
Abstract
Background:
Family caregivers of persons with dementia often feel unprepared for end-of-life and preparedness predicts caregiver outcomes in bereavement. Existing questionnaires assessing preparedness have limitations. A multi-dimensional questionnaire assessing family caregiver preparedness for the end-of-life of persons with dementia is needed to identify caregivers at risk for negative outcomes in bereavement and evaluate the quality of strategies within a palliative approach.
Aim:
To develop a multi-dimensional questionnaire titled ‘Caring Ahead’ to assess feelings of preparedness for end-of-life in family caregivers of persons with dementia.
Design:
A mixed methods, sequential design employed semi-structured interviews, a Delphi-survey and pilot-testing of the questionnaire, June 2018 to July 2019.
Setting/population:
Participants included five current and 16 bereaved family caregivers of persons with symptoms advanced dementia from long-term care homes in Ontario, Canada; and 12 professional experts from clinical and academic settings in Canada, Europe, United States.
Results:
Interviews generated three core concepts and 114 indicators of preparedness sampling cognitive, affective and behavioural traits in four domains (i.e., medical, psychosocial, spiritual, practical). Indicators were translated and reduced to a pool of 73 potential questionnaire items. 30-items were selected to create the ‘Caring Ahead’ preparedness questionnaire through a Delphi-survey. Items were revised through a pilot-test with cognitive interviewing.
Conclusions:
Family caregivers’ feelings of preparedness for end-of-life need to be assessed and the quality of strategies within a palliative approach evaluated. Future psychometric testing of the Caring Ahead questionnaire will evaluate evidence for validity and reliability.
Keywords
Family caregiving for persons with dementia is associated with negative outcomes in bereavement.
Negative outcomes are predicted by family caregivers’ preparedness for end-of-life.
Preparedness is modifiable through strategies supporting a palliative approach.
Existing questionnaires used to assess preparedness have limitations.
Core concepts of preparedness for end-of-life included managing the situation, fulfilling obligations and adapting to loss.
Indicators of preparedness included engaging in life review, reconciling with the person with dementia, knowing what the dying process may be like, communicating about goals and preferences with healthcare professionals and having affairs in order.
Further research is needed to evaluate psychometrics of the Caring Ahead questionnaire.
Healthcare professionals should assess preparedness to identify caregivers of persons with advanced dementia in need of support.
Researchers should design/evaluate interventions to address preparedness core concepts and indicators.
Introduction
Family caregivers of persons with dementia can experience unique challenges and barriers to accessing care that impact their well-being into bereavement.1–3 New dementia and palliative care frameworks aim to address inequities by promoting the early introduction of a palliative approach.4–7 Approximately half of deaths of persons with dementia occur in long-term care institutions making long-term care the ideal location to introduce a palliative approach.7,8
A palliative approach focuses on providing holistic care to promote quality-of-life and prepare persons with life-limiting illnesses and their families for end-of-life. 9 Guidelines for dementia care often negate aspects of care essential to a palliative approach such as end-of-life management, grief/loss and spiritual care.10,11 Up to 50% of family caregivers report feeling unprepared for end-of-life and death preparedness predicts well-being in bereavement.12–17 Caregiver death preparedness (i.e., readiness for death) can be modified through strategies supporting a palliative approach.13–17 However, outcome measures used to evaluate strategies within a palliative approach are often limited to the documentation of resuscitation status.11,18,19 Assessing preparedness rather, could provide a holistic, outcome measure to evaluate the effectiveness of strategies.
Caregiver death preparedness is a multi-dimensional, dynamic construct that has been defined as a ‘self-perceived cognitive, affective and behavioural quality or state to maintain self-efficacy and control in the face of loss and death’ (p. 4). 20 The Theoretical Framework of Preparedness for End-of-Life 21 and the Caregiver Preparedness for End-of-Life with Dementia model 20 describe preparedness as having medical, psychosocial, spiritual and practical domains with underlying cognitive, affective and behavioural traits (see Figure 1). Preparedness has been linked to end-of-life conversations, which supports the assessment of preparedness as a holistic outcome measure for strategies supporting a palliative approach.20–24
‘Caregiver preparedness for end-of-life with dementia’ model.
