
Abstract
Background:
Hospital-to-home transitions in palliative care are fraught with challenges. To assess transitions researchers have used patient reported outcome measures and qualitative data to give unique insights into a phenomenon. Few measures examine care setting transitions in palliative care, yet domains identified in other populations are likely relevant for patients receiving palliative care.
Aim:
Gain insight into how patients experience three domains, discharge readiness, transition quality, and discharge-coping, during hospital-to-home transitions.
Design:
Longitudinal, convergent parallel mixed methods study design with two data collection visits: in-hospital before and 3–4 weeks after discharge. Participants completed scales assessing discharge readiness, transition quality, and post discharge-coping. A qualitative interview was conducted at both visits. Data were analyzed separately and integrated using a merged transformative methodology, allowing us to compare and contrast the data.
Setting and participants:
Study was set in two tertiary hospitals in Toronto, Canada. Adult inpatients (n = 25) and their caregivers (n = 14) were eligible if they received a palliative care consultation and transitioned to home-based palliative care.
Results:
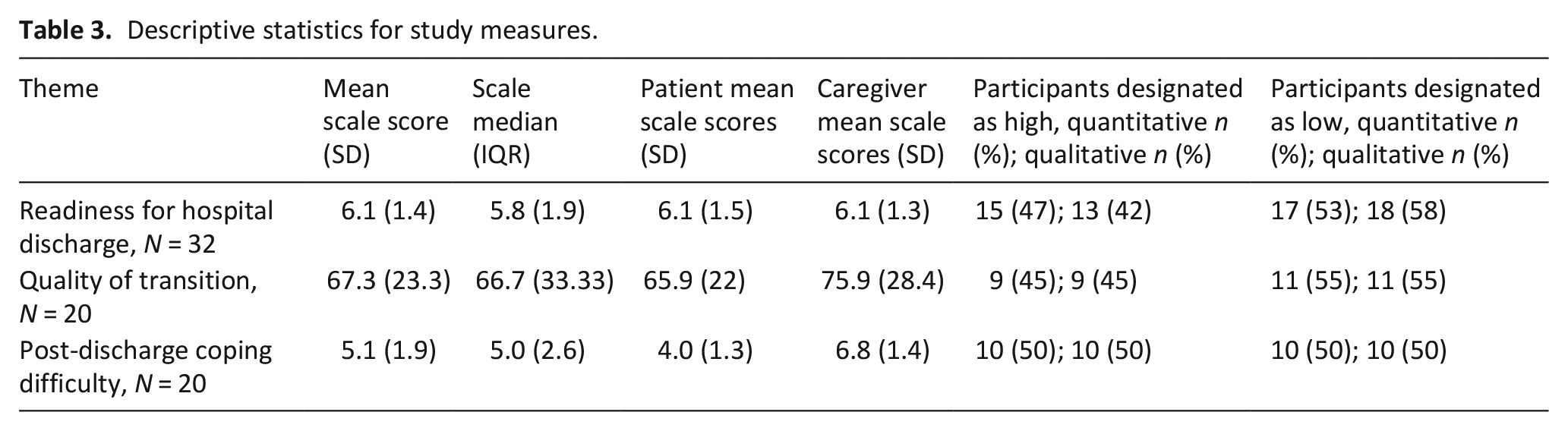
Results were organized aligning with the scales; finding low discharge readiness (5.8; IQR: 1.9), moderate transition quality (66.7; IQR: 33.33), and poor discharge-coping (5.0; IQR: 2.6), respectively. Positive transitions involved feeling well supported, managing medications, feeling well, and having healthcare needs met. Challenges in transitions were feeling unwell, confusion over medications, unclear healthcare responsibilities, and emotional distress.
Conclusions:
We identified aspects of these three domains that may be targeted to improve transitions through intervention development. Identified discrepancies between the data types should be considered for future research exploration.
Keywords
What is already known about the topic?
• Transitions between care settings can be fraught with challenges.
• As a result of the desire to spend end of life at home, a common transition for palliative care patients is from the hospital to the home.
• Researchers have used qualitative methods to assess transitions, identifying challenges in continuity of care, collaboration, and logistics.
• Patient reported outcome measures (PROMs) and patient reported experience measures (PREMs) can add patient and family member voices to evaluations of care quality and their transition experience.
• There are few measures that assess these care setting transitions in patients receiving palliative care, yet domains identified in other populations are likely relevant for palliative patients.
What the paper adds?
• By using a mixed methods study design, the two data types offer complementary insights; the PROM/PREM findings provide structure for better understanding three domains of a transition, whereas the qualitative insights offer explanations and reasons for why or how these findings occur.
• Positive transitions were characterized by feeling well supported, managing medications, feeling well, and having healthcare needs met.
• Challenging transitions involved feeling unwell, confusion over medications, not understanding their health-related responsibilities, and emotional distress.
• By identifying discrepancies between the qualitative and quantitative data, we found that PROM/PREM outcomes may have been affected by participants’ eagerness to go home, not having healthcare needs met, and unexpected reduced capacity once home.
Implications for practice, theory, or policy?
• For each domain of the transition from hospital to home (i.e. discharge readiness, transition quality, and post-discharge coping), the agreement between the qualitative and quantitative data, for both positive and negative outcomes, suggests areas that are clearly important to palliative care patients and/or caregivers in transitions that future interventions can aim to address.
