
Abstract
Background:
Understanding what makes a ‘good death’ in the child with life shortening illness is important, as it informs appropriate and effective end-of-life care. Above play, peer contact and opportunities for assent, prior literature review found meeting needs and managing control were critical. The influence of disease types, location of death and palliative care support remains unclear.
Aim:
Explore how a good death for children can occur in the real-world context and identify factors influencing it.
Design:
A qualitative multiple-case study. The case was defined as family and professional caregivers of children who died, stratified across disease categories (cancer or non-cancer) and palliative care contact. Data collection included (1) interviews, (2) artefacts, (3) clinical notes. Framework Analysis facilitated in-depth within and cross-case analysis.
Setting/participants:
Singapore health-care context. Respondents included bereaved parents, health and social care providers from hospital, and a community palliative care service.
Results:
Five cases were constituted, with eight parents and 14 professionals as respondents. Eight common themes were identified, sub-categorised under three domains and interpreted theoretically: (1) Antecedents: Letting go, Acknowledging the child, Closure (2) Determinants: Suffering, Control, Systems and processes (3) Attributes: Comfort, Dying not prolonged. These factors were consistent across all cases, regardless of individual diagnoses, place of care and palliative care access.
Conclusions:
Elements that universally influence a good death are revealed within an ecologically sound and holistic conceptual framework. The impact of attitudes among healthcare professionals, and service delivery at systems level highlighted in this study have immediate applications in practice and policy.
● Perceptions of a good death in adults with life limiting illness may not apply to children ● The dying experience between children with different diagnoses has not been compared ● Evidence is mixed on the individual impact of dying at home and palliative care in paediatric literature
● Commonalities exist in the caregiver experience among children dying from different life shortening conditions ● A good death in children bears unique qualities around comfort, and where dying is not prolonged ● Elements like control and closure for example, at personal and systems levels, ultimately determine the quality of dying and death
● Caregivers perceive that no matter what age or ability, priorities of the child should become central during this period ● Letting go by caregivers is strongly associated with ceding control, with both resulting in minimised overall suffering ● A ‘supportive’ environment that keeps the family together brings the most ‘comfort’
Introduction
The World Health Organisation reported that 6.3 million children across the world died in 2017. 1 More than half had serious medical conditions that resulted in premature demise. 2 Death occurs nowadays in very complex patients, often on intensive care, within a societal culture that has unrealistic expectations of what medicine can do.3–5 Other than escalated healthcare expenditure, wider implications of systemic factors on the individual experience have not been extensively explored. When the underlying illness proves refractory to treatment and the child is expected to die, though at first counter-intuitive, a good death often becomes the common goal for all stakeholders involved.6,7
There has been considerable debate in adult literature on the notion of a good death in the medically ill and the ramifications this has for care. Six major components were thought to constitute a good death in adults. 8 Notwithstanding commonalities like physical suffering and family grief, there are fundamental differences in the clinical and social contexts between the dying child and adult. 9 Specific to children with life shortening illness, our integrative review synthesised paediatric evidence and rendered theoretical propositions for a good death occurring within a healthcare ecosystem: (1) Individual needs, the total experience, and control between preservation and letting go add to give a sense of suffering; (2) Perception of a good death is enhanced when this suffering is reduced. 10 Multiple stakeholders are impacted, like parents, siblings, grandparents, not forgetting professional caregivers, who together form an intimate network around the child. 11 The attributes of a good death in children have not been well described empirically. Ito et al. 12 identified 13 characteristics of a good death for Japanese children with cancer. Unique themes include opportunities for play, peer support, assent, and the child not being aware of impending death. There is currently mixed evidence on terminally ill children dying at home and the benefits of paediatric palliative care, yet assumptions around their influence on quality of dying are prevalent.13,14 Lastly, the experiences of the family with a child dying from cancer and that of a non-cancer condition can differ, even if themes of grief and loss are common.15,16
A contemporary and contextualised study of the experience associated with a child dying from any serious medical condition, that takes into consideration broader structural, cultural and societal factors, over and above individual stakeholder perspectives is hence timely.
Method
Research question: How and why can a good death be achieved in a child with life shortening illness, from the perspectives of family and professional caregivers?
Design
A qualitative multiple-case study design,17,18 with Critical Realism as ontological foundation. Critical Realism facilitates understanding of a multi-dimensional social phenomenon within a complex system, focusing on ‘structures’ with hidden ‘forces’ that drive events, while uncovering experience and meaning at stakeholder levels. 19 Hallmarks of case study research applied here: a deliberate process in selecting cases, triangulation of data from multiple sources, and search for disconfirming evidence. 20
Study setting
The study was conducted in one children’s hospital in Singapore. It does not have an in-house specialist paediatric palliative care service. Before their death, children with life shortening conditions were mostly cared for either in the oncology or intensive care wards. The rest died at home. They might receive end-of-life support from the country’s only community paediatric palliative care service. Charity run, its diverse services include home visits, allied health inputs, in-home respite, out-of-hours support and bereavement care. There were no dedicated inpatient children hospice resources in Singapore at the time this study was conducted. There has not been any strategy document or guidance for paediatric palliative care, as it is still a developing subspecialty locally.
Sampling multiple cases
What makes a ‘case’ has been variably defined.18,21,22 It is in essence an integrated ‘system’ with a ‘boundary’ and ‘working parts’. 23 In this study, it refers to a child with life shortening illness in the last months of life, supported by caregivers (both professional and informal) within the health and social care system. The phenomenon in focus is good death.