Despite the complexity of preparedness, the construct is often assessed with a single-item or a generic questionnaire such as the Preparedness for Caregiving Scale.25,26 This is problematic because single-items are unidimensional, require abstract-thinking and are occasion-specific.27–29 Generic questionnaires are also less responsive to detecting change over time than condition-specific questionnaires and do not assess specific content and concerns, which reduces face and content validity.26–30 In contrast, multi-item, condition-specific questionnaires investigate dimensionality, explore variance in core concepts and individual items and avoid occasion-specific effects.27–30 Hence, a multi-item, condition-specific questionnaire is needed to assess caregiver preparedness for end-of-life of persons with dementia and act as an outcome measure for strategies supporting a palliative approach.
Methods
Aims
In this study we aimed to develop a multi-dimensional questionnaire to assess caregiver preparedness for the end-of-life of persons with dementia.
Design
This sequential mixed methods study was guided by the Instrument Development and Construct Validation framework. 31 We used three phases (qualitative → QUANTITATIVE) to: (1) generate questionnaire items; (2) select questionnaire items and (3) evaluate questionnaire face validity and response process (Figure 2). The protocol was approved by the Hamilton Integrated Research Ethics Board (#4503).
Mixed methods design: exploratory, sequential quantitative dominant status, instrument-variant design (qualitative → QUANTITATIVE).
Phase 1
Design
A qualitative, interpretive descriptive approach was first used to explore core concepts of preparedness beyond the surface, identify behavioural indicators and generate questionnaire items in summer, 2018.31–35
Population/setting
Purposive and maximum variation sampling were used to recruit 16 bereaved caregivers for interviews from six long-term care homes in Ontario, Canada. 32 To minimise researcher intrusion and participant distress, participants were recruited with the aid of partners (e.g., long-term care Director) who acted as gatekeepers and asked participants for permission to share their contact information with us.36,37 Participants were English-speaking, primarily female (57%), bereaved (10 months on average), adult-child caregivers (70%) who had cared for a person with dementia living in long-term care. Participants described persons with dementia as having symptoms of late-stage dementia prior to death (e.g., difficulty swallowing, frequent infections, immobility, incontinence, limited verbalisation and facial recognition). 1
Data collection
A semi-structured interview guide with questions organised around preparedness domains (i.e., medical, psychosocial, spiritual, practical preparations) was used to conduct in-person or telephone interviews.20,21 Participants were asked to describe events, activities and feelings of preparedness which occurred during the last year of the person’s life. Informed, written consent was obtained and participants were provided with a list of supportive resources.35–37 Interviews were audio-recorded, transcribed and proofed.
Analysis
We followed Braun and Clarke’s (2014) process for reflexive thematic analysis. We used an iterative, inductive, data-driven approach to: (1) organise the data with surface-level codes; (2) identify behaviours perceived as facilitating and indicating caregiver preparedness during the year prior to death; (3) search for, define and agree upon overarching themes that represented core concepts of preparedness. 34 Authors independently analysed three transcripts and met together to agree upon codes and themes. PD then analysed the remaining transcripts extracting participant quotes as evidence and met frequently with the authors to ensure the findings were data-driven.34,35 We then translated the behavioural indicators and facilitators into potential questionnaire items sampling preparedness core concepts, domains, and traits based on participants’ direct-quotes.20,21,30–32
Phase 2
Design
A cross-sectional Delphi-survey was next completed to generate consensus and select/revise items for the questionnaire in winter, 2019.38,39
Population/setting
Purposive, convenience and maximum variation sampling was used to recruit seventeen panelists (including five caregivers and 12 professional experts) via email to participate in the Delphi-survey. Caregiver panelists included participants from Phase 1 who had requested further participation and volunteers within the Alzheimer Society or Canadian Frailty Network known to the authors (response rate 63%). Professional expert panelists were reputable academics or clinicians in the field of dementia, caregiving and palliative care contacted via publicly available emails (response rate 55%). 30 A sample of 15–20 participants has been described as adequate for a Delphi-survey and no panelist attrition occurred between rounds.38,39 Caregiver panelists were English-speaking, 59 years old on average, 60% were female, 80% were adult-children of a person with dementia, and 60% were bereaved. Expert panelists had an average of 20 years of experience (see Table 1).
