
Abstract
Background:
Patients express a variety of needs, some of which are labeled social and spiritual. Without an in-depth exploration of patients’ expressions of these needs, it is difficult to differentiate between them and allocate appropriate healthcare interventions.
Aim:
To gain insight into the social and spiritual needs of patients with a life-limiting illness and the distinction between these needs, as found in the research literature.
Design:
A mixed-methods systematic review and meta-aggregation were conducted following the Joanna Briggs Institute (JBI) approach to qualitative synthesis and the PALETTE framework and were reported according to the PRISMA statement. This review was registered in PROSPERO (CRD42019133571).
Data sources:
The search was conducted in PubMed, EMBASE, CINAHL, Scopus, and PsycInfo. Eligible studies reported social and spiritual needs from the patients’ perspective and were published between January 1st 2008 and October 2020. The quality of evidence was assessed using JBI Critical Appraisal Tools.
Results:
Thirty-four studies (19 qualitative, 1 mixed-methods, and 14 quantitative) were included. The five synthesized findings encompassing social and spiritual needs were: being autonomous, being connected, finding and having meaning, having a positive outlook, and dealing with dying and death.
Conclusion:
What literature labels as social and spiritual needs shows great similarities and overlap. Instead of distinguishing social from spiritual needs based on patients’ linguistic expressions, needs should always be explored in-depth. We propose a socio-spiritual approach that honors and preserves the multidimensionality of patients’ needs and enables interdisciplinary teamwork to allocate patient-tailored care.
Keywords
Patients express multidimensional needs in the palliative phase of their illness, some of which are labeled as social and spiritual needs;
When needs are labeled as social or spiritual, it is often unclear on what grounds;
Hence, healthcare professionals experience challenges concerning time, knowledge, and experience in identifying, understanding, and addressing social and spiritual needs.
This mixed-methods review is the first study combining qualitative and quantitative studies to distinguish between social and spiritual needs of patients in the palliative phase of their illness;
Identifying needs through a socio-spiritual approach offers the possibility to respect the social and spiritual dimensions as both distinct and interrelated.
Attending to patients’ social and spiritual needs requires experience and knowledge-based dedication and awareness from healthcare professionals;
Combining qualitative and quantitative assessment methods helps patients express their needs;
More research is necessary into the interaction and interconnection of social and spiritual needs specifically and multidimensional needs in general.
Introduction
Palliative care aims to optimize the quality of life of patients faced with a life-limiting illness and their families by relieving physical, psychosocial, and spiritual suffering. 1 Both Saunders’ concept of “total pain” and the biopsychosocial-spiritual model of care cover the aim of palliative care and assign a vital role to the social and spiritual dimensions. 1 Although the social and spiritual dimensions are pivotal in patients’ quality of life and dying,2,3 these dimensions are not often adequately assessed in practice.4–6 The benefits of assessing these dimensions, however, are widely supported.7–13
Social and spiritual dimensions of quality of life and dying
There is no clear definition of the social dimension of quality of life and dying. Literature shows it encompasses social relationships, which make people happier and give them a sense of identity, companionship, and meaning in life.3,14 This dimension also covers emotional support and assisting in practicalities, such as financial help, informational support, and affectionate support. 15 Connections and relationships give patients a reason to live and enable them to better cope with the reality of dying. 16 Combining these aspects, sociality can be defined as the dimension of human life related to how people make and maintain relationships with others and that concerns how values, norms, rules, and roles are respected.14–18 Life-threatening illnesses can challenge patients’ sociality; limiting their autonomy, independence, and performance status and affecting their social, professional, and family roles as well as changing their bodily appearance. 19 Consequently, the perception of a limited future makes it more challenging to formulate own goals, expectations, values, and interests concerning one’s social context.20,21
In contrast to the social dimension, the spiritual dimension seemingly does have a clear definition. According to the definition adopted by the Spiritual Care Reference Group of the EAPC, spirituality “is the dynamic dimension of human life that relates to the way persons (individual and community) experience, express and/or seek meaning, purpose, and transcendence and the way they connect to the moment, to self, to others, to nature, to the significant and/or the sacred.” 22 A current review, however, shows definitions of spirituality and the spiritual dimension are, despite the consensus definition, still disputed. 23 Studies showed that up to 80%–90% of patients had reported spiritual needs.24,25 Murray et al. contrasted spiritual with psychosocial needs and defined them as “needs and expectations which humans have to find meaning, purpose, and value in their life.” 4 For some people, religion is a component of their spirituality, but this may not hold for others. For those who do consider religion meaningful, their level of observance or belief will vary from person to person. 4