Four to eight cases were anticipated for maximal variation, 24 sampled against key factors influencing the experience of dying: cancer or non-cancer diagnoses; access to specialist palliative care. 25 Data saturation and patient availability determined the final number. Key criteria for case selection: (1) Child’s age between 1 and 18 years at time of death; (2) Suffered from a life shortening condition, either cancer or other diagnoses in Association for Children’s Palliative Care categories; 26 (3) Died between 6 and 24 months before (to minimise distress and capture contemporary experience).27,28
Sampling respondents within cases
Two categories of respondents were sampled: formal and informal caregivers. At least one participant (up to four) from each category must be recruited to make a case. Key criteria for recruitment: (1) Cared for the child 1 month before death; (2) Above 21 years of age; (3) Could give consent and spoke English. With data collection planned after death, the dying child’s perspective was solicited indirectly through caregivers.
Recruitment of respondents
Primary physicians were first contacted about the study. Invitation packs were sent through them to informal caregivers, with instructions to contact the study investigator (PHC) if they were interested to participate. Family caregivers were asked to suggest other caregivers as respondents. Once data collection with at least one family caregiver was performed, interviews with primary physicians followed. They were similarly asked to suggest other healthcare providers as respondents.
Multi-source data collection
In-depth, semi-structured interviews (audio recorded with an encrypted device) were conducted by PHC. Prior written consent was obtained. PHC performed verbatim transcription, while CW and SH audited in portions for accuracy. Field notes were one of multiple sources of data. A research journal documented emerging ideas. An interview guide informed by study objectives was used. This underwent iterations as data were analysed. Interviews occurred within a 12-month period (July 2017 to August 2018). PHC accessed documents ahead like case notes, care plans and do not resuscitate (DNR) forms for milestones or sentinel events around the death to anchor and deepen discourse, yet not making prior assumptions. Before interviews, family caregivers were asked to bring photographs, videos or other physical items left behind as keepsakes. Their associated memories or meanings were explored at interviews.
Data analysis
Framework Analysis 29 incorporated both case and theme-based approaches. Broadly, case-oriented analysis examined relationships among variables within a single case, followed by comparisons across cases in search of similarities, patterns and divergent views.30,31 Specific to case study research, Yin 18 detailed a two-stage process: Pattern matching locates associations between study findings to propositions or framework 21 drawn from literature review or theory within a case. 32 Theoretical replication compares findings from one case with another, again guided by the a priori conceptual framework, which is developed further. Without relying on large or representative samples, ‘sophisticated descriptions and powerful explanations’ are produced, that are not only readily generalisable but also high on ecological validity (richly contextualised and hence translatable). 33 The copious and varied data were managed using NVivo (version 11) qualitative data analysis software.
