
Abstract
Background:
Patients in palliative care are usually conceptualised as recipients of support from family caregivers. Family caregivers in palliative care are typically defined as providers of support to patients. Little is known about reciprocal dimensions of support provision between patients and family caregivers in palliative care.
Aim:
To identify processes of mutual support between patients and family caregivers in palliative care and factors that contribute to or obstruct mutual support between patients and family caregivers in palliative care.
Design:
Systematic review and narrative synthesis of original peer-reviewed research published between January 2000 and March 2020.
Data sources:
Medline, CINAHL, Embase, AMED, PsycINFO and PsycARTICLES.
Results:
After full-text screening, 10 studies were included. We identified that patients and family caregivers in palliative care can support one another by mutually acknowledging the challenges they face, by remaining positive for one another and by jointly adapting to their changing roles. However, patients and family caregivers may not routinely communicate their distress to each other or reciprocate in distress disclosure. A lack of mutual disclosure pertaining to distress can result in conflict between patients and family caregivers.
Conclusions:
Few studies have focused in whole or in part, on reciprocal dimensions of support provision between patients with advancing non-curable conditions, and their family caregivers in palliative care. Further research is required to identify key domains of mutual support between patients and family caregivers in palliative care.
Family caregivers are a primary source of support to patients in palliative care.
Provision of support between the patient and family caregiver in palliative care is often assumed to be unidirectional – from family caregiver to patient.
Little is known about reciprocal dimensions of support provision between patients and family caregivers in palliative care.
Mutual support between patients and family caregivers in palliative care can be underpinned by mutual recognition of each other’s needs and by remaining positive for one another.
Patient and family caregiver failure to disclose their distress to each other can result in conflict between the patient and family caregiver and limit mutual support between the patient and family caregiver.
Support from the wider family can allow for greater emotional engagement between patients and family caregivers in palliative care.
Reconceptualising the patient in palliative care as having capacity to provide support to family caregivers is needed to advance our understanding on this topic.
Supporting patients and family caregivers in palliative care to disclose their distress to each other has potential to alleviate concerns for both patients and family caregivers and promote concordance among patients and family caregivers in the decision-making process.
Introduction
The palliative care trajectory can be accompanied by a period of considerable distress for patients. 1 Distress can be physical, psychological, and existential in nature, comprising of fatigue, pain, sadness and worry. 1 Between 30% and 40% of patients in palliative care experience acute levels of psychological morbidity. 2 Patients in palliative care rely heavily on assistance from informal sources of support such as family. 3 The term family in palliative care includes not only formalised relationships, but also those that are self-defined or patient-defined as significant. Family caregivers in palliative care are family members, friends and or other people who have emotional and social bonds with a patient, who undertake significant nonprofessional or unpaid care for patients. 4 They provide a combination of physical, psychological, social and existential support to their family member. 5 They also experience high levels of physical, emotional and psychological burden, in their case, associated with their caregiving role. 6 In some cases, family caregivers in palliative care can also feel ill-equipped in their caregiving role 7 and patient overestimation of caregivers’ self-efficacy can result in anxiety and dissatisfaction among family caregivers. 7
Caregiving by family caregivers comprises a significant component of caregiving in palliative care. 8 As the delivery of palliative care services moves increasingly to community and/or primary care, 9 there is a growing expectation that family caregivers will become even more involved in the delivery of palliative care. 10 Moreover, fiscal constraints in formal care provision means that patients in palliative care may become increasingly dependent on family caregivers. 11 Family caregivers in palliative care are by context key stakeholders in the decision-making process12,13 and they operate as an extension to formal services. 14
Notwithstanding the central role of family caregivers in palliative care in caring for their family member, there has been less focus on how patients function as providers of support to their caregiver or how both support one another in palliative care. 15 Studies in palliative care have reported on caring roles enacted by patients towards family caregivers. For example, patients have been shown to prioritise their family caregiver’s wellbeing and attempt to reduce the burden they place on them. 16 Patients have also concealed their own needs from their family caregiver and encouraged family caregivers to take respite during their caregiving role to alleviate their family caregiver distress. 17
However, the mutual nature of support provision between patients and family caregivers in palliative care is not well understood. We know that the burden that patients in palliative care feel that they impose on their family caregivers and the duty that family caregivers feel towards the person they care for can make both prioritise each other’s needs over their own. 18 Indeed, studies in palliative care have shown how remaining positive for one another can help both patients and family caregivers adjust to advanced illness 19 and how remaining collectively steadfast in the face of illness is a dimension to caring. 20 However, reciprocal dimensions to support provision between patients and family caregivers are not routinely mapped out. 15 A systematic review of mutual support between patients and family caregivers in palliative care is therefore useful to enhance our understanding of patients’ and family caregivers’ negotiation of the palliative care journey as a unit.