• The identified discrepancies between qualitative and quantitative data indicate areas for future exploration.
Introduction
Transitions of care, the coordinated movement of patients between different healthcare settings, healthcare providers, or intensity of care,1,2 are critical junctures in patients’ care trajectories. During transitions, patients and caregivers may experience challenges including disruption in care plans, lack of communication, uncertainty, and safety concerns.1–4 From a health system perspective, poor transitions can lead to greater health service use, increased likelihood of 30-day readmissions, and higher healthcare spending. 4
To understand transitions, researchers have developed various validated patient-reported outcome measures (PROMs) and patient reported experience measures (PREMs). 5 PROMs/PREMs support patient-centered care and enable the assessment of quality of care over time.6,7 Multiple reviews have synthesized domains of care transitions, with measures to identify patient safety during a transition,2,6,8 coordination of care,9,10 quality of the transition,11–13 and continuity of care.10,12 Yet, few of these assess a transition in care settings, and none assess these in patients receiving palliative care. As a result, the literature in palliative transitions focuses on the impact of palliative care on health service utilization; assessing discharge support, readmissions, and costs.14,15 This focus overlooks qualitative findings highlighting the importance of continuity of care, coordination and collaboration, and clear logistic support.16,17
Palliative patients are likely to experience many transitions in care settings because of their serious conditions, 18 a common one being from hospital-to-home.19–22 The lack of validated PROMs/PREMs makes measurement of transition outcomes difficult in this population. Validated measures have been developed for other populations to capture domains of transitions relevant to hospital-to-home transitions, namely discharge readiness, transition quality, and post-discharge coping.23,24 While these domains are likely relevant for transitions in palliative care patients, determining the applicability and experience within palliative care will provide valuable inputs for future service enhancements. To this end, we adopted a mixed methods approach to develop insight into how palliative patients experience these three domains during hospital-to-home transitions.
Methods
Research question
How do palliative care patients and/or caregivers experiences of discharge readiness, transition quality, and discharge coping impact their hospital-to-home transition?
Study design
Using a convergent, parallel mixed methods study design25,26 we evaluated the transition experience. 27 Mixed methods are designed to offset methodological limitations by offering distinct yet overlapping data that can be used to contextualize and corroborate findings. We made use of a pragmatic approach, 25 which facilitates weaving together two contrasting and inherently different methodologies by accepting “singular and multiple realities” open to interpretation. Our qualitative and quantitative data were collected concurrently, analyzed separately, and integrated to give insight into the hospital-to-home transition. 28
Setting/population
Potentially eligible patients: (1) were at least 18 years of age; (2) had a Palliative Performance Scale score ⩾30%; 29 (3) received palliative care from an inpatient consultation service at one of two tertiary hospitals (Toronto General Hospital and Mount Sinai Hospital) located in Toronto, Canada; (4) were referred to a home-based palliative care program; (5) were fluent in English; and (6) had capacity for consent. We included caregivers fluent in English with the capacity to consent. In some circumstances the patient and caregiver participated as a dyad and if the patient was unable, the caregiver participated alone.
Sampling
We made use of a purposive sampling strategy, wherein we intentionally selected participants who would be able to speak to the hospital-to-home transition. Given that we only examined descriptive statistics of the quantitative data, we sampled patients until we had achieved theoretical saturation in our qualitative data.
Recruitment
Saturation was indicated by recurring themes in the data through ongoing analysis during recruitment. Potential participants were identified twice-weekly by the palliative care consultation team. Individuals were approached by study staff, informed of the study, and provided written consent to participate.
Data collection
Study staff visited participants for data collection on two occasions from October 2018 to 2019. Visit 1 occurred in the hospital up to 4 days prior to the patient being discharged home. Visit 2 occurred once the patient was home and had been seen by the palliative care physician, approximately 1 month after discharge. Data collection occurred in the same order for each participant; first completing the quantitative surveys, then completing the qualitative interview.
Quantitative data
The patient and/or caregiver were asked to complete three scales. The PROM scales were: Readiness for Hospital Discharge Scale (RHDS, where lower scores imply low readiness) 24 and Post-Discharge Coping Difficulty Scale (PDCDS, where higher scores imply a poor transition). 13 The PREM scale was the Care Transitions Measure-3 item (CTM-3, where lower scores imply a low quality transition). 30 These scales have been widely used in discharge transition research. Detailed descriptions and evidence of reliability and validity in adult medical surgical patients are included in Table 1. A demographic survey was completed at the first visit. If the patient felt unable to complete the scales, the caregiver completed patients’ demographic data on their behalf and completed the scales reporting their own perceptions of the patient transition.
Description of data collection.