Ethical considerations
Ethics approvals were obtained both in Singapore (1 Sep 2016, National Healthcare Group DSRB reference: 2016/00720) and at the Faculty of Health and Medicine Research Ethics Committee in Lancaster University, United Kingdom (7 Nov 2016, reference: FHMREC16012). Though never used, access to a counsellor was provided to all respondents. Power influence by the senior clinician-investigator (PHC) was minimised, ensuring direct care had not been provided previously (respondents informed), and reiterating to professionals, particularly those of lower grade, that study participation was entirely voluntary. Besides regular meetings with supervisors (two co-authors), potential biases and risks of being an ‘insider researcher’34–36 were managed reflexively throughout. 37
Results
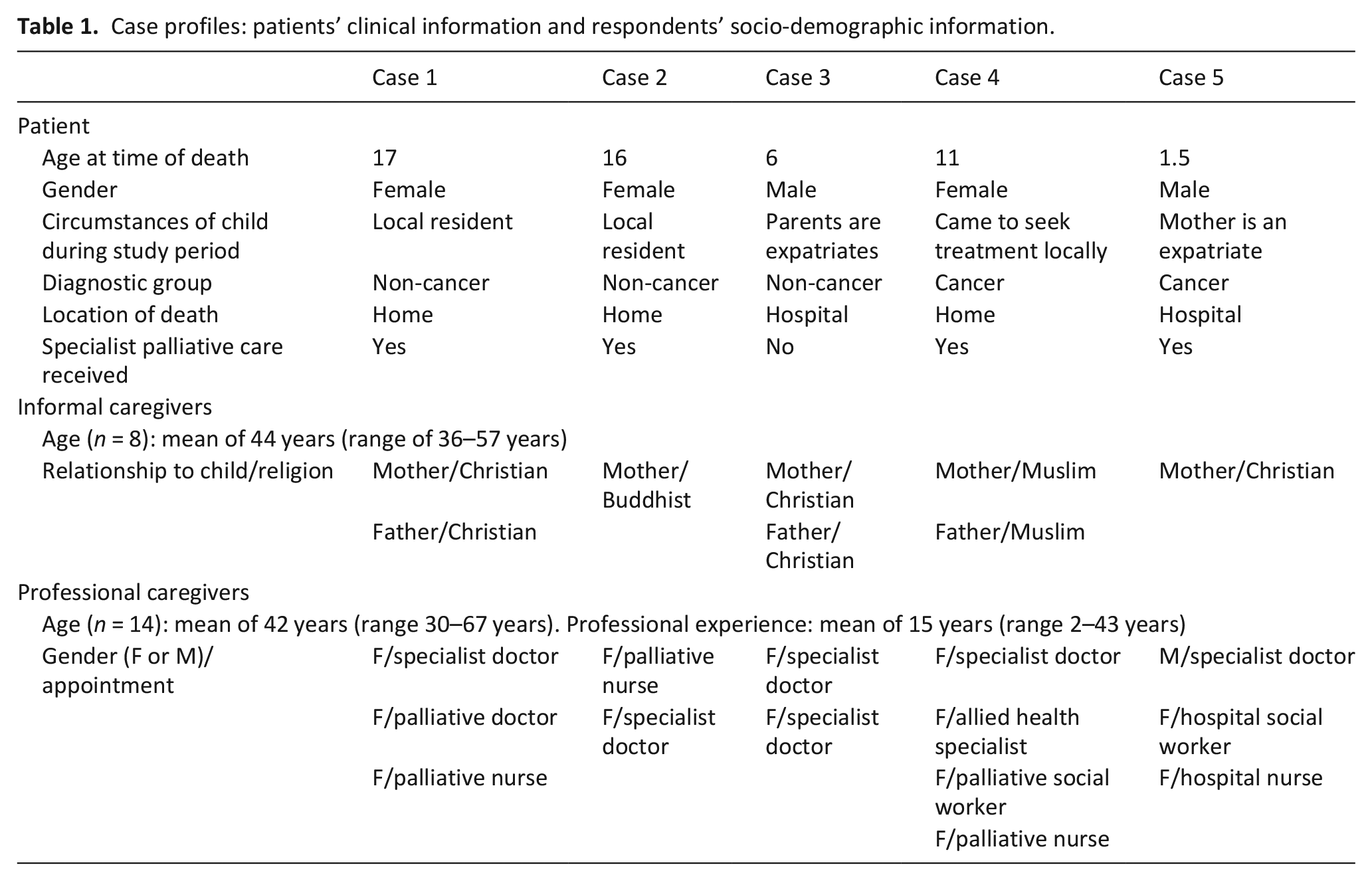
Five cases that included twenty-two interview respondents were assembled, with heterogeneous data generated. Two families approached failed to participate. One remained uncontactable after sending a reminder while the other family changed their mind. Relevant information collected are summarised in Table 1. Informal caregivers interviewed (n = 8) were all parents. One father did not want to participate (case 2) while the other was in conflict with the mother solely responsible for the child’s care (case 5). Though up to four in a family could participate, these parents had not suggested other informal caregivers as suitable respondents. Each interview lasted a mean of 87 min (range of 57–111 min). All except one multi-disciplinary healthcare professionals (n = 14) were female. Their interviews lasted a mean of 62 min in duration (range of 44–79 min).
Case profiles: patients’ clinical information and respondents’ socio-demographic information.
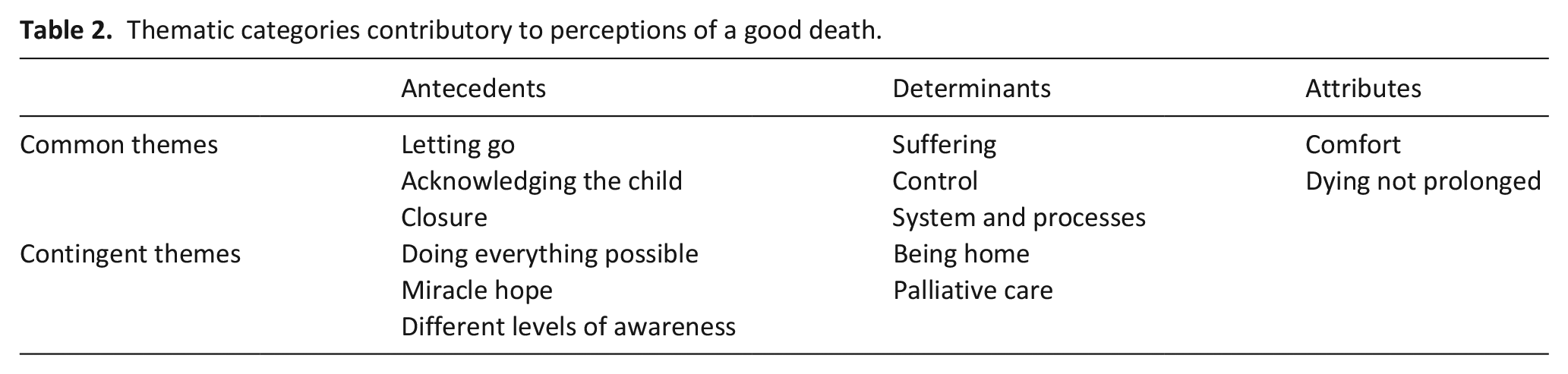
Cross-case analysis revealed eight common and five contingent thematic categories (Table 2). Common themes were universal across all cases in their salience; contingent themes, though equally relevant, applied only in a subset. All themes were further grouped under three domains, based on their relationship with a child’s death. An antecedent here refers to any event, object or phenomenon that precedes death. Determinants refer here to factors or agents that directly or indirectly influence the outcome of death and dying. Attributes refer to the intrinsic nature of what is perceived as a good death. Consistent with the aim of this paper to uncover elements of a good death across all life shortening conditions in children, only common themes are discussed here.
Thematic categories contributory to perceptions of a good death.
