
Abstract
Background:
Caring for family members of dying patients is a vital component of end-of-life care, yet family members’ needs at the end of life may be unmet.
Aim:
To explore hospital clinician assessment and facilitation of family needs and practices to support families at the end of life.
Design:
Descriptive study utilising a retrospective medical record audit.
Setting and Sample:
Undertaken in a large public hospital, the sample included 200 deceased patients from four specialities; general medicine (n = 50), intensive care (n = 50), inpatient palliative care (n = 50) and aged rehabilitation (n = 50). Data were analysed according to age; under 65-years and 65-years or over.
Results:
Deceased patients’ mean age was 75-years, 60% were Christian and Next-of-Kin were documented in 96% of cases. 79% spoke English, yet interpreters were used in only 6% of cases. Formal family meetings were held in 64% of cases. An assessment of family needs was undertaken in 52% of cases, and more likely for those under 65-years (p = 0.027). Cultural/religious practices were supported/facilitated in only 6% of all cases. Specialist palliative care involvement was more likely for those aged 65-years or over (p = 0.040) and social work involvement more likely for those under 65-years (p = 0.002). Pastoral care and bereavement support was low across the whole sample.
Conclusions:
Prioritising family needs should be core to end-of-life care. Anticipation of death should trigger routine referral to support personnel/services to ensure practice is guided by family needs. More research is needed to evaluate how family needs assessment can inform end-of-life care, supported by policy.
Keywords
Caring for family members of dying patients is a vital component of end-of-life care.
Family members of dying patients want respectful and compassionate care, to be supported in their distress, and to have their personal, cultural and religious needs respected.
Formal family meetings are used to reach treatment consensus, but may also be a missed opportunity to gather information about family support needs and preferences for end-of-life care.
Anticipation of death should be a trigger for assessment of family support needs, and routine referral/involvement of social work and pastoral care support services/personnel.
Assessing and honouring the cultural, bereavement and support needs of family members is essential.
Research is needed to measure and evaluate how assessment of family needs can inform clinical practice to better support families at the end of life, supported by policy.
Background
One of the main purposes of palliative care is to improve the quality-of-life for terminally ill patients and their families. 1 Whilst family members may understand a dying person’s prognosis, 2 family members are often not prepared for death,2,3 with inadequate information, emotional and bereavement support impacting family preparedness. 4 Family members of dying patients want expert, respectful and compassionate care, 5 anticipatory guidance 6 and to be supported in their distress. 7 When death is imminent, family members prefer to stay close to the dying person, 8 say goodbyes, 9 and to be supported in following their cultural rites and family traditions.10,11 Yet, significant variation in practice can exist. In acute and critical care settings where the biomedical model potentiates a focus on curative actions,12,13 acceptance that the patient is dying can be delayed 14 and assessment and facilitation of family needs overlooked. The aim of this study was to explore hospital clinician assessment and facilitation of family needs and practices to support families at the end of life.
Methods
Following ethical approval from the health service (RES-19-0000121L-51299, 12th March, 2019) and University (2019-117, 22nd March, 2019), a descriptive study utilising a retrospective medical record audit was undertaken between June and October, 2019. The study was conducted at a large tertiary public hospital in Melbourne, Australia, which serves a culturally diverse and rapidly ageing population. A sample of 200 adult inpatients who died in 2018 was used. The sample was stratified according to consecutive deaths across four inpatient specialities; general medicine (n = 50), intensive care unit (n = 50), inpatient palliative care (n = 50) and aged rehabilitation (n = 50). The purpose of selecting these different inpatient specialities was to provide a realistic representation of hospital inpatients, ensure heterogeneity in clinical practice factors, and to capture variations/differences in the provision of end-of-life care. All patients admitted to inpatient palliative care received care from a specialist palliative care physician and multidisciplinary palliative care team. For patients admitted under general medicine and aged rehabilitation, and into the intensive care unit, specialist palliative care involvement was by referral, and at the discretion of a member of the treating team.
