
Abstract
Background:
Impaired readiness may hinder purposeful advance care planning in cancer patients. To reduce barriers to participation in end-of-life decision-making, a collaborative intervention was developed combining a psycho-oncological approach of dignity-based and cognitive-behavioural interventions, followed by a standardised advance care planning-process.
Aim:
To evaluate the novel collaborative advance care planning-approach by synthetising cancer patient and carer perspectives on communicational and relational effects.
Design:
As a sub-project of a mixed-methods evaluation study, we conducted an inductive content analysis of qualitative interviews with advanced cancer patients and caregivers to deeply explore the focused impact of a collaborative advance care planning-approach on communication and relationship dynamics.
Setting/participants:
Twelve patients with advanced cancer and 13 carers who participated in a collaborative advance care planning-intervention.
Results:
The collaborative advance care planning-approach was consistently evaluated positively by participants. Transcriptions of the semi-structured interviews were coded, analysed and merged under three main themes concerning communicational and relationship dynamics: action readiness, content readiness and impact on future communication and relationship.
Conclusions:
The novel intervention served to foster individual readiness – including action and content readiness – for advance care planning-discussions by addressing highly individualised barriers to participation, as well as specific end-of-life issues. In addition, societal readiness could be promoted. Although the brief psycho-oncological intervention could not fully meet the needs of all participants, it can be used to develop individual psychotherapeutic strategies to improve different facets of readiness. The collaborative advance care planning-approach might require more time and human resources, but could pioneer successful advance care planning.
Keywords
Advance care planning (ACP) is seen as an impactful measure to optimise end-of-life communication and improve patient-centred outcomes, but there are a variety of barriers to engaging in the discussion process.
Psycho-oncological care can reduce emotional distress and improve the quality of life of cancer patients and their families.
Psychological interventions have been shown to have positive effects on healthy adults’ readiness to address end-of-life issues, suggesting a potential approach to promote readiness among patients with advanced illness.
This study demonstrates benefits of an innovative intervention supporting advance care planning with advanced cancer patients and their carers by preceding psycho-oncological sessions.
Our collaborative advance care planning-approach had pertinent effects on communication and relationship, particularly on action, content and societal readiness for advance care planning.
Despite the demand for more time and human resources, the collaborative approach could serve as a precursor to end-of-life conversations and increase the number of reliable advance care planning-discussions.
Psycho-oncological interventions prior to advance care planning not only strengthen readiness for advance care planning, but may also serve as a screening tool to identify patients with deeper barriers to dealing with terminal illness, in order to refer them to advanced therapeutic services.
Introduction
In recent years, there has been growing awareness of the importance of patient-centred end-of-life care including shared decision-making. In this respect, advance care planning (ACP) has been advocated as a crucial element of high-quality palliative care. 1 Advance care planning is a structured conversational process enabling ‘individuals to define goals and preferences for future medical treatment and care, to discuss these goals and preferences with family and healthcare providers, and to record and review these preferences if appropriate’. 2
Cancer patients and their caregivers show high levels of distress and palliative care needs. 3 There is little doubt that advance care planning improves many patient-relevant endpoints.4,5 Additional evidence suggests psychological benefits for patients’ families. 6 Accordingly, Johnson et al. 7 argue that advance care planning should be understood relationally and implemented as a family-centred, social process rather than an individual directive.
However, inconsistent evidence for some outcome parameters, limited uptake for advance care planning despite awareness-raising initiatives, and situational and organisational barriers led some to challenge the utility of advance care planning. 8 Still, open communication in families is not only an indicator of higher congruence in care preferences 9 but also associated with less aggressive care shortly before death and better quality of life. 10 Indeed multiple psychological barriers lead to reservations to engage in end-of-life conversations in the family context. 11 The resulting taboo nature of death and dying impedes a successful initiation of advance care planning-discussions. 12 Nevertheless, even patients who committed to advance care planning may display impaired readiness, especially when discussing potential end-of-life scenarios. Facilitators must therefore permanently adjust the sequence and depth of conversations, 13 yet compromised readiness may hinder a constructive conversation flow or even cause serious distress following standard advance care planning-discussions.
Psycho-Oncology is concerned with patients’, families’ and caregivers’ responses to cancer, studying psychological, behavioural and psychosocial factors involved in the risk, detection, course, treatment and outcome of cancer. 14 Psycho-oncological care reduces emotional distress and improves quality of life of patients and their partners helping them to cope with the disease.15–17 Combined value-based and motivation-based interventions had positive effects on healthy adults’ readiness to engage in end-of-life topics. 18 Strikingly, even though a nationwide voluntary certification process in Germany led to an increase in psycho-oncological care-frequency, the minority of cancer patients make use of psycho-oncological services, with weak data pointing to individual reservations, hindering patient characteristics, but also organisational-structural hurdles.19–22
Acknowledging a multitude of barriers for advance care planning-uptake at an individual and interpersonal level, 23 a mixed-method randomised controlled trial was designed to investigate the efficacy and effectiveness of a collaborative advance care planning-approach. To improve access and quality of advance care planning the intervention targeted psychosocial barriers of advanced cancer patients and informal caregivers towards end-of-life discussions applying dignity-based and cognitive behaviour-based interventions preceding a standardised advance care planning-process.24,25 This qualitative research adds to the literature by exploring cancer patients’ and carers’ perceptions of a novel collaborative advance care planning-model evaluating combined effects focusing on communication and relationship dynamics.
