
Abstract
Background:
New public health approaches to palliative care such as compassionate communities aim to increase capacity in serious illness, death, and loss by involving civic society. Civic engagement has been described in many domains of health; a description of the characteristics, processes, and impact of the initiatives in palliative care is lacking.
Aim:
To systematically describe and compare civic engagement initiatives in palliative care in terms of context, development, impact, and evaluation methods.
Design:
Systematic, mixed-methods review using a convergent integrated synthesis approach. Registered in Prospero: CRD42020180688.
Data sources:
Six databases (PubMed, Scopus, Sociological Abstracts, WOS, Embase, PsycINFO) were searched up to November 2021 for publications in English describing civic engagement in serious illness, death, and loss. Additional grey literature was obtained by contacting the first authors. We performed a quality appraisal of the included studies.
Results:
We included 23 peer-reviewed and 11 grey literature publications, reporting on nineteen unique civic engagement initiatives, mostly in countries with English as one of the official languages. Initiatives involved the community in their development, often through a community-academic partnership. Activities aimed to connect people with palliative care needs to individuals or resources in the community. There was a variety of evaluation aims, methods, outcomes, and strength of evidence. Information on whether or how to sustain the initiatives was generally lacking.
Conclusions:
This is the first review to systematically describe and compare reported civic engagement initiatives in the domain of palliative care. Future studies would benefit from improved evaluation of impact and sustainability.
Keywords
Public health perspectives on palliative care transcend an individual, service-centered interpretation of palliative care, and value community responses such as civic engagement.
Previous studies in different domains of health and wellbeing have described the positive impact of civic engagement initiatives, but a systematic description of civic engagement initiatives in palliative care is lacking.
All initiatives were initiated after the year 2000, except for one that was initiated in 1995. The year of initiation ranges from 2000 to 2020. Given the fact that we searched for publications in English, a majority of the initiatives are located in countries with English as one of the official languages.
All initiatives in this review engaged with the community in their development, most often through a community-academic partnership. Initiatives offered a variety of civic engagement activities generally aiming to provide a link between seriously ill people and their caregivers and other resources in the community.
Although we found that all the evaluation studies showed a positive impact; most conducted either a process or an outcome evaluation without including sustainability as one of the evaluation outcomes.
Considering the variation in quality of the evaluation studies, there is a need to conduct in-depth evaluations measuring both the impact of the civic engagement initiatives and the mechanisms that lead to this impact.
Future research should evaluate factors that influence the sustainability of a civic engagement initiative, and should evaluate the influence of embedding the initiative in a compassionate city context on its continuation.
Background
Demographic and epidemiologic trends increasingly confront individuals with the challenges of serious illness, caregiving, dying, loss, and bereavement, whether as the person with serious illness, a caregiver, or just as a relative, friend, neighbor, etc.1,2 Palliative care can offer added value in this regard by increasing the quality of life of both the person with serious illness and their informal carers. However, as is discernible from recent discussions in the literature about the definition and branding of palliative care,3–5 the term comes with different interpretations. A common interpretation of palliative care is one that sees it as a formal healthcare service approach aimed at optimizing individual care relationships and improving distressing symptoms for patients and those close to them.3,4 Others point to the informal dimension and affirm that palliative care is also provided by friends, family members, and the wider community.3,4 In turn, public health perspectives on palliative care insist on the social ecological dimension where palliative care is framed as more than a response to the individual problems and challenges of serious illness by healthcare services or informal caregivers, but includes societal actions designed to improve or promote health and wellbeing around illness, death, dying, loss, and bereavement.5–7 Kellehear, 8 for instance, has formulated this in the notion of caring for one another during times of confrontation with serious illness, death, dying, loss, or bereavement as a responsibility for everyone.
Compassionate communities have grown out of this public health approach and entail “A community of people who are passionate and committed to improving the experiences and well-being of individuals who are dealing with a serious health challenge, and those who are caregiving, dying, or grieving. Members of a Compassionate Community take an active role in supporting people affected by these experiences. This can be done through connecting people to helpful resources, raising awareness about life and end of life issues, and building supportive networks in the community (p. 1).” 9 However, engaging community members on topics such as serious illness, death, and loss can be a challenge. Civic engagement is an important way of engaging people in civil society,8,10,11 and can be interpreted as collective action undertaken to help improve connections between, or conditions for, people in the community.12–14 We interpret civic engagement as an umbrella term for both volunteering and informal caregiving as the context is the community, as it can be both performed from a personal connection with the person receiving support, as is the case in caregiving, or from a broader social interest position, as is often the case in volunteering.12–15
Previous studies have described the positive impact of such civic engagement initiatives in other domains of health and wellbeing,16–21 for example, serving as a bridge between older people and youth.17,18 However, the context, processes, evaluation, and impact of civic engagement initiatives in palliative care have not yet been systematically described. Consequently, the aim of the review is to systematically describe and compare the reported initiatives of civic engagement in serious illness, death, and loss in terms of the context in which they were initiated, their development and sustainability, whether and how they were evaluated, and their impact. By describing these characteristics, we aim to provide inspiration for current or developing initiatives, for the activities they can undertake, and for ways to sustain and evaluate them.
Specific research questions are:
(1) In what context, why and for whom are civic engagement initiatives around serious illness, death, and loss initiated?
(2) How are they developed and how are they sustained?
(3) How have they been evaluated, and what is their impact?
Methods
Protocol and registration
A protocol of the review was prospectively registered in Prospero July 5th, 2020. Registration number: CRD42020180688 (https://www.crd.york.ac.uk/prospero/#recordDetails). The protocol was edited on March 29th 2021, in order to clarify our focus on civic engagement, instead of the narrower term “volunteering.”