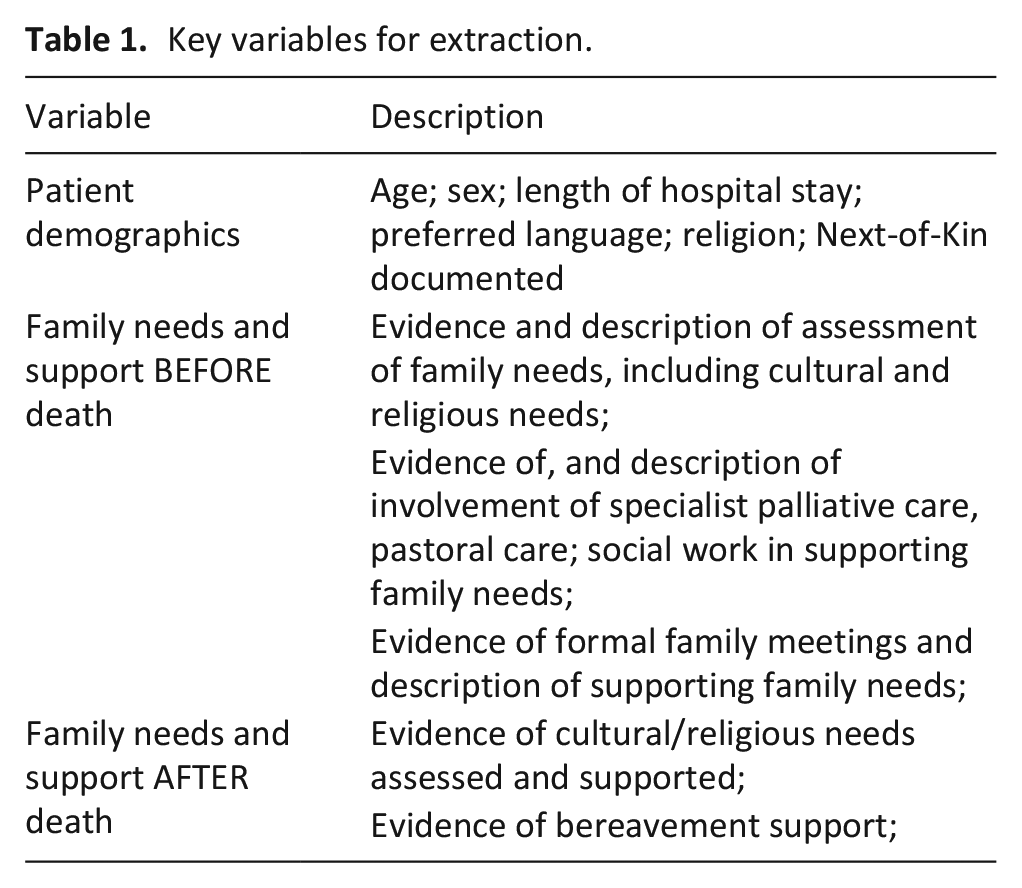
Patient demographic characteristics and key variables related to assessment and support of family needs before and after death were extracted from the medical record, including formal family meetings, involvement of specialist palliative care, pastoral care and social work, and descriptions of how family needs were supported, including facilitation of cultural and religious needs (Table 1).
Key variables for extraction.
Frequencies and percentages were calculated for categorical variables; continuous variables were summarised as means and standard deviations. Where data were not normally distributed, median and IQR are reported. Cross-tabulations and Chi-square statistics were calculated to explore differences between those aged under 65-years and 65-years and over. Two-tailed p ⩽ 0.05 was considered significant. For some variables, text data were collected from the medical records to further aid understanding. Text data were not analysed formally, but selected to depict the range or diversity of clinicians’ actions and responses.