Methods
Study design
Col-ACP is a mixed-method randomised controlled trial evaluating a complex advance care planning-intervention including psycho-oncological sessions (cf. Figure 1). A qualitative approach was embedded to further specify the intervention’s impact through in-depth feedback by patients and carers.
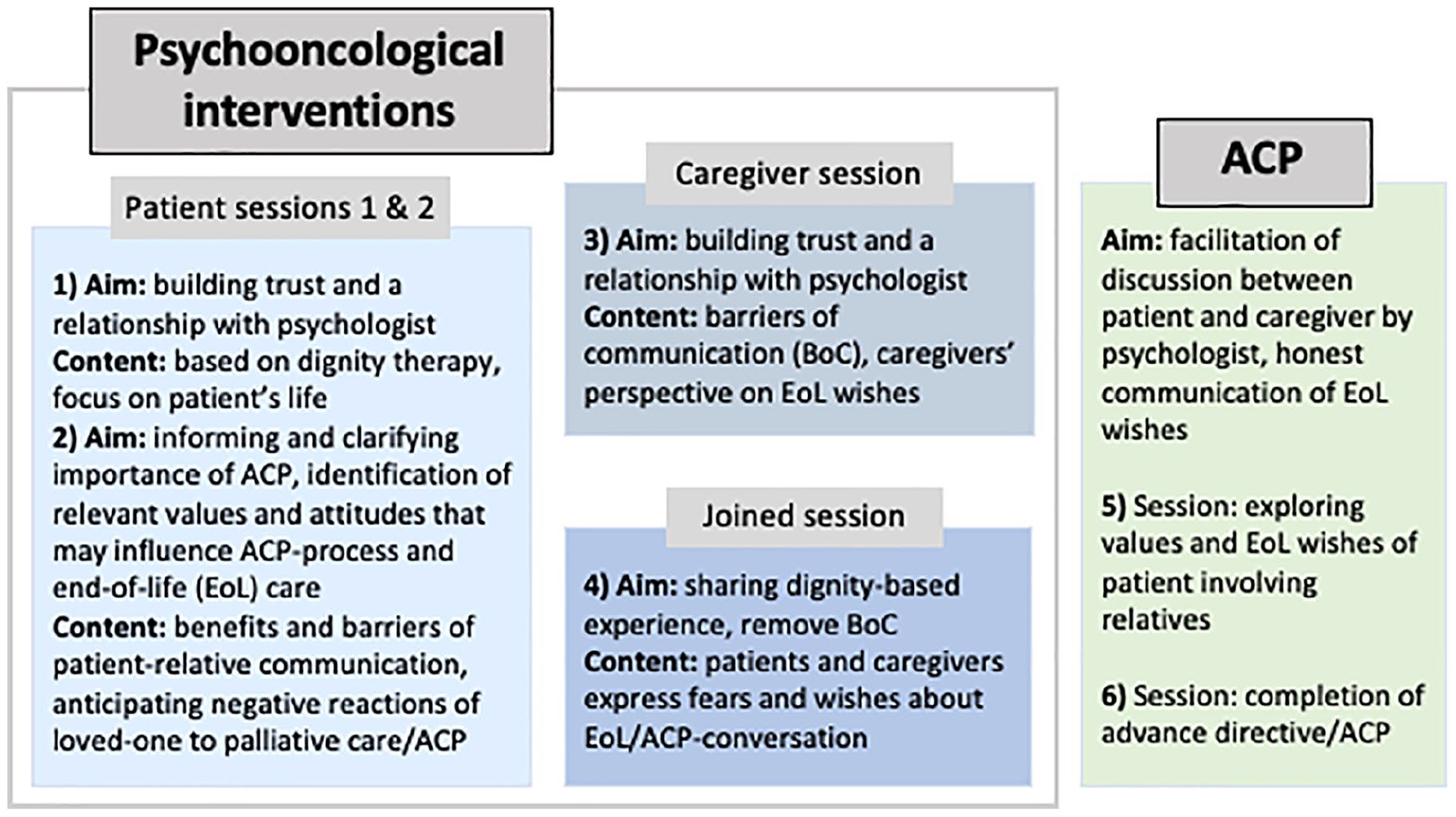
Conduction of the collaborative ACP-approach.
The intervention included a total of six sessions. The first session focused on important milestones in the patient’s life story using a dignity therapy question protocol. In the second session, the patients elaborated on the relevance of planning their end-of-life phase under psychological guidance. This did not only encompass discussing potential benefits but also barriers to engage in effective patient-family communication and advance care planning. Identification and modification of these barriers were based on intervention techniques of cognitive behavioural therapy, taking into account existential approaches. To incorporate relatives’ perspective, a third session was conducted with family carers only, analogous in content and technique to the second session. Session 4 provided a moderated conversation process to patients and carers aiming at sharing the dignity-based experiences in order to identify and remove individual barriers to end-of-life communication. Finally, the last two sessions were dedicated to the standardised advance care planning-process. The duration of each of the first four sessions was set at about 50 min; the length of the advance care planning discussions was entirely based on individual needs. The maximum length for the intervention phase was predetermined to be 16 weeks. Intervals between the individual micro-interventions were agreed individually with the patients and their relatives. An extensive research protocol comprising detailed information on study design, participant characteristics, recruitment sites and methods, the intervention, data collection process and analysis has been published in an open access format. 25 The col-ACP-study was registered at ClinicalTrials.gov (NCT03387436).
