
Abstract
Background:
Muslims are the largest religious minority in Europe. When confronted with life-threatening illness, they turn to their local imams for religious guidance.
Aim:
To gain knowledge about how imams shape their roles in decision-making in palliative care.
Design:
Direct Content Analysis through a typology of imam roles. To explore motives, this was complemented by Narrative Analysis.
Setting/Participants:
Ten Turkish imams working in the Netherlands, with experience in guiding congregants in palliative care.
Results:
The roles of Jurist, Exegete, Missionary, Advisor and Ritual Guide were identified. Three narratives emerged: Hope can work miracles, Responsibility needs to be shared, and Mask your grief. Participants urged patients not to consent to withholding or terminating treatment but to search for a cure, since this might be rewarded with miraculous healing. When giving consent seemed unavoidable, the fear of being held responsible by God for wrongful death was often managed by requesting fatwa from committees of religious experts. Relatives were urged to hide their grief from dying patients so they would not lose hope in God.
Conclusion:
Imams urge patients’ relatives to show faith in God by seeking maximum treatment. This attitude is motivated by the fear that all Muslims involved will be held accountable by God for questioning His omnipotence to heal. Therefore, doctors may be urged to offer treatment that contradicts medical standards for good palliative care. To bridge this gap, tailor-made palliative care should be developed in collaboration with imams. Future research might include imams of other Muslim organizations.
Keywords
To Muslims it is important that medical decisions are in accordance with Islamic values.
In life-threatening illness, Muslims ask imams for religious advice on medical decision-making. So far, it is unknown how imams view and perform this task in palliative care.
Imams advise the faithful not to consent to withholding or terminating treatment based on diagnostics because they feel this does not align with belief in God’s omnipotence and will.
Imams are reluctant to advise patients to consent to termination of treatment for fear that all Muslims involved will be held accountable for someone’s death by God in the afterlife.
Fatwas by Muslim expert committees play an important role in shaping medical decision-making in palliative care.
Palliative care tailored to the cultural religious needs of Muslim minorities must be developed.
Implementing adequate palliative care for Muslim minorities requires sustainable collaboration with imams and their congregations.
Introduction
With a share of five per cent of the total population Muslims are one of the largest religious minorities in Europe. 1 Many of them have a Turkish background. 2 A characteristic of terminal illness in Muslims is an intensified focus on religion to cope with this profound event.3–6 In this context, religion not only provides beliefs concerning death but also functions as a normative framework in medical decision-making.7–11 Particularly in palliative settings, Muslims, like Christians and Jews, call on their religious leaders to learn the religious permissibility of treatment proposals.4,12–14 They contact mosque-based imams who fulfill similar roles as pastors and rabbis.7,12,15 In addition to leading the five daily prayers and preaching the Friday sermon, imams serve their congregations by conducting rites of passage (involving birth, marriage, and death), providing spiritual care, religious education and answering questions about Islamic law, including those about medical decision-making.12,16–18 As yet, no research has been done into the way imams in the West perform their task in palliative care and their role. Hence, there is a knowledge gap regarding their contribution to the dynamics of doctor-patient relationships. To better understand medical decision-making in palliative care among Muslims, it is therefore important to investigate how they are guided by their imams.
Methods
Design
We undertook an interview study and qualitatively analyzed the gathered interview data to shed light on the attitudes and motivations of imams in the performance of palliative care. We aimed to discover which roles they see for themselves and how they construct these roles in the stories they tell. The two sub-aims warranted two methodological approaches. For the first aim we used a Directed Content Analysis. This is characterized by thematic structuring of texts using a pre-existing theoretical framework. 19 The second aim concerning construction of their role in their stories was explored through Narrative Analysis. Narrative Analysis conceives personal accounts as narratives in which individuals give meaning to experienced reality to construct their identity in interaction with their audience. 20
Setting
The study took place in the Netherlands where Muslims comprise 5% of the population. 15 The majority are of Turkish and Moroccan descent; they make up 37% viz 36% of the Muslim population and have their own religious organizations.17,21,22,23
Study population
Since our research team included a native speaker of Turkish, we focused on Turkish imams.
Recruitment
Imams of Turkish mosques in the four largest Dutch cities and surrounding municipalities were purposefully selected according to the following criteria: (1) being an experienced and full-time professional imam; (2) having received formal Islamic training in their country of origin; (3) having regularly advised and spiritually guided congregants in palliative settings.24
Ethical considerations
Participants gave written consent after being informed about the purpose of the study. Due to the sensitivity of the issues, all agreed to encoded use of data. Names were therefore deleted in the transcripts. The Academic Medical Center’s Medical Research Ethics Committee ruled that the Dutch Medical Research Involving Human Subjects Act (WMO) did not apply (Ref: W21_192 # 21.209app.).