Results
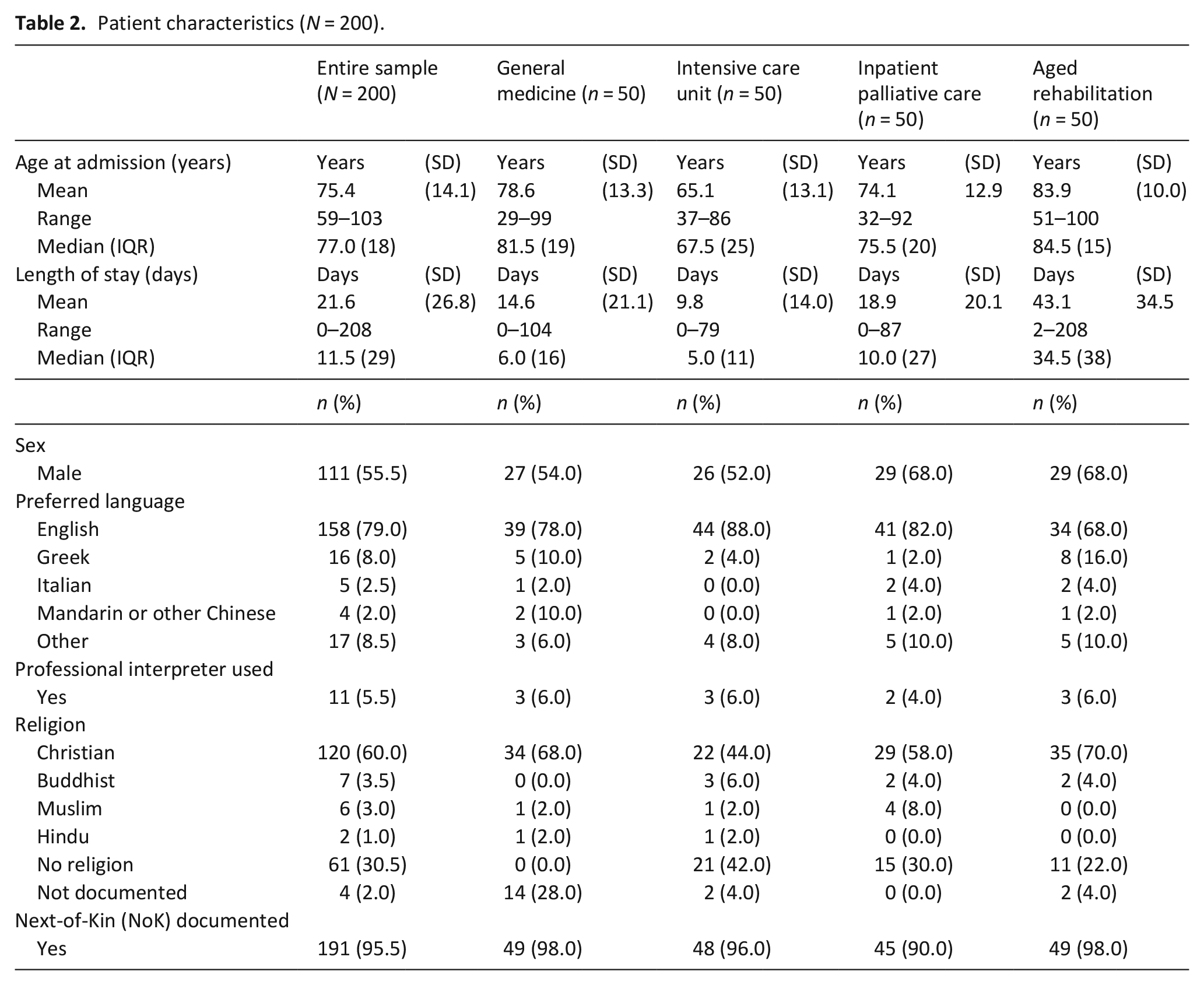
For the entire sample, deceased patients’ mean age was 75.4 (SD 14.1) years; just over half (55.5%, n = 111) were male, and 60.0% (n = 120) identified as Christian. 79.0% (n = 158) indicated English was their preferred language, yet a professional interpreter was used in only 5.5% (n = 11) of cases. In 95.5% of cases (n = 191) a person was listed as Next-of-Kin in the medical record (Table 2).
Patient characteristics (N = 200).