Setting
For the entire col-ACP trial, we recruited adult cancer patients with non-curable diseases and their family carers from in and outpatient settings of the University Hospital of the Philipps-University Marburg (Department of Haematology, Oncology and Immunology, Department of Oncological Urology, Department of Oncological Gastroenterology, Department of Radiation Therapy), the oncological rehabilitation centre Klinik Sonnenblick in Marburg, and the specialist community palliative care team of the county of Marburg-Biedenkopf.
Sampling
The col-ACP trial was open to all neoplastic entities. Patients were screened with the ‘surprise question’, 26 however, were excluded if the treating physician expected survival to be less than 4 months after randomisation. Further exclusion criteria were incapacity to perform the study intervention (e.g. ECOG ⩾ 3), insufficient German language skills and cognitive inability to give informed consent. For this sequential qualitative study, we targeted a purposeful sample of patients and family caregivers after completing advance care planning-discussions to capture a breadth of views.
Recruitment
We enrolled participants of col-ACP recruited from oncological inpatient and outpatient settings of the University Hospital of Marburg to be able to approach patients personally. All participants gave their informed written consent before study participation.
Data collection
To evaluate the intervention comprehensively, we saw the need to address the research subject through a qualitative evaluation. This served to gauge subjective views of individuals, but also group phenomena, in order to complement the quantitative results of the randomised controlled trial. To that end, the multidisciplinary research team (C.S., P.B., J.R., M.K., S.H.) developed an open-ended question interview guide aiming at the participants’ experience with the intervention (for an English translation cf. supplemental material). In particular, we examined how participants engaged in the conversation process, how end-of-life decisions were made, and to what extent communication and relationships changed post-intervention. Two researchers (T.M., A.G) conducted face-to-face semi-structured interviews that were digitally audiotaped. We interviewed patients and caregivers separately to avoid potential mutual influence or conflicts that could have been triggered by dyadic interviews. Open communication was encouraged by emphasising the interviewer’s independence from the col-ACP main research team. Recruitment was completed when the research team agreed that data saturation was achieved. 27 Interviews were transcribed verbatim but care was taken to anonymise patient, carer or staff identifiable references. For publication, illustrative quotes were pseudonymised and translated from German into English by a fluent speaker.
