
Abstract
Background:
Goals of care discussions ensure patients receive the care that they want. Recent studies have recognized the opportunity for allied health professionals, such as nurses, in facilitating goals of care discussions. However, the outcomes of such interventions are not well studied.
Aim:
To compare the outcomes of goals of care discussions led by physicians and nurses.
Design:
This is a retrospective cohort study of patients admitted to an Internal Medicine unit from January 2018 to August 2019. A comprehensive chart review was performed on a random sample of patients. Patient’s decision to accept or refuse cardiopulmonary resuscitation was recorded and analyzed. Analysis was stratified by patients’ comorbidity burden and illness severity.
Setting/Participants:
The study took place at a tertiary care center and included 200 patients. Patients aged ⩾ 18 were included. Patients who have had pre-existing goals of care documentation were excluded.
Results:
About 52% of the goals of care discussions were completed by nurses and 48% by physicians. Patients were more likely to accept cardiopulmonary resuscitation in nurse-led discussions compared to physician-led ones (80.8% vs 61.4%, p = 0.003). Multiple regression showed that patients with higher comorbidity burden (OR 0.71, 95% CI: 0.62–0.82), more severe illness (OR 0.89, 95% CI 0.88–0.99), and physician-led goals of care discussions (OR 0.30, 95% CI: 0.15–0.62) were less likely to accept cardiopulmonary resuscitation.
Conclusions:
There was a significant difference between the outcomes of goals of care discussions led by nurses and physicians. Patients were more likely to accept aggressive resuscitative measures in nurse-led goals of care discussions. Further research efforts are needed to identify the factors contributing to this discrepancy, and to devise ways of improving goals of care discussion delivery.
Goals of care discussion is an important aspect of patient care.
While physicians and residents were considered the most acceptable professional groups to engage in the decision-making aspect in a goals of care discussion, recent studies have recognized the opportunity for allied health professionals, such as nurses, in facilitating goals of care discussions.
The outcomes of goals of care discussions among healthcare professionals are not well studied.
This study demonstrated a significant difference in the outcomes of goals of care discussions led by physicians and nurses and found that patients were more likely to choose to accept cardiopulmonary resuscitation after nurse-led discussions.
This difference was particularly pronounced in patients who had the highest comorbidity burden and illness severity.
There was a significant difference between the outcomes of goals of care discussions led by nurses and physicians, which may reflect a difference in inter-professional perspectives, as well as the delivery of goals of care discussions.
These findings prompt the need for interdisciplinary education and collaboration in this domain.
The results of this study will help inform policies surrounding goals of care discussions and resuscitation orders.
Background
Goals of care discussions ensure that patients and their families are active participants in the decision-making process surrounding patients’ medical care, and that the health care team will respect the patients’ wishes and provide the appropriate level of care. Goals of care conversations involve an understanding of patients’ values and preferences in the context of their current clinical situation. The results include medical orders for the use or non-use of life-sustaining treatments. Patients who had an opportunity to discuss goals of care with a healthcare professional were more likely to receive care that was consistent with their preferences.1,2 In a study of patients with advanced cancer, goals of care discussions were associated with less aggressive medical care, with lower rates of ventilation, resuscitation, and intensive care unit admission. 3 Less aggressive medical care in this setting was also associated with better patient quality of life. 3 Adhering to patients’ do-not-resuscitate preferences not only underscores patient autonomy, but can have significant economic impact on the healthcare system. 4
In a recent survey of clinicians, while physicians and residents were considered the most acceptable professional groups to engage in the decision-making aspect in a goals of care discussion, involvement of nurses was deemed appropriate. 5 Nurses often share a strong therapeutic relationship with patients and are in a unique position to contribute to goals of care discussions. Nurse-led goals of care initiatives have been shown to increase engagement in goals of care discussions and documentation.6,7 However, the outcomes of goals of care discussions led by physicians and nurses have not been examined in the current literature.