Phase 2 Delphi-survey panelists.
Data collection
The survey was piloted with one caregiver, one expert nurse researcher and two graduate students.38,39 We used LimeSurvey, a secure online survey platform to administer the survey with implied consent. 40 In Round 1, panelists rated the importance of items using a 7-point Likert scale with anchors (1 = Strongly Disagree, 7 = Strongly Agree) and suggested changes to item wording.38,39 In Round 2, panelists were provided with the item Content Validation Index (CVI), of each panel’s (i.e., expert and caregiver) median scores and the original wording of revised items. Panelists then provided a dichotomous rating (rate 0/1) to ‘accept or reject’ items selected based on consensus in Round 1 and re-rated items (from 1 to 7) that had met partial criteria for consensus. The survey was stopped after Round 2 when the item pool was reduced.30,38,39
Analysis
Criteria for item selection consensus was defined as: CVI ⩾ 0.8 and a median score of ⩾6 from both panels. Consensus from both panels equally values perspectives and using multiple selection criteria efficiently reduces items.38,39 Content analysis of panelist comments guided item revision and exclusion. 31 Upon completion of the Delphi-survey, a draft questionnaire comprised of the selected items was compared to a Content Validation Matrix to ensure that the questionnaire adequately sampled three core concepts, four domains and four traits of preparedness.20,21,30,31,38
Phase 3
Design
A cross-sectional pilot-test and cognitive interview with the developed questionnaire was conducted to explore face validity and response process in spring, 2019.30,31,41,42
Population/setting
Purposive and criterion sampling and advertising flyers were used to recruit three current caregivers from three long-term care homes in Ontario. 30 Participants were female, between 35 and 68 years old and included one spouse and two adult-children. Persons with dementia were living in long-term care and were described as having symptoms of advanced dementia. 1
Data collection and analysis
Participants provided informed, written consent for the in-person questionnaire pilot-test and cognitive interview. Cognitive interviewing is a process whereby participants: complete a questionnaire with an interviewer; explain their interpretation of questions (i.e., response process) by ‘thinking-aloud’ and make suggestions to increase items’ face validity.30,31,41,42 A semi-structured interview guide with questions such as, ‘what does this statement mean to you?’ was followed and field notes were recorded to document participants’ interpretations and suggestions. Field notes were analysed through content analysis to categorise and compare recommendations. 41
Results
Phase 1 Findings
Three core concepts of preparedness emerged from interviews with bereaved caregiver participants including: (1) managing the situation to meet the needs of the person with dementia, (2) fulfilling obligations to meet the moral and legal needs of society and (3) adapting to loss to meet the emotional needs of the caregiver. One hundred and fourteen behaviours perceived as indicating and facilitating preparedness such as planning, organising, knowing, coping and accepting were identified and translated into a pool of questionnaire items sampling perceived core concepts, domains and traits of preparedness.20,21 Through discussions with one caregiver and one expert (nurse researcher in dementia/caregiving) the pool of items was subsequently reduced to 73 for the Delphi-survey (see Table 2). The ‘psychosocial’ domain label was replaced with ‘relationships and personal’ to reduce jargon. 30 Items were organised according to one primary domain to reduce respondents’ cognitive workload and less sensitive items were positioned at the beginning of the questionnaire to minimise potential distress during the next phase.30,42
Phase 1 findings: Preparedness indicators, quotes and potential questionnaire items (n = 73) sampling preparedness domains, traits and core concepts.
Preparedness traits. Beh: behaviour; Aff: affective; Cog: cognitive; core concepts; Control: managing the situation, maintaining a sense of control; Oblig: fulfilling obligations; Adapt: adapting to loss.
Indicators were translated into a pool of potential questionnaire items three based on participant’s direct quotes and aimed to adequately sample the perceived three core concepts, three underlying traits and four domains of preparedness.