Aims
The purpose of this review was to systematically identify and examine original evidence on mutual support between patients and their family caregivers in palliative care. The review aimed to identify processes of mutual support between patients and family caregivers in palliative care and describe factors that can contribute to or obstruct mutual support between patients and family caregivers in palliative care.
Methods
We undertook a systematic review and narrative synthesis of original peer-reviewed studies published in full and in English between January 2000 and the end of March 2020, pertaining to mutual support between family caregivers and patients in palliative care. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart 21 to map out the number of records identified, included and excluded, and the reasons for exclusion. The review was carried out between January 2020 and March 2020.
Search strategy
The search was conducted using the following databases: Medline; CINAHL; Embase; AMED; PsycINFO and PsycARTICLES. Search term pathways used in electronic searches were as follows: Palliative care/terminal care/hospice care/end of life care/palliative approach/advanced illness/serious illness/progressive illness ‘AND’ family carer*/family caregiver*/primary caregiver*/primary carer*/patient*/family* ‘AND’ psychosocial support/social support/mutual support/support exchange/reciprocal support/reciprocity. The asterisk in this case was used in order to capture the plural case of these terms. The above search terms were chosen in order to capture studies comprising patients and/or family caregivers in palliative care living with advancing non-curable illness. With respect to mutual support, we chose specific search terms that would capture reciprocity and exchange of support between patients and their family caregivers.
Inclusion/exclusion criteria
We included original empirical peer-reviewed studies that reported on mutual support and/or reciprocity between patients and family caregivers where it was evident that patients and/or family caregivers had received or were receiving palliative care. Given the aims of our review, appraisal pertaining to validity and reliability standard in systematic reviews of interventions was not appropriate. Our protocol was not to exclude on the basis of evidence level because studies to answer our review questions were as to be expected empirical studies which ranged in evidence level (e.g. cohort studies, qualitative studies). For the purpose of this review, we defined palliative care as treatment which aims to meet the physical, social and emotional needs of patients with clearly advancing, non-curable conditions and their caregivers. We did not limit the review to specialist palliative care or to end-of-life care. We included not only studies which sampled both patients and the family caregivers, but also studies that sampled only patients or only family caregivers once the data generated pertained to mutual support or reciprocity between patients and family caregivers. We excluded literature that was not original peer-reviewed published studies (i.e. grey literature) and studies not published in full and in English.
Extraction
The first author (RMcC) ran the search and completed a first screen of all titles and abstracts. Both RMcC and the last author (GF) then independently screened each title and abstract based on the inclusion/exclusion criteria. For articles that were deemed to possibly meet the inclusion criteria, full texts of these articles were retrieved by RMcC and read independently by RMcC and GF. Any disagreements regarding inclusion at this point were resolved through discussion and further review of the article. Figure 1 outlines the PRISMA flow diagram of the conducted review. We tabulated the included studies into a Table 1 under the standard domains of authors, sample, location, methods, study aims and a summary of key findings.