In the Regina region of the Saskatchewan Health Authority, nurses (registered nurses and licensed practical nurses) are trained to initiate and establish patients’ goals of care independently, a responsibility shared with physicians. The objective of this study was to compare the outcomes of goals of care discussions led by nurses and physicians. Our hypothesis is that patients are more likely to accept cardiopulmonary resuscitation after nurse-led goals of care discussions compared to physician-led ones.
Method
Research question
In patients admitted to an Internal Medicine ward at Regina General Hospital, is there a difference in the outcomes of goals of care discussions led by nurses versus physicians?
Design and data collection
A cross-sectional retrospective chart review was conducted on a random sample of 200 patients. From the electronic medical records, demographic information (age, gender), clinical information (comorbidities as measured by the Charlson Comorbidity Index, 8 and severity of illness as measured by the National Early Warning Score 2 9 ) were recorded. A goals of care discussion requires an understanding of a patient’s baseline health status and their current illness severity. Both factors, along with the patient’s personal values and beliefs, contribute to the outcomes of a goals of care discussion. In this study, the Charlson Comorbidity Index and the National Early Warning Score 2 were used to provide objective measures of each patient’s baseline health status and illness severity, respectively. The Charlson Comorbidity Index provides a summary measure of comorbidities based on 19 weighted medical issues and is a well-validated tool that has been shown to predict 1-year mortality. 8 The National Early Warning Score 2 is based on six physiological parameters and determines the degree of illness in patients. National Early Warning Score 2 predicts patients at high risk of deterioration, 10 with high scores associated with early mortality.11,12
Every patient who is admitted to the hospital is asked to fill out a document that outlines their goals of care. While in the emergency department or when first admitted to the ward, a healthcare professional (including physicians or nurses) will have a goals of care discussion with the patient. In this study, only a patient’s resuscitation preference (to accept or refuse cardiopulmonary resuscitation) was examined, recognizing that a goals of care discussion encompasses many other aspects. When the patient’s goals of care preferences are documented, the results include medical orders for the use or non-use of life-sustaining treatments. Only the first goals of care documentation completed after admission was reviewed. The professional group of the person completing the goals of care documentation (i.e. nurse, resident, or physician) and the choice indicated were recorded. In this study, nurses include registered nurses, who have completed a four-year post-secondary university nursing program with a bachelor’s degree, and licensed practical nurses, who have completed a two-year nursing diploma program.
Setting
Subjects were patients admitted to an Internal Medicine ward at Regina General Hospital. Regina General Hospital is one of two tertiary care centers in Saskatchewan, Canada, serving a population of approximately 500,000.
Population
Chart review was conducted on a random sample of 200 patients. Inclusion criteria include adult patients aged 18 or over admitted to an Internal Medicine unit at Regina General Hospital between January 2018 to August 2019. Exclusion criteria include patients with an established goals of care decision documentation prior to the current admission.
Data analysis
Baseline characteristics of patients with nurse-led goals of care discussions were compared against those with physician-led goals of care discussions. Intergroup comparisons were performed using Chi-square or Fischer’s Exact test for categorical variables and Whitney-Mann-U test for continuous variables. The comparison was stratified by Charlson Comorbidity Index (0–2 Mild, 3–4 Moderate and ⩾5 Severe) and National Early Warning Score 2 (0–4 Low, 5–6 Medium, ⩾7 High) categories.8,9 Finally, multivariable logistic regression was used to elicit predictors of patients’ goals of care choices using sex, Chalrson Comorbidity Index, National Early Warning Score 2, and the healthcare professional leading the goals of care discussion as independent variables. Independent variables were selected a priori. A sample size of 200 was determined based on an estimate 20% of patients declining cardiopulmonary resuscitation, our a priori decision to include 4 variables, and an event per variable of 10. 13 Statistical analyses were completed using IBM® SPSS® version 22. For all statistical analyses, a p-value of less than 0.05 was considered significant.
Ethical issues
There were a number of ethical issues that were considered in this study. First, goals of care discussions should respect patient autonomy. However, in cases where patients lack the capacity to make medical decisions for themselves, substitute decision makers were involved in the goals of care discussions. Second, the outcomes of goals of care discussions can affect decisions surrounding medical care. There may be inherent differences between how a nurse and a physician leads a goals of care discussion. Nurses at Regina General Hospital are trained to lead goals of care discussions. However, patients do have the right to request a goals of care discussion led by a physician. This study received approval from the Research Ethics Board of the Regina region of the Saskatchewan Health Authority (REB-19-77).