Review design
We conducted a systematic, mixed-methods review of civic engagement initiatives in palliative care reported in peer reviewed literature, following the “Methodological guidance for the conduct of mixed-methods systematic reviews.” 22 Results were reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 23
Search strategy
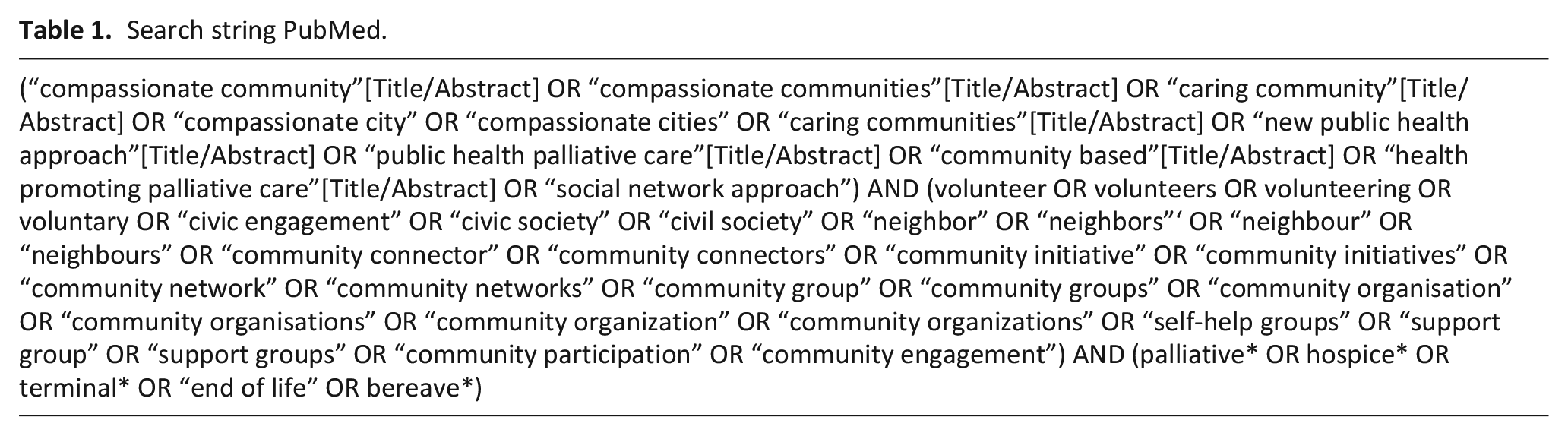
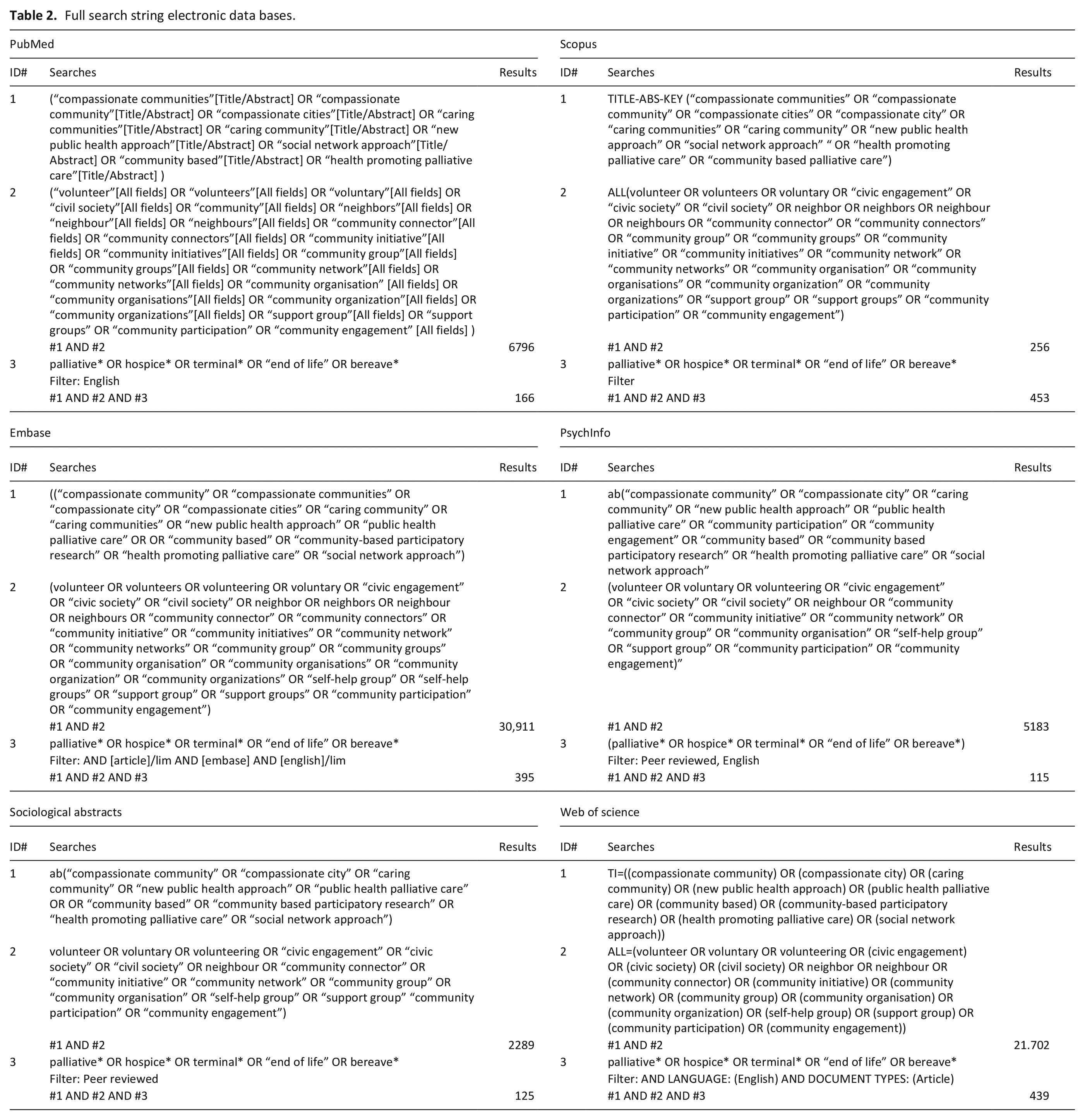
Due to the dearth of knowledge on the domain of civic engagement in serious illness, dying and loss, we argue it is a good first step to start from peer reviewed literature to gain a first insight into initiatives that are being researched. Peer reviewed literature in English language publications was searched through six databases: PubMed, Scopus, Sociological Abstracts, Web of Science, Embase, and PsycINFO, by using set eligibility criteria. In Scopus, Sociological Abstracts, Web of Science, Embase, and PsycINFO a limit was applied to acquire peer reviewed literature only. A search string was developed by the research team in cooperation with a librarian from the VUB library consisting of three main elements and their synonyms: compassionate communities, palliative care, and civic engagement. The search string does not include “care” because this term is a too general description of compassionate communities, or a public health palliative care approach. Instead we used the term “caring communities” because it is more specific, and sometimes used as a synonym for compassionate communities. The search string was validated in PubMed (Table 1) and translated to the other databases (Tables and figures, Table 2). No limited timespan for literature was applied in the databases. Literature was searched up to November 2021. We searched the reference list of the included articles for peer reviewed literature on other initiatives. Next, additional grey literature publications (including websites of initiatives) were searched by contacting the first authors of the included articles. We contacted fifteen authors of whom eleven replied after sending a reminder e-mail. For those initiatives we did not have the contact details from the authors or for which the author did not reply, we performed a limited Google search in order to include the official website of initiatives. We performed a limited Google search for five of the initiatives.
Search string PubMed.
Full search string electronic data bases.
Eligibility criteria
Publications were eligible for inclusion if:
(A) They were written in English, and
(B) Described one or more civic engagement initiative in which community members identify certain challenges in their community concerning serious illness, death, and loss, and
(C) Decide to mobilize collectively in order to address these issues.
Publications were excluded if:
(D) They reported on public engagement that is essentially service-centered, meaning that the engagement work has the main aim of enhancing the quality or reach of a professional service, and the engagement is described as a formal part of this service.
Study selection
The articles from the database searches were imported into the electronic systematic review program Rayyan. Duplicates were removed by the program. The imported peer reviewed literature was first screened on title and abstract. Articles were either given the label “included,” “excluded,” or “maybe.” Articles that were labeled as “included” or “maybe” in the first screening were subjected to a full text screening. In order to be eligible, articles had to meet the three inclusion criteria and not fall within the exclusion criterion. The screening and study selection were independently performed by two researchers (LDEE and BQ). There was an initial disagreement about 19 articles between the researchers, 16 of which were resolved. The three remaining disagreements were resolved by an independent screening by a third reviewer (TS). The study selection resulted in 23 included publications, reporting on nineteen unique civic engagement initiatives.