Antecedents
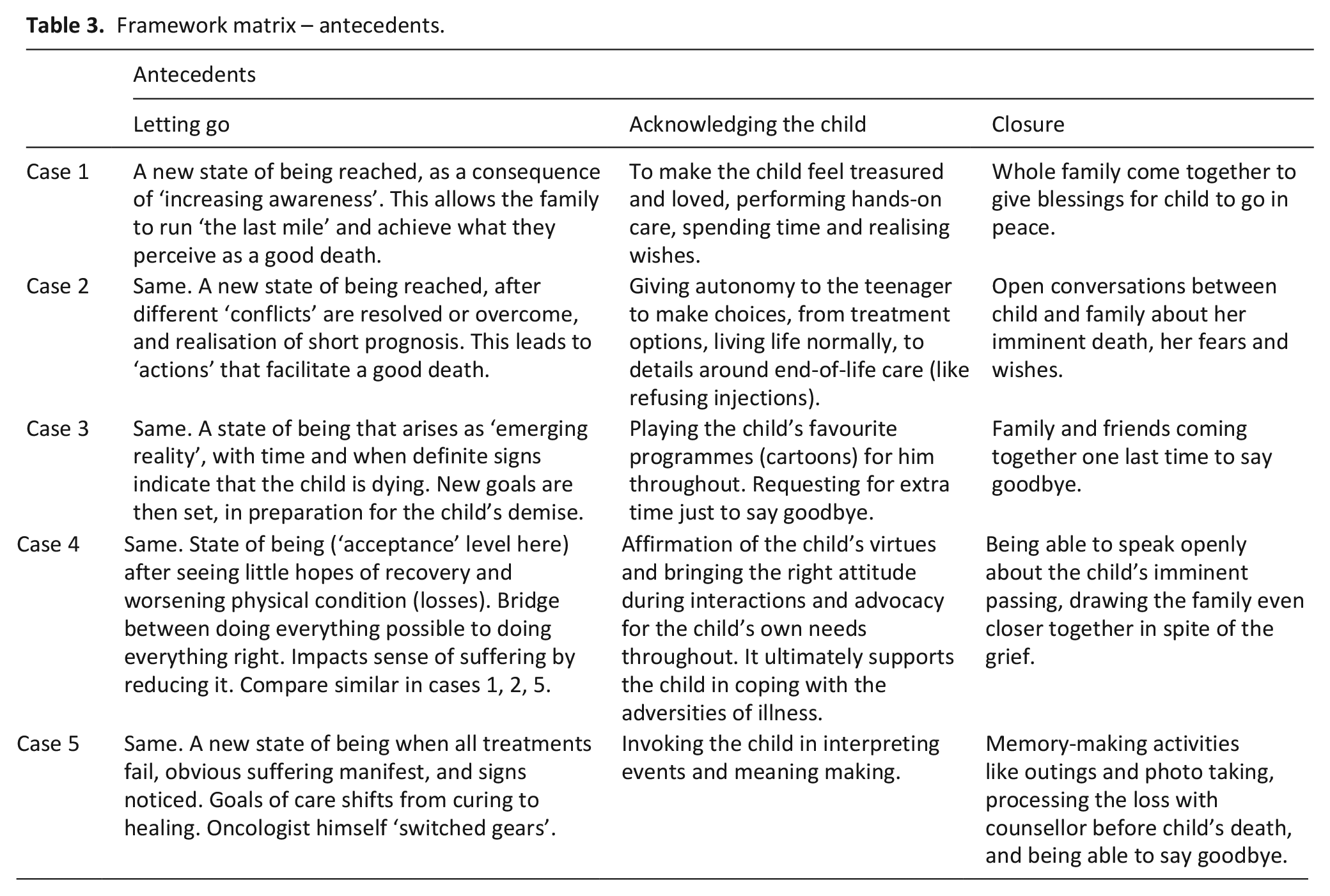
Three common themes are grouped under ‘antecedents’; individual narratives specific to each case are represented in Table 3.
Framework matrix – antecedents.
Letting go
This signified a turning point in the dying trajectory, where stakeholders (parents or professionals) reached a new state of being with developing insights that the child’s condition was worsening. It could be triggered by personal observations after frequent admissions or upon noticing signs of disease progression; alternatively, having assimilated information from doctors leading the care. Letting go was like a bridge between doing everything possible and doing everything right, with considerably positive outcomes. ‘In his [father] shift to palliative care, although I offered it, it took some time . . . He wants to be absolutely sure that he has explored everything, before he went down that road’. (oncologist in case 4). Letting go ultimately reduced suffering. This could occur after experiencing suffering or as a prelude to minimising suffering. ‘Maybe last half the year, when she has very frequent fever . . . Most of the time, she’s sleeping. Drowsy, because of medicine, fever . . . I think she has quite frequent diarrhoea, which is like, almost, can be eight – nine times per day . . . I think that’s the max that, I think, she’s [voice cracks] I mean as a child?. . . It’s like, so much suffering’. (mother in case 1).
Acknowledging the child
This applied whether the child was non-communicative (case 1), very young (case 5) or unresponsive (case 3) and more so, if older and self-determining. ‘Because throughout the treatment, the parents’ wishes prevail. But in the end – that they should consider what the child wants’. (oncologist in case 4) Respondents argued that the child ought to be central in all things, particularly when prognosis became guarded (estimated in weeks to short months). ‘One thing is very important – if this type of situation comes, make her understand, that she is the special one. It is very important because, maybe you cannot get another chance’. (mother in case 4). Acknowledgement might be achieved in various ways; making the child feel treasured and loved, or providing them the autonomy to make treatment choices. This enhanced the child’s coping at a time of many losses. ‘Yeah. So, only when we talk about these happy memories [child’s achievements] – I think it took that time away. It created a bubble, I guess, for that – for that moment of being happy and being able to – talk about things’. (social worker in case 4).
Closure
This was likened to a ‘send-off’ that all families performed. ‘In fact, she hold out for 1 month . . . There must be something holding up . . . We, as a family . . . We have to be together, and wish her the best . . . We actually, come closer together. We no more argue, we do not, we just do our good thing, we support. And we always come to say: ‘Freya, you need to go. You go’. (father in case 1) Conversely, closure was tacit in the perceptive child, when unusually serious conversations conspired. ‘Father was able to discuss with Alina about death and dying . . . ‘You should feel lucky, because – when you are dying, your parents are beside you, and looking after you. You know, when baba – it’s time for Baba to die, I’m not sure my parents will be there to hold my hand.’ . . . So therefore, the last few weeks that she had gotten with the parents is no longer a very burdensome period, but it’s more like – a gift’. (palliative nurse in case 4). Rather than an act of separation widely associated with conventional notions of closure, stakeholders drew closer physically, emotionally and spiritually. It appeared to be supportive in bereavement too, as memories of ‘farewell’ activities and conversations were reminisced.