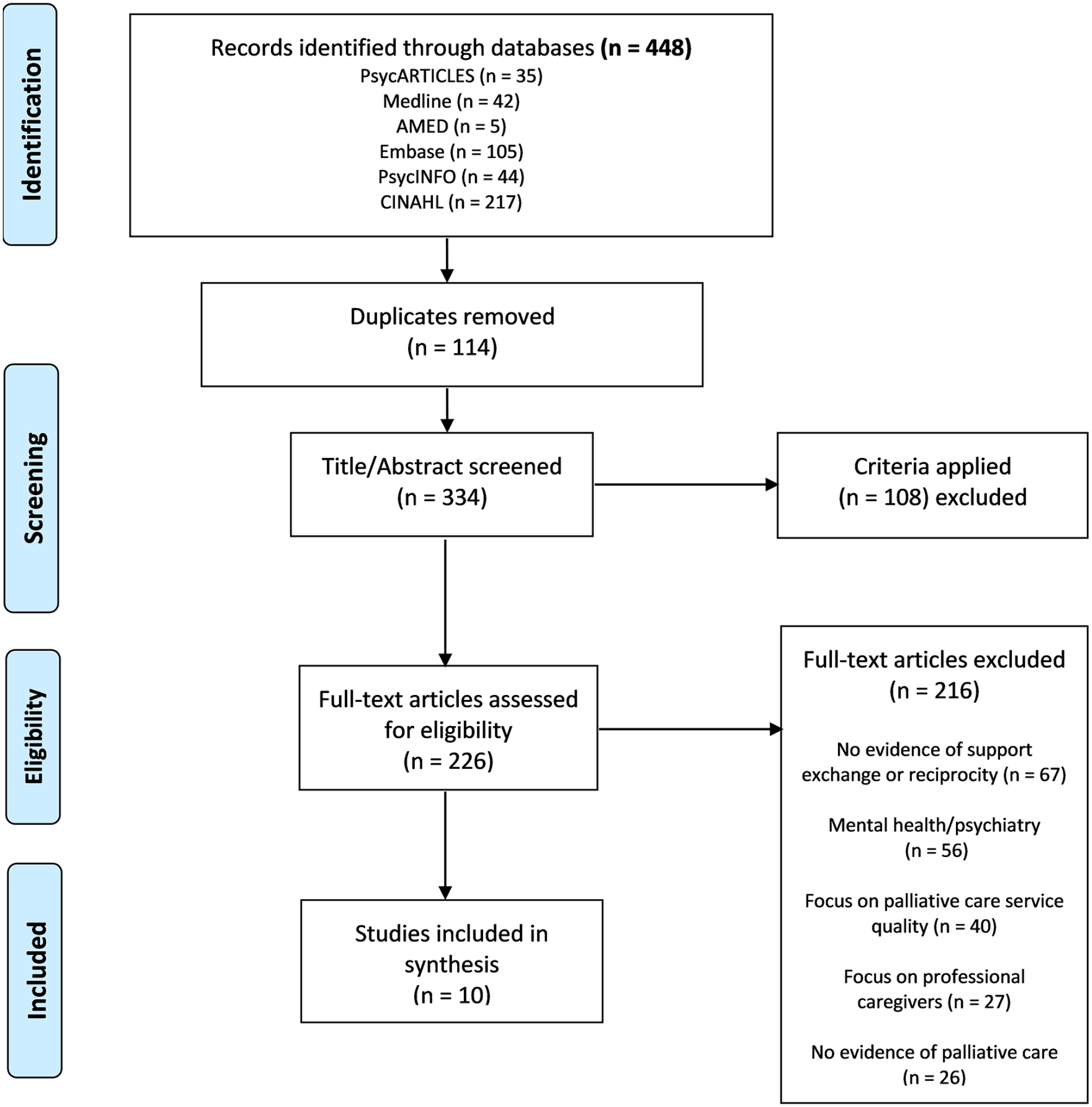
PRISMA flow diagram.
Summary of studies.

Quality assessment
The quality of each selected study was assessed by using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers 32 tool. This tool allows for a systematic and replicable method of assessing the quality of studies from a variety of methodological designs. Studies are given a quality assessment score based on a 14-item checklist for quantitative studies and a 10-item checklist for qualitative studies. Quality rating scores range between 0 and 1.0 for each study. We used this tool because it allowed us to compare quality across selected studies. The quality of each included study was independently assessed by RMcC and GF and where scores differed, the central value was taken. The quality of studies 32 ranged from adequate to strong. Table 1 includes the quality metric for each included study.