Results
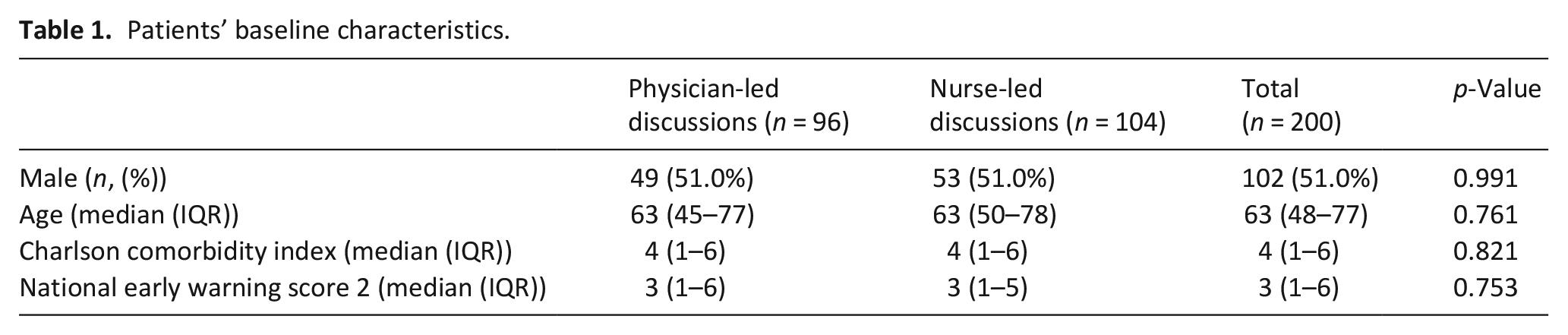
A total of 200 patients admitted to the Internal Medicine service were reviewed. The median age was 63 years (IQR 48–77). About 51% of the patients were male. The most prevalent comorbidities were diabetes mellitus (n = 53, 26.5%), chronic obstructive pulmonary disease (n = 50, 25.0%), and congestive heart failure (n = 44, 22.0%). Baseline patient characteristics and distribution between the two intervention groups were included in Table 1. There was no significant difference in sex, age, Charlson Comorbidity Index, or National Early Warning Score 2 scores between the two cohorts (Table 1). Overall, there was a significant association between the healthcare professional having the goals of care discussion and the discussion outcomes. Patients were more likely to accept cardiopulmonary resuscitation after nurse-led goals of care discussions than with physician-led ones (80.8% vs 61.4%, p = 0.003) (Figure 1).
Patients’ baseline characteristics.
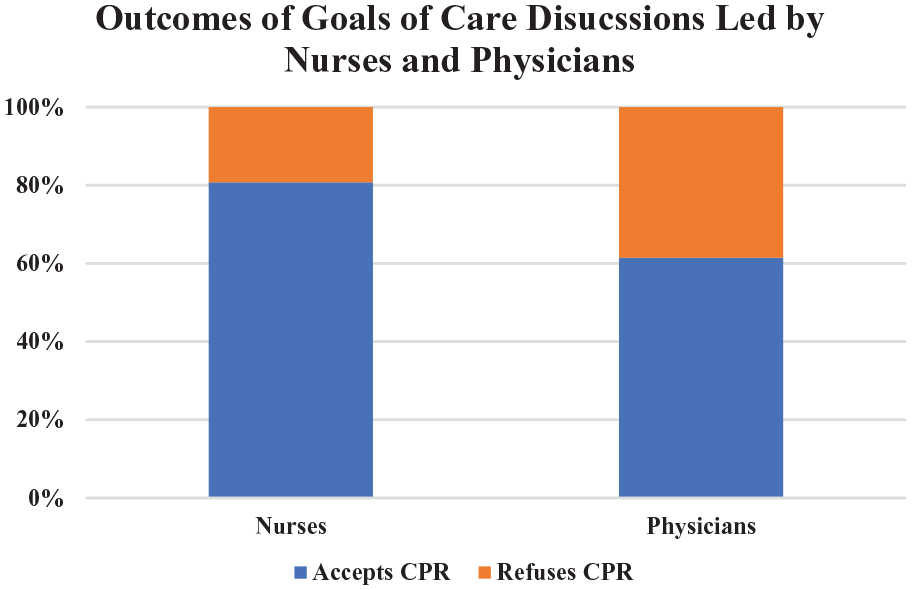
Goals of care discussion outcomes based on professional group leading the discussions.