Determinants
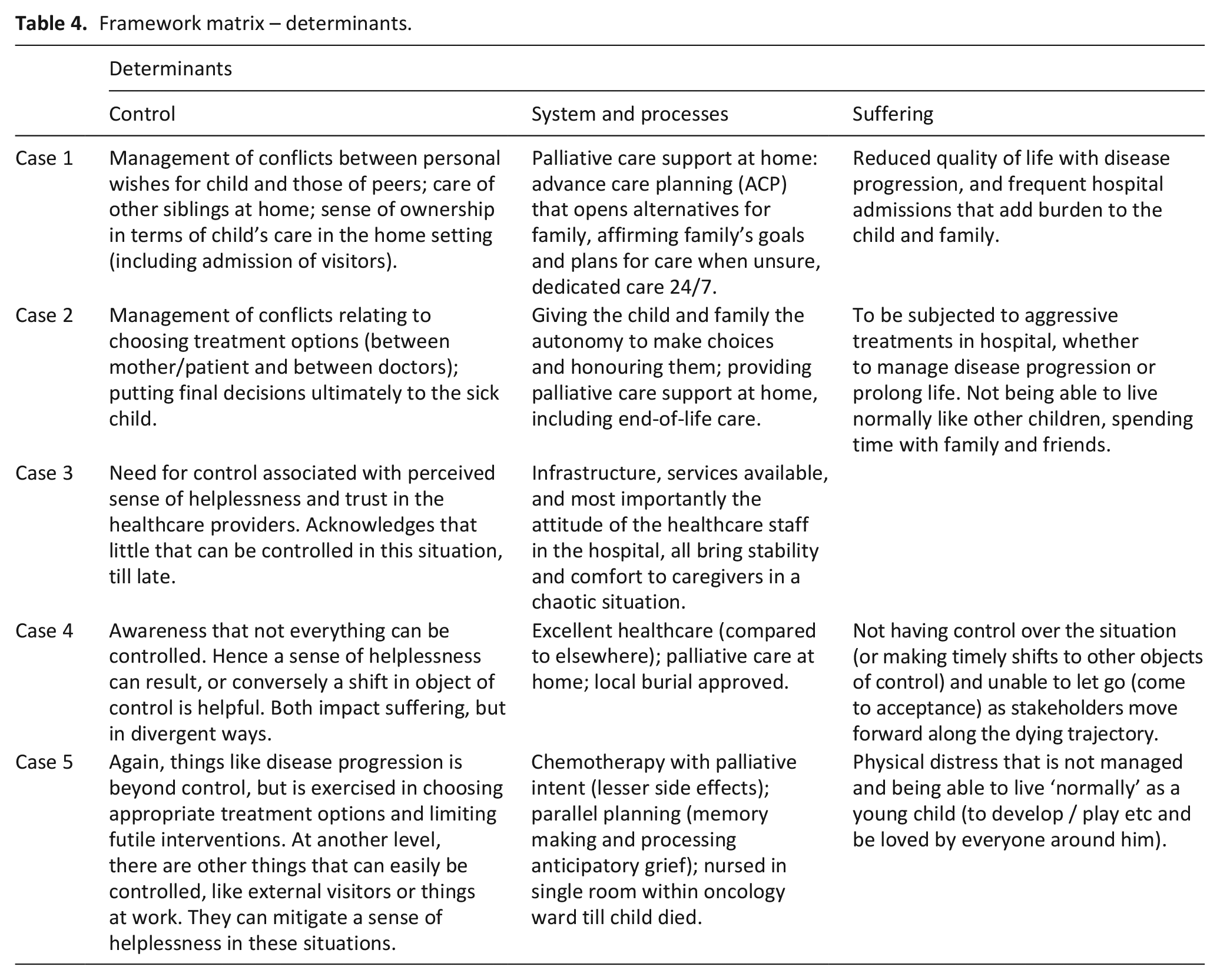
Three themes were grouped under ‘determinants’ (Table 4).
Framework matrix – determinants.
Control
This surrounds mastery over conflicts. The dying child posed a special type of conflict to all stakeholders, family caregivers or healthcare professionals alike. With control slipping as the child deteriorated medically, this produced a sense of helplessness that revealed another facet of suffering. ‘[Her daughter’s prayers to wake up being able to walk were not answered] That time, I’m just feeling . . . Most helpless person in the world. I couldn’t do anything . . . My one and only daughter, she just wanted some assurance from me!’ (mother in case 4). When futility of averting certain death was acknowledged, the sense of helplessness and burden of suffering reduced. This was achieved in one of two ways – resignation: ‘At the beginning . . . They want things all out, and then up to a point, they see that, you know, even you do more, you don’t get better benefits. And so they will withdraw’ (neurologist in case 1) or acceptance, processing challenging situations over time at both cognitive and emotional levels: ‘At some point, there has to be a full stop. It’s just where your full stop is. Uh, and whether you are willing to accept that’. (neurologist in case 3). In the interim, two simpler measures helped; shifting object of control to something else, or just trusting doctors to do their best.