While the social and spiritual dimensions are distinct, the similarities between the linguistic expressions associated with both the social and the spiritual dimension are striking. Social work literature often pays attention to the spiritual dimension by underlining the importance of the existential dimension and the need for collaboration between social workers and spiritual carers to address patients’ needs.26–28 The other way around is less the case: literature concerning the spiritual dimension appears to appropriate parts of the social dimension and is more focused on the legitimation of its field. 23 Concepts like “connection” and “autonomy” are then easily interpreted unilaterally as spiritual, without acknowledging how these concepts relate to the social dimension as well.23,29 Studies have mainly focused on patients’ spiritual needs. 24 Although more and more studies focus on the social dimension of healthcare in general – that is, socioeconomic level, housing, availability –, research concerning patients’ social needs in the palliative phase is staying behind.
Recurrent themes of patients’ needs
Previous reviews have identified recurrent themes that encompass patients’ needs concerning the spiritual dimension.30–32 These themes concern, amongst others, a “need for meaning,” “need for relationships,” “need for control” and “need for independence.” Throughout these reviews and some primary studies, these themes frequently recur, although sometimes phrased differently. Given the recurrence of the same themes throughout studies, it is unlikely for a new study to find patients’ needs concerning the spiritual dimension that do not fit already identified themes. A similar review has also been conducted on patients’ psychosocial needs. Although this review studies psychosocial needs, no definition of the corresponding dimension is provided in the article. This lack of focus could explain why for instance “spiritual distress” is presented as a psychosocial need specific to heart failure patients. 33 The needs patients express and that are labeled social or spiritual in these reviews show similarities on a linguistic level. Therefore, themes identified for patients’ needs concerning the spiritual dimension are potentially suitable for the social dimension and vice versa.
A thorough review of patients’ social and spiritual needs in the palliative phase of their illness is vital to identifying and understanding patients’ needs, and starting appropriate healthcare interventions, and allocating fitting healthcare providers. Therefore, this mixed-methods systematic review synthesizes the existing evidence on the social and spiritual needs of patients with a life-limiting illness to gain insight into these needs and the distinction between them.
Methods
Design
Studies on patients’ social and spiritual needs in the palliative phase of their illness are heterogeneous in terminology and study design. 24 Since both qualitative and quantitative study designs focus on the same outcomes, being patients’ social and spiritual needs, an integrative mixed-methods design was employed. This design is optimized to fit multiple study designs and types of data. 34 We employed the Joanna Briggs Institute (JBI) approach to qualitative synthesis or meta-aggregation to synthesize both qualitative and quantitative data. 35 This method enabled the researchers to assess findings across studies and produce generalizable statements.
Furthermore, performing a literature search within the field of palliative care is challenging due to variations in patient characteristics, diseases, and involved stakeholders, which lead to a broad range of topics.36–38 Therefore, we used the Palliative cAre Literature rEview iTeraTive mEthod (PALETTE) framework for developing an appropriate search strategy. 39 Furthermore, this systematic review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) framework. 40 The protocol of this study was registered in Prospero (registration number: CRD42019133571). 41 No ethical approval was needed.
Databases and searches
A preliminary search was conducted in PubMed for studies on patients’ social and spiritual needs in the palliative phase, resulting in the first selected series of studies. By using these studies and consulting information specialists at COCHRANE and specialists within the fields of social work and spiritual care, the terminology employed to describe and study these needs became more transparent, making it possible to gather adequate synonyms, resulting in additional searches. As a result, common needs in the social dimension of healthcare, for example, education, finances and community, turned out to not contribute to the search and were therefore left out. Following the PALETTE method, this process of identifying new studies and adjusting the search string was repeated until the search strategy was validated, meaning it identified all “golden bullets” (see Appendix 1). 39
The final search was constructed using a Domain Determinant Outcome (DDO) outline (Table 1): D) palliative care, D) the social and spiritual dimensions, O) patients’ needs and the patient perspective. The search was set out on April 28th, 2019, without any limits, and was updated on October 1st, 2020, in five online databases:
Search strategy PUBMED.