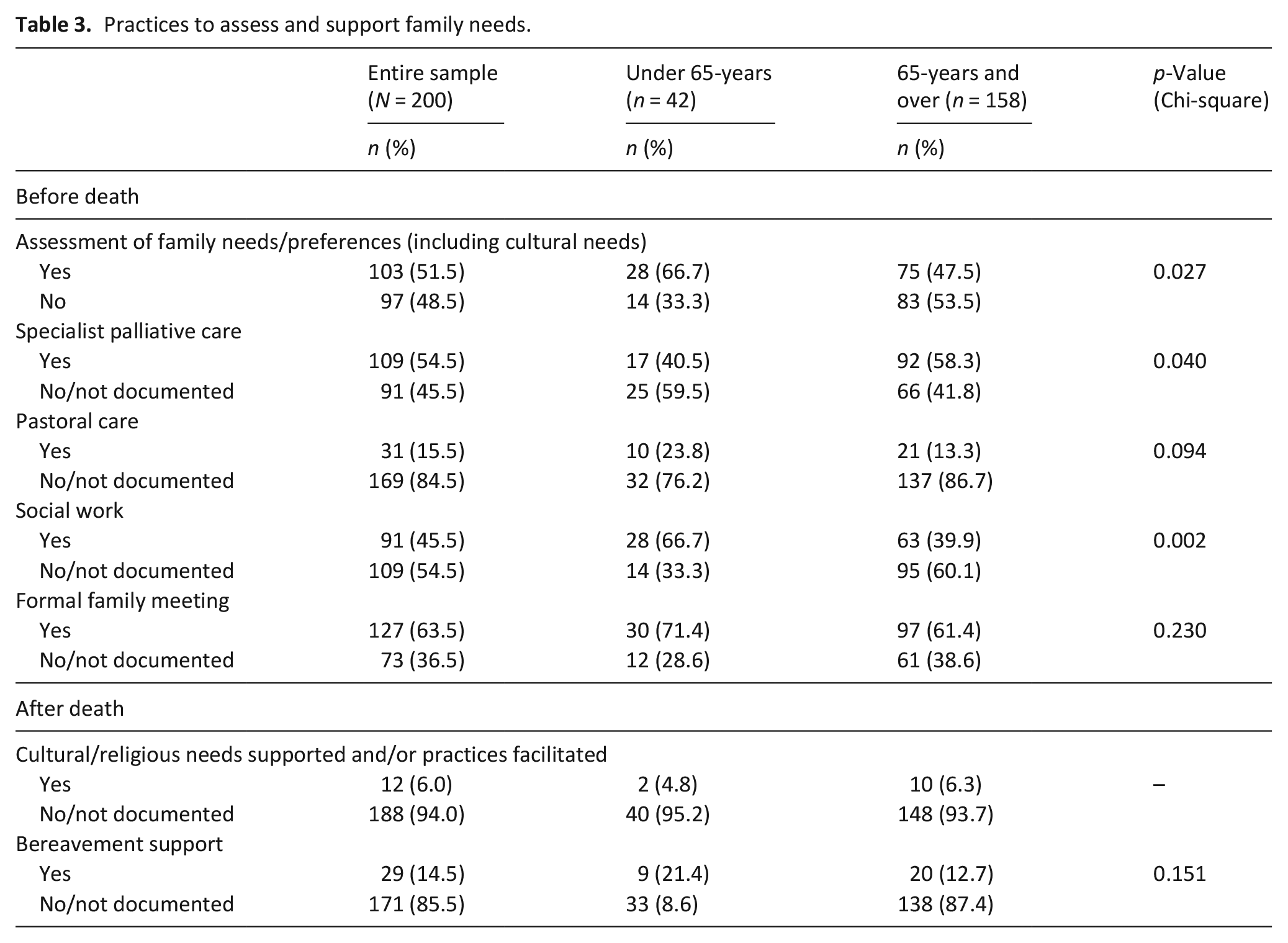
In 51.5% of all cases (n = 103), there was evidence of formal assessment of family needs and/or preferences (including cultural needs), before patient death. This was statistically more likely for those aged under 65-years (66.7%, n = 28, p = 0.027) (Table 3). Clinician written entries detailed cultural and religious needs and requests associated with patient death, such as: ‘the patient must be buried within 24 hours of death due to cultural needs’ (Case 3-22, Age 65-years, Inpatient Palliative Care Unit).
Practices to assess and support family needs.
In another, a clinician entry described family’s request for religious needs to be facilitated: ‘. . .requesting 1 hour post death for cultural practices, monk coming in daily for 1-hour chanting’ (Case 3-36, Age 85-years, Inpatient Palliative Care Unit).