System and processes
This theme referred to material and non-material ‘structures’ (described in Critical Realism), with attitudes of providers specifically highlighted by parents. Examples of material structures included hospital emergency department and the community palliative care team. Non-material structures referred to services like good oncology care and 24/7 medical support at home. Whether structural or attitudinal, aspects of systems and processes engendered two positives – stability and comfort. A sense of stability was supportive, when uncertainty and chaos were rife. ‘We were the people who cared for him, from the beginning until the end of his life . . . So, in terms of the plan, it was always Dr T [intensivist] and myself, right. We did try to sit down with the family, for several family conferences, I mean, these were . . . perhaps frequent enough . . . we always touched base, and we knew what we were saying for the patient’. (neurologist in case 3). Comfort that is outside the physical realm was equally precious. ‘In a moment of difficulty in the last day, Dr A was 10-min phone call away. That matters to us . . . But the *urge* I saw in her, in her expressions. That matters to us . . . The very comfort it creates, at that second, for everybody’. (father in case 4). In contrast, there were apparent gaps and areas that did not work well. ‘They came in with a packet, and it was basically Daniel’s skull . . . And he said, ‘Do you want this?’ And I asked, ‘What is it?’ And he said, ‘It’s the skull.’ And I was like, ‘Well. You know, what do I do with it?’ I said, ‘Do I keep it for later, when we do the repair surgery?’ . . . And he kind of looked at me, like he didn’t know what to say . . . When you look back, you go, ‘He already knew that Daniel was not going to make it.’ (mother in case 3). Blindly following routine procedures to return personal items like implants or lumps removed from the body certainly went very wrong here.
Suffering
Beyond common notions of physical suffering, nuances in the interpretation of suffering were noted. Not living normally: Peculiar to the paediatric setting, having opportunities to participate in activities other children the same age engage in was critical. This was perceived as empowering, and not to be derailed by sickness. ‘For a one-and-a-half-year-old, what you really need is to walk and explore, and move around. That’s where they reach their developmental milestones. That’s, the innate nature to be able to do that. And despite his illness, he still had that’. (social worker in case 5). Having recurrent hospitalisations: Mentioned exclusively by respondents from case 1 and 2; the children in both instances had non-cancer conditions. We postulate their journey (and experience) of illness may be different than families with children suffering from cancer. The former survived many prior admissions that took their toll. These families soon began to see hospitalisation ‘routines’ as suffering. Not having control: This narrative was shared only by families of children with cancer (case 4 and 5). The association between control and suffering was discussed previously.
Attributes
The last two common themes were grouped under ‘attributes’ (Table 5).
Framework matrix – attributes.
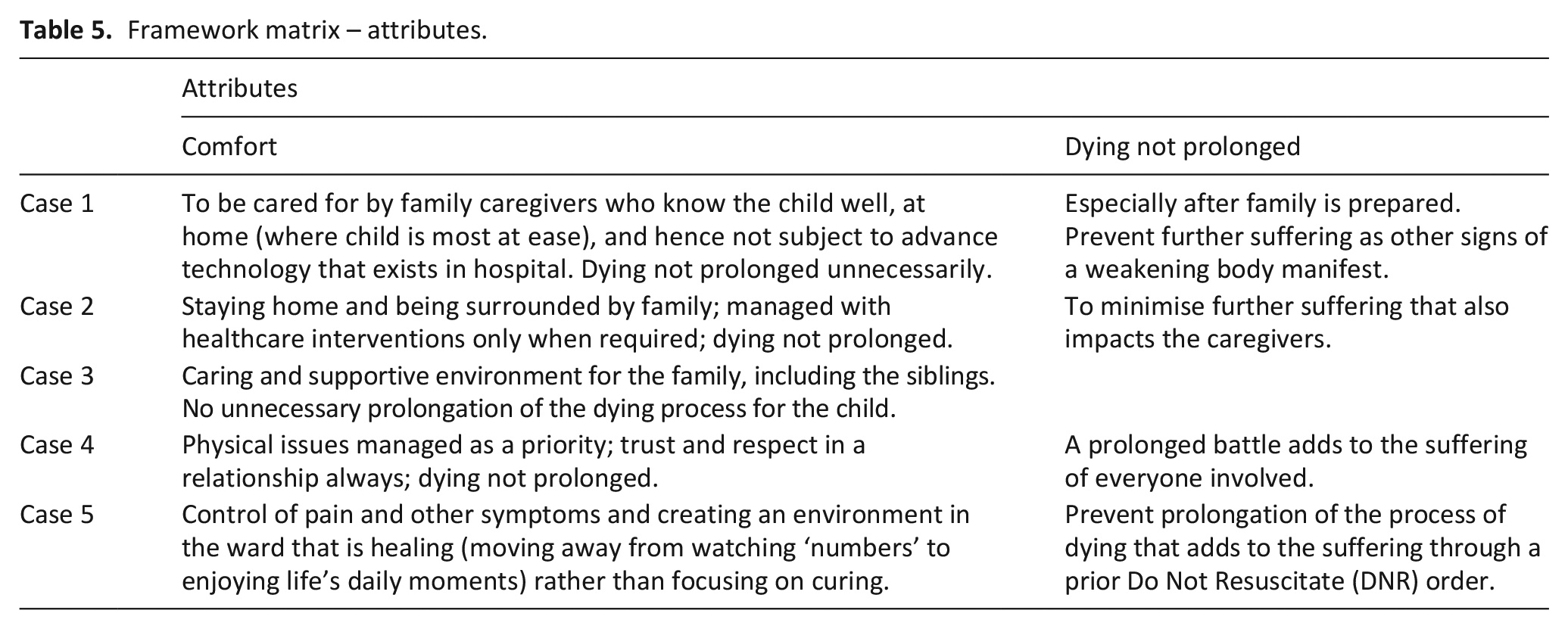
Comfort
Similar to the theme of suffering, narratives of comfort were stratified along disease categories. Close to family: This was best illustrated in case 1 and 2 with children who suffered from non-cancer conditions. ‘We can correspond, by looking at her, her reaction, her sound-calling, her discomfort. We can sense, what is going on. So, by doing that, we know that, what is the next step to support her . . . We know inside out about her’. (father in case 1). Both children eventually died at home. The boy in case 3 (also non-cancer) stayed under intensive care throughout, but his family was always by the bedside. Management of distressing symptoms: For two other children in case 4 and 5 who had terminal cancer, priority from a comfort perspective was focused on active management of pain and other physical symptoms. ‘If the child is having a lot of pain, and then breathlessness is not well-controlled, then I think – we can hardly talk about a Good Death. I think the physical aspect is the priority’. (palliative nurse in case 4). Caring and supportive environment: This came strongly from cases 3, 4 and 5 that had not specifically mentioned staying close to family. The environment in question appeared to be around staff attitude and a ‘comfort zone’ within which these families reside, regardless of location. ‘It is very easy to fill up the child’s mind . . . Just being with her and respecting her . . . When a child is in that situation, right, the question should be, “What environment should be there around” . . . So *create* home, wherever it is’. (father in case 4).