PubMed, EMBASE, CINAHL, Scopus, and PsycInfo. The strategy was validated in PubMed, and minor adjustments were made for use in other databases. The adapted search strategies for the other databases can be found in Appendix 2. Additionally, a manual search of both Google Scholar and reference lists of the included studies was performed by the reviewer (TL) to check the search strategy’s validity.
Eligibility criteria and study selection
A study was eligible for inclusion if it met the following criteria: (1) the objective of the study was to assess patients’ social and/or spiritual needs; (2) the studied needs were described from a patient’s perspective through either qualitative or quantitative inquiry; (3) the study population needed to consist of patients in the palliative phase of their illness in any healthcare setting; (4) the study was a full report that was published in English, German or Dutch. A “need” was defined as a functional, emotional, social or spiritual issue as perceived by the patient, which requires professional assistance.42,43 Preliminary searches showed an increase in study frequency and quality from 2008 onward. Therefore, we excluded studies published before 2008.
Two researchers (TL and EdG) independently screened titles and abstracts to identify relevant studies using Rayyan: a web-based screening program that supports researchers to systematically and methodically select and compare citations independently. 44 Full texts were retrieved if the abstract did not provide enough information to allow selection or if the study passed the first eligibility screening. Two researchers (TL and EdG) also independently performed full-text screening. When information on eligibility criteria remained unclear after the full-text screening, the first author of the study was contacted by e-mail and requested to send additional information. The researchers resolved any disagreements, and when they did not meet a consensus, this was discussed within the research team.
Data extraction
Two researchers (TL and EdG) extracted data on the study’s location, research question, study design, participants, setting, data collection method, and outcomes. Based on Cochrane methodology, a purposefully created data extraction form was used to accommodate qualitative and quantitative studies.45,46 This form was pilot tested on three qualitative and three quantitative studies to ensure consistency, after which the research team approved them. The data was analyzed using Nvivo 12 software. 20
Quality appraisal
The quality of qualitative and quantitative studies was assessed using the JBI Critical Appraisal Checklist for Qualitative Research and the JBI Checklist for Analytical Cross-Sectional Studies. 47 The checklist for qualitative studies consisted of ten items concerning a study’s congruity, researcher and participants’ position, ethical considerations, and consistency of the conclusions. The quantitative studies consisted of eight items concerning outcome measurement, confounding, and statistical analysis. Two reviewers (TL and EdG) independently appraised the individual components of the checklists by indicating if a study did (+1) or did not (+0) adhere to the quality requirement or whether this was unclear (+0.5). A third reviewer was accessible when a consensus was not reached (ST). A summary score was finally calculated for each study. The quality appraisal did not affect studies’ inclusion since studies with lower appraisal scores could still contain valuable information on patients’ needs.
Extraction and integration of findings and data-aggregation
Findings from both qualitative and quantitative studies were extracted. A finding was defined as “a theme, category, or metaphor reported by authors of original papers.” 48 Before aggregating the qualitative and quantitative findings, quantitative data had to be transformed or qualitized into a compatible format. The numerical values of standardized questionnaires were provided with a qualitative label “present” or “not present” in the studied population, comparable to quantitative dichotomization.49,50 This leveled out any differences between qualitative and quantitative studies, no longer warranting separate analyses and syntheses of the findings. 50 This approach fitted this review since both qualitative and quantitative studies addressed the same outcome and research questions. 34 Findings in both qualitative and quantitative studies were assumed to complement one another. 51
The JBI method of meta-aggregation was then used to extract findings, categorize these findings, and finally synthesize them. Three levels of evidence exist for these findings: (1) unequivocal, (2) credible, and (3) unsupported. 52 Unequivocal evidence is supported by citations that were not open for challenge. Credible evidence was supported by citations that were open for interpretation. Unsupported findings were not supported by any citations. 53
The findings and categories were aggregated based on similarity in meaning. Two researchers (TL & EdG) studied all findings before categorizing them by theme. A consensus on the categories was sought within the research team, after which the findings were synthesized. These synthesized findings were used as a reflection on patients’ needs.