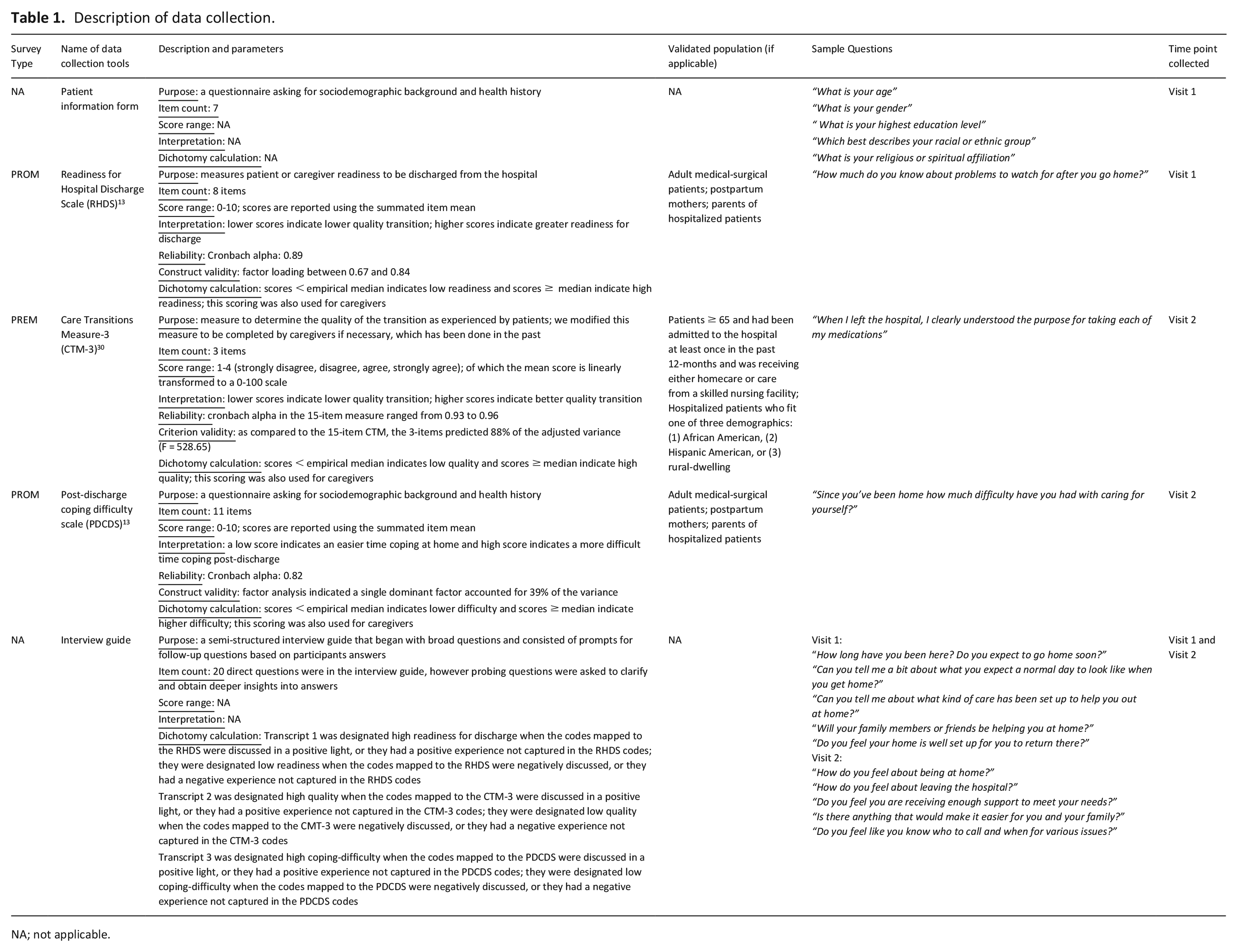
NA; not applicable.
Qualitative data
Our method of inquiry was based in grounded theory, wherein we systematically and intentionally collected and reviewed qualitative data. Semi-structured interviews were conducted after completing the scales in the hospital (Visit 1) and in the home (Visit 2) by SRI, JV, and SS. Interview questions were co-created with the research team and patient advocate (MS). The questions explored expectations and the experience of hospital-to- home transitions (see Table 1). All interviewers had past qualitative research experience and mock interviews were conducted with a patient advocate (MS) prior to commencing the study. Dyads were interviewed together. All interviews were conducted in-person, audio recorded, and transcribed verbatim.
Data analysis
Consistent with convergent parallel design, we analyzed the quantitative and qualitative data independently and then integrated our findings.
Quantitative data
We presented descriptive statistics on survey scores, then dichotomized participants into binary high or low levels for each of the scales based on the median to prepare for comparisons of survey and interview data. For details on this process see Table 1.
Qualitative data
The initial codes were developed inductively through grounded theory approach (see Isenberg et al., 31 for more details). Transcripts were analyzed and coded throughout the interview process by a minimum of two reviewers (SS, SRI, TK) using MaxQDA data analysis software; 32 disagreement was resolved through discussion.
Integration
To integrate our data we made use of a merged transformative methodology,25,33 where our qualitative data was transformed to quantitative (i.e. dichotomous) variables for comparison. To transform the qualitative data we mapped the developed codes onto the scale concepts. The qualitative data were then compared to the scale items using the MaxQDA crosstabs function and by examining the codes and in vivo quotes of each participant independent of the quantitative scores (SS). Each Visit 1 transcript was summarized as high or low discharge readiness and Visit 2 transcripts were summarized as high or low quality of transition and post-discharge coping difficulty ((SS) see Table 1). For unclear designations, a second reviewer was consulted (SRI).
Once translated into dichotomized components, we manually and statistically compared the data. For this portion of the analyses, we used caregiver scores when patients were not able to directly respond, to represent the experience of the patient/caregiver dyad in the discharge transition. The manual comparison involved examining the data for similarities and contradictions, which offered rich detailed understanding of the transitions phenomena as a whole. Further, we statistically compared the scales to the qualitative data using a kappa agreement coefficient (scores ⩽ 0 = poor, 0.01–0.20 = slight, 0.21–0.40 = fair, 0.41–0.60 = moderate, 0.61–0.80 = substantial, and 0.81–1 = almost perfect). 34 This process provides context and rigor for readers.