Phase 2 Findings
Twenty-four questionnaire items met selection criteria in the Delphi-survey. A Content Validation Matrix of the 24-items revealed conceptual gaps, therefore the authors retained an additional six items which met partial criteria from the item pool.30,31 Hence, a thirty-item questionnaire was developed as a result of the Delphi-survey (see Figure 3 for item flow). Caregiver panelists requested pertinent examples be included with items (e.g., aware of changes to expect such as problems with swallowing). In contrast, expert panelists recommended the deletion of examples from items to avoid causing distress (e.g., pneumonia, moving houses) and the use of ‘softer’ language (e.g., ‘I am confident’ changed to ‘I believe’ (see Supplemental File A).
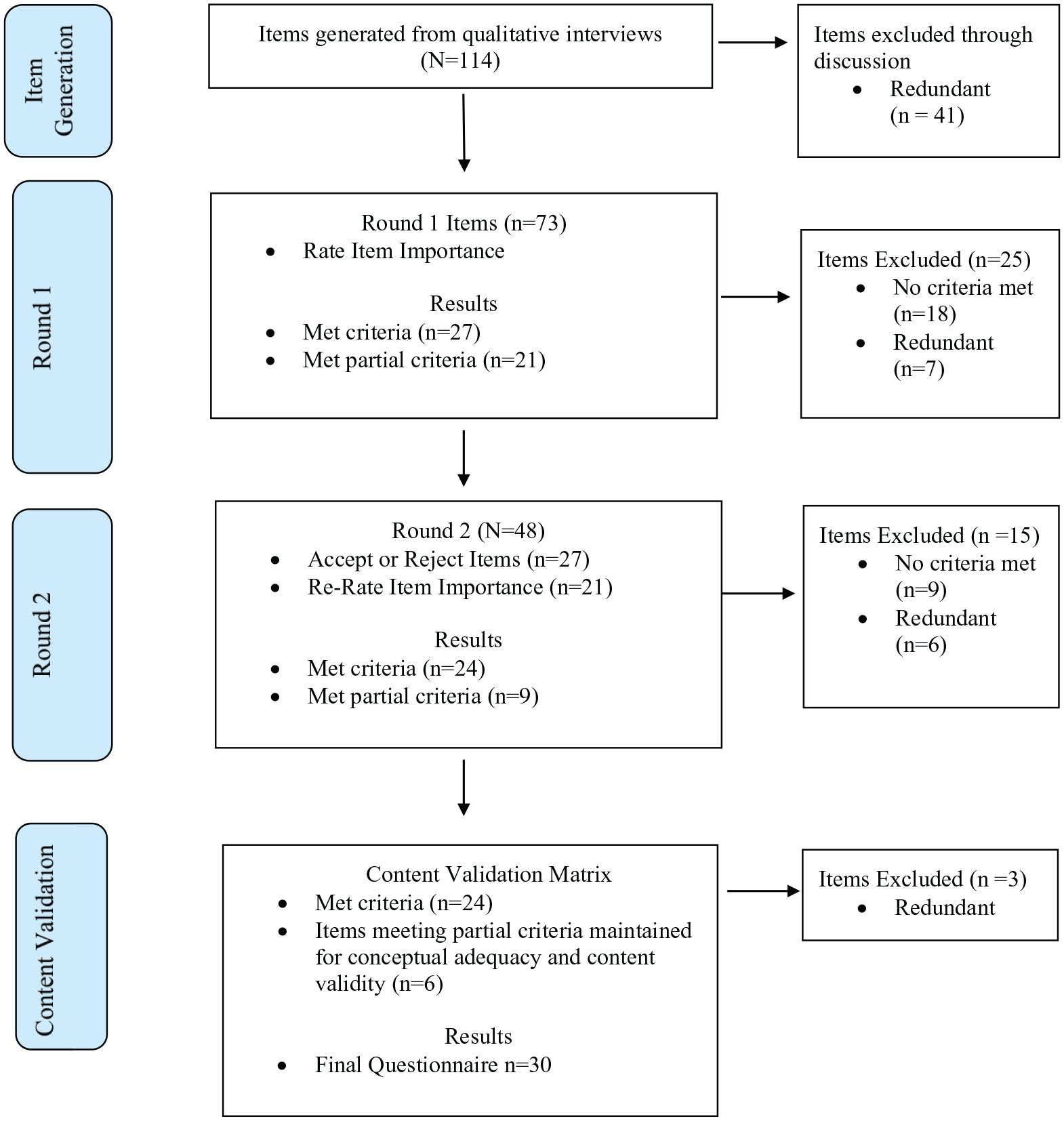
Phase 2 Delphi-survey item flow.