Medical record entries also specified family post-mortem needs such as: ‘. . .specific Jewish needs, not to touch body after death’ (Case 4-43, aged 93-years, General Medicine unit)
Formal family meetings were held in 63.5% (n = 127) of all cases. Yet medical record entries suggested meetings focussed on reaching treatment consensus rather than assessing or supporting family needs: ‘Family initially resistive to EOLC [end-of-life care] wanting active Tx [treatment], however upon further discussion were accepting of EOLC [end-of-life care]’ (Case 3-27, Aged 82-years, Inpatient Palliative Care).
When comparing those aged under 65-years and those aged 65-years and over, specialist palliative care were involved in 54.5% (n = 109) of all cases, and this was statistically more likely for people aged 65-years and over (58.3%, n = 92 p = 0.040). Pastoral care were involved in 15.5% (n = 31) and more so for people under 65-years, although not statistically significant. Social work were involved in 45.5% (n = 91) of cases overall, and this was statistically more likely for those aged under 65-years (66.7%, n = 28, p = 0.002) (Table 3).
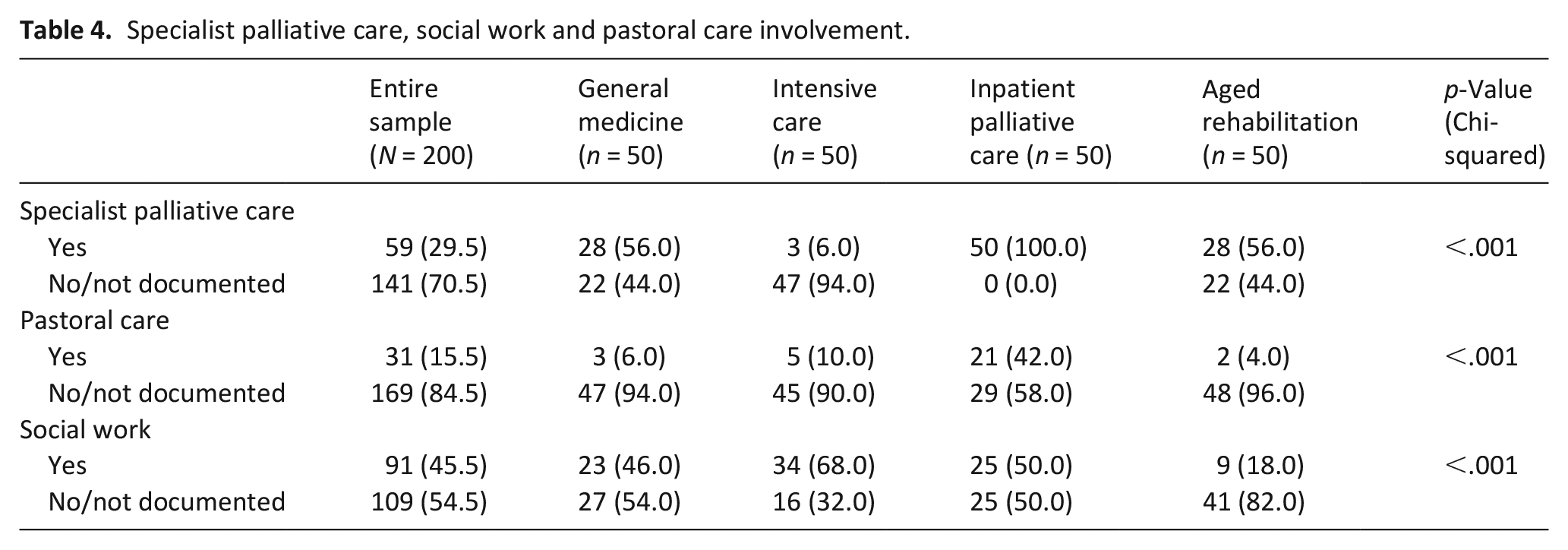
When comparing rates of specialist palliative care, social work and pastoral care involvement across inpatient specialities, patients in intensive care were statistically least likely to have specialist palliative care personnel involved in their care (p < 0.001). Pastoral care involvement was statistically more common for those admitted to inpatient palliative care (p < 0.001) (Table 4). Social work personnel involvement was most common for those admitted to intensive care (p < 0.001). For example, social workers in the intensive care assessed family needs: ‘. . .family requesting help with respecting pt [patient] wishes of a private funeral but also allowing extended family and friends to mourn. SW [Social Work] assisted’ (Case 2-23, Aged 85-years, Intensive Care Unit).