Ethical issues
All participants were consented following institutional approval at the University Health Network and Sinai Health (REB#18-5686 and #18-0172-E respectively).
Results
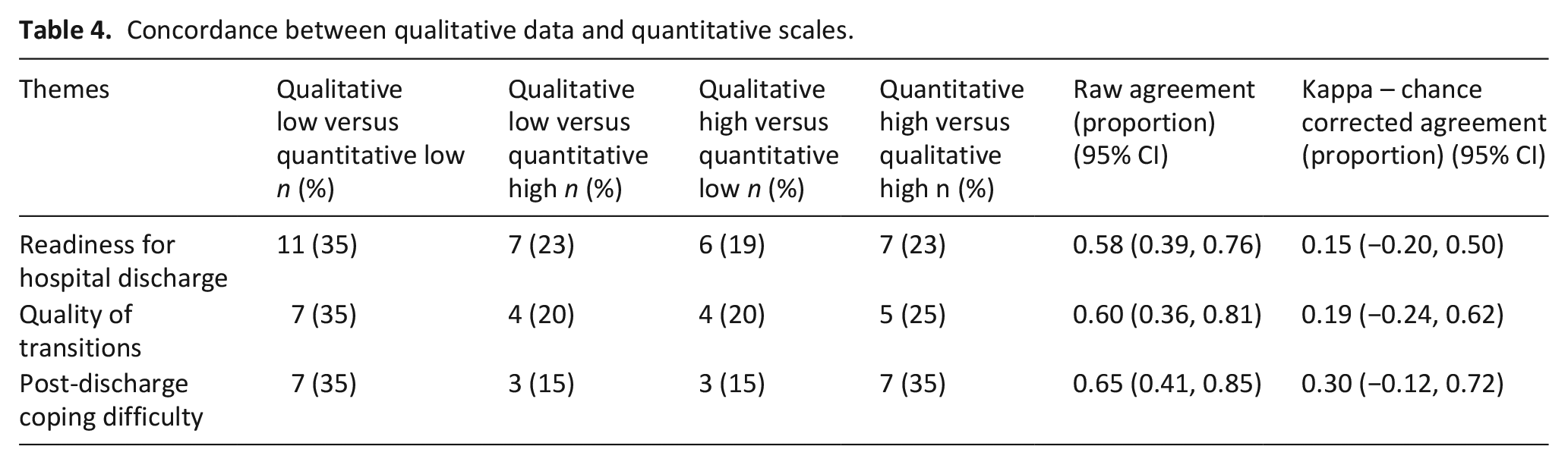
Seventy eligible patients were approached for the study. From this, 39 participants engaged in Visit 1 of the study, of whom 25 were patients, 7 were family caregivers of patients unable to respond to study surveys and/or interview, and 7 caregivers participated in a dyad interview (see Figure 1). Twenty-three participants took part in both visits. Interviews were on average 