Data collection
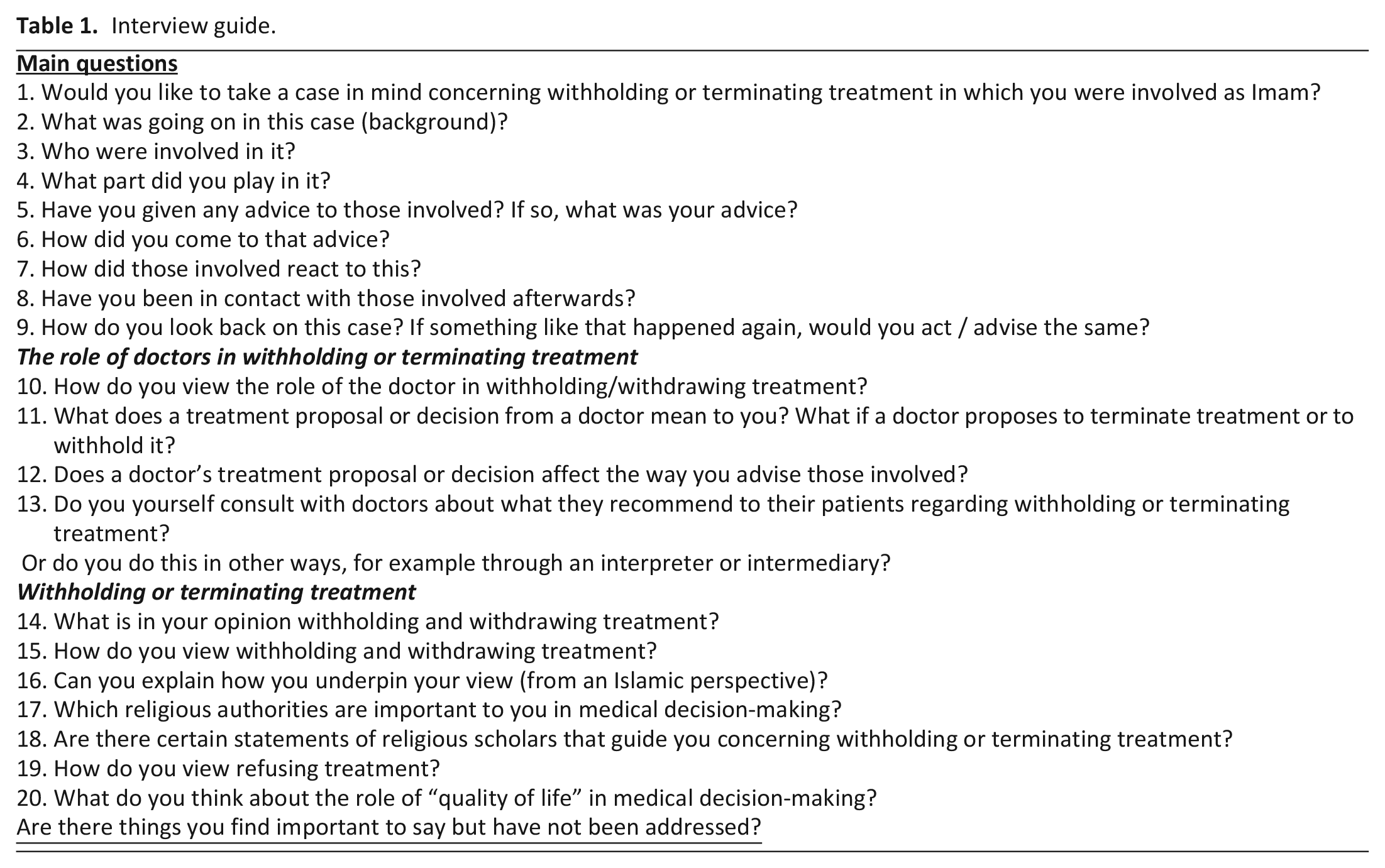
Semi-structured interviews were conducted in Turkish between February 2018 and June 2019 by NT, of which four together with GM. All interviews took place in the mosques in which the participants served as imams, in space suitable for undisturbed conduct of in-depth interviews. Participants were asked to talk about a case that involved withholding or terminating treatment they had been professionally involved in. Following an interview guide, they were encouraged to explore their thoughts and feelings (Table 1). Interviews lasted one to two hours and were recorded and transcribed verbatim. Participants were sent their transcript by email and given the opportunity to voice second thoughts. Once they agreed with the content, interviews were translated into Dutch by NT. Translations were checked for accuracy by an independent native Turkish speaker with an academic proficiency in Dutch. Based on this, final versions were determined.
Interview guide.