Synthesis
We conducted a narrative synthesis of the selected studies.33,34 A narrative synthesis is commonly used to synthesise evidence from studies that are heterogenous in design and does not necessarily intend to transform data beyond the findings of the primary studies. 33 It adopts a textual approach to the process of synthesis to tell the story of findings from the included studies. 34 First, we looked exhaustively at the evidence in each study that captured and/or shaped processes of mutual support between patients and family caregivers, including factors that enabled or restricted mutual support between patients and family caregivers. We then collated and summarised the evidence from each study. 34 Next, we explored relationships in the data, by comparing the data both within and across the studies. 34 Looking iteratively for similarities and differences in the data both within and across studies helped us identify the evidence that more fully encapsulated key processes of mutual support and the factors that impacted on it. We then grouped findings into categories 34 which we felt best described key processes of mutual support and/or key factors that shaped mutual support. Both the grouping of findings into categories and the labelling of the categories were decided upon by mutual agreement between authors.
Findings
Ten studies22–31 met the inclusion criteria and were included in the synthesis. The studies extracted varied in scope, design and in their aims (see Table 1). Of the studies included, seven were qualitative22,24,25,27–29,31 and three were quantitative23,26,30 (including one randomised-controlled trial, 30 one longitudinal-cohort study 23 and a cross-sectional cohort study 26 ). The studies were conducted in the UK,22,29 Canada, 26 Denmark, 30 Sweden, 27 Colombia, 28 and the United States.23–25,31 All studies sampled participants through healthcare settings including a hospital oncology department, 30 a neurology outpatient clinic, 22 an oncology outpatient clinic, 26 specialist cancer centres,24,25,29 a hospital palliative care unit 28 and a hospice. 31 Family caregiver participants were caregivers of cancer patients only in all studies except one 31 which included caregivers of both cancer and non-cancer patients. None of the studies found reported exclusively on mutual support between patients and family caregivers in palliative care and only one study 25 aimed from the outset to investigate processes of support and care between patients and family caregivers. Across 9 of the 10 studies that included carer participants in the sample, family caregivers were reported as spouses,24–26 partners of a couple, 23 a mixture of family members and friends,28,29 a mixture of partners (of a couple) and adult children27,30 and as non-familial related caregivers. 31
Constructing a shared view
A common way in which patients and family caregivers supported one another was through mutual acknowledgement and understanding of the challenges they both faced.22,24,25,28,31 Shared acknowledgement and understanding was important when patients and family caregivers received new information about the patient’s trajectory and/or when the patient’s physical condition had changed. 31 Indeed, mutual understanding of the situation at hand enabled patients and family caregivers to communally appraise treatment options and make decisions about care in a timely manner.24,28 Consensus among patients and family caregivers in the decision-making process was a feature of positive dyadic coping between patients and family caregivers.23,29,30 However, consensus also featured (inversely) in the context of mutual avoidance.23,30
Shared positivity
Mutual acknowledgement and understanding was in most cases underpinned by patients’ and family caregivers’ efforts to foster optimism for each other.23–25,30 Shared positivity was perceived as being mutually beneficial because it enabled both patients and family caregivers to maintain hope for the future. 25 Remaining positive for each other was also framed by acknowledgement of past positive experiences they had shared and were grateful for. 25 Indeed, remaining positive as a unit assisted patients and caregivers to adjust to changing circumstances24,25 and adjusting well together was in some cases, a latent dimension to how patients and family caregivers supported each other.23,25,29
Shared positivity was a feature of positive dyadic coping and was generally associated with both better dyadic adjustment and less illness related distress for both patients and family caregivers. 23 However, due to the perceived importance patients place on a shared positive outlook, caregivers sometimes felt it necessary to remain visibly optimistic for patients even in the face of significant concerns. 25 In addition, caregivers’ compartmentalisation of negative emotions and their positive emotional support of the patient could result in emotional burnout in caregivers. 31
Importantly, the wider family encouragement of patient and family caregiver shared positivity helped patients and family caregivers sustain their positive support and encouragement of one another.26,28 Increased support from members of the wider family alleviated caregiver distress and the degree to which patients perceived themselves a burden on the family caregiver.26,28 The presence of other family member support allowed for greater emotional engagement between patients and their family caregivers. 26 By contrast, in situations where support from the wider family was reported as absent, family caregivers reported feeling alone and difficulty in remaining positive for the patient. 31
Shared distress
Both patients and family caregivers reported distress during the course of illness.22,24–26,29–31 Family caregivers’ observation of the patient in physical and emotional distress caused significant emotional distress for family caregivers. 27 Emotional distress encountered by family caregivers had the capacity to escalate patients’ emotional distress22,24,30 and stressful situations encountered by both patients and family caregivers was perceived to increase distress for each other. 30 Overall, patients and family caregivers were interdependent for perceived emotional distress.