29 min, with a range of 7–80 min. Patient characteristics are described in Table 2(a) and (b). Qualitatively themes are integrated with quantitative findings in the narrative presentation of results. Table 3 presents the summary quantitative descriptive results; Table 4 presents the crosstabulation of quantitative findings with dichotomized qualitative findings.
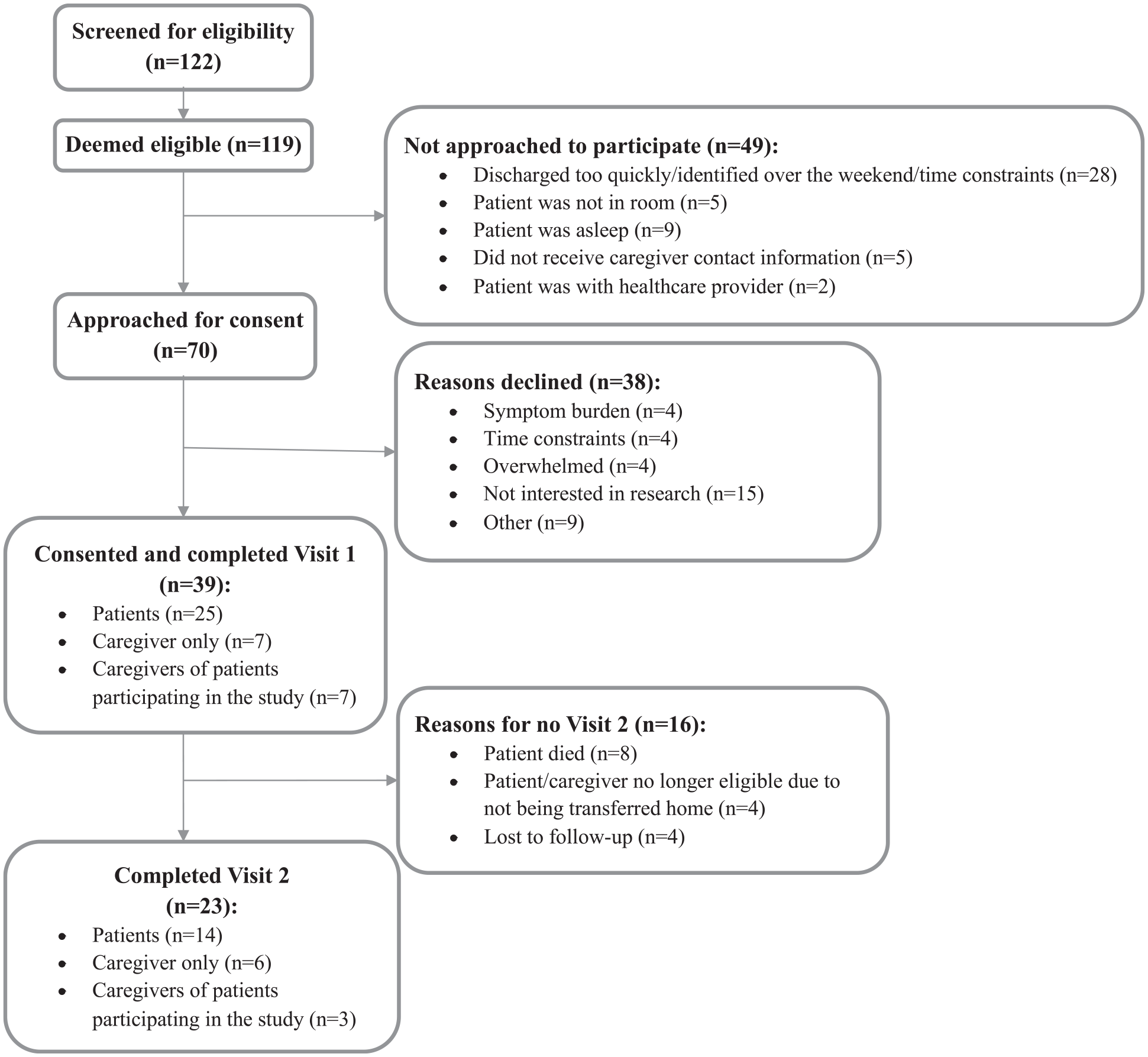
Recruitment flow chart.
Demographics of patients and caregivers.
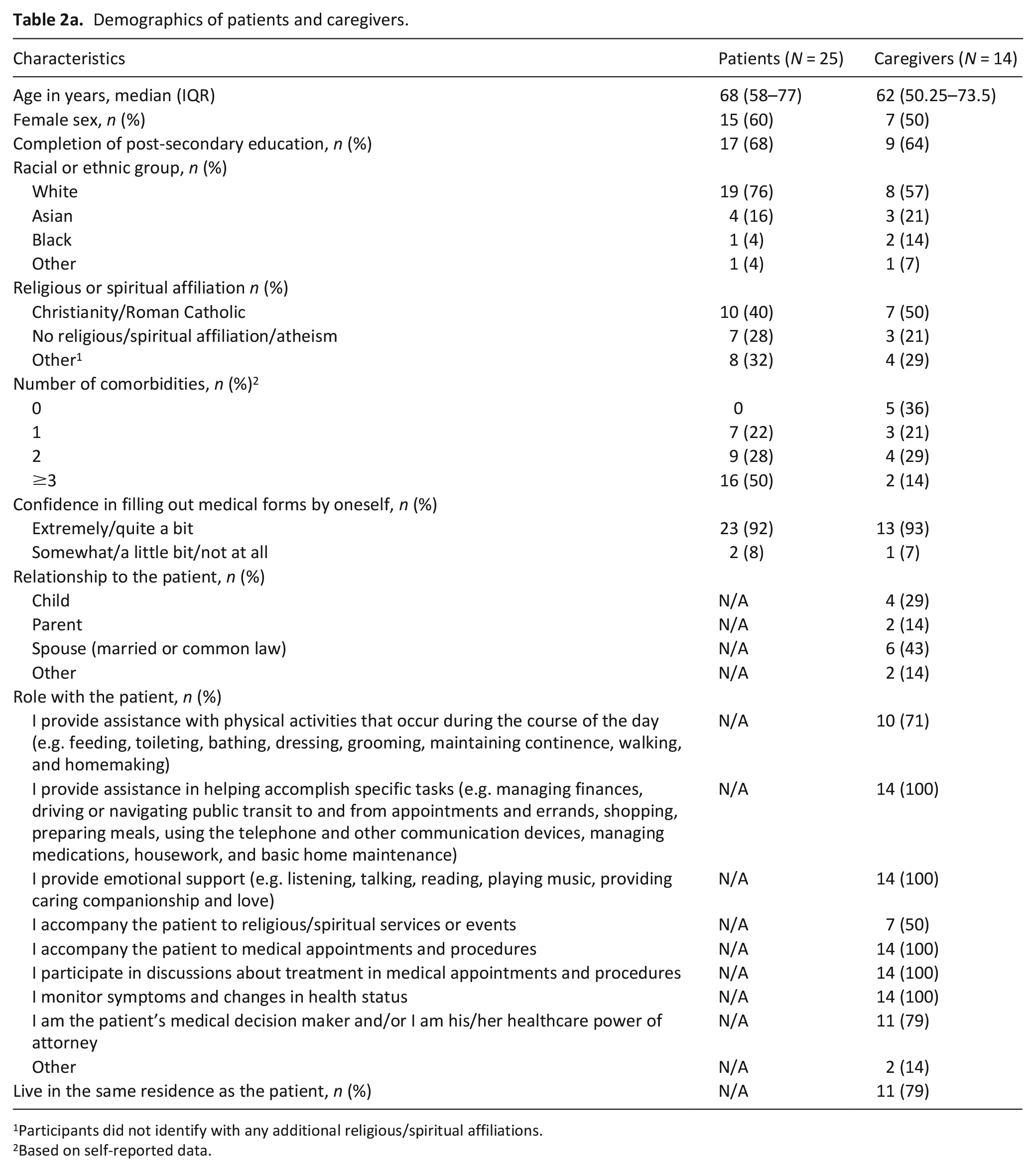
Participants did not identify with any additional religious/spiritual affiliations.