Data extraction
Data were extracted from the included peer reviewed and grey literature publications to answer the research questions on their context, development and evaluation. A data extraction form was pilot tested for the identified studies found in PubMed. This resulted in the following variables for which data were extracted from the included publications:
– Regarding the context of the initiatives: (1) name of the initiative, (2) year of initiation (3) country and continent, (4) reason for initiation, (5) target group.
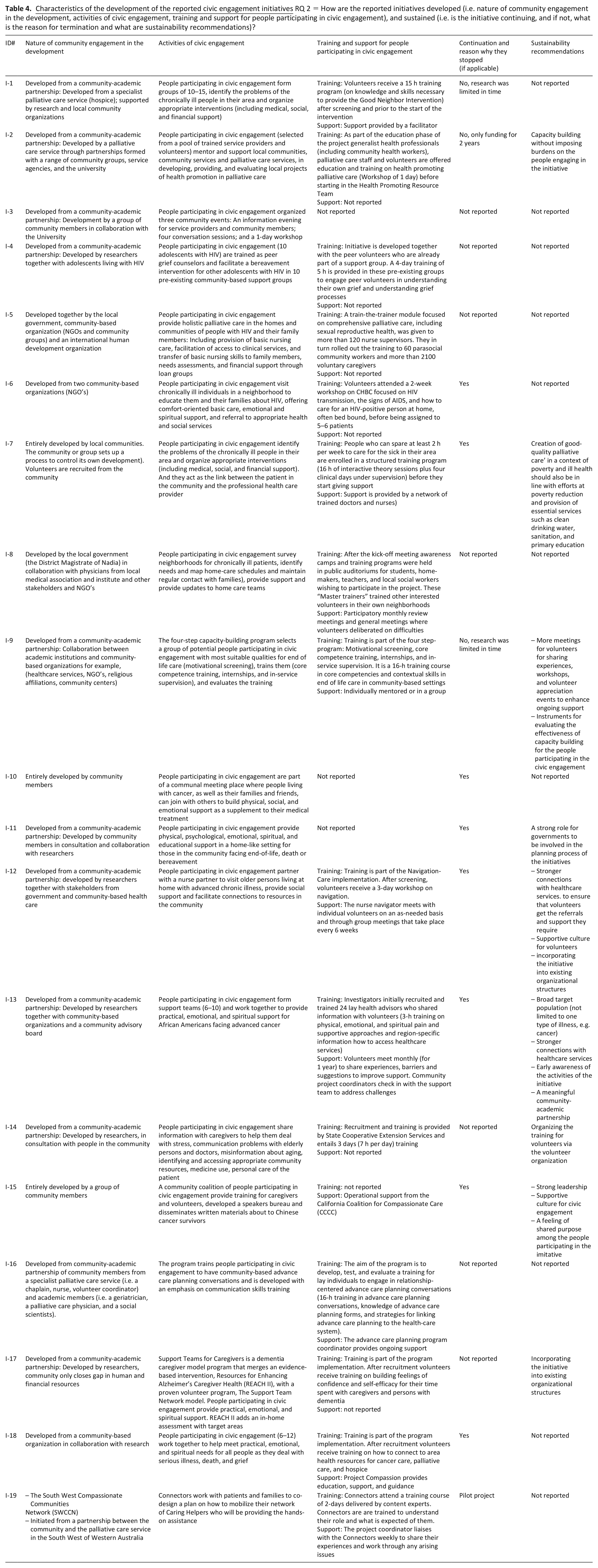
– Regarding development of the initiatives: (1) nature of community engagement in the development (i.e. did the community develop the initiative themselves? Or if not, were they informed, consulted or did they collaborate with others partners in the development?), (2) activities of civic engagement, (3) training and support for people participating in civic engagement, (4) continuation (i.e. is the initiative still ongoing at the moment of this publication and if not, what are the reasons for termination), and (5) sustainability recommendations (i.e. recommendations from studies to other initiatives to increase or ensure the continuation of their civic engagement activities).
– Regarding evaluation of the initiatives: (1) the aim of the evaluation, (2) evaluation design (3), data collection methods, and (4) impact of the initiative.
For each variable, exhaustive data from the article was put directly in the data extraction form (Tables 3–5). This data was supplemented by the data from the reference list search and from the grey literature search. Data extraction was independently performed by LDEE (entirely) and by BQ for 25% of the publications (five articles).
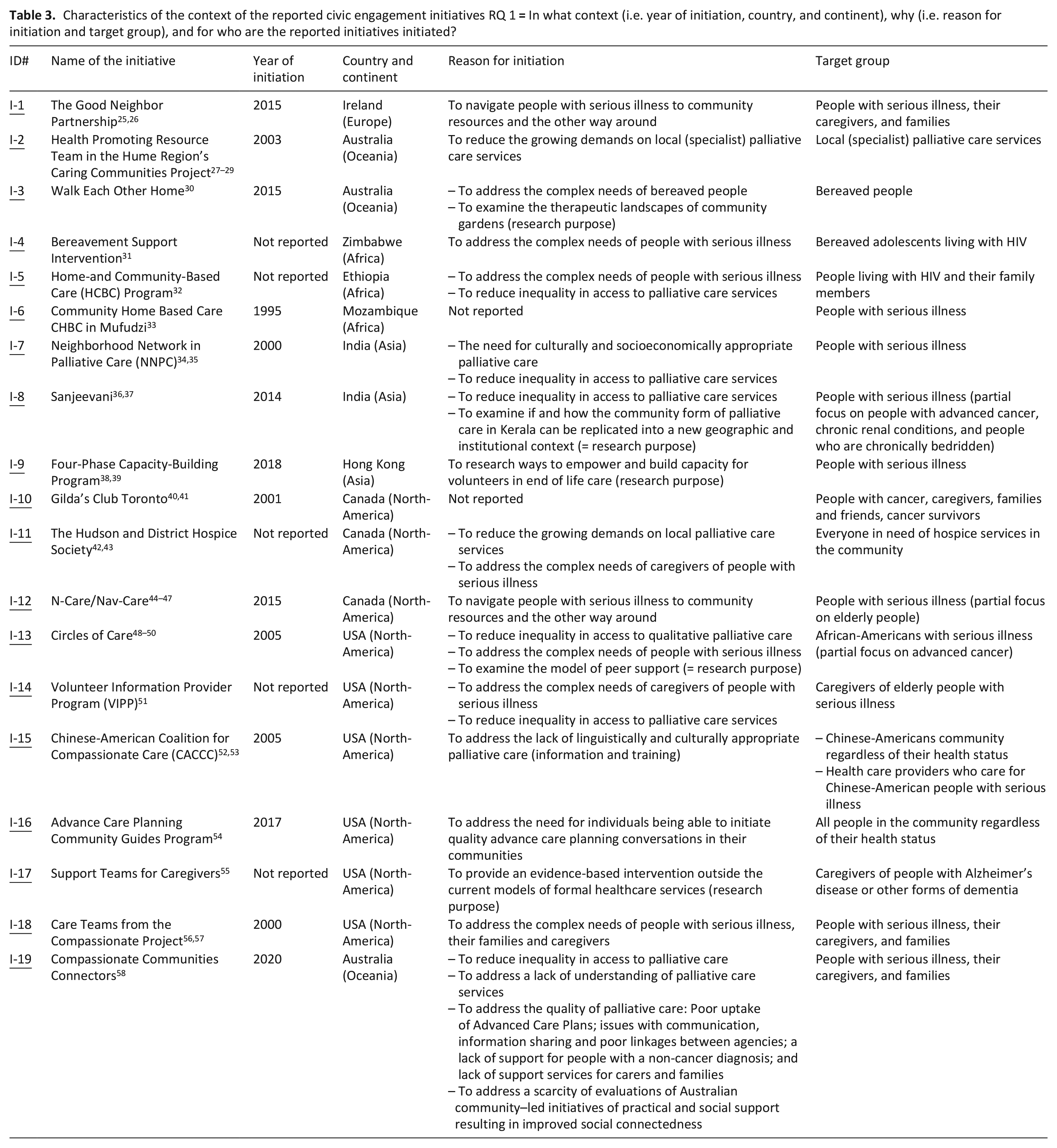
Characteristics of the context of the reported civic engagement initiatives RQ 1
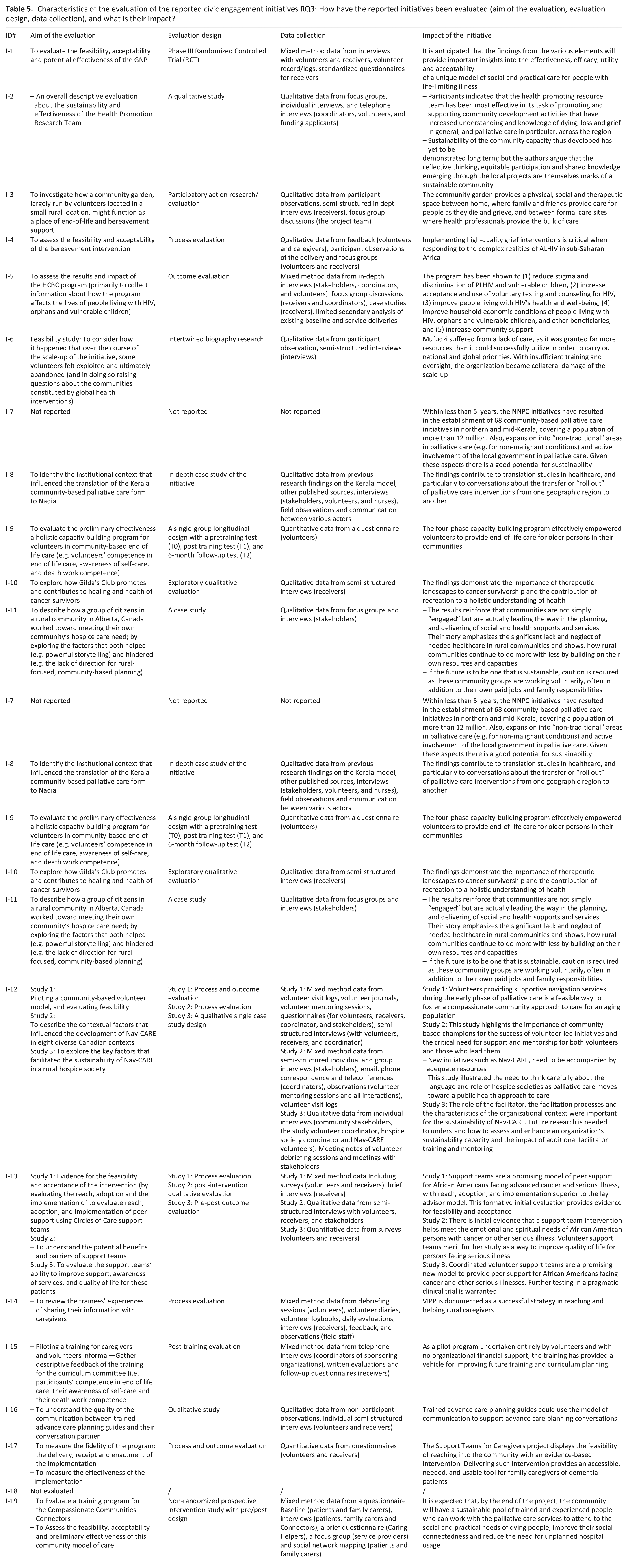