Phase 3 Findings
During the pilot-test, three current caregiver participants reported that the questionnaire content was acceptable (not distressing), relevant and applicable and the length was appropriate (not burdensome). Based on participants’ redundant response process and consistent recommendations ambiguous items were clarified (Question [Q]2, Q8, Q14, Q22, Q28), preferred language was incorporated (Q5, Q9) and inclusivity was enhanced (Q7, Q19). Specifically, participants recommended adding examples and using universal direct language to clarify items. The item ‘knowing what the dying process may be like’ was revised to clarify ‘for my family member with dementia’ (Q8). Examples were added to clarify changes to expect as dementia progresses such as ‘swallowing, eating difficulties’ (Q2).
In terms of language, the words ‘wishes’ was preferred over the word ‘goals’ (Q5) and the words ‘has died’ perceived as more appropriate and direct than the words ‘is gone’ (Q9). Participants explained that many persons with dementia were cognitively unaware or ‘gone’ for years before death, making this an inappropriate euphemism. Participants did not all identify with the examples of traditions so ‘personal traditions’ was added (Q19), and lastly the reference to ‘my family’ was revised to ‘important people in my family member’s life’ (Q7) to be more inclusive (see Table 3 for final revised questionnaire items).
Phase 3 findings: final questionnaire items (n = 30).
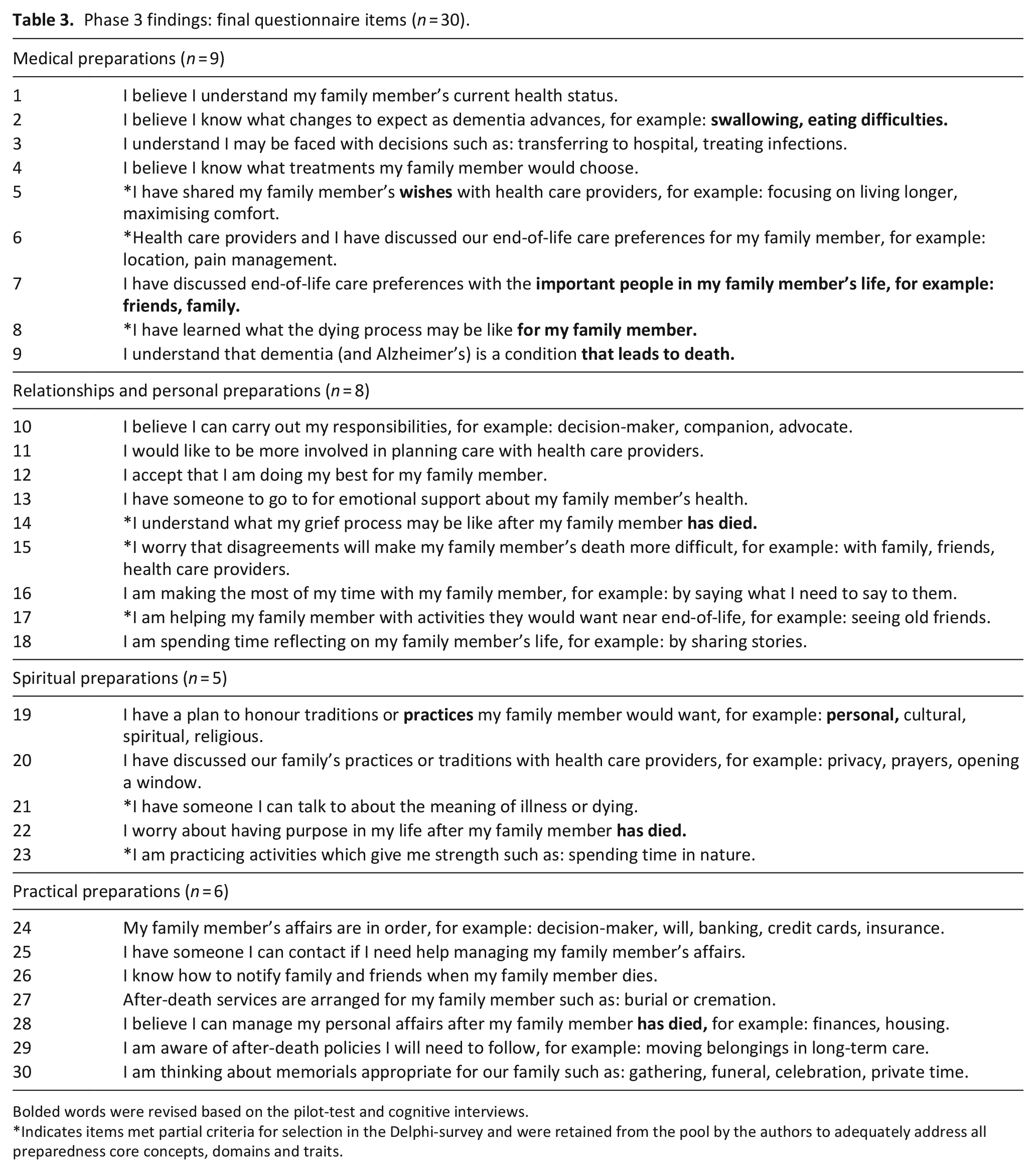
Bolded words were revised based on the pilot-test and cognitive interviews.
Indicates items met partial criteria for selection in the Delphi-survey and were retained from the pool by the authors to adequately address all preparedness core concepts, domains and traits.
Discussion
Main findings
The purpose of this mixed methods study was to develop a multi-dimensional, condition-specific questionnaire to assess preparedness for end-of-life in family caregivers of persons with dementia. Core concepts and indicators of preparedness were identified and items selected, revised and piloted through three study phases to develop the ‘Caring Ahead’ questionnaire. The final questionnaire included 30-items translated from preparedness indicators and participant quotes. Questionnaire items are organised in four domains: medical, relationships/personal, spiritual and practical; aim to sample three core concepts: managing the situation, fulfilling obligations and adapting to loss; and three traits of preparedness: cognitive, affective and behavioural.