Results
Search and selection strategy
The final, updated search yielded 13,973 studies after the removal of duplicates. After title and abstract screening, 50 full texts were assessed for eligibility. This review finally included 34 studies (see Figure 1).

PRISMA flowchart.
Characteristics of the included studies
In total, 19 qualitative studies, 1 mixed-method study, and 14 quantitative studies were included, the characteristics of which are presented in Table 2. These studies represent 4465 patients, 2544 (57%) women.
Study characteristics.

This mixed-methods study presents results on two studies separately – for example, populations are also presented separately.
Cross-sectional data were compared for two populations and presented separately.
The quality of the qualitative and quantitative arms of this mixed-methods has been assessed separately.
When a variable is unknown, this is presented as “?”.
The qualitative studies report on the results of 565 patients, 292 (52%) women, with a median of 18 participants per study. 13 of the 19 studies focused on cancer as the primary diagnosis,54,56,57,59,61,62,64,66–69,71,99 others focused on heart disease (n = 1), 55 lung disease (n = 2),58,60 and multiple (chronic) diseases (n = 2).65,70 For one study the diagnosis was not reported. 63 Data was collected through interviews (n = 16),55–66,68,69,71,99 a focus group (n = 1), 54 a qualitative questionnaire (n = 1), 67 and patient records (n = 1). 70 Populations from these studies mostly originated from Europe (n = 7),54,55,60,62,65,67,69 Asia (n = 5),59,61,66,68,99 and the United States (n = 4),58,63,64,70 followed by Oceania (n = 2),57,71 and the Middle East (n = 1). 56
The mixed-methods study included 165 patients, 90 (54%) women, divided over a qualitative and a quantitative arm. 72 Data was collected through interviews and a survey on patients who have cancer.
The quantitative studies included 3728 patients, 2162 (58%) women, with a median of 165 participants per study. All quantitative studies included patients with cancer,73–76,81,82,84,85,87,89,91,94,96 except one in which the type of disease is unclear. 93 Study designs were predominantly cross-sectional survey studies (n = 11).73,76,81,82,85,87,89,91,93,94,96 Other designs were an observational study (n = 2),74,84 and a randomized controlled trial (n = 1). 75 Origination of the populations from quantitative studies was: United States (n = 4),74,75,87,89 Europe (n = 4),76,81,84,85 Oceania (n = 2),91,94 Middle East (n = 2),82,93 and Asia (n = 2).73,96
Of the included studies, European and Asian studies predominantly had a qualitative study design: respectively 6/10 and 6/8. Oceanian and Middle Eastern studies predominantly had a quantitative design, respectively, 3/5 and 2/3. Study designs from studies in the United States were divided fifty-fifty. Results showed that not all needs are found equally by qualitative and quantitative studies.
Quality appraisal
Tables 3, 4, and 5 show the quality appraisal of the included studies.
Quality appraisal of qualitative studies.