Escalation of distress for patients and family caregivers was associated with common negative dyadic coping29,30 and poor adjustment to different and/or new roles.24,25,30,31 For example, distress for both patients and family caregivers arose from their concerns about financial matters or change in roles, with some family caregivers having to cease or limit their professional roles because of caregiving duties, with some being forced to prepare for the financial burden arising from providing care and anticipated funeral expenses.22,24,29 Perceived distress about the future was also shared because of mutual concern about how each other would cope with further deterioration in the patient’s health. 22 Of note, shared distress in the absence of close relatedness resulted in an escalation of negative feelings towards each other. 30
Some patients and family caregivers sought to conceal their concerns for the benefit of each other.22,24,25 Non-disclosure by family caregivers was perceived effective by family caregivers to help the patient maintain a positive outlook for the future. 25 However, reluctance to disclose feelings of distress to one another could result in both patients and family caregivers internalising their distress.24,25 Internalisation of distress by patients and family caregivers could then undermine mutual support and increase tension between patients and family caregivers. 24 In some cases, patients reported frustration and an increase in conflict between them and their family caregiver if patients perceived that their family caregiver avoided communicating their distress to them or did not reciprocate in disclosure of distress. 24
Negotiating new roles
Both patients and family caregivers acknowledged the challenge of adapting to their new and/or altered roles – as a care recipient or caregiver.24,25,29,31 Adjusting to the responsibility for the care and pain management of the patient was particularly challenging for some family caregivers27,28 and they struggled when their efforts did not alleviate the patient’s suffering. 29 For both patients and family caregivers, the process of adapting to new roles included accepting the need to relinquish previously held professional roles24,29 and negotiate the conflict arising from changing roles with their partner.25,31 Both patients and family caregivers reported change in the balance of power and control between them.24,25,30,31 Perceived change in balance of power was associated with role reversal, for example, in cases where those who were previously dependent on the other became the caregiver.24,25,30 However, reciprocal support between patients and family caregivers was also expressed even when patients and caregivers had exchanged dependent roles. 31
Some family caregivers indicated that adapting to their new role as a family caregiver was hindered by a lack of social relatedness 26 or support from the wider family. 31 Insufficient support from other members of the family as perceived by family caregivers, frustrated family caregivers particularly in situations where support from the wider family was perceived as tokenistic by the family caregiver and was limited primarily to when death of the patient was imminent. 31 Feeling unsupported by other family members made family caregivers feel isolated and/or lacking in self-efficacy in their role as a family caregiver.27,29,31
Discrepancy in mutual support
Discrepancies existed among patients and family caregivers in terms of supporting one another. Family caregivers were less likely to communicate their distress to patients compared to how often patients communicated their distress to them. 23 Some patients rated their family caregivers more positively than the family caregivers rated them (the patient) in terms of ability to give support. 23 Some family caregivers viewed their needs as secondary to those of their family member whom they cared for 24 and sacrificed their own interests in the process of caring.22,27 Family caregivers strove to conceal their concerns from patients to remain ‘strong’ for patients 29 even though they revealed their concerns to healthcare professionals and other members of the family.24,25 Patients also valued their family caregiver’s wellbeing over their own and they concealed their physical symptoms in their effort to alleviate family caregiver burden. 22
Patients’ and family caregivers’ ability to support one another was also shaped by how patients and family caregivers reciprocated or did not reciprocate in their spiritual support of one another.25,31 A shared emphasis on spirituality was a dimension to enabling patients and family caregivers to support one another. 31 Conversely, differences or conflict between patients and family caregivers on the relevance of spirituality meant that offers of spiritual support by one to the other were judged ineffective. 25
Discussion
This review aimed to identify processes of mutual support between patients and family caregivers in palliative care and to describe factors that can contribute to or obstruct mutual support between patients and family caregivers in palliative care. As stated, none of the studies found reported solely on mutual support between patients and family caregivers and only one study 25 had aimed to explore processes of mutual support between patients and family caregivers. Nearly all studies were conducted in developed western countries which could affect verbal expressions of mutuality and expression of support, or indeed propensity to engage in research focused on relationships and family support. Overall, the literature reviewed suggests that patients and family caregivers can support one another by mutually acknowledging the challenges they face, by fostering optimism for one another, and by negotiating together the change in their roles. However, in order to minimise causing distress for each other, patients and family caregivers may not routinely communicate their distress to each other or reciprocate in disclosure of distress. A lack of mutual disclosure can result in conflict between patients and family caregivers. Distress for both patients and family caregivers can arise in part, from the challenges associated with changing roles. Family caregiver distress can escalate if they feel unsupported by other members of the family.