Limitations
Study limitations included the small sample size in the Delphi-survey compared to other Delphi-studies which have reported sample sizes over 50. 44 The Delphi-survey response rate (57%) was also lower than the recommended 70% and could result in response bias and instability.30,38,39 However, response stability has been demonstrated in Delphi-surveys with approximately 20 respondents, and mental health studies often have smaller sample sizes with adequate stability reported.38,39 The sample small of caregivers (n=3) recruited to pilot-test the questionnaire in Phase 3 of this study was less than the suggested sample size of five participants for cognitive interviewing and questionnaire development studies and is therefore a limitation. 41 However, demographic variability amongst the participants and redundancy in item responses were demonstrated, which suggests reliability in the questionnaire item response process.30,31,35 Future studies will evaluate questionnaire psychometrics with 200 caregivers to align with sample sizes in the majority of instrument development studies. 45
Study participants were primarily female and white, which may influence the transferability of the questionnaire to caregivers of other genders, cultures/races. Similar sample demographics have been reported in other instrument development studies including the Caregiver Grief Scale 46 and the Carer Support Needs Assessment Tool 47 which suggests this is a common phenomenon. Targeted recruitment of diverse participants in future studies is needed to explore transferability, sex and gender-based analysis. 48 Lastly, persons with dementia were living in long-term care and were described by participants as having symptoms of advanced dementia. Therefore, further research is needed to explore the transferability (i.e., acceptability, content and face validity) of the questionnaire for caregivers of persons with early stages of dementia or outside of long-term care.