Analysis
Transcripts were managed using MAXQDA Analytics Pro. We performed an inductive content analysis based on the analytical framework proposed by Mayring, 28 widely used in medical qualitative research working with large amounts of written data. The analysis was conducted in several analytic steps. In early stages of the analysis, discrete sections of text representing relevant ideas were clustered to codes by A.P. through line-by-line review of five interview transcripts for each participant group. Ensuring a structured approach in this step of the analysis, each code received a ‘code definition’. Passages assigned to codes were compared both within and across interviews and overarching themes were identified and formed into a structure of codes. A.P. then applied the developed code structure to all transcripts and expanded it in an iterative process as new aspects arose. To enhance rigour and confirmability, four additional authors read all transcripts. Repetitive team meetings served to review preliminary results and iteratively identify and redefine pertinent themes emerging from the data exploring the intervention’s impact on communication and relationship of cancer patients and their carers.
Ethics
Ethical approval was obtained from the institutional review board of the Philipps-University Marburg (ID-No.: 173/17). The study was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice guidelines and the EU data collection directive. This study is reported following the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 29
Results
Participants
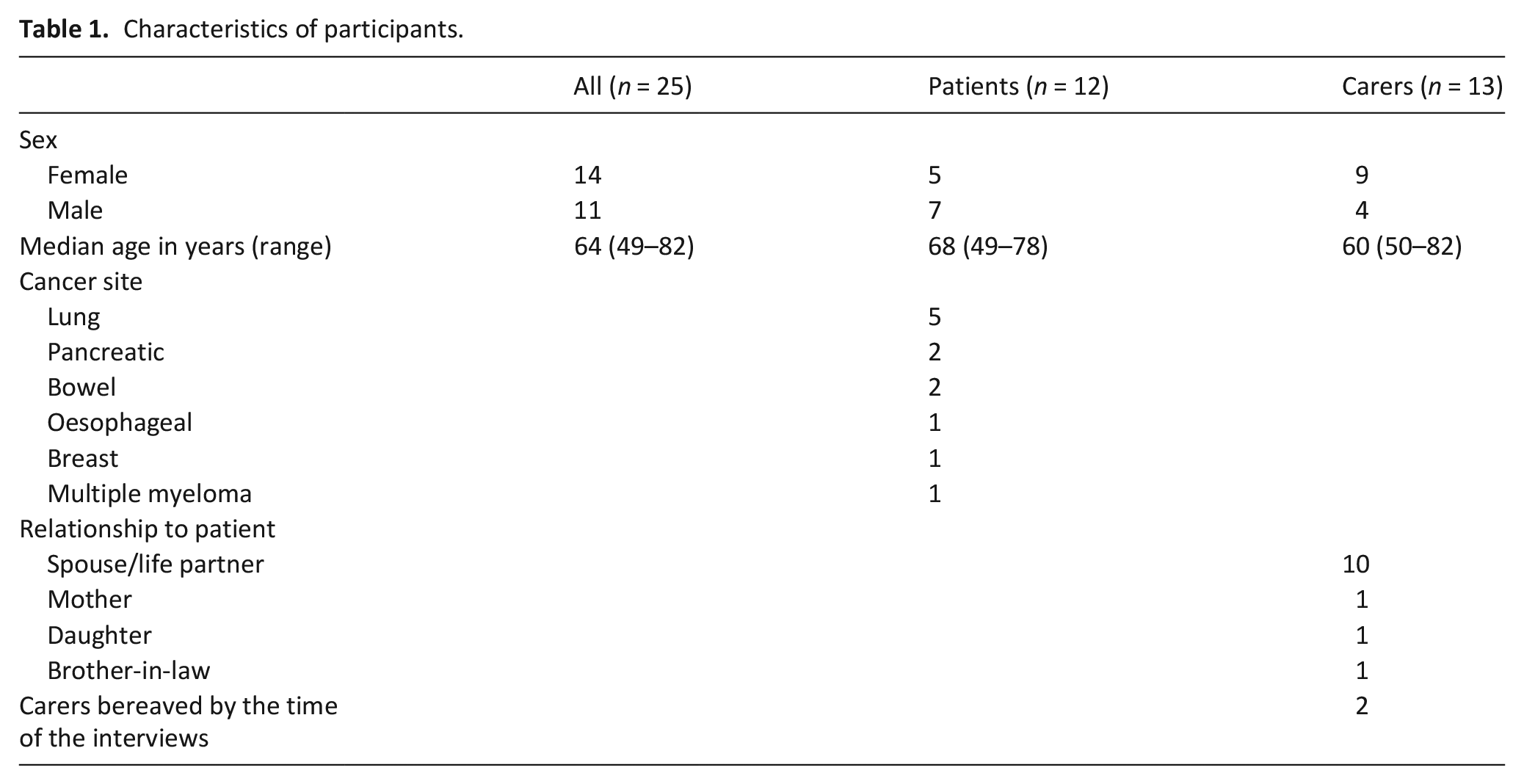
We performed interviews with 12 patients and 13 caregivers of 13 different patients between April 2018 and December 2020. The median interval between the last advance care planning-appointment and the qualitative interviews was 72 days for patients and 76 days for caregivers. Participant characteristics are provided in Table 1.
Characteristics of participants.
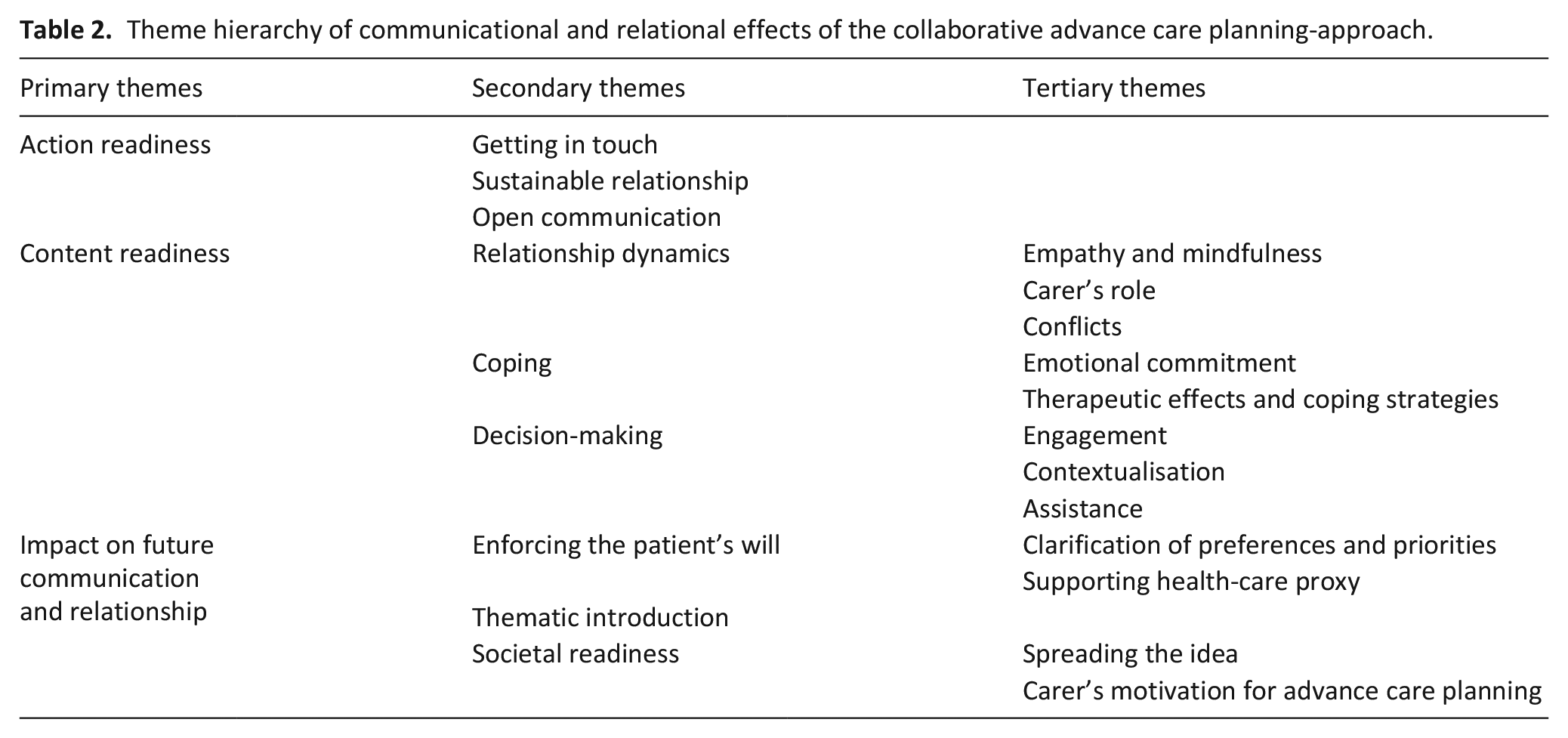
Our qualitative study revealed relevant influences of the intervention on communication and relationship. Three main themes emerged: action readiness, content readiness and impact on future communication and relationship (for an overview including subthemes cf. Table 2). In the following, we refer to the term action readiness as an essential factor when deciding whether to participate in advance care planning-conversations. Content readiness includes the ability to identify one’s values and wishes and to address different end-of-life issues during the advance care planning-process for decision-making. Within impact on future communication and relationship, we distinguished societal readiness, which encompasses the ability to engage with advance care planning on society-level.