By comorbidity and illness severity scores
There was no significant difference in the outcomes of nurse-led versus physician-led goals of care discussions among patients with mild or moderate Charlson Comorbidity Index. Among patients with severe Charlson Comorbidity Index, there was a significant difference (69.4% versus 40.0% accepting cardiopulmonary resuscitation, nurses versus physicians, p = 0.005), with patients more likely to accept cardiopulmonary resuscitation after nurse-led goals of care discussions (Table 2).
Outcomes of goals of care discussions based on Charlson comorbidity index and national early warning score 2 categories.
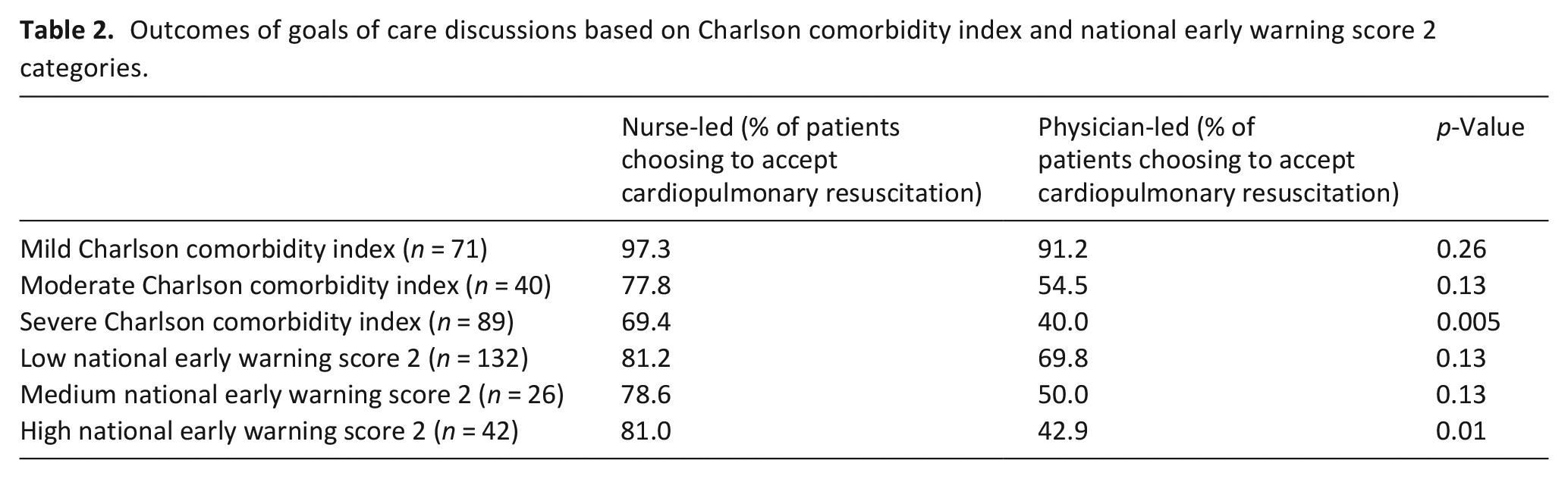
There was no significant difference in the outcomes of nurse-led versus physician-led goals of care discussions among patients with low or medium National Early Warning Score 2. Among patients with high National Early Warning Score 2, there was a significant difference (81.0% vs 42.9% accepting cardiopulmonary resuscitation, nurses versus physicians, p = 0.01), with patients more likely to accept cardiopulmonary resuscitation after nurse-led goals of care discussions (Table 2).