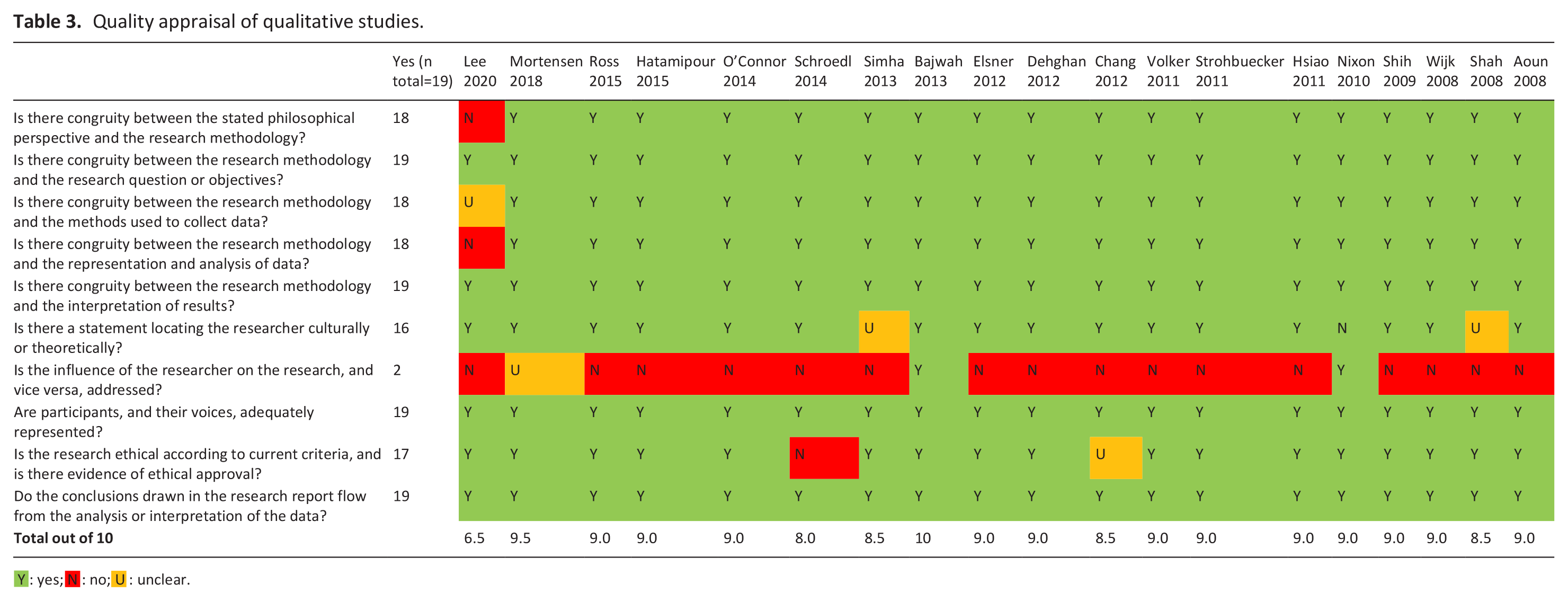
Y : yes; N : no; U : unclear.
Quality appraisal of mixed-method study.
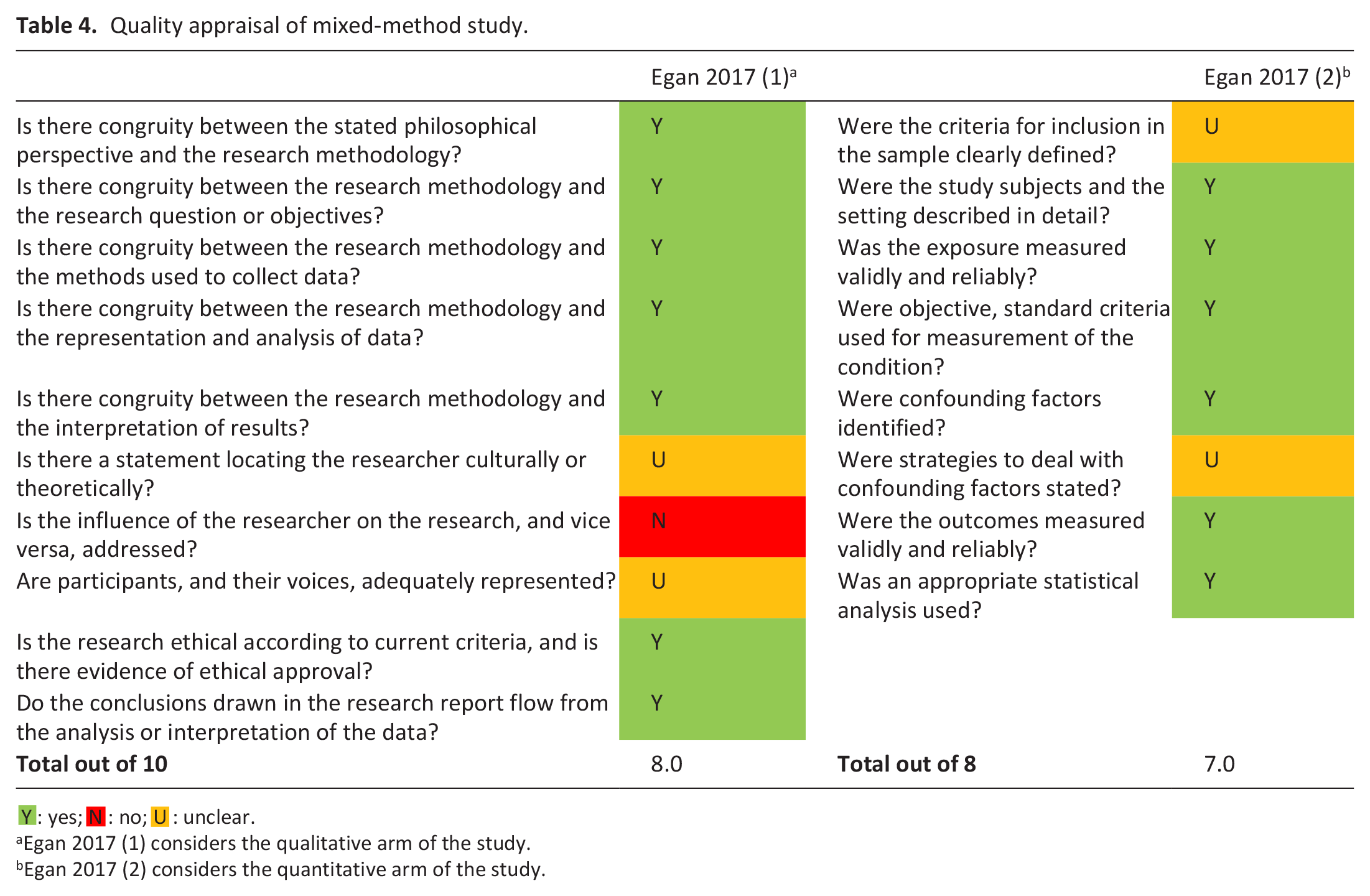
Y : yes; N : no; U : unclear.