Data analysis
The research team provided written comment on the translated transcripts once data collection started. After six interviews no new variations were found. To generate a richer dataset, four more interviews were conducted. The results confirmed our previous findings. GM analyzed the content using Ajouaou’s typology as an analytical framework. 16 Using religious terms commonly known among Muslims, this typifies the basic functions imams perform in accordance with the expectance of congregation members who appeal to them for pastoral care. The typology distinguishes jurist (applier of Islamic law), exegete (interpreter of the Quran and the traditions of the Prophet Muhammad), missionary (preaching correct religious doctrine and the corresponding way of life), adviser (giving practical advice for dealing with difficult situations), prayer leader (leader of the five daily obligatory prayers), guide in rituals and blessings (pastor at prayers and rituals at rites of passage) and teacher (teaching religious skills such as performing obligatory prayer and reciting the Quran) (Table 2). The performance of these roles is situational and represents complementary and often overlapping modes that imams use to approach a pastoral issue. With a view to interpretative reliability, NT randomly coded five interviews through this framework, after which it was concluded that these results matched those of GM. Subsequently GM structured the stories within the interviews applying Labov’s approach, which assumes narratives have distinctive features. These are the Abstract (what the story is about), Orientation (what, when and to whom something happened), Complicating Action (what happened after this), Evaluation (the moral of the story), Resolution (the outcome) and optional Coda which takes the audience back to the present moment (and. . .here we are). The Evaluation is pivotal. It concerns language that storytellers use to make value judgments about their characters’ actions (“in doing