What this study adds
New insight into indicators and core concepts of preparedness was gleaned through this study that helped to produce the Caring Ahead questionnaire with current evidence for face and content validity. These findings should assist healthcare professionals and researchers to assess caregivers’ feelings of preparedness, identify caregivers in need of support, design and evaluate strategies aligned with a palliative approach. However, future research is needed to evaluate questionnaire psychometrics (i.e., content, construct, predictive validity and reliability) in a larger sample and with different populations.
Unique preparedness indicators described by participants in this study such as: fulfilling rituals/traditions, facilitating life completion and reconciling with persons with dementia highlight the importance for healthcare professionals and researchers to explore all areas of preparedness and not focus narrowly on the medical domain. Preparedness indicators identified in this study also reflected problem and emotion-focused coping behaviours (e.g., learning/knowing, planning, organising) that have been previously reported as facilitating feelings of preparedness for death.49-51 Evidence exists for associations between coping behaviours such as emotional-support, acceptance, problem-focused coping included as indicators on the Caring Ahead questionnaire and positive mental health outcomes (e.g., reduced depression and anxiety). 52 Therefore, the Caring Ahead questionnaire may predict caregiver outcomes in bereavement.
Sensitive strategies to minimise intrusion and distress were used to recruit and retain participants in this study such as gatekeeping (i.e., person known to potential participants asks for permission to share contact information with researchers) and providing question examples for the interview/Delphi/pilot-test.36,37 Similar strategies should be employed by researchers and healthcare professionals administering the questionnaire in the future. The Serious Illness Conversation guide for example, recommends that healthcare professionals plan ahead for serious discussions and (1) assess the person’s level of knowledge; (2) ask for permission to discuss the future/serious illness and (3) ascertain information preferences. 53
Insight into the language preferences of caregivers and experts related to dying was also gained from this study. Euphemisms are defined as language substitutions, replacements or social safeguards to soften words that are considered taboo or harsh. 54 While, multiple experts in the Delphi-survey suggested items needed to be ‘softened’ or less harsh, caregivers perceived that euphemisms (e.g., is gone) impeded item clarity. Euphemisms have been reported as: obscuring the truth, contributing to miscommunications, paternalistic and used to avoid end-of-life discussions.54–57 Healthcare professionals’ use of clear language such as ‘imminent death’, ‘dying’ and ‘end of life’ is associated more often with a malignant diagnosis and with the involvement of palliative care providers. 55 Hence, caregivers of persons with dementia may be more at risk of experiencing miscommunications which reduce preparedness for death. Healthcare professionals and researchers should therefore communicate with universal terms such as ‘dying’ and ‘end-of-life’ in order to normalise and not obscure approaching death.
Conclusion
The 30-item ‘Caring Ahead’ questionnaire which aims to assess caregiver preparedness for death in dementia was developed in this study. This questionnaire aims to reflect the multi-dimensional nature of preparedness with items sampling underlying traits, domains and core concepts. Evaluation of the questionnaire with current caregivers of persons with dementia living in long-term care is currently underway. Once tested, this questionnaire can be used by healthcare professionals, researchers and policy-makers to identify family caregivers with limited areas of preparedness and as a holistic outcome measure for strategies supporting a palliative approach.
Supplemental Material
sj-pdf-1-pmj-10.1177_0269216321994732 – Supplemental material for Caring ahead: Mixed methods development of a questionnaire to measure caregiver preparedness for end-of-life with dementia
Supplemental material, sj-pdf-1-pmj-10.1177_0269216321994732 for Caring ahead: Mixed methods development of a questionnaire to measure caregiver preparedness for end-of-life with dementia by Pamela Durepos, Noori Akhtar-Danesh, Jenny Ploeg, Tamara Sussman and Sharon Kaasalainen in Palliative Medicine
Footnotes
Author contributions
Each author participated in the design, analysis and reporting of this study in all three phases.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are grateful for funding in the way of grants and scholarships including: Alzheimer Society of Canada Brant, Haldimand-Norfolk, Hamilton-Halton Branch; Canadian Frailty Network Interdisciplinary Fellowship 2018–2019; Canadian Institutes of Health Research 159269; Canadian Nurses Foundation; Registered Nurses Foundation of Ontario, Mental Health Interest Group.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.