Based on self-reported data.
Clinical characteristics of patients affiliated with the study.
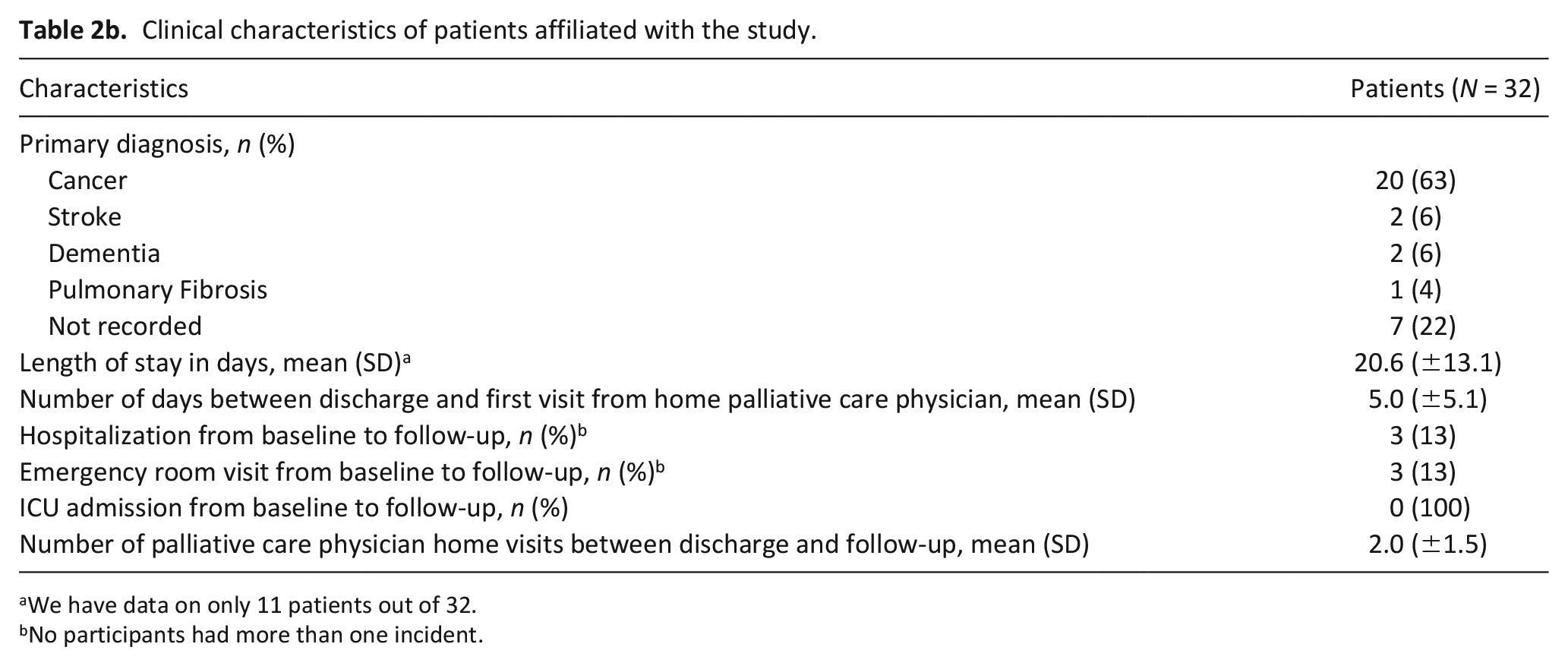
We have data on only 11 patients out of 32.
No participants had more than one incident.
Descriptive statistics for study measures.
Concordance between qualitative data and quantitative scales.
Readiness for discharge
The median score of the RHDS data was 5.8 (IQR, 1.9), with 47% categorized as high readiness and 53% indicating low readiness. This contrasted slightly with our qualitative data, with 42% expressing high readiness, and 58% expressing low readiness for discharge. The chance corrected kappa score was 0.15 (95% CI: −0.20, 0.50).
Those who indicated they had high readiness in both their qualitative and RHDS data (n = 7, 23%) felt they knew how to perform care tasks at home, had sufficient community support, and believed administrative issues delayed their discharge from hospital. A patient described this experience saying: “The biggest challenge I’ve had is being told several different discharge dates and they don’t happen. Not necessarily because there’s medical issues, but administrative” (Female patient-35 years).