Findings identified in this review resonate with the wider literature, including literature beyond palliative care. A study on distress and quality of life in patient and caregiver dyads facing stem cell transplant in cancer, 35 also found distress among caregivers and patients to be interdependent and that patients’ physical wellbeing accounted significantly for caregiver wellbeing. Correlation of symptoms between stroke survivors and their family caregivers has also shown that family caregivers experience increased emotional distress caring for their family member when they perceive their family member becoming more severely affected by their illness. 36 In stroke survivorship, family caregiver optimism also has capacity to alleviate patient distress. 37
The importance of mutual understanding between patients and family caregivers has been reported elsewhere (e.g. inflammatory arthritis, multiple sclerosis), where jointly negotiating the effects of illness was also a prerequisite for dealing with the impact of the condition on both patients and family caregivers.38,39 Findings pertaining to conflict between patients and their family caregivers in our review has been reported among groups not typically associated with palliative care.37,40–42 For example, distress for patients with overactive bladder syndrome and their family caregivers, can also lead to a lack of communication and limit mutual understanding between patients and family caregivers. 40 The emotional and physical burden of mental illness have also resulted in feelings of conflict and ambivalence between patients and their family caregivers. 41 Conflict among dyads in spinal cord injury can also arise because of difficulty negotiating new roles. 42
The findings of our review point to how patient and family caregiver support of one another in palliative care can be mediated by the wider family. Support from other family members can have a positive effect on both patients and family caregivers but a lack of support from other family members can be particularly stressful for family caregivers and make it more challenging for them in their caregiving role. These findings are consistent with palliative care literature.43,44 Understanding the processes of mutual support between patients and family caregivers in palliative care also needs attention to the wider social contexts of patients’ and family caregivers’ experiences in palliative care and how these contexts impact on how patients and family caregivers reciprocate in their support of one another. Support exchange between patients and family caregivers in palliative care is also mediated by contexts beyond the dyad that shape patients’ and family caregivers’ capacity to support each other.
Strengths and limitations
This review was limited to original peer-reviewed journal publications and excluded all grey literature. Although a search through grey literature might have identified additional evidence for this review, limiting our review to the above allowed us to assess objectively the methodological quality of each piece of evidence that we included. A wider ‘scoping’ review pertaining to mutual support between patients and family caregivers in palliative care would broaden further our understanding of this phenomenon.
Another limitation of this review is that we limited our inclusion to studies reporting on patients with clearly advancing conditions likely to result in their death. Palliative care can serve the needs of people with life-limiting or life-threatening illness at different stages of non-curable conditions. A systematic review of the evidence in palliative care along the full illness trajectory would serve to expand on our review findings. Due to the small number of studies which addressed this topic, in addition to studies that sampled both the patient and family caregiver, we included studies that sampled only patients or only family caregivers once the data generated pertained to mutual support or reciprocity between patients and family caregivers. Therefore, it is possible that in these studies, the evidence reflects only what patients or only what family caregivers perceived as mutual or reciprocal. Finally, we limited our review to a 20-year period. A review from inception to the end period could have extracted other studies that met other inclusion criteria.