so, she did the right thing”) or fragments in which they step out of their story to comment on it for the purpose of conveying its moral to their audience (“You should know that it is beyond my responsibility to speak out on such things.”). Carefully evaluating how stories are told provides insight into the deeper meaning, motives and values the narrator wants to convey to his audience. 25 After finalizing the results, AdlC and GM created a typology of the narratives.
Summary of the different roles of imams.
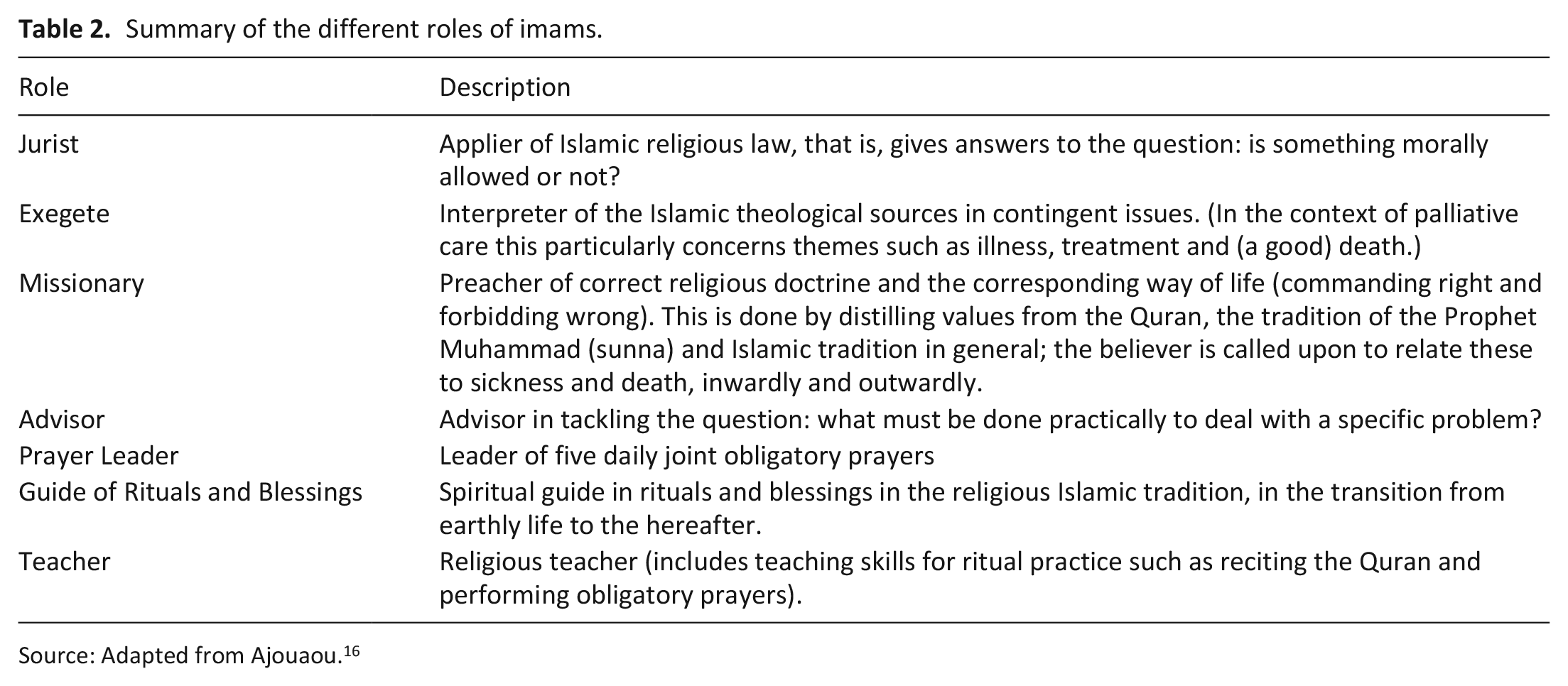
Source: Adapted from Ajouaou. 16
Results
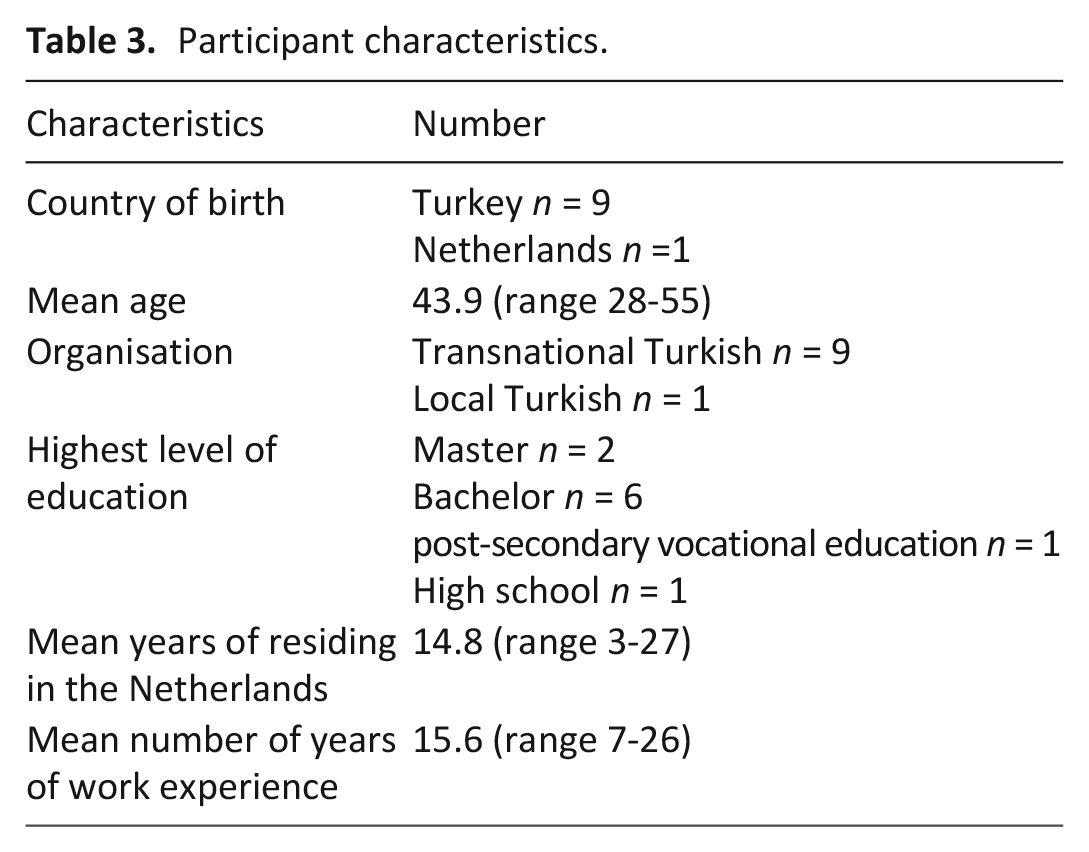
Twenty-seven candidates were approached. Twelve were not selected due to lack of experience with palliative care. Five declined to participate due to personal considerations or policies in their organization prohibiting their participation. Ultimately, 10 participated in the study (Table 3). We came across the roles of Jurist, Exegete, Missionary, Adviser and Guide in Rituals and Blessings.
Participant characteristics.
Jurist
Congregants appealed to participants with the question whether a proposal to terminate treatment was in accordance with Islamic law. In exercising this jurist role, participants urged patients to continue treatment. Muslims are not allowed to interfere in life and death because God decides on this.
“You should continue until the end. Do not discontinue based on arguments such as: it is painful and harms the patient. These are all useless things. Just keep going. . .Even though the patient screams in pain day and night. . . I cannot interfere in divine matters.” (Participant 8)
Continuing treatment meant that when a doctor declared all treatment options to have been exhausted, a second opinion had to be requested. To ensure proper understanding of afterlife religious consequences of decision-making, a Muslim doctor was strongly preferred for this task. What was striking was that withdrawing treatment was associated with killing the patient.