Alternatively, those who had low readiness in both their qualitative and RHDS data (n = 11, 35%), cited that they did not know how to care for the patient or themselves and did not feel physically well enough to be at home. A caregiver illustrated this saying: I feel like okay, I can deal with one thing, but I don’t know, like, how to change the dressing. I still have to constantly ask the nurses ‘Could you please change her dressing’ you know? There’s not one thing where I independently do something for her so like there’s nothing where I can say I independently 100 percent know how to do this and I’ve fully done it and I’m confident in it by myself, you know? (Female caregiver-27years)
Exploring the differences between the qualitative and RHDS data, we found participants who indicated they had low readiness in their RHDS responses but expressed higher readiness in their interviews (n = 7, 23%). This sense of readiness was apparent when five out of these seven participants responded “yes” when asked directly if they felt ready to go home. One participant stated “Oh, yeah, been there and done that. I can go home” (Female patient-68 years), yet she indicated on her survey that she did not feel ready (RHDS = 5.25/10).
Whereas those who expressed they were quantitatively ready but not qualitatively ready (n = 7, 23%) emphasized both stress and uncertainty about how the process was going to occur, one stated:
It’s such a stressful time, I don’t remember what people say. And people give me information about what to do and where to go, and I shake my head yes, because I hear them and then 2 s later, I have no idea what they’ve said. And that’s a real worry (Female caregiver-82 years).
Quality of transition
Regarding the quality of the transition, the median score for the CTM-3 was 66.7 (IQR, 33.33) with 45% indicating they had a high-quality transition and 55% indicating they had a low-quality transition. Similarly, for the qualitative categorization, 45% experienced high-quality and 55% experienced low-quality transition, with a chance corrected Kappa score of 0.19 (95% CI: −0.24, 0.62).
Participants who had concordant high-quality transitions in both qualitative and CTM-3 data (n = 5, 25%) spoke about having their healthcare needs met through receiving appropriate equipment, reassurance, and having a clear understanding of their responsibilities once they were home. One caregiver spoke about the ease of the process: Oh [the transition] went smoothly, I was amazed. They came in, they set the bed up, it was two minutes and they were out the door. Then they brought [the patient] home, put him in bed and it was great. (Male caregiver-72years)
For those who had a corresponding low qualitative score with a low CTM-3 score (n = 7, 35%), the common challenges were a lack of clarity around responsibilities once they were home and confusion around medications. For example, the wife of a patient discussed not recognizing how much assistance her husband would need at home: Well, I think I was totally unprepared for what in actuality happened when we got home. First of all, my husband was on a very high dose of medications and he was like almost comatose. It was like he was walking around in a trance. He couldn’t do anything himself. He needed total care. All of a sudden. . . he had been doing this before he went to the hospital. He dressed himself. He showered himself. He could not do anything like that [once home]. (Female caregiver-75years)
A clear discrepancy emerged among those with low qualitative designations but high CTM-3 scores on the surveys (n = 4, 20%). Patients, caregivers, or dyads expressed not having their healthcare needs met, as one participant mentioned not having appropriate equipment to support herself once home: Well, I mean I came home weak as a kitten. . . I mean I would fall, and I would have to crawl to the nearest structure to pull myself up. (Female patient-61years)
For those who scored low on the CTM-3, but had high qualitative results (n = 4, 20%) this might have been a result of changing healthcare needs the longer they were home. One participant stated this saying: At the beginning, I had more energy and. . . I was feeling pretty good and just didn’t feel like I needed the PSW, now I may change that again, because I’ve not felt as good. (Female patient-51years)
Coping difficulty once home
The median score for the PDCDS was 5.0 (IQR, 2.6). Survey distribution had 50% of participants indicating they had low coping difficulty and 50% high coping difficulty. Our qualitative data had 55% of participants with low coping difficulty and 45% with high coping difficulty. The discrepancies resulted in a kappa of 0.3 (95% CI: −0.12, 0.72).
Among participants categorized in both their quantitative and qualitative as high coping difficulty (n = 7, 35%), common reasons included an inability to cope with physical side-effects, experiencing challenges managing equipment, and experiencing emotional challenges when returning home. One participant spoke about her challenges navigating at home: Yeah, well you learn when you come home. You learn how to handle your own situation. We were not in a good position at all when we came home. Didn’t know how to handle the machine, the people were inadequate. Now I’m setting up the people and we know how to handle the machine, because my husband worked it out. (Female patient-77years)
For the participants who were categorized as having low coping difficulty on both qualitative and quantitative data (n = 7, 35%), key reasons were having a sense of community, feeling happy to be home, and having sufficient care providers at home. When asked about how she felt about being home, one patient stated: “Oh, I love being at home, much better than being in the hospital. You know, you sleep better. You eat better. You’re around your family. . .” (Female patient-72 years).
The discrepancies between the qualitative and quantitative data were among those who were designated as having high coping challenges based on the qualitative data, yet their PDCDS scores indicated low coping difficulty once home. The qualitative data suggested this was because participants experienced challenges with their physical wellbeing once home. A patient and his daughter said:
The first few weeks were a little bit scary because he was really weak and there are a lot of stairs in our home, in his home, and. . .
And the fact that I wasn’t well when I came home and I started vomiting. Everyone started. . . got a little uptight and concerned and like oh no, it’s all starting again. (Male patient-58years)
Similarly, another patient discussed expectations and reality were very different, saying: “I didn’t expect to come home and experience so much fatigue” (Male patient-62 years).