Characteristics of the evaluation of the reported civic engagement initiatives RQ3: How have the reported initiatives been evaluated (aim of the evaluation, evaluation design, data collection), and what is their impact?
Data synthesis and analysis
We conducted a convergent integrated approach to synthesize data from qualitative, quantitative, and mixed-method studies. 22 We produced a descriptive paragraph on each of the included studies, thereby providing textual descriptions not only of the qualitative data but of the quantitative and mixed-method studies as well. Consequently, the author (LDEE) examined the assembled data and grouped this data into categories, based on their similarity in meaning. These categories were reviewed by and discussed together with author B.Q. in order to come to a consensus.
Quality appraisal
We performed a quality appraisal of those civic engagement initiatives that were evaluated in a study. The quality appraisal was conducted using a self-developed tool based on the Mixed Method Appraisal Tool (MMAT) 24 (Tables and figures, Table 6). We adapted two screening questions from the MMAT: (1) are there clear research questions or is the aim of the evaluation clear? and (2) does the collected data allow us to answer the research questions or aim? If one or both of these screening questions was answered negatively, the appraisal was stopped and a score of 0 out of 4 was assigned. If both screening questions could be answered “yes” the following two self-developed screening questions were answered: (1) are the results adequately derived from the data? (2) is the conclusion sufficiently substantiated by data?, For each question answered “yes,” one point was given. Next, we calculated a total quality score by summing the scores of the individual questions, ranging from 0 to 4, with higher scores indicating better quality. Quality appraisal was entirely performed by LDEE, and by BQ for 25% of the included articles (five articles).
Quality appraisal tool.