Dying not prolonged
Everyone was unanimous about not prolonging the process of dying, to minimise the suffering that each child and family go through, particularly when the final outcome was certain. ‘I wouldn’t say her death had not been – peaceful, but I would say the prolonged – the prolonged battle with her illness was what was suffering’. (social worker in case 4).
Synthesis of all insights
Two major theories informed iteration of findings at advanced stages of data interpretation: Ecological Systems theory 38 and Trajectory framework. 39 To illustrate the confluence of factors that influenced perceptions of a good death, a diagrammatic representation was created (Figure 1). It highlights the short and unpredictable trajectory that ends in death – one that is perceived to be ‘good’ – for the child with a life shortening condition.
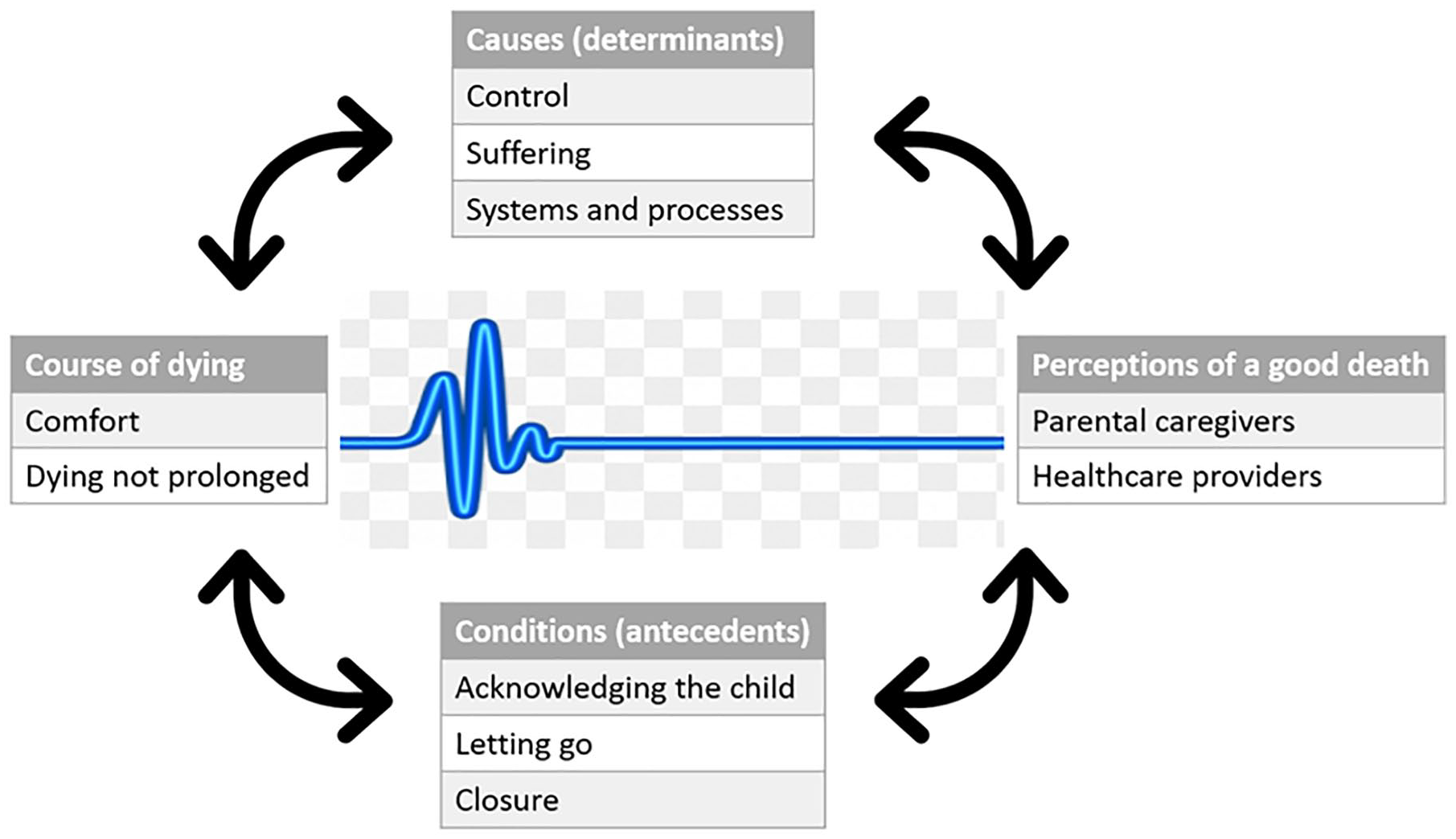
Good Death – a composite perspective from family and professional caregivers.