“Yes, well. . .. of course, you do. . . don’t misunderstand me. The judgments of both Muslim and non-Muslim doctors are valuable because they are both medical experts. A judgment or proposal from a non-Muslim doctor must of course also be respected. But when it comes to ending a human life, we must think a hundred times. This involves ethical and religious responsibility. In Islam, killing a person is like killing all people on earth. It is a terrible act with unimaginably great responsibility . . . and sin. . . I wouldn’t like to bear that as an imam. I don’t know if a non-Muslim doctor is aware of this. . . aware of Islamic ethics and values and their consequences in the afterlife. But a Muslim doctor does. That makes all the difference.” (Participant 10)
In cases where patients could not be kept alive with life support most participants transferred the role of jurist to fatwa councils within their organizations by asking these religious expert committees whether it was permissible to unplug. The imam then communicated the committee’s affirmative response to the relatives. This allowed the imam and family members involved to avoid interfering in divine matters and thereby becoming responsible for the religious consequences of decision-making.
“You should absolutely consult the Committee so that neither you nor I bear any responsibility for it. I discuss those things with you and, although I will give you a likely answer, I refer you to the Committee. It is the Committee that takes the decision.” (Participant 1)
Exegete
Four participants exercised their role of exegete by establishing causal relationships between their interpretations of the Quran, which they consider to be God’s word, and what they believed to be the divinely determined outcome of the disease process. They transferred their exegesis to the patient’s family by advising them on how to act in medical decision-making. Therefore, they interpreted a positive course of the disease as God’s reward for their endurance. This meant that a patient’s recovery after following their advice to disagree with the proposal to discontinue treatment was ascribed to their having acted according to God’s command.
“It was on a Friday . . . My wife called me. I heard in her voice that she was almost crying, as I am now (participant speaks in a trembling voice, GM). I asked what had happened. She said. . . “Ms. . . called me. Her mother has got better.” I asked her how. My wife replied: “She can’t walk but she got better . . . she can talk. . .I thought. . . I started to philosophize and said to myself: if they had unplugged her based on my advice or that of another imam or someone else. . . that would have been a great sin. I thanked God for this. When we act, with the Quran as reference . . . then we are sustained by verses like: “He leads them to a right path (Quran 5:16, GM).” I said to the patient’s daughter: “Your mother will heal even more because you have acted according to God’s command. You have sought healing and have expressed your fear of responsibility. Believe me . . . God is going to help you.” (Participant 2)
Missionary
In discussing life-threatening illness, participants positioned themselves toward the interviewers as missionaries, preaching how Muslims should deal with this in terms of correct beliefs and attitudes. Central to their view on the right Muslim attitude was never to give up hope. Unlike with unbelievers, there was no question of hopelessness among Muslims when doctors did not expect their patients to recover. Therefore, the participants saw not initiating treatment on grounds of futility as un-Islamic. Good Muslims must believe in God’s omnipotence to cure.
“The bottom line is that we shouldn’t forget that God has absolute power, that He is omnipotent. When we philosophize about why someone loses hope, we must question his faith in God. Doing nothing to initiate treatment or not starting treatment at all by saying it is useless is un-Islamic.”(Participant 6)
Adviser
Participants provided practical advice on how to cope with life-threatening illness. This advice was complementary to their religion-based advice, viz aimed at prolonging life and avoiding responsibility for the patient’s death by not agreeing to terminate treatment. Family members were advised to take heart from similar cases in which patients recovered against all odds, since doctors could be wrong.
“We know and have seen that there are those who have returned to normal life - perhaps not as comfortably as before - who had been said to never, ever show a sign of life other than a last breath. This is proof enough for us to not pull the plug. Moreover, we see that doctors are often mistaken. And we should not forget that we would eventually be killing someone without valid reason or by mistake. I said we should look at it from this perspective.” (Participant 2)
Guide in Rituals and Blessings
Participants performed rituals aimed at guiding the dying in their transition to the afterlife. Unlike the other roles that concerned religious responsibilities, this role was directed at serving the needs of the dying. Reciting a specific chapter of the Quran and gently encouraging the dying to utter the Islamic creed were ways of easing the burden on the patient. Moving the dying to utter the Muslim testimony of faith served as a reaffirmation of faith before the soul left the body.