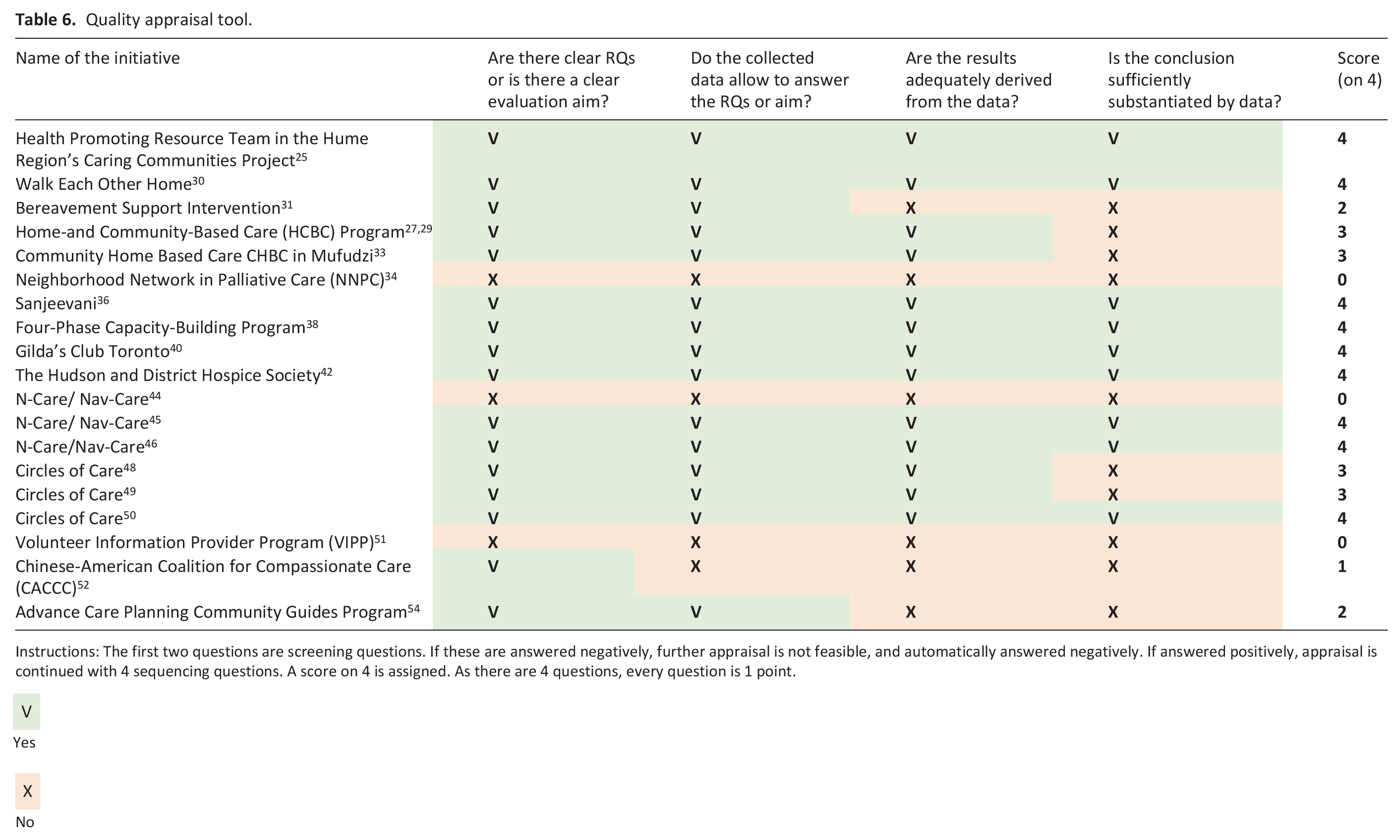
Instructions: The first two questions are screening questions. If these are answered negatively, further appraisal is not feasible, and automatically answered negatively. If answered positively, appraisal is continued with 4 sequencing questions. A score on 4 is assigned. As there are 4 questions, every question is 1 point.

Yes

No
Results
Study selection
The process of study selection is depicted in a PRISMA flow chart 23 (Figure 1). From the 23 included publications, we searched the reference lists and found two additional peer reviewed publications that met the eligibility criteria. These two additional articles were not identified through the database search because they focused on one specific serious illness (dementia or cancer) and could therefore not be identified using the general terms (palliative* OR hospice* OR terminal* OR “end of life” OR bereavement*) included in the search string. In the next phase, we included eleven additional grey literature publications by contacting the first authors of each of the articles.
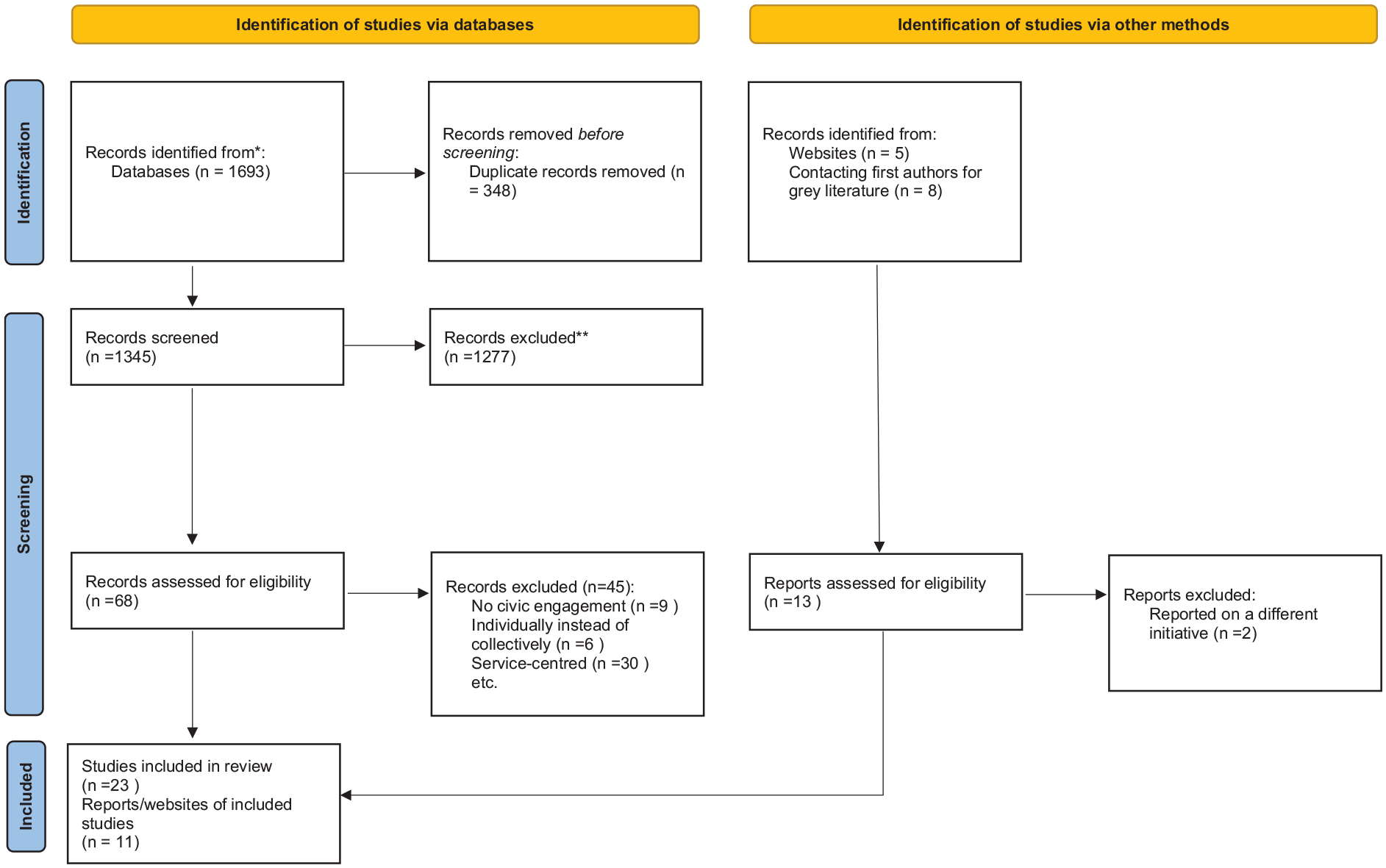
PRISMA flowchart of the study identification, screening, eligibility, and inclusion process.