Theme hierarchy of communicational and relational effects of the collaborative advance care planning-approach.
Action readiness
To facilitate goal-oriented discussions, prerequisites had to be established to promote participants’ action readiness.
‘Getting in touch’
Some participants indicated that they had not known how to create an advance directive, especially when critical of the practicalities of standard tick-box directives. Some admitted that they had avoided end-of-life issues in everyday life and consequently intentionally or subconsciously postponed writing advance directives. Participation in col-ACP was therefore seen as a convenient opportunity to overcome one’s reticence and thus confront end-of-life decisions.
You really have to take time for this topic, and this was the framework for it. That’s why it was good. Otherwise, it wouldn’t have been done. You always put it off anyway. Like a tax declaration ((laughs)). (Carer 3, daughter)
Sustainable relationship
Participants appreciated when the facilitator created a non-judgemental, empathetic atmosphere that allowed free expression of thoughts.
After all, there are people who have no understanding when you say you don’t want to be on life support even though you are, let’s say, gone. If I’m not there mentally, what’s the point of living? And there are people who have no understanding for that, and here you have understanding for that. Here you can express it freely. That is actually the essence of the whole story. (Patient 5, male)
Most participants valued the supervised emotional approach to end-of-life issues by the facilitator, which enabled a smooth communication process characterised by openness.
And now, with [the facilitator], I was able to talk very clearly and unambiguously about death and how to actually continue. He took away my reluctance to talk about it, and in this context, we also made an advance directive. (Patient 11, female)
Open communication
Many participants pointed out advantages of open communication facilitating the conveyance of attitudes towards illness and dying. The majority of family carers indicated that they became more aware of patients’ priorities and preferences during the intervention. Openness can thus facilitate changes in relationship.
Because he is an extreme person and he has of course decided that if he can’t do sports anymore, he doesn’t want to be treated anymore. He then basically said, first comes his sport and then the family. I thought it was good to know that now. (Carer 7, wife)
However, not all participants managed to open up emotionally. Some patients, all male, displayed a very matter-of-fact approach implying they did not want to engage in profound end-of-life conversations.
And yes, we saw no need to have deeper conversations. My wife knows the course, she knows the disease, behaves accordingly. And that is ideal in the current situation. (Patient 6, male)
Content readiness
Relationship dynamics
Empathy and mindfulness
Our collaborative advance care planning-approach exceeds a mere patient-centred intervention by providing for close involvement of relatives. Many participants, patients and carers alike, showed empathy for their relatives who were emotionally burdened by the discussions.
And then he started to cry, because I mean, hats off! Death is breathing down your neck! Well, that’s. . .living with it. . . I admire him. I don’t know if I could cope with it as well as he could. (Carer 7, wife)
For some pairings, this resulted in a more relaxed and understanding interaction within and beyond advance care planning-discussions.
Yes, you are more considerate. In the past, when things didn’t go so well, we used to squabble. And now it’s more like: “Ommm”. (Carer 10, husband)
Carer’s role
The carers’ perceptions of their role within discussions and ultimately the decision-process varied greatly. Their interpretation ranged from a passive to a supportive, advisory role to mostly one of the key players in a shared decision-making process.
Anyway, we discussed it for both of us and then decided how we wanted it. And that’s why it’s always easier when there are two of you. (Carer 1, husband)
Patients for the most part connoted their carers’ presence positively. Better absorption of new information, being on the same level of knowledge but also communication of their wishes to inform carers’ future decisions were central concerns in this context.
We were in agreement on the subject, but now she has also been intensively informed about what is really going on. Because it’s not a simple decision, even if it’s in writing. She still has to make a decision, which is not so easy either. (Patient 5, male)
Patients’ views on the range of carers’ activity levels within the discussion were similar to those of the carers’, but the perspective on decision-making responsibility differed. Many patients did not feel that their relatives’ participation or opinion influenced their decisions.
He was there and could express his opinion and did not agree with a lot of what I wanted. And, but that’s my decision, that’s what I said, I decide for myself what concerns me and you have to stick to it. (Patient 3, female)
Conflicts
Few participants reported disagreement or serious conflicts during the intervention leading to emotional distress. However, these seemed to build on already existing disputes.
We always clashed anyway, and I don’t know if the conversations made him close up even more. True to the motto: ‘My wife said it after all, she knew it.’ Because it was such a -, that’s our relationship now. When I said something, he always said something else. That’s why at some point I just gave up. I said, ‘It’s no use, it’s over.’ He has parents, he has friends, if they can reach him somehow, that’s fine. I can only accompany him. (Carer 11, female partner)
Nevertheless, it becomes apparent that despite facing a life-threatening illness it is precisely entrenched behavioural patterns and relationship conflicts that represent relevant barriers to end-of-life conversations to which a collaborative advance care planning-approach can respond.