“It concerned a patient, an old aunt, at the end of her life. We went there. As just said . . . considering the verse “You alone we worship . . .” (Quran 1:4, GM). She was at her last stage of life. You just know that. For these situations, some criteria have been set out in Islamic jurisprudence. . . Yes, what are these things? What does our Prophet advise us to do in these situations? The thing you do should is mentally ease the burden on the patient. Read chapter Yā Sīn (chapter 36 of the Quran, GM). Whether the patient hears that or not. . . only God knows. Try to remind her of the tawḥīd (God’s oneness, GM), shahāda (the Muslim testimony of faith, GM) and ṣalawāt (sending blessing upon the Prophet Muhammad, GM) without burdening her. Especially tawḥīd and shahāda, because perhaps the moment of departure of the soul from the body is the final test. I have tried to perform all these rituals to the maximum with this patient.” (Participant 1)
Narrative analysis
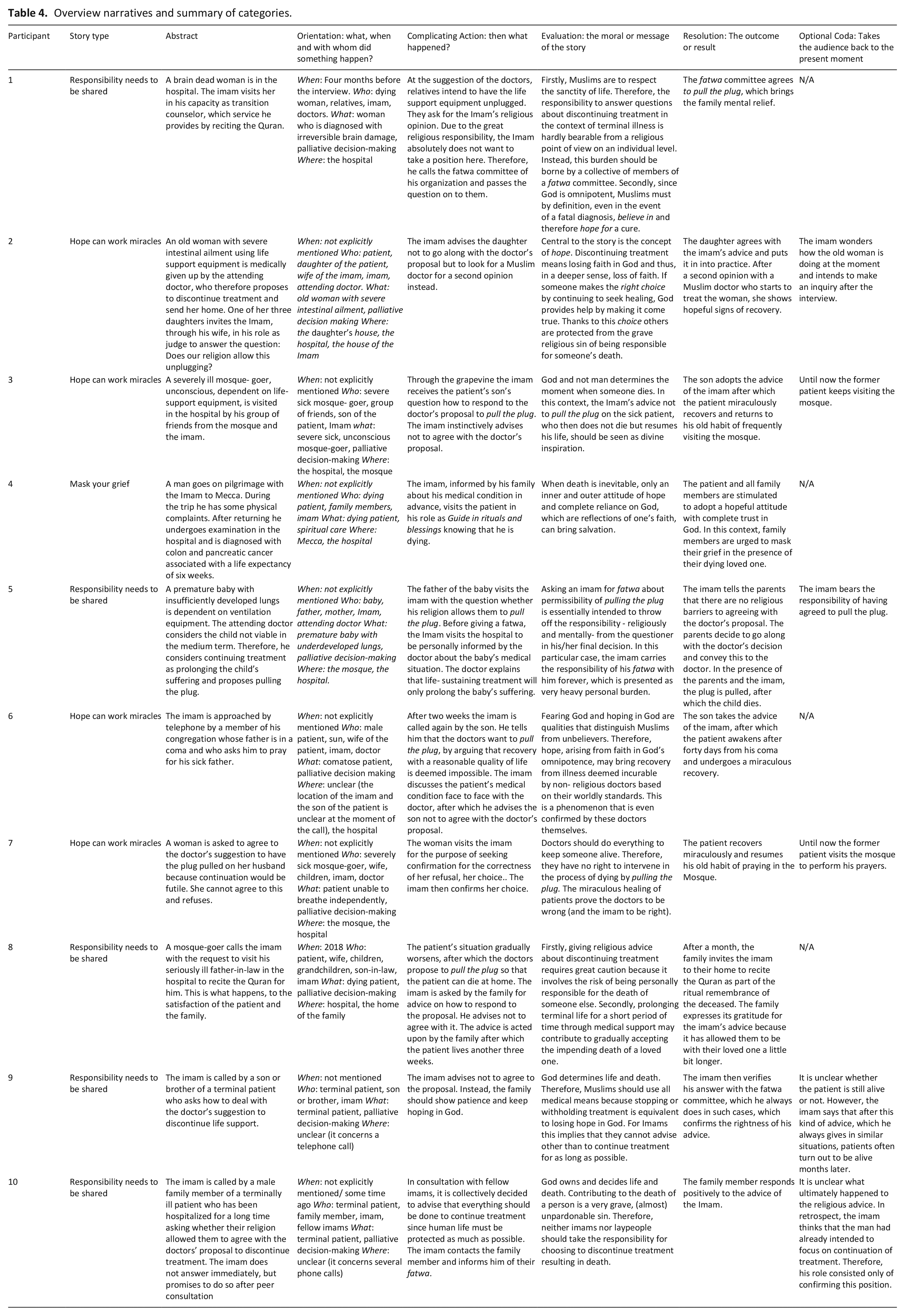
To enrich the Directed Content Analysis, we studied the stories told by the participants. The aim was to reveal the underlying meaning using Labov’s approach. Therefore, we focused on the evaluation, that is the story elements that show how the narrator wants it to be interpreted by the audience. Three narrative types were distinguished: Hope can work miracles (participant 2, 3, 6, and 7), Responsibility needs to be shared (participant 1, 5, 8, 9, and 10) and Mask your grief (participant 4) (Table 4).
Overview narratives and summary of categories.