Results on civic engagement initiatives
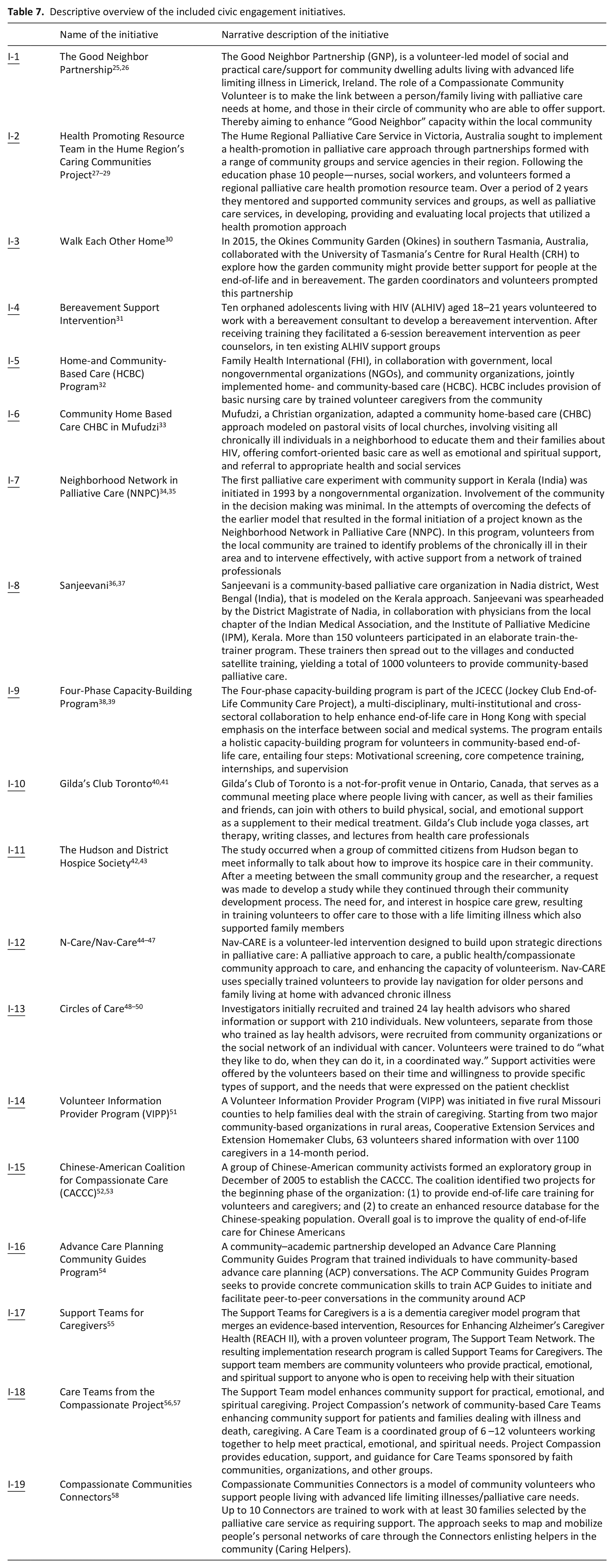
The 23 peer reviewed and 11 grey literature publications reported on nineteen unique civic engagement initiatives, included in Table 7, a descriptive overview of the included civic engagement initiatives.
Descriptive overview of the included civic engagement initiatives.
Characteristics of the context of the initiatives
All initiatives were initiated after the year 2000, except for one that was initiated in 1995. 33 The year of initiation ranges from 2000 to 2020, with an equal distribution of initiatives being initiated in the first and second decade. Given the fact that we searched for publications in English, a majority of the initiatives are located in countries with English as one of the official languages, except from the initiative in Ethiopia. 32 We found initiatives in North America40–58 (in Canada or in the USA), Oceania27–30 (Australia and in Europe25,26 (Ireland). Other initiatives are located in Asia34–39 (India, Hong Kong) and Africa31–33 (Zimbabwe, Ethiopia, and Mozambique). The geographic distribution of the initiatives is depicted on a map (Tables and figures, Figure 2).
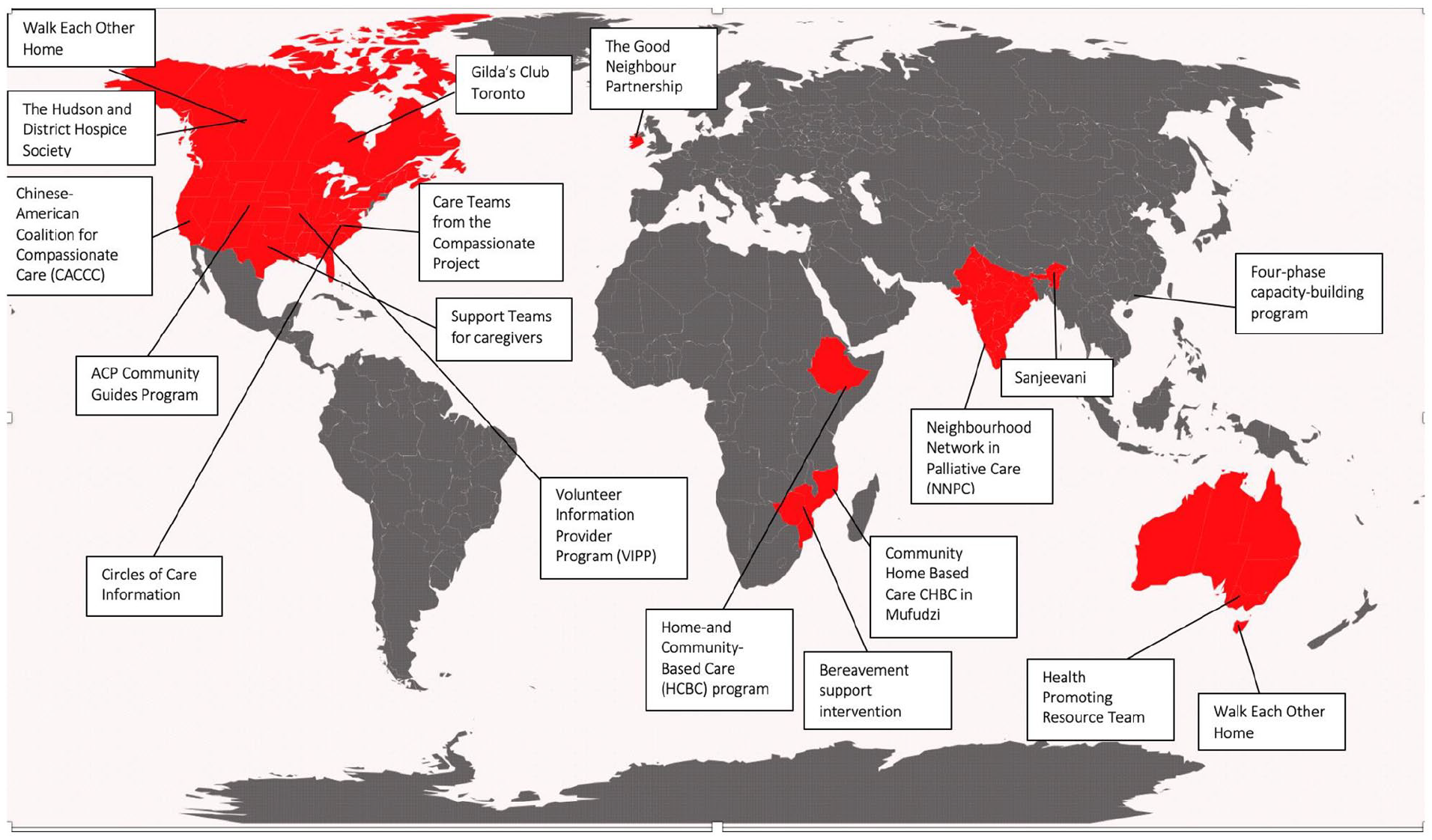
Geographic distribution of the initiatives.