What this review adds to existing knowledge
The findings of the review highlight the complex nature of relations between patients and family caregivers in palliative care. Shared understanding and positivity can enable patients and family caregivers adjust to progressive illness and engage effectively in the decision-making process. However, patients and family caregivers also experience distress and do not routinely communicate their concerns to each other. In some cases, disclosure can be more challenging for family caregivers. In practice, attention should focus not only on alleviating distress for patients and family caregivers but also on how patients and family caregivers can best communicate their distress to each other. Facilitating patients and family caregivers in this context has potential not only to alleviate distress for both patients and family caregivers but also to increase concordance between patients and family caregivers in the decision-making process.
Conclusions
The studies extracted in our review varied in scope and design. The small number of studies found to answer the review questions combined with broadly very different aims across studies makes it difficult to fully extrapolate findings of the review. Nonetheless, the findings from this review have some key implications for research and practice.
As stated, we found that none of the studies extracted reported exclusively on mutual support between patients and family caregivers in palliative care and that only one study had aimed from the outset to investigate processes of support and care between patients and family caregivers. A limited focus on mutual support between patients and family caregivers could in part be a consequence of how we traditionally conceptualise in research and practice the roles of patients and family caregivers in palliative care. Although patients and family in palliative care are treated by healthcare professionals and researchers as a ‘unit’ of care,45,46 more-often-than-not, patients in palliative care are defined as recipients of care from family caregivers, and family caregivers are defined as providers of support to patients. Research in palliative care that is sensitive to the bidirectional nature of support between patients and family caregivers and to the wider caring and family roles that patients and family caregivers can have in relation to each other, is needed to advance our understanding of mutual support between patients and family caregivers in palliative care.
Literature pertaining to mutual support between patients with advancing non-curable illness and their family caregivers in palliative care has reported primarily from people with cancer and/or their family caregivers. However, palliative care is not limited to people who live with cancer and multiple other diagnostic groupings (e.g. neurodegenerative disease, chronic heart failure and chronic obstructive lung disease) access palliative care services. Studies pertaining to mutual support between patients with advanced illness and family caregivers in palliative care that extends to other conditions would be beneficial to expand on what we now know about mutual support between cancer patients and family caregivers in palliative care.
The findings suggest that support from the wider family can allow for greater emotional engagement between patients and family caregivers in palliative care and alleviate distress for family caregivers. However, family caregivers’ perceived lack of support from other members of the family can make it more difficult for family caregivers to adjust to the demands of caregiving. Research to identify how the wider family can best support the patient and family caregiver in palliative care and alleviate distress for the family caregiver could be beneficial. Indeed, attention to wider socio-cultural contexts in palliative care is always necessary. Socio-cultural contexts (e.g. life-course trajectories, social inclusion) do shape the experience of death and dying, 47 which in turn can impact on mutuality between patients and family caregivers in palliative care.
Further research is required to identify key domains of mutual support between patients and family caregivers in palliative care. Understanding better what actions or interactions constitute mutual support between patients and family caregivers and the conditions that impact positively or negatively on patients’ and family caregivers’ abilities to support one another, can help guide interventions in palliative care focused on enabling supportive relations between patients and family caregivers.
Supplemental Material
sj-docx-1-pmj-10.1177_0269216321999962 – Supplemental material for Mutual support between patients and family caregivers in palliative care: A systematic review and narrative synthesis
Supplemental material, sj-docx-1-pmj-10.1177_0269216321999962 for Mutual support between patients and family caregivers in palliative care: A systematic review and narrative synthesis by Rachel McCauley, Regina McQuillan, Karen Ryan and Geraldine Foley in Palliative Medicine
Footnotes
Author contributions
G.F. conceived the study and supervised the work. G.F. and R.McC. designed the research strategy and screened studies. R.McC. extracted and synthesised the evidence. G.F. contributed to the synthesis. R.McC. wrote the manuscript and G.F. contributed to writing in all sections of the manuscript. R.McQ. and K.R. commented on the design and research strategy. G.F., R.McQ. and K.R. critically reviewed drafts for intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was supported by a Trinity College Dublin Provost’s Project Award obtained by G.F. (primary investigator) which funds PhD Scholarship for R.McC. St. Francis Hospice Dublin supported Open Access of this publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.