Typology of narratives
Hope can work miracles
Doctors propose withholding or terminating treatment because they consider recovery to be impossible. After following the imam’s advice to disagree with this, the patient shows miraculous signs of recovery. The message is that God is omnipotent, so nothing is impossible. If Muslims continue to hope by searching for a cure, basing that hope in a firm belief in God, He may reward them by making it happen.
“At the initiative of a Moroccan doctor, they transferred her to another hospital. After two days they heard from the Moroccan doctor that there was hope, the hope of being able to open her bowels. To be honest, I got more curious and said to my wife: ‘Give them a call and ask them about the latest situation.’ Madam (the patient’s daughter, GM) said that her joy had made her forget to inform us. . . ‘My mother’s intestines have opened. This Moroccan doctor made an extra effort. . . a Muslim doctor has done a lot.’ My previous advice to the daughter was . . . I must mention this . . . that according to verse 53 of sūrah Al-Zumar (Quran chapter 39, GM) we must not despair of God and according to sūrah Yusuf (Quran 12: 87, GM) those who despair of God are the disbelievers. And so, we should not forget that it is God who grants healing.” (Participant 2)
Responsibility needs to be shared
Agreeing to terminate treatment is associated with religious burden. This burden stems from the relationship between terminating treatment and the subsequent death of the patient. The possibility of such an association—and thus being responsible for the chain of events—implies a potential contribution to the patient’s death. Consequently, those involved fear being held liable by God in the afterlife for the capital sin of culpable death. Therefore, advice on terminating treatment cannot be taken by imams alone but must be shared.
“Yeah. . . withholding treatment. . . terminating treatment. Right at that point, a sane imam or a believer with knowledge of Islam in his own individual capacity cannot say yes and agree with such a doctor’s decision. I’ve been through many situations like this. You have arrived at the last crucial, deciding moment. From where you should get the last word, the all-determining word. The sentence: yes. . . treatment can be terminated; the plug can be pulled. Islamic community Millî Görüş (Turkish religio-political Islamic organization, GM) has a fatwa commission. A decision of this committee, therefore, is not of an individual person but a committee consisting of at least twelve expert (religious, GM) scholars. Diyanet (the Turkish presidium for Turkish affairs, GM) also has a fatwa committee. I can refer such situations to these committees. A verdict must come from these kinds of committees. So, as a mosque imam I cannot take such a responsibility. Because, may God protect us, even if the chance is one in a thousand of a wrong pronunciation, an imam cannot take that responsibility. For in the Quran, there is a verse that says: whosoever slays a soul – unless it be for another soul or working corruption upon the earth – it is as though he slew mankind altogether. . . (Quran 5: 32, GM). This could confront us with being guilty of killing humanity in its entirety. As an imam, I absolutely cannot assume such a great responsibility.” (Participant 1)
Mask your grief
When death is inevitable, only God can bring salvation by giving eternal live in heaven. Qualifying for such salvation requires an attitude in which the dying fully trusts God. Therefore, religious guidance should focus on stimulating the dying to reinforce this trust by affirming his/her belief in God.
“Guiding him spiritually and reminding him of religious things was also something I wanted to do as an imam. The only thing that would keep him going was faith. Surrender to God, trust in God, the only one who could help. Belief in God. . .There is nothing else that keeps man on his feet.” (Participant 4)
To prevent the dying from becoming ineligible for salvation by giving up hope in God, family should radiate hope and hide their grief in direct contact with the dying.
“I explained to them that a family has many tasks. Being a family during the disease process requires a particular course. The family should be aware of this. Their job is to keep the patient from giving up hope in God. Although the family is affected by the patient’s illness, they should not show this to the patient but radiate hope. They should not let the patient notice a negative influence (of his sickness, GM) on their body language (and should hide, GM) their psychological breakdown, as much as possible.” (Participant 4)
Discussion
Main findings
This study shows how imams construct their roles in palliative care. Our Directed Content Analysis informs the Narrative Analysis by showing how transformation of this task is modulated through its role content. In turn, the Narrative Analysis informs the Directed Content Analysis by revealing motives behind religious advice and demonstrating its function within the story types. Our Directed Content Analysis revealed two patterns in response to proposals to withhold or terminate treatment. Where the first aims to maximize treatment, the second revolves around dealing with religious responsibility. The pattern aimed at maximizing treatment is narrated through the narrative Hope can work miracles. Modulated through the role content of exegete, the how of the story explains healing as God’s reward for striving for maximum treatment. This is complemented through the role of adviser by pointing out misdiagnoses in which patients recovered. The missionary-linked content, the why of the story, underscores God’s omnipotence. Consequently, diagnostics that imply absence of cure should be rejected. Therefore, medical decision-making is constructed as a matter of faith in which not giving treatment (for reasons of hopelessness or futility) represents disbelief while hope for miraculous healing by striving for maximum treatment objectifies true belief in God.