Reasons for initiation vary. Most cited reasons were to address the complex needs of people in the community with serious illness and/or their caregivers and families,30,32,42,43,48–50,56,57 to reduce inequality in access to quality palliative care,32,34–37,48–51,58 and for research purposes30,36,37,48–50,58 such as to examine a model of peer support48–50 or to study ways to empower and build capacity for civic engagement in end-of-life care.38,39
Target populations of the initiatives included healthcare providers,27–29,52,53 all people in the community regardless of their health status,42,43,54 or people in the community with a serious illness, their family or caregivers.25,26,30–41,44–53,55–58 Some of the initiatives partially focused on people with a specific condition such as HIV and AIDS31,32 or cancer.36,37,40,41,48–50 Others partially focused on adolescents, 31 older people,44–47 African-Americans,48–50 Chinese-Americans,52,53 bedridden people,36,37 or cancer survivors.40,41
Characteristics of the development of the initiatives
In all the initiatives, the community was involved in the development process. Twelve out of 19 were developed from a community-academic partnership.25–31,38,39,42–51,54,55 In eight of these initiatives, the community led the development and consulted or collaborated with a research team.25–31,42–47,54,56,57 In the other four, the community was involved to a limited extent; researchers developed the initiative in consultation or collaboration with community members.30,38,39,51,55 The other seven initiatives were entirely community-owned and were driven and developed by community organizations and/or governments without any input from research,32,33,36,37,58 or by individual community members.34,35,40,41,53
The actions of the initiatives were generally aimed at linking people with care needs to those in the community who could provide help, to professional health care or to other community resources.32–37,44–47,58 Additionally, activities included identifying the problems of the chronically ill people in their area,25,26,32,34–37 providing social and emotional, physical, spiritual, practical, or financial support for ill people in the community or those affected.32,34–37,40–42,44–50,55–57
Almost all the initiatives included training for those participating in civic engagement.25,26,30,32–36,38,39,44–51,54–58 The intensity and content of the training varied per initiative. The content included training on navigation to community resources and how to access them,44–50,54,56–58 and competencies in providing palliative care and end-of-life care.25,26,31–35,38,39 As well as training, a minority of the initiatives provided ongoing support to those participating in civic engagement,25–29,34–39,44–50,54,57,58 such as individual feedback opportunities with a mentor or peer-support group meetings.36,37,44–50,58
Eight out of 19 initiatives mentioned continuing their civic engagement activities.33–35,40–43,48–50,52,53,56,57 These eight were either entirely developed by the community31,34,35,40,41,52,53 or by a community-academic partnership in which the community had made a far-reaching contribution in the development process.42–47,56,57 Of the remaining initiatives, a majority did not report whether they still existed. The three that explicitly mentioned they had stopped,25–29,38,39 reported that funding ceased, or the research had been time-limited from the beginning. For the other ten, information was lacking on their intentions regarding sustainability.30–32,36,37,51,54,55,58 A majority of studies did make recommendations to other initiatives to increase the sustainability of their civic engagement activities.27–29,32,34,35,42,43,50–55 The sustainability recommendations varied, and included ongoing education and mentoring of people participating in civic engagement,38,39,51 and creating a culture of civic engagement in the community.44–47,52,53
Characteristics of the evaluation of the initiatives
An evaluation study was conducted for 1825,27,29–34,36,38,40,42,44,45,48–50,55,58 of the 19 initiatives. Most of these studies involved a process evaluation25,30,31,33,36,40,45,48,49,51,54; a minority evaluated outcomes27,32,38,50 or conducted both a process and outcome evaluation.44,55 The majority of the initiatives were evaluated using qualitative27,30,31,33,36,40,42,46,49,54 or mixed method25,32,44,45,48,51,52,58 data collection including interviews, focus groups, observations and surveys. The quality of the evaluation differed between the initiatives. Three received a score of 0 (out of 4),34,44,51 as a result of not being able to answer the two screening questions positively. One initiative received a low score of 1 52 as a result of answering negatively to the three follow up questions. Furthermore, most of the initiatives received a score of 2 or 3.27,29,31,33,48,49,54 A minority had an evaluation of a very high quality and received a score of 4.25,30,36,38,42,45,46
Most of the evaluation studies focused on one particular aspect of the initiative, such the role in healthcare or the voluntary organizations in the development process. 36 Also the feasibility, acceptance and reach of initiatives25,31,44,48,58 was measured and their preliminary effectiveness on certain outcomes27,29,32,40,50,55 (e.g. empowered people to provide end-of-life care for older persons in their communities 38 ); there were studies on how an initiative contributes to the health of cancer survivors, 40 on how a community garden might function as a place of end-of-life and bereavement support, 30 and the contextual factors that helped (e.g. community-based champions) and hindered (e.g. the lack of direction for rural-focused, community-based planning for hospice care by government) people in their civic engagement activities. 45 Almost all the initiatives demonstrated positive benefits as a result of civic engagement,27,29–32,34,38,40,42,44–46,48–52,54,55 including increased understanding and knowledge of dying, loss and of palliative care in the community.27,29 A minority of the studies included the sustainability of the initiative in their results, for example, if the future is to be one that is sustainable, caution is required as these community groups are working voluntarily, often in addition to their own paid jobs and family responsibilities. 42
Discussion
Main findings
This review identified nineteen unique civic engagement initiatives concerning serious illness, death, and loss, often referred to as “compassionate community initiatives.” The identified initiatives are mostly located in countries with English as one of the official languages. Activities performed by community members participating in them included various forms of support, including identifying the problems of the chronically ill people in their area and organizing appropriate interventions. In those initiatives that still existed at the time of this review, the community had the lead in the development process. Although sustainability is a common challenge for all the initiatives, none of the evaluation studies focused on sustainability but consisted mostly of either a process or an outcome evaluation, and were often focused on one particular aspect of the initiative, for example, researching the institutional context in which an it developed. 36
Civic engagement: Blind spot in non-English speaking contexts
In 1986 the Charter for Health Promotion was adopted in Ottawa, Canada, in order to give direction to a new public health approach in various domains of health and wellbeing. The translation of this health-promotion approach to the domain of palliative care was first explored by Allan Kellehear in 2000 in an Australian context. Kellehear 59 founded the compassionate city movement, in which geographically defined regions work toward culture change concerning serious illness, death, and loss by working together with various stakeholders, including local governments, cultural organizations, health and social care organizations, schools, etc. In the following years, the compassionate city movement found support mainly in Australia and in the UK where the political welfare system considers volunteering and civic engagement as an essential supplement to the mainly service-driven organization of palliative care.60–62 We identified nineteen civic engagement initiatives worldwide, almost all in countries with English as one of the official languages. This finding triggers a few critical notes. Firstly, we must note that we only searched for publications in English, thereby excluding those written in other languages. Also, as it often concerns bottom-up initiatives, there is a chance that some are not reported or described in scientific literature—particularly in non-English speaking contexts. Secondly, the civic engagement initiatives we found mainly originated from a bottom-up compassionate community approach instead of a conjuncture of top-down mediations (e.g. creating a supportive policy) and bottom-up approaches (e.g. stimulating community action), as is the case in compassionate cities. This may give the impression that the civic engagement movement is an extension of the Anglo-Saxon compassionate city influence; however, literature shows that some African and Asian regions had already organized themselves into compassionate communities before the concept came into use in Australia and the UK. 63 Future research should therefore investigate the potential blind spot of starting compassionate communities in non-English speaking contexts or not published in English, together with the cultural and political aspects that influence the initiation of civic engagement.