Egan 2017 (1) considers the qualitative arm of the study.
Egan 2017 (2) considers the quantitative arm of the study.
Quality appraisal of quantitative studies.
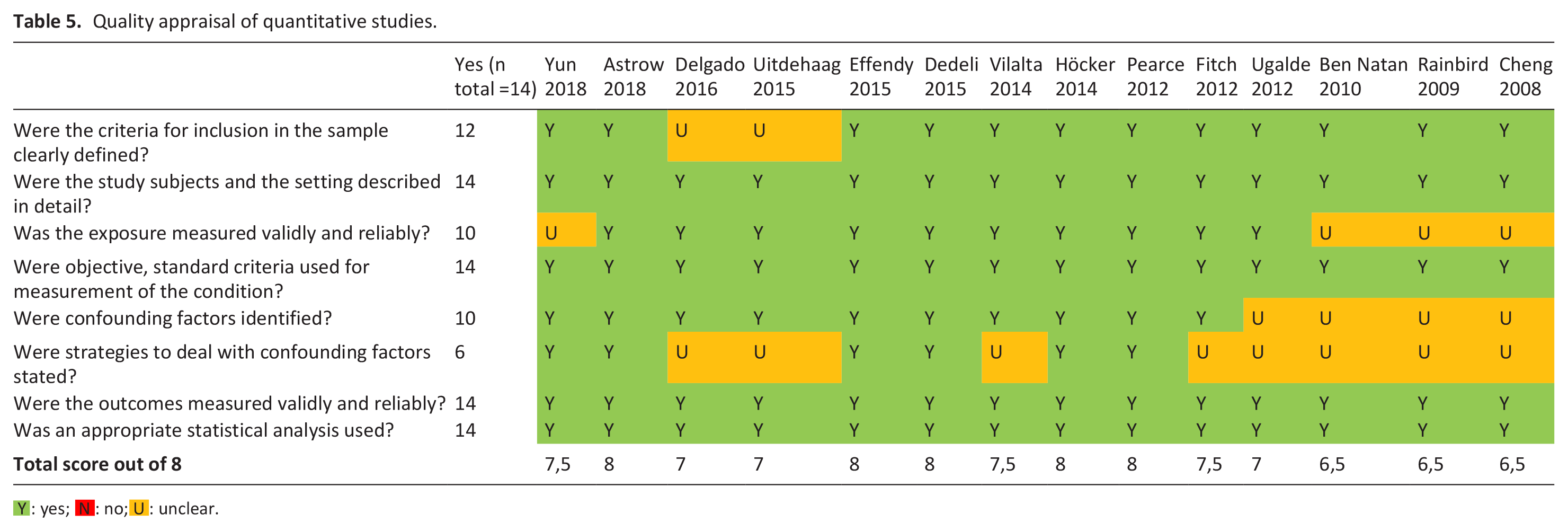
Y : yes; N : no; U : unclear.