Factors associated with patients’ goals of care decisions
Patients’ sex was not significantly associated with patients’ goals of care discussion outcomes (OR 1.15, 95% CI: 0.58–2.30), while Charlson Comorbidity Index and National Early Warning Score 2 were significant predictors of patients’ goals of care decisions. Those with higher Charlson Comorbidity Index (i.e. older patients or those with more comorbidities) (OR 0.71, 95% CI: 0.62–0.82) and those with higher National Early Warning Score 2 (OR 0.89, 95% CI: 0.81–0.89) were less likely to accept cardiopulmonary resuscitation. Those who had a physician-led goals of care discussion were also less likely to accept cardiopulmonary resuscitation (OR 0.30, 95% CI: 0.15–0.62). These results are shown in Figure 2.
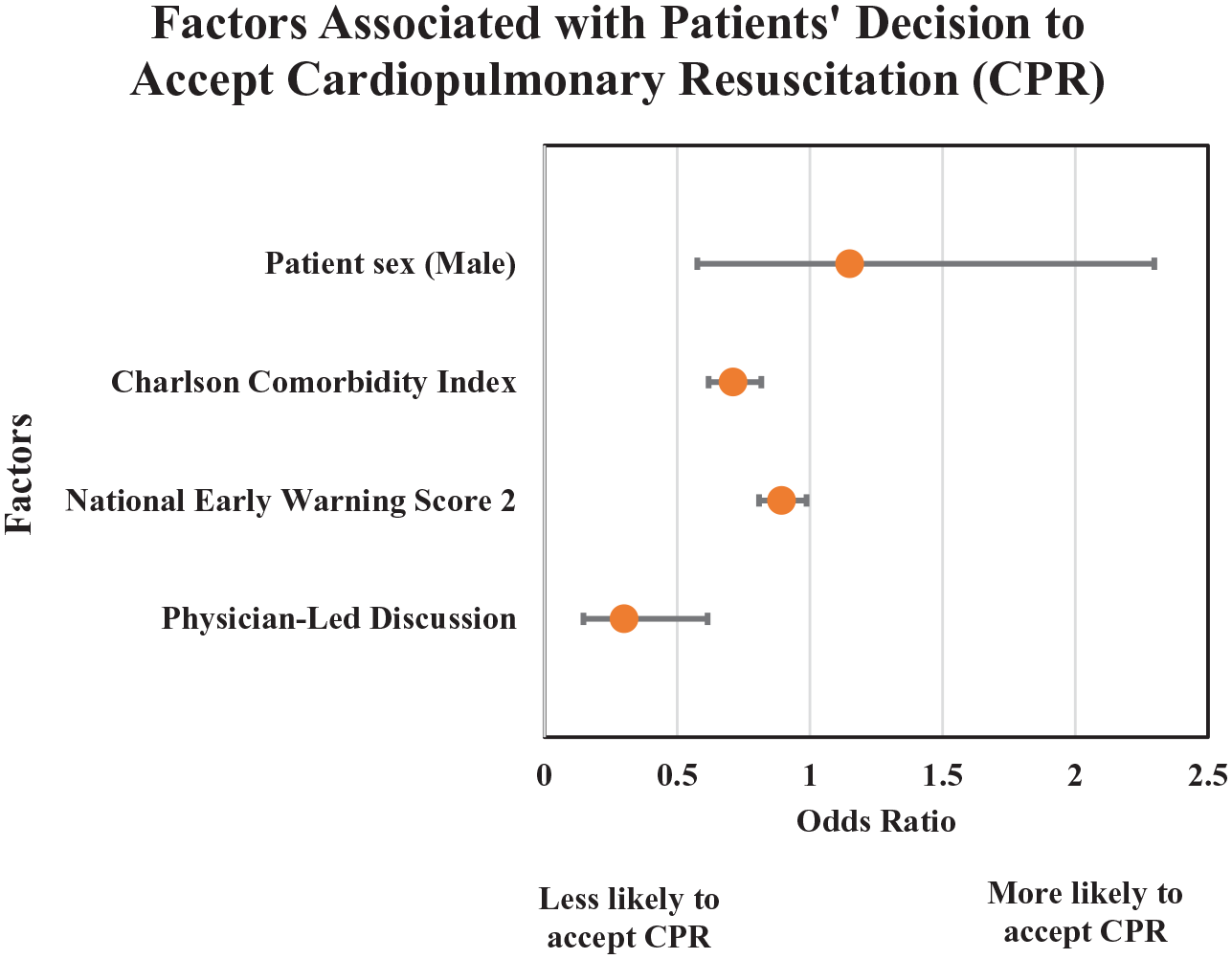
Factors associated with patients’ decision to accept or refuse cardiopulmonary resuscitation after goals of care discussions.