Specialist palliative care, social work and pastoral care involvement.
After death, bereavement support was offered by social work in 14.4% (n = 29) of cases (Table 3). Evidence of practices to support family cultural or religious needs after death were identified in only 6.0% (n = 12) of all cases, such as attendance by a religious leader, or documenting when family requests were observed: ‘. . .religious book and fabrics placed on pts [patient’s] chest’ (Case 2-22, Age 76-years, Intensive Care Unit).
Discussion
This study reports care and support practices provided to families of dying hospital patients, and identifies potential missed opportunities, with important implications for clinical practice. These findings suggest there is need for improvement in practices associated with assessing and supporting family needs and to improve consistency within and across inpatient specialities.
Whilst an assumption was made that the preferred language of deceased patients and Next-of-Kin were the same, these data indicate underuse of professional interpreters; a surprising finding given language is one of the most significant barriers to high-quality end-of-life care 15 and professional interpreters are fundamental to ensuring effective, person-centred and culturally-sensitive communication. 16
Formal family meetings are essential to optimal care planning, particularly when death is anticipated. 17 These findings suggest a missed opportunity to also use formal family meetings to gather information that can be used to inform practices to support families and raise the question of why anticipated death did not trigger an assessment of family support needs, and routine referral/involvement of social work and pastoral care. Of note, these findings also suggest referral/involvement of specialist palliative care, social work and pastoral care is setting-dependent; with pastoral care involvement more common for patients in inpatient palliative care and social work involvement more common for those admitted to intensive care. Social workers are integral to supporting optimal family-centred care 18 and addressing emotional, social and existential concerns at the end of life. 19 Given these factors can act as barriers to timely support for families in hospital, 20 time spent assessing and supporting family needs, including spiritual and cultural needs is a priority area. 21 These suggest a missed opportunity to use anticipation of death as a trigger to prioritise family needs beyond formal family meetings.
Not every dying patient requires specialist palliative care, which may partially explain the low rates of specialist palliative care involvement in this study. However, as a speciality discipline, palliative care is responsive to the needs, preferences and values of people and their families. 22 Therefore, greater specialist palliative care involvement may result in increased opportunities to assess and address family needs. Previous research however, has suggested that not all clinicians who provide end-of-life care can refer to specialist palliative care personnel,11,23 and that referral is less likely when there is no specialist palliative care team onsite, 24 suggesting systemic organisational, policy and practice change is key.
Limitations
The challenge with a medical record audit is that it is not possible to determine with any certainty if documentation is an accurate representation of actions associated with care provision, or a reflection of what was deemed important enough to document. Additional actions to support family members may have occurred but were not documented.
This work is retrospective, and hence limited by the evidence available in the patient medical record. Whilst clinical factors such as vital signs and medications administration routinely documented, it is possible that other care actions, such as the occurrence of informal bedside family meetings, verbal offers of additional support declined by family, and facilitation of cultural rites and rituals may have occurred but were not recorded in the medical record. Similarly, because data were collected by retrospective review and not direct observation, it was not possible to measure the quality of family support. Whilst an a priori decision was made to include deceased patients from four inpatient specialities to maximise heterogeneity, the study was conducted in one health service, so findings may not be generalisable to other settings.
Conclusion
Practices to assess and support family needs are key to high quality end-of-life care. These findings suggest patient deterioration and/or anticipation of death should be used to routinely trigger referrals to specialist support personnel to ensure practice is guided by, and supports family needs at the end of life. While not every dying patient needs specialist palliative care input, given that the focus of palliative care includes patients and their families, prioritising family needs should be core to end-of-life care. Furthermore, greater specialist palliative care involvement across practice settings may aid in more consistent assessment of family needs. These findings also suggest that more research is needed to measure and evaluate how assessment of family needs can inform clinical practice to better support families at the end of life, supported by policy.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of Kate Neale, RN, for her contribution to data collection for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research received funding from the Centre for Quality and Patient Safety Research, Institute for Health Transformation at Deakin University, Australia.