Fourteen of the nineteen qualitative studies achieved at least 9/10 quality criteria. The main weakness across these studies was a lack of reflexivity, with only two of the nineteen qualitative studies achieving this criterion. As a result, the influence of the researchers on data collection and analysis is not apparent.
In the mixed-methods study, data on the qualitative arm was not reported in as much detail as was the data on the quantitative arm.
Of the quantitative studies, eleven of the fourteen studies achieved at least 7/8 quality criteria. The main weakness across these studies was a lack of strategies to control for confounding, with only seven of the fifteen studies achieving this criterion.
A summary score of the quality assessment is presented in Table 2. The quality of the studies was not of influence on the aggregation.
Transformation of quantitative data
Quantitative studies all used surveys to identify the prevalence of social and spiritual needs through prespecified items. These items were organized thematically or divided into subcategories: “social needs,” “spiritual needs,” “religious needs,” or even more specific “reassurance,” and “thoughts about end of life.” In this study, the themes/subcategories in the surveys were regarded as equal to the themes that resulted from thematic analyses in qualitative studies. Studies focusing on patients’ needs in a more general fashion only thematized their items to their corresponding dimensions, for example, “social needs,” “spiritual needs.” In these instances, the individual items of the survey were regarded as distinct themes. Themes and items from surveys were only reported as findings in the synthesis when patients reported them as prevalent.
Synthesis and meta-aggregation of findings
We developed five synthesized findings from 18 categories based on 243 unique findings: 84 qualitative and 159 quantitative findings. Table 6 shows the synthesized findings, categories, and findings. For qualitative findings, the level of evidence of these findings is reported: (1) unequivocal, (2) credible, and (3) unsupported. Since quantitative studies report on the prevalence of needs and provide no further illustrations, no level of evidence is reported. When a quantitative 5 finding is prevalent, it is included in the meta-aggregation.
Synthesized findings, categories, findings, and their level of evidence.

Quantitative findings reflect survey items. No further illustrations are given since the primary studies do not provide them.
These synthesized findings represent needs that patients express in the palliative phase of their illness concerning the social and spiritual dimensions and will be discussed in the following paragraphs.
Synthesized finding 1: Being autonomous
Studies showed various ways in which patients express their need to be autonomous—Figure 2 shows which categories of needs constitute this synthesized finding.