No, I don’t talk about my disease either, I, he [husband] talks much more about his disease [. . .] There are whiners, ((laughs)) but I’m not one of them. So my illness is out of the picture. It’s hard and difficult, but it’s left out, because he has so much to do with his little aches and pains, so he babbles to me all day long and I accept that. (Patient 3, female)
Coping
Emotional commitment
The collaborative advance care planning-approach fostered coping strategies for both, patients and their caregivers. Most participants indicated that the intervention provided facilitated in-depth engagement with the illness, possible courses, and potential treatment goals. Although all patients were informed about their advanced cancer, the advance care planning-intervention helped some participants becoming fully aware of the diagnosis.
Retrospectively, I was a little bit influenced or impressed by the fact that I am in this palliative stage, although I don’t really feel that unwell. (Patient 8, male)
However, the intervention’s emotional impact was mixed. Relief, confidence, and hope were positive emotions that participants reported in the interviews.
Of course, it’s also relieving. Sometimes it’s better to give something away to strangers than to your own partner, because the relationship of trust is based on a completely different foundation. (Patient 6, male)
Sadness and fear were the dominant negative emotions experienced by participants that had to be addressed.
No, one is just afraid of death. That is the only thing. If it’s really. . .when they say “the end of life”. I mean, you never know when it’s going to be finished. No one can say. (Carer 5, wife)
Only a few participants reported serious emotional distress resulting from the discussions, which eventually continued after the conversation ended.
And that was very difficult for me, to talk about it and think about it, I have to say. It pulled me down so much that I had to deal with it for days. (Carer 9, wife)
Therapeutic effects and coping strategies
Although in some cases participants felt emotionally burdened by the conversations, they were able to derive positive effects in the long term. Some patients and carers alike saw immediate therapeutic effects of the intervention.
The conversations were actually always, well, I always said that I always had the feeling that it was like taking an inner bath. Yes, I always felt as if I could let out all the dirt inside that was weighing me down. That’s why I’ve always found it so cleansing, from the inside out. (Carer 2, wife)
As a result of the intervention, participants succeeded in aligning their emotional-focused coping strategies.
Cancer is an asshole, remains an asshole. I have it and I’m ready to fight. For me, that is the way of thinking about dying and talking about dying. That I can do it so well now and that I know what I want and what I don’t want, that has already changed my perspective. Since then I can deal with it better, since then I have also become a bit tougher, no longer so emotional. (Patient 11, female)
Decision-making
Engagement
Participants recognised the value of approaching the issues of illness and dying, identifying and verbalising attitudes and concerns to ultimately establish treatment goals. In this context, they treasured information gained, clarification of questions, thought-provoking impulses and sensitisation to distinct topics.
The conversations gave us so much information that we were able to think clearly. It was really very informative and somehow you could also understand your own decisions better. (carer 8, brother-in-law)
While relatives for the most part engaged in conversations to record patients’ preferences, some patients felt unable to make end-of-life decisions. These patients did not feel constrained by their disease or felt overwhelmed struggling to empathise with their own end of life. Others were in early stages of coping with their disease, so they could not embrace a focus other than cancer treatment.
They wanted to know what I wanted when I was about to die. I haven’t been in that situation before, never, that I was about to die. [. . .] Yes, that is difficult. Because I’m not focused on death, but on life. (Patient 1, female)
In a few patients, content readiness premised on the understanding that decisions were not definitive or irrevocable. In this respect, they referred to the possibility of being able to amend the advance directive should their perspective change.
Which [advance directive] is not really important, because I can change it at any time. So I didn’t see it as important. I can change my mind at any time, want something else, and decide. (Patient 3, female)
Contextualisation
Previous experiences with family and friends supported carers in building bridges to end-of-life topics.
Another thing we realized, a cousin who had a metal apparatus in his throat for three or four months and had to be artificially ventilated. . .And then he died afterwards. I don’t want that, for example. (Carer 1, husband)
In contrast, patients tended to relate end-of-life decisions directly to their own needs and priorities established with the facilitator.
I found it very pleasant because he phrased everything precisely so it is important for my particular case, in case resuscitation or something like that has to happen [. . .] I’m not that attached to it [life], although I still have a family, but I don’t want to suffer for long, I’d rather go to the other side. (Patient 8, male)
Assistance
Participants, especially those who already had conventional advance directives, highlighted clear benefits of the individual-centred concept of advance care planning to make precise end-of-life decisions.
I already had one earlier through the nursing service. And the advance directive that was recommended to me here, let’s just say, is more detailed and more precise. Well, there is no grey area or few grey areas, which was the case with the other one. (Patient 5, male)
Moreover, some patients who had not previously had advance directives stated that they would not have felt able to do so on their own valuing the facilitator’s expertise in helping patients understand and complete advance directives according to their wishes.
And as I said, [the facilitator] helped me very well with what I wouldn’t have been able to do on my own. Who knows what kind of crap I would have ticked off, how I would have understood the question if I read it myself or if I had it explained to me - that’s a huge difference! That’s why I would always do it with someone. . . (Patient 10, male)
Impact on future communication and relationship
While most participants had not noticed any relevant changes in their post-interventional relationship or communication style, individual implications became apparent in the course of the interviews.
