burdensome. All felt that regardless of if assisted hydration is mentioned, it is important to discuss hydration in all cases, to avoid misunderstandings and assumptions.
Theme 4: Society, workplace culture and education: Contextual factors affecting assisted hydration practice
Cultural factors influencing views about AH
Participants discussed how societal factors impact on their practices and attitudes, as well as those of patients and families. Some participants noted that the concept of terminal dehydration may be perceived as undignified and barbaric, and how this impacts on the nature of the discussion required. Some referenced long-term societal shifts in place of death, and how these shifts have impacted on people’s experiences and expectations of dying, resulting in assisted hydration-related issues taking on greater significance. Some noted that people from certain cultural or religious backgrounds may attach (even) more importance than others to issues of nutrition and hydration, including maintenance of hydration up to the end of life. One participant reflected on their own cultural background and its influence on their practice:
Changing practice over time: the legacy of the Liverpool Care Pathway
Some hospice-based participants felt their organisations’ practices have changed in recent years, becoming more open to considering assisted hydration, although provision remains rare in this setting. Many felt that some attitudes remain overly fixed regarding assisted hydration being inappropriate for all dying people; many related episodes describing assisted hydration provision being opposed strongly by hospice staff. Some participants’ narratives equated the concept of a ‘good death’ with the non-provision of assisted hydration.
Not a simple conversation
In the hospital setting, participants noted how in some cases patients’ and families’ mistrust of the medical establishment and doctors’ motives can result in more challenging conversations. Trust was seen as harder to generate in hospitals, due to increased likelihood of previous negative experiences, less continuity of care, and more difficult prognostication. Most felt that while discussing assisted hydration became easier with experience, it remains a particularly challenging topic for junior or generalist clinicians. Many felt that junior doctors avoid starting assisted hydration-related conversations due to fears about incorrectly predicting prognosis, or about whether families are ready for cessation of assisted hydration.
Educating healthcare professionals: A difficult topic to teach
Many participants felt that communicating and decision-making about assisted hydration at end of life are difficult topics to teach. Role-modelling of individualised conversations was identified as a useful technique. Some felt junior doctors prefer protocols and can be overly rigid about assisted hydration provision for dying people being universally incorrect and felt teaching resources should address this. One recalled personal experiences of engaging with teaching material:
Discussion
Main findings
Geriatricians and palliative care doctors reflected on clinical, practical, and ethical challenges associated with making decisions and communicating about assisted hydration at end of life, and about the wider social and cultural climate that influences these decisions and conversations. A tension was apparent between participants’ aspirations to provide individualised assisted hydration-related care, and barriers that can make this aspiration difficult to achieve.
Strengths and Limitations
AK has worked clinically with some participants as a trainee, potentially affecting the dynamic and content of some interviews. AK kept a reflexive diary and took field notes to mitigate this eventuality. The sample size was small and represents a single region of the UK; while this region’s population is economically diverse, the comparative lack of population ethnic diversity may have impacted on participants’ experiences and may reduce the transferability of these findings. 25 The sample would have included other medical specialties to provide greater breadth of opinion from generalist providers of end-of-life care; recruitment proved challenging in the context of the COVID-19 pandemic. Assisted hydration practice varies across the globe 3 and findings from the UK may not translate closely to countries with different cultural and legal frameworks. Nevertheless, this research aims to highlight points of practice that are applicable to all settings.
In sampling medical experts who routinely deliver palliative care, this research provides a snapshot of their current practice, much of which may be worthy of emulation. Greater understanding of this group’s practices and opinions may result in transferable learning that is useful to other clinicians and in the development of undergraduate and postgraduate medical education materials. However, this selection omits several narratives: those of clinical nurse specialists, and of generalist physicians and junior doctors, whose experiences may help with developing understanding of the educational needs of non-specialist providers of palliative care. Most importantly, the perspectives of dying people and their relatives remain poorly understood. This research focuses on how doctors say they communicate and make decisions; further studies could usefully explore how such interactions take place in reality.