Discussion
Goals of care discussion is an important aspect of patient care, as it allows healthcare professionals to understand and respect patients’ preferences with regards to resuscitation and end-of-life care. Physicians are often perceived as the most appropriate professional group to lead goals of care discussions. 5 However, research has shown that engagement is often low, with many patients without clear goals of care documentation and their physicians not aware of their resuscitation preferences.6,14 Nurses, who spend a significant amount of time caring for admitted patients, often develop a strong therapeutic relationship with their patients, and are in a unique position to contribute to goals of care discussions. Studies have shown that nurses are willing and often desire to be engaged in goals of care discussions.15,16 Nurse-led initiatives can lead to an increase in goals of care conversations and documentation.7,17 Nonetheless, while healthcare professionals agree that nurses’ involvement in goals of care discussions can be helpful,14,15 the role of nurses in this process is not well defined. An integrative review of 19 studies found that few nurses demonstrated the knowledge or confidence in having a goals of care discussion with patients. 18 A lack of support, education, and time have been cited as barriers. 19 Furthermore, in a number of goals of care initiatives led by nurses, despite an increase in the completion rate of goals of care discussions and documentations, these projects failed to improve medical care or patient wellbeing.6,7
Major findings/results of the study
In this study, patients were more likely to choose to accept cardiopulmonary resuscitation after nurse-led compared to physician-led discussions. We observed the biggest difference in goals of care outcomes in the subset of patients with the highest comorbidity burden and who were the most severely ill on admission.
What this study adds
A potential factor is that healthcare professionals may have different perspectives regarding goals of care. A study by Petterson et al. 20 showed that nurses assign greater value to patient autonomy, while physicians placed more weight on non-maleficence, when asked about resuscitation decisions. While both are important principles to uphold in goals of care discussions, different emphases may result in different outcomes. A respect for autonomy is built upon the basis of informed patients. Unfortunately, the public often has misconceptions regarding resuscitation. A study of long-term care residents and inpatients on geriatric wards in Hong Kong showed that most subjects overestimated the success rate of cardiopulmonary resuscitation and favored accepting this intervention. 21 After being informed of the outcomes of cardiopulmonary resuscitation, up to 20% who initially accepted cardiopulmonary resuscitation reversed their decisions.21,22 It is conceivable that physicians, who focuses more on non-maleficence during goals of care discussions, spend more time educating patients regarding the risks and poor outcomes of resuscitation, leading to less patients choosing to accept cardiopulmonary resuscitation.
Another potential contributor to this difference is the ability of nurses and physicians to predict prognosis. In order for patients to make informed decisions regarding their goals of care, an understanding of their disease trajectory and life expectancy is pertinent. Studies have shown that while nurses are better at recognizing imminent death, 23 physicians are generally more accurate when it comes to predicting 6-month mortality. 24 Recognition of patients who are approaching their end of life facilitates the discussion of do-not-resuscitate orders. There is also uncertainty when it comes to predicting life expectancy, with physicians tending to underestimate survival, 25 and nurses erring on the side of optimism. 26 As a result, patients who believe they have a longer life-expectancy may preferentially choose to accept cardiopulmonary resuscitation. Healthcare professionals’ biases when providing patients with a prognosis may influence patients’ decisions to accept or refuse cardiopulmonary resuscitation. This emphasizes the need for interdisciplinary communication prior to goals of care discussions with patients.