Discussion
Main findings
This qualitative multiple-case study on perceptions of a good death for children found eight universal elements that shaped lived experience, above individual characteristics like age, diagnosis or care settings. The conceptual framework represented in Figure 1 embraced the confluence of causes, conditions and time. Previous theoretical propositions for a good death, like what constitutes suffering and its impact on the quality of death, are now updated: (1) Characterised by ‘comfort’ and dying that is not prolonged; (2) A function of causes and conditions bounded by time; (3) Influenced by elements at personal and systems level, above case heterogeneity.
What this study adds
No previous study addressed perceptions of a good death in children across both cancer and non-cancer groups. A predominant focus on suffering (mostly in the physical dimension) in related studies as a proxy for good death remains flawed. This study attempts to address those gaps. Reference to a good death is prevalent in the adult setting,40–42 but its application within paediatrics can be problematic. Some perceive a child’s death as unnatural and could never be good. 43 Prior reviews on a good death in a similar group of children either drew heavily on adult literature 43 or focused on a specific group like cancer. 44
Published more recently, our review reported the ‘sphere of influence’ model for a good death; it depicts a dynamic and multi-layered ecosystem that incorporates different elements (needs, experiences and control) and players (patient, family caregivers and professionals) within a space bounded by the healthcare setting. 10 Despite rendering a comprehensive overview of a good death, the sphere of influence model did not capture the journey of illness that precedes death. It is a period which appeared to strongly influence stakeholder perspectives. The latest construct consists of eight definitive elements classified within antecedents, determinants and attributes that operate along what stakeholders perceived as an uncertain and fluctuating course. Instead of a fluid balance between three levers (needs, experience and control) adding to suffering that in turn informs quality of death, the relationships and associations between factors are now made explicit. Not only are elements like ‘control’ and ‘letting go’ refined, new dimensions like ‘acknowledging the child’ and ‘closure’ are revealed. The overarching concept within the sphere of influence model that recognises the influence of physical and socio-cultural ‘structures’ on events, experience and sense-making now has its own place as ‘systems and processes’ under determinants.
Findings grounded in the real-life context took into account systemic factors, both structural and social, that influenced events and ultimately impacted experience. This expansive yet situated understanding is sensitive to individual history, culture and time, even as circumstances evolve rapidly along each dying trajectory. Underpinned by the ontological paradigm of Critical Realism and informed by concepts within Ecological System theory 38 and Corbin and Strass’ Trajectory framework, 39 the ecological validity of study findings fosters vicarious knowing among practitioners, and would be instructive to service planners at policy levels.45,46 Deconstructing a good death to expose common intervening causes and conditions revealed areas within healthcare that professional caregivers and policy makers can immediately address, like efforts to acknowledge the child at this time and providing 24/7 medical support at home.
Strengths, weaknesses and study limitations
A robust, yet flexible case study methodology47,48 was adhered to throughout. Multiple perspectives 49 from five purposively created case studies, and triangulation of data sources 20 produced rich and detailed empirical data. 50 Parental narratives evoked by the artefact of their boy’s skull bone for instance provided deep insight into process norms as determinants.
Evolving perspectives over time among stakeholders is acknowledged.51,52 This is managed through a narrow study inclusion window of 6–24 months after death. Among informal caregivers, only parental perspectives were eventually obtained. A minimum inclusion age of 21 years might have prevented participation by siblings; and recalling an instance during study recruitment where one parent decided that she would be the only family participant despite her mother’s eligibility as grandparent, we believe some degree of safeguarding may also be contributory. Though predominance of female gender is typical among paediatric providers, it is unclear how having only one male professional caregiver influenced findings. In this study, the ‘voice’ of the child only came through their respective proxies. Any emerging clarity around the good death construct should be seen in that light.
Given a context-dependent phenomenon like good death, study findings here may not appear readily transferable. However, with a research ontology that sits between positivism and constructivism, 53 and conclusions drawn from an empirically strengthened conceptual framework, case-to-case translation (or inferential generalisation) and analytic or conceptual generalisation beyond a single context like Singapore are most valid.54–56
Future research
Researchers across the world can add to still scarce evidence by building on this study’s foundational good death model. Theoretical propositions embedded within, like how a good death is shaped above case heterogeneity by universal elements at personal and system levels, should be expanded through targeted research questions using quantitative or mixed method study approaches, performed on a larger sample across different regions. To obtain a wider family perspective, study invitation letters to parents could specify other stakeholders of interest explicitly, like siblings and grandparents, including enclosing customised information packs for each group. 57 Given its implications on suffering, future studies could explore the theme ‘letting go’ further, including perspectives of the young person if possible. The good death construct here could inform conception of a quality of dying and death measure for children equivalent to the adult version58,59 that has proven useful as an objective proxy measure for a good death.
Conclusion
While some may question if the death of a child can ever be good, this study has identified universal elements perceived by major stakeholders as critical for a good death. If the death of a sick child ever becomes inevitable or anticipated, we now stand better guided.
Footnotes
Acknowledgements
Mr Zhi-Zheng Yeo from the research service in HCA Hospice Care, Singapore supported preparation of the manuscript (in particular its citation management). The first author is grateful for his contributions.
Authorship
PHC conceived the study, obtained ethics approval, collected and analysed the data, and prepared first drafts of the manuscript. CW and SH advised on the research design, audited the process of data analysis, supervised interpretation of findings, and refined subsequent manuscript iterations. All authors approved the final version of the study report submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
As the study formed part of a PhD thesis, ethics approvals were obtained from both the university in United Kingdom and local hospital in Singapore where data collection occurred (details included within the paper). All participants had provided informed written consent before their semi-structured interviews.
Data management and sharing
The first author may be contacted to obtain further clarifications on aspects of the study not provided in this paper or supplementary material, including access to the research protocol or other relevant data, wherever ethically or legally appropriate.