Enforcing the patient’s will
Clarification of preferences and priorities
Some patients confided previously unexpressed, detailed preferences and priorities to their carers to ultimately adequately guide them in making future end-of-life decisions.
I find that important. Because now I know one hundred percent what he wants and what it is like. Well, you always talk about it, but what do you do? You talk about it only fleetingly, what you did before. . .always fleetingly at times. You have already thought about what the person wants but now you know it in black and white. (carer 12, mother)
Patients found it reassuring to have their end-of-life wishes defined but also respected.
And he says to me: ‘Mum, everything will be done the way you want it. No one decides anything else. I make sure of that.’ And that is important to me. That’s all I need. Yes. That’s all I need. (Patient 3, female)
Clarification of matters and anticipatory end-of-life planning in the patient’s best interest relieved the burden on relatives who had previously found themselves unprepared to be confronted with difficult decisions for another person.
Yes, we were just glad that it was done. When the time comes that everything is settled. It makes you feel calmer inside to put it that way. It’s satisfying. (Carer 10, husband)
Supporting health-care proxy
Guidance on patients’ wishes led to a perceived strengthened position in patient advocacy among caregivers and a readiness to enforce the patient’s interests if necessary.
And we probably won’t have any big problems with that. Because it is clear what [patient’s name] wants in his directive and no one can shake it. That is what [patient’s name] demands and that is what will be enforced. (Carer 8, brother-in-law)
However, some carers felt the burden of responsibility that comes with being appointed as surrogate decision-makers.
Yes, it’s a lot of responsibility that
Thematic introduction
Many participants perceived end-of-life discussions initiated by the intervention to be completed and only gave little space in everyday life to end-of-life topics.
But we didn’t talk about it that much because we had already talked about everything before. Because when the three of us including the facilitator came together, we had already started talking. So we did talk with each other and afterwards we didn’t need to talk that much because everything was already clear. (carer 12, mother)
However, some participants felt empowered by the psycho-oncological interventions to more easily pursue end-of-life conversations with their loved ones.
Somehow there were reservations and through these conversations with [facilitator] I was able to talk about it better with my relatives. . .that you simply face the subject more openly. Myself, for myself it was like that, and through that with my relatives as well, as I said, because he gave me tips or showed me ways or suggested [. . .] That makes it easier, that has a tremendous influence on the life I have now. (Patient 11, female)
Societal readiness
Spreading the idea
Without exception, all study participants gave a final positive assessment of the intervention and recognised it as a suitable and useful concept to deal with and plan for disease progression.
Well, it did something for me. For my mental side. And also for my knowledge around it. But these are things, if you don’t have anything to do with the subject, then you don’t come to some things logically. The whole thing was positive, really good. (Patient 8, male)
Participants expressed the effort to carry the idea to the outside motivating others to engage in advance care planning.
I would definitely recommend this to others. I have a friend who also has breast cancer for the second time. She was with us the other day, so we asked her: “Do you have one?” (Carer 10, husband)
Carers’ motivation for advance care planning
Newly gained insights from discussions had direct implications for carers’ readiness to make health arrangements for themselves. Most carers felt enabled to determine their own priorities and encouraged to create their personal advance directives.
Well, it raised the idea [. . .] in the family, that we will also make an advance directive. And that way we can make sure that we won’t vegetate. (Carer 8, brother-in-law)
Discussion
Our findings provide valuable insights into patient and carer perspectives on the effects of an innovative advance care planning-intervention on communication and relationship dynamics within and beyond end-of-life discussions. Indisputably, the approach was favourably evaluated by all participants but two main conclusions need to be drawn from our qualitative study. Firstly, psycho-oncological access to advance care planning strengthens readiness for advance care planning-discussions by contributing to a comprehensive preparation of patients and relatives for end-of-life decisions. Secondly, it may help to explore psychological barriers, but also to differentiate between therapeutic support needs and autonomous decisions that hinder readiness to engage in end-of-life decision-making.
There is firm evidence that advance care planning increases the completion of advance directives and the occurrence of end-of-life discussions. 5 In our study, the collaborative approach particularly strengthened action and content readiness supporting a logic model of key mechanisms for successful advance care planning for advanced cancer patients. 30 Moreover, in addition to bolstering individual readiness, positive effects on societal readiness have been reported. Societal engagement with the concept, in turn, suggests a reinforcement of individual readiness.
For promoting higher patient readiness, some organisational, informational, communicative, and emotional barriers had to be addressed. In line with earlier research, our study demonstrated that open communication was connoted positively by most participants, 31 but seemed to be enhanced by building a sustainable relationship with the facilitator through the psychological pre-sessions. The successive exposure (step-by-step ‘getting in touch’ technique) to dignity-based and cognitive behavioural interventions enabled most patients and caregivers to engage in advance care planning-discussions. We contribute to the evidence for conventional advance care planning-interventions that gaining new information and thought-provoking insights was highly valued by participants as it empowered them to make informed decisions and to acquire some sense of control over their medical future. 31 Besides, discussing and disclosing values and care preferences with surrogates, relevant patient-centred constructs in advance care planning, reassured patients that their best interests will be adequately served at the end of life.32,33 Furthermore, they hoped to remove a burden from their relatives and make it easier for carers to assert their priorities. 33 Most carers did feel relieved by patients’ documentations, but some sensed a weight of responsibility that comes with the task.
In addition to facilitating decision-making, many participants reported a consolidation of empathic intrafamilial communication, a promotion of psychological processing, and ultimately coping with the disease as a result of the intervention. This can be assumed to be an effect decisively attributed to the collaborative approach, which on the one hand strengthens individual resources in the disease process, but on the other hand also aims to reduce communicative barriers.