Among those who had high coping difficulty scores (n = 3, 15%) but reported low coping challenges qualitatively, this was potentially because of the removal of the uncertainty; participants feeling like they were able to do things once they were home. For example, one patient stated: Just not knowing what was going to happen because like I don’t have bars. I don’t have. . . like if I fell or something, what am I going to do? But I’m still in the stage where I’m fine, that I can do most everything and just a little help from the PSWs again for showering. They do meal prep, some cleaning. So yeah, it’s a lot better than I thought it was going to be. (Female patient-51years)
Discussion
Main findings
This study examined discharge readiness, transition quality, and subsequent post-discharge coping of hospital-to-home transition in palliative care patients. Scores on the three domains provide evidence of need for attention to the hospital-to-home transition to support improved quality of care and outcomes. While there was some level of convergence of quantitative scores and qualitative representations of the transition experience, the qualitative findings also pointed to differences in how patients narrate their experiences.
What this study adds?
Using a mixed methods approach, our findings suggests that discharge readiness, quality of transition, and post-discharge coping offer valuable insight into the hospital-to-home transition. Specifically, the agreement between the qualitative and quantitative data, for both positive and challenging transitions, suggests areas that are clearly important to palliative care patients/caregivers in transitions, above and beyond utilization and readmission concerns. Whereas the discrepancies indicate areas for future examination. Interestingly, the scores showed lower readiness35,36 and transition quality,37–39 and poorer coping difficulty,40,41 pointing to the challenges of transitions for palliative care patients and opportunities to improve the transition experience for these patients.
Participants who were ready to go home highlighted the importance of community support upon returning home; whereas those not ready cited feelings of uncertainty and stress. Findings are well-supported by an existing concept analysis review 42 that found community support contributes to a sense of discharge safety. What is more challenging, and an insight from this study, is meeting the needs of those who express readiness to go home, yet are primarily motivated by a desire to leave the hospital and may not be adequately prepared to transition home. This is concerning because older adults who feel unsupported in the transition process may disengage from the process altogether, leading to a worse transition. 43 Discerning the difference between eagerness and readiness may be challenging, yet it is critically important to promote readiness for discharge.
Those who experienced a high-quality transition, as per the concordant data, felt they had reassurance and support, their equipment needs met, and a clear understanding of their responsibilities at home. Those who had concordant low-quality transitions had poor understanding of their responsibilities and experienced confusion with their medications. These findings align with other studies examining transitions of care in older adults and general inpatients.1–4 Qualitatively, participants recalled their healthcare needs not being met and confusion around medication, but quantitatively their responses suggested the opposite. Within palliative care, healthcare needs may be more nebulous and change more rapidly than other populations. 44 As a result, it may be challenging for patients and caregivers to articulate their needs as they move from hospital-to-home. The gap between the level of support in hospital and expected independence at home is clearly challenging to navigate for patients and has been documented in past studies.2,45 Finding ways to help caregivers and patients better understand their needs and how to meet them is imperative.
Examining post-discharge coping difficulty, participants with little difficulty identified having community and healthcare provider support and were happy to be at home. In contrast, those with high difficulty mentioned their physical symptoms, challenges with equipment, and emotional distress. Practical findings are well-substantiated in previous literature, with caregivers citing difficulty caring for unwell patients and frustrations with equipment. 46 Participants with conflicting qualitative and quantitative data discussed emotional distress due to holding expectations in the hospital that they would manage well once home, yet not having that capacity once home. Dose et al., 47 found similar results, with patients feeling an “unexpected disruption” upon experiencing a different reality than expected when receiving hospice-at-home. Our study builds on this, as participants experiencing little difficulty do not express feeling the same emotional distress. It may be beneficial to set clear expectations that hospital discharge does not imply a pre-hospitalization capacity, but rather that patients no longer need acute levels of care.
Limitations
The limited number of individuals completing Visit 2 may have impacted our ability to detect changes. Only 57% of approached individuals consented to participate and our participants’ scores were very similar, suggesting a homogenous sample that may trend toward those who were less ill. Regarding outcomes, these scales are all self-reported and using the median to dichotomize scores may have created an artifactual threshold contributing to the low concordance. Merging the experiences of patients and caregivers helps to focus on the transition as a joint patient/caregiver experience, but the caregiver experiences may have been overshadowed due to large numbers of patients included. Conducting the scales first and focusing on three domains may have inhibited emergences of other domains important to palliative care patients. Finally, the RHD scale was administered up to 4 days before discharge, potentially impacting readiness since readiness increases the closer the patient gets to discharge.
Conclusions and implications
Integrating qualitative and quantitative data provided overlapping but distinct perspectives into the experience of discharge readiness, quality, and post-discharge coping. Concordant data should be used to support an intervention targeted toward these domains that is tailored to a palliative care population’s need within a transition. Discrepancies should be considered areas to examine further in future studies examining hospital-to-home transitions. Given our findings, future research should validate these scales in a palliative population to ensure patients’ voices are heard throughout the course of the transition.
Footnotes
Acknowledgements
This work was completed while Stephanie Saunders and Sarina Isenberg were affiliated with the Temmy Latner Centre for Palliative Care, part of Sinai Health in Toronto Ontario.
We would like to thank our colleagues at Toronto General Hospital and Temmy Latner Centre for Palliative Care, part of Sinai Health in Toronto, CA.
Authors’ contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Temmy Latner Centre for Palliative Care’s Golda Fine Award; the University of Toronto’s Department of Family and Community Medicine Cass Family Grant for Catalyzing Change.
Statement about data
Data is unavailable for confidentiality reasons and small sample size. For questions regarding data please contact the corresponding author.