Finally, patients’ preference to accept cardiopulmonary resuscitation may be a reflection of nurses’ hesitancy in taking on the responsibility of a life-or-death decision. This is in part due to a lack of clear delineation of a nurse’s role in goals of care discussions. 27 Surveys have shown that while nurses are deemed acceptable in initiating a goals of care discussion and acting as a decision coach, the final decision is most appropriately made by the patient in conversation with a physician. 5 This is particularly true for do-not-resuscitate orders. In this study, only 19.2% of nurse-led goals of care discussions resulted in do-not-resuscitate orders, versus 38.6% of physician-led ones. A survey conducted in Iran showed that both physicians and nurses believed that nurses were not qualified to issue do-not-resuscitate orders. 28 A similar study conducted in the US showed less partisan findings. When physicians and nurses were asked about their beliefs and attitudes regarding do-not-resuscitate discussions, the majority (69%) of physicians were in support of having nurses initiate such conversations. 29 Furthermore, nurses indicated that they would find the discussion a rewarding clinical experience. 29 It is evident that there is controversy surrounding whether nurses should issue do-not-resuscitate orders. Therefore, nurses, in leading goals of care discussions, may demonstrate a bias towards what is perceived as the “safer” approach of accepting cardiopulmonary resuscitation.
In an ideal situation, goals of care discussions should involve a multi-disciplinary team, with physicians, nurses, and other allied health professionals each offered the opportunity to communicate and contribute to the conversation. However, this can pose a challenge from a time and human resource perspective. It is increasingly recognized that non-physician healthcare professionals can be trained to lead to goals of care discussions. Nurses, in particular, are in a unique position to advocate for their patients in this regard. More education is needed to empower nurses to effectively explore and establish patients’ goals of care. The focus of the education should cover not only life-sustaining measure options, but also the outcomes of these measures in the context of patients’ individual illness severity. This will help mitigant some of the discrepancies in the outcomes of goals of care discussions led by nurses and physicians observed in this study.
Strengths and limitations of the study
The strengths of this study include its novelty and clinical relevance, as well as a straightforward study design. To our knowledge, this is the first study comparing the outcomes of goals of care discussions led by different healthcare professionals. This adds to the existing literature on physicians and nurses’ perception of goals of care discussions. This study has a number of limitations. First, its retrospective nature precludes strong claims regarding causation. The data can only speak to a difference in the outcomes of goals of care discussions, and not the content or quality of the process. The exclusion of patients with pre-existing goals of care documentation would have led to an underestimation of patients with do-not-resuscitate orders. Second, this study took place in one Internal Medicine ward in Saskatchewan, Canada, and may not be generalizable to other services or sites. Third, goals of care in this study was narrowly defined as patients’ decision to accept or refuse cardiopulmonary resuscitation. In a clinical setting, goals of care is comprised of many elements of clinical care. It should not only be about the dying process but should focus on how the patients want to live. Further research is indicated to explore these other aspects of goals of care.
Conclusion
In this study, we examined differences in the outcomes of goals of care discussions led by physicians and nurses and found that patients were more likely to choose to accept cardiopulmonary resuscitation after nurse-led discussions. This difference was particularly pronounced in patients who had the highest comorbidity burden and illness severity. Potential factors contributing to this discrepancy include a difference in perspectives on goals of care, uncertainty in prognosis prediction, as well as concerns regarding the responsibility of do-not-resuscitate orders. Nurses and non-physician healthcare professionals are key participants in the goals of care discussion process and further education is needed to empower all individuals to lead effective goals of care discussions.
Footnotes
Author contributions
Karen Ho was responsible for the conception and design of the study, data acquisition, and manuscript preparation. Krystyna Wang was responsible for data collection and manuscript preparation. Adam Clay was responsible for the analysis and interpretation of data, as well as proofreading of the manuscript. Elizabeth Gibbings was responsible for the conception and design of the study, proofreading of the manuscript, as well as the supervision of this study.
Data management and sharing
The data that support the findings of this study are available on request from the corresponding author, KH.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
This study received approval from the Research Ethics Board of the Regina region of the Saskatchewan Health Authority (REB-19-77).