Civic engagement initiatives: Commonalities and differences
The initiatives that we identified show great variation in their context, development and evaluation, but there are also important commonalities. These include engaging communities in providing a link between a person with palliative care needs and those in their community who are able to offer help.44–47,58 This differs from the common service-centered approach that primarily focuses on clinical contributions and treating illness. Rather, compassionate communities apply a salutogenic approach by trying to increase the overall wellbeing of people through health-promotion. 7 Accordingly, in these initiatives, the community as the core of social interactions provides this social support for people confronted with illness, death, and loss. Another important commonality is that most of the initiatives provide training and ongoing support for community members involved in civic engagement. This includes, for instance, individual feedback sessions with a mentor or group sessions with peers.36,37,44–50,58 Although such training and support is widely provided by the initiatives, many of them recommend that it is a recurrent event throughout the entire course of the initiative, in order to increase the chances of sustainability.38,39,44–46
A lack of information on sustaining civic engagement initiatives
Some the evaluation studies mentioned the sustainability of the initiative in their results, for example, the role of the facilitator and the characteristics of the organizational context are important for the sustainability of the initiative. 64 However, although the evaluation studies measured for instance the feasibility and applicability of the civic engagement activities, the results of these feasibility study were often not discussed in the light of whether or not to continue the initiative, or under which conditions the initiative should continue to exist. The three initiatives that explicitly mentioned they ended,25–29,38,39 and provided reasons for not continuing, all indicate that funding ceased or research was time-limited from the outset. From this we can tentatively suggest that in community-academic development processes sufficient attention should be paid to empowering the community to continue the initiative when the research ends. Additionally, initiatives should search for alternative funding sources if necessary. As suggested in some of the publications, activities may also be more sustainable if integrated into a context of broader public involvement for encouraging a civic engagement culture in the community.44–47,52,53 Compassionate city programs have been suggested for the purpose of facilitating and stimulating ongoing community action. Through involvement of stakeholders and endorsement by the city council they provide an overarching structure for community engagement, build public health policy, create supportive environments, enhance personal skills, and reorient health services toward the topics of illness, death, dying, loss and bereavement. 8 Future research should investigate the influence of embedding civic engagement initiatives in a compassionate city context on their sustainability.
The need for a thorough evaluation of civic engagement initiatives
Evaluation of civic engagement initiatives remains a challenge. Although all evaluations reported positive outcomes, the results are impossible to compare across the different initiatives as they vary in quality, content and in the way they were studied. Literature suggests that frameworks on how to evaluate civic engagement initiatives in palliative care are needed to build up a robust body of evidence that allows us to increase the overall quality of the evaluation.65–67 Existing guidelines on such complex interventions recommend evaluating both the process of development and the impact of the initiative by using a mixed-method approach to data collection.64,68 Although some of the studies do use mixed method data collection, evaluation is often limited to either the process of development or to specific outcomes. Additionally, the evaluation studies exclusively focus on whether the objectives of the intervention are achieved, rather than providing a clear rationale for the choice of objectives and outcomes. Future research could be ground breaking in sharing experiences not only of measuring the impact of such initiatives but also of better comprehending in which context and through which mechanisms impact can be achieved.
Strengths and limitations of this review
A mixed-methods review is the most suitable design to systematically describe a variety of initiatives in different contexts. Since compassionate community volunteer initiatives often rely on public promotion, additional grey literature on the included initiatives was also searched. By searching and retrieving data from both peer reviewed and grey literature, we were able to provide a more comprehensive description of the initiatives, including the characteristics of their context, development, and evaluation. Due to the dearth of knowledge on the domain of civic engagement in serious illness, dying and loss, we argue it is a good first step to start from peer reviewed literature to gain a first insight into initiatives that are being researched. However, having received only additional grey literature for six of the initiatives by the authors, and by performing only a limited Google search for websites of the initiatives, we potentially missed other grey literature documents. An independent grey literature search could have provided us with additional data (e.g. reports, secondary websites, blogs) on the included initiatives, or on initiatives that have not been evaluated and therefore are not published in peer reviewed literature. Consequently, we recommend further research to perform a systematic review of grey literature, in addition to this review. However, since we included peer reviewed publications and additional grey literature, it is not surprising that most of those included have already been evaluated in a study. Due to the fact that we included only publications in English, we are likely to have missed initiatives from non-English speaking countries. Furthermore, by using general terms such as “serious illness” and “bereavement” in our search string, we may have missed articles on one specific serious illness or condition. However, focusing on specific serious illness or condition was not an exclusion criterium in this review. Consequently, we did include articles that beside their general description of palliative care or serious illness also mentioned a specific illness or condition, for example, dementia or cancer.
Conclusion
This review identified civic engagement initiatives concerning serious illness, death, and loss around the world, initiated in the first and second decades of the 2000s. The initiatives vary considerably but also share some fundamental characteristics. They all draw on community engagement for their development, they aim to connect people with palliative care needs to people or other resources in the community that can address these issues, and have all reported benefits in—albeit often limited—evaluation. The systematic description of the characteristics, strengths and challenges of the initiatives provides a basis for more informed future civic engagement initiatives concerning serious illness, death, and loss. Such future initiatives may particularly need to pay attention to their integration into public health policy, the need for a thorough evaluation that provides a rationale for the original choice of objectives and outcomes, and a reflection on sustainability based on the results of their evaluation. Better evaluation of civic engagement initiatives in palliative care could contribute to building a body of evidence, and could allow comparison between initiatives.
Footnotes
Authors’ Note
MeSH in PubMed were used for “community based”, “community network”, “volunteering”, “palliative care”. For the other concepts no MeSH headings exist.
Author contributions
All authors contributed to the concept of the article, the study design, the interpretation of the data and the data analysis. LDEE and BQ performed the study selection and data extraction. LDEE, and TS drafted the article. The draft was revised by all authors. All authors gave approval for the final version.
Data management and sharing
Additional data will be made available on request from the corresponding author (LDEE), including all the data extracted and analyzed of the included publications.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the project “CAPACITY: Flanders Project to Develop Capacity in Palliative Care Across Society,” a collaboration between the Vrije Universiteit Brussel, Ghent University, and the Catholic University Leuven, Belgium. This study is supported by a grant from the Research Foundation—Flanders, file number S002219N.
Research ethics
This article does not involve researching human subjects, hence it did not require approval of an Ethics Committee or IRB.