Interestingly, patients’ rationales behind and attitudes towards decision-making often differed fundamentally from carers’ views which does not only seem to apply to the novel intervention but adds new insights on patient decision-making concepts to the existing literature for advance care planning. Of particular relevance appeared contrasting perceptions concerning the carer’s influence on decision-making. Though many carers considered themselves part of a shared decision-making process, carers’ participation was not necessarily required to establish content readiness since patients mostly regarded their decisions as independent and uninfluenced by their relatives. These results build on earlier research finding that patients often saw no need for relatives’ involvement in decision-making and tended to participate alone in the advance care planning-process. 33 The fact that, nonetheless, patients considered relatives’ participation – as required by our study design – positive could be owed to patients’ desire to prepare their relatives for their role as advocates. 34 Despite the discrepant perceptions of the carer’s role in decision-making, the concept seems to be useful in providing the opportunity for patients to communicate wishes openly and to provide reassurance that these will be followed. Additionally, carers benefit not only from information gain but also from the feeling of participation and empowerment to make end-of-life decisions in the patient’s best interest.
Despite our intervention, some patients faced challenges in establishing content readiness as previously described for standard advance care planning-interventions. 13 Although all patients agreed to participate in the study after being informed about the rationale and intervention itself, some did not feel ready to make far-reaching decisions for all end-of-life scenarios. Psycho-oncological assessments within the collaborative approach may assist to determine if impaired readiness is rooted in considered autonomous decision-making that ought to be accepted or in psychological barriers that may be addressed therapeutically. Despite the additional psycho-oncological support offered, the collaborative approach may not generally succeed to alleviate end-of-life discussions for all patients. This evidence on impaired content readiness could provide arguments to advance care planning-critics, who fear that respect for patient autonomy will turn into a new paternalism that exerts pressure on people to make binding statements about impending treatment scenarios. Care teams must thus self-critically reflect upon their own plausible aspiration for certainty in end-of-life decision-making through advance care planning to avoid unreasonable demands on patients feeling reluctant to make provisions for health crises. 35 Hence, psycho-oncological interventions for patients with limited readiness should first target stress issues of primary concern to the patient before confronting them with end-of-life decisions. Nevertheless, even if patients choose not to engage in end-of-life decisions, insights gained could potentially inform carers about motives and thus equip them for reasonable proxy decision-making.
Strengths and limitations
This qualitative approach provided cancer patients’ and carers’ perspectives on a new intervention that could not have been captured by quantitative research. Nevertheless, our findings may have been influenced by a unique sample comprising participants that were willing to engage in lengthy conversations but also in a time-intensive mixed-method study. It is therefore conceivable that less committed pairings would have reported psycho-oncological sessions having mitigating effects on readiness. Furthermore, our methodology did not allow us to elaborate the sub-interventions’ impact, so that only the overall effect of the collaborative advance care planning-approach could be assessed instead of distinguishing individual benefits of the sessions. Thus, general effects of advance care planning were certainly also recorded, which cannot always be clearly delimited from the collaborative intervention.
What does this study add?
Our qualitative study revealed that the collaborative advance care planning-approach had an impact predominantly on action and content readiness. Even though the intervention might require more time and human resources, it could serve as a precursor to end-of-life conversations and increase the number of reliable advance care planning-discussions. It may further identify individuals with a need for psycho-oncological support beyond collaborative advance care planning to establish readiness. In lower-resource settings, screening for psychological barriers to advance care planning could narrow the target population and thus promote feasible implementation. Quantitative data from our mixed-method study on patients’ and carer’ quality of life, levels of distress and depression as well as communication barriers will complement our results to thoroughly evaluate the effects of the collaborative advance care planning-approach.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211043209 – Supplemental material for ‘It was like taking an inner bath’: A qualitative evaluation of a collaborative advance care planning-approach
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211043209 for ‘It was like taking an inner bath’: A qualitative evaluation of a collaborative advance care planning-approach by Anna J Pedrosa Carrasco, Martin Koch, Teresa Machacek, Anna Genz, Svenja Herzog, Jorge Riera Knorrenschild, Pia von Blanckenburg and Carola Seifart in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163211043209 – Supplemental material for ‘It was like taking an inner bath’: A qualitative evaluation of a collaborative advance care planning-approach
Supplemental material, sj-pdf-2-pmj-10.1177_02692163211043209 for ‘It was like taking an inner bath’: A qualitative evaluation of a collaborative advance care planning-approach by Anna J Pedrosa Carrasco, Martin Koch, Teresa Machacek, Anna Genz, Svenja Herzog, Jorge Riera Knorrenschild, Pia von Blanckenburg and Carola Seifart in Palliative Medicine
Footnotes
Acknowledgements
Our sincere thanks go to Katharina Nagelschmidt and Nico Leppin for their support in delivering the intervention.
Author contributions
C.S., P.B. and J.R. conceptualised, planned and supervised the col-ACP-project. C.S., P.B., J.R., M.K., S.H., T.M. and A.G. developed the qualitative interview guide. T.M. and A.G. conducted the patient and carer interviews. A.P., M.K., T.M., S.H. and C.S were involved in the qualitative analysis of data. A.P. drafted the manuscript. All authors provided critical comments on drafts of the manuscript and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The whole project was funded by the German Federal Ministry of Education and Research (funding-ID: 01GY1708).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.