Miracle-driven belief in cancer patients is known to reduce the ability to understand prognostics. 26 Patients’ relatives sometimes believe that God’s omnipotence manifests itself through intervention in the course of the disease.27,28 In our data such belief—attached to striving for maximum treatment, aimed at inviting God to perform a miracle, as it were—is not just optional but presented as a condition for being a faithful Muslim. In a taxonomy that classifies God-attributed miracles, unshaken evocations concern a category in which belief in miracles is embedded in religions with worldviews enjoying supreme authority. 29 Since Muslims are committed to consistency between religious norms and treatment proposals affirmed through their imams, this is likely to affect clinical practice.30,31 Projected onto our results, it evokes an image in which religion-based belief and evidence-based medicine are antithetical.26,32–34
The second pattern, which concerns religious responsibility, is narrated through the narrative Responsibility needs to be shared. The how of the story concerns the probability of being held accountable by God in the hereafter that comes with the role of jurist. This is due to interference with the moment of death by agreeing to withhold or terminate treatment. The missionary-role-linked message is that God disposes over life and death. Therefore, those who agree to terminate treatment run the risk of unauthorized access to His domain.
The tendency among participants to pass on questions about medical decision-making to fatwa committees is a present-day form of the traditional Islamic way of dealing with applied ethics. In it, imams are part of hierarchical structures in which fatwas are no longer the domain of the individual mufti.16,35,36 They are now part of the collective effort of expert committees.35,37–39 Our data show that participants made exclusive use of such fatwas issued by their own organizations. Imams disseminate viewpoints on decision-making in palliative care that have been determined top down among their congregants.2,22,40–42 Some of our participants issued fatwas themselves. This fits within a development in which imams fulfill tasks because the institutions that provide these in the country of origin are lacking.16,18,43
Strengths and limitations
Participants were aware that the interviewers were Muslims. We believe that this shared religious identity made it easier for them to speak about the sensitive nature of palliative care. However, our sample predominantly consisted of imams representing transnational organizations. Therefore, one might wonder to what extent our data are personal views or representations of the formal Islamic views and policies of these organizations. We believe this characteristic constitutes both strength and limitation. A strength is that our research provides insight into how imams as representatives of organizations contribute to the shaping of palliative care. A limitation is that is not always clear where personal views were expressed. Conversely, we think that they saw representing normative Islamic views as obvious, as this was linked to their professional identity. Another limitation is that our sample is limited to Turkish imams. Therefore, different results might be observed in follow-up studies including imams from other Muslim minorities.
What this study adds
Our study shares similarities with earlier research among lay-Muslims about end-of-life decision-making. A common denominator is the view that God is omnipotent and disposes over life and death.44–47 For some this means that treatment may be withheld or terminated to avoid suffering because God ultimately decides the moment of death, while this is very hard for others since it undermines belief in God’s omnipotence to cure.44–47 Our findings suggest that imams emphasize God’s omnipotence to cure by pushing for maximum treatment. Striking in this context was the impact of fear among participants. Taking medical decisions in palliative care for family members is known to evoke negative emotions, including the fear of interfering with God’s plan.48–51 It is this fear that motivated participants to refrain from issuing statements about withholding or terminating treatment. This suggests that they view issuing fatwas in such cases as synonymous with becoming decision-makers.
Our findings reveal a gap between palliative care tailored to individual patient needs and an afterlife-orientated approach by imams that stresses the religious responsibilities of all involved.44,45,52 This is worrisome since research points to unequal access and less favorable outcomes of palliative care among minorities.52,53 What is needed is tailor-made palliative care embedded within cultural-religious frameworks that meets the specific needs of Muslim patients and their social system. 52 To develop this requires policy and concrete action from healthcare providers to build sustainable relationships with imams and their congregations aimed at working together in the interest of the Muslim patient. 53
Conclusions
The imams’ insistence on maximizing treatment in their advice to patients’ relatives in medical decision-making in palliative care is intertwined with the fear of being held accountable by God for intervening with His omnipotence and will. As a result, clinical practice may face negative attitudes among Muslims toward proposals to withhold or terminate treatment which are at odds with medical views on good palliative care. To bridge this gap, palliative care policies tailored to the needs of Muslims need to be developed in close cooperation with imams and their congregations. To broaden the understanding of imams’ contributions to palliative care, future research should include imams of different ethnic backgrounds.
Footnotes
Acknowledgements
We express our sincere appreciation to Nazmi Yilmaz (NY) for reviewing the translations of the transcripts of the interviews.
Author contributions
GM, NT, AdlC, GW, and HvL designed and wrote this study.
Data management
The data are available on request from the first author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.