What this study adds
The lack of inclusion of patients in decision-making about assisted hydration at end of life appears to be standard practice. This is incommensurate with NICE guidance 11 and shared decision-making principles. Dying people should be involved in decisions to the extent that they choose, 26 which entails asking them their preferences, and doctors perform poorly when estimating patients’ preferred roles in decision-making. 27 However, participants indicated that when patients have limited energy and days to live, raising questions about assisted hydration may be burdensome and may relate more to the clinician’s agenda. Patients may not find assisted hydration as burdensome as clinicians seem to expect. 28 Careful, individualised reflection is required regarding whether the exclusion of patients from hydration-related decision-making is a conscious choice with the aim of reducing burden, or whether this exclusion relates to time pressure, discomfort with these conversations, or the extra conversational and associated emotional work required. For these conversations to include patients while shared decision-making is still possible, professionals and systems need to be equipped to recognise dying at an earlier stage than occurs in current hospital-based clinical practice. 12
Practitioners will draw their own conclusions regarding the extent to which ‘treating the family’ is acceptable. Classic models of shared decision-making uphold Western ideas about autonomy by focussing on doctor-patient dyads 29 ; however, some evidence suggests that patients do wish for families to be included in decision-making.30,31 Participants’ described practices suggest that as patients approach end of life, doctors are more likely to deviate from strict interpretations of best-interests decision-making, and involve family in decision-making. It may be helpful for clinicians to view interactions with dying patients and their families through the lens of relational autonomy.32,33
Many communication strategies outlined above echo those set out in existing research 34 and in the Cambridge-Calgary model of clinical communication. 35 Assumptions must be avoided regarding whether the approaches described by participants constitute best practice. Results largely confirm previous findings that demonstrated discourses of uncertainty and suggest that doctors sometimes avoid discussions for ‘protection’ of family – or themselves. 2 In carefully selected circumstances, it seems reasonable not to specifically discuss assisted hydration, as long as hydration has definitely been discussed, patient and family understand what to expect regarding fluid intake and have had opportunity to express their views. When communicating, clarity about whether assisted hydration is being discussed or offered is essential (as with discussions about cardiopulmonary resuscitation). 36
Participants described several barriers to high-quality communication in the hospital setting. Moreover, families may have more difficulty trusting what they hear, and are more often asked to reconcile themselves to assisted hydration ceasing, rather than not starting. Although some ethicists may deny a distinction between acts and omissions, 37 participants suggested that they, patients and families find cessation of assisted hydration harder to process38,39; the widely-used time-limited trial of assisted hydration is a practical solution. 40 The number and quality of hospital-based discussions about assisted hydration are unlikely to improve unless resources are less thinly stretched, and unless clinicians observe practice and receive education that engenders comfort with uncertainty and avoids dichotomous right-vs-wrong viewpoints.
Challenges are often different in a hospice environment, where non-provision of assisted hydration is highly normative. 4 ‘Hospice philosophy’ may predispose to a reified conception of good death as one which is as ‘natural’ and de-medicalised as possible. 41 Hospital-based practitioners may need reminding that active treatment until death is not always the right course of action; hospice-based professionals may need reminding that it is not always wrong. Individualisation of care is always essential – but entrenched workplace cultures can stymie attempts to individualise. Clinicians can challenge inflexible viewpoints and contribute to culture change.
Participants felt that non-specialist junior doctors on a Palliative Medicine rotation tended to be inconfident with assisted hydration-related conversations at the start of the placement, needing specific pointers in order to develop independence. It is unclear whether existing UK-based programmes of undergraduate and postgraduate education effectively address communication and decision-making about assisted hydration, although ‘understanding’ of the topic is referenced in the 2014 Association for Palliative Medicine curriculum for undergraduate medical education. 42 Approaches that explore how individualised care can be provided in practice may be helpful, alongside existing approaches explaining why this is necessary.
Conclusion
This research indicates the benefits of routine proactive discussion of hydration in all cases; clinicians face difficult decisions about timing and what exactly to include, including whether it is necessary to mention assisted hydration in every case. Although the Liverpool Care Pathway has been withdrawn, the ‘one size fits all’ mentality for which it was blamed may still linger. Clinicians must actively oppose this in education and in practice, and strive to provide individualised care, while navigating the plethora of challenges involved in conversing and making decisions about assisted hydration.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221097309 – Supplemental material for Medical communication and decision-making about assisted hydration in the last days of life: A qualitative study of doctors experienced with end of life care
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221097309 for Medical communication and decision-making about assisted hydration in the last days of life: A qualitative study of doctors experienced with end of life care by Arjun Kingdon, Anna Spathis, B�rbara Antunes and Stephen Barclay in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank Dr Richella Ryan for her help with piloting the interview schedule and Angela Harper for her administrative support.
Author contributions
AK conducted the study and wrote the manuscript. SB and AS helped to conceptualise the study and provided supervisory input. BA dual-coded the first five interviews. All authors have read and approved the manuscript.
Data sharing
Data relating to this review can be obtained by contacting the lead author at
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
The study protocol was approved by the University of Cambridge Psychology Research Ethics Committee (PRE.2019.063, August 2019).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AK is funded by a Health Education East of England Academic Clinical Fellowship. SB is part funded and BA is fully funded by the National Institute for Health Research (NIHR) Applied Research Collaboration East of England (ARC EoE) programme. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.