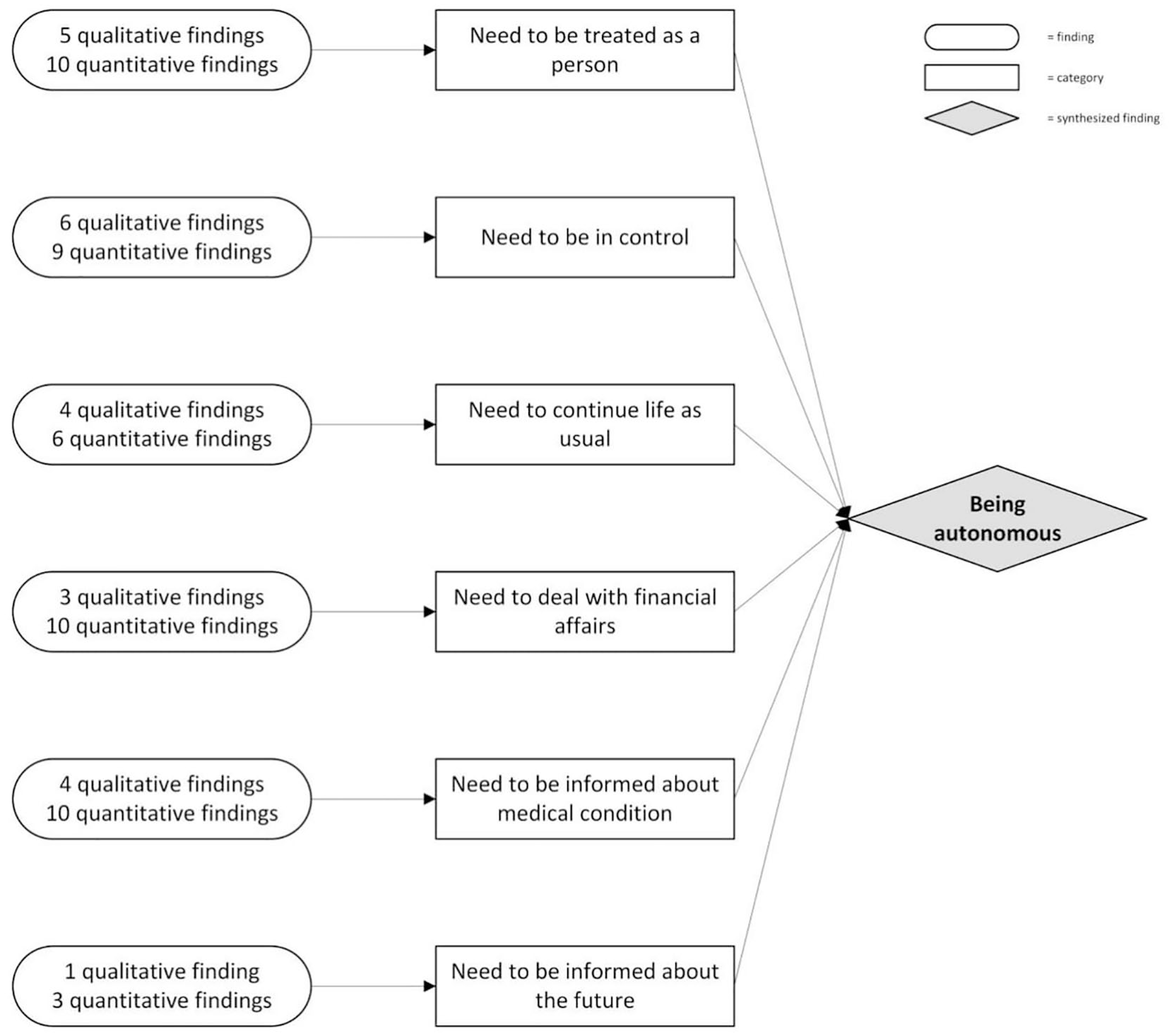
Synthesized finding 1: being autonomous.
Most simply, being autonomous can be explained as being one’s person and one’s capability for self-governance, that is, being directed by desires and wishes that are not imposed externally.19,100 Being autonomous touches upon patients’ need to be treated and seen as the person they are,56,65,68 and to continue life as usual.60,67,99 It also concerns staying in control over their lives,57,60,64,65,99 the care they receive, 19 and their financial concerns.54,62,73,75,94 To achieve this, patients expressed the need to be informed about their medical condition58,61,91,94 and their future. 58 Patients’ need for wanting to be autonomous relates to both the social and spiritual dimension: for some, autonomy relates to practicalities, values, and roles; for others, it touches upon their identity and core being, and for some patients, wanting to be autonomous related to all aspects listed above. Needs concerning being autonomous and decision-making are approached differently in Asia and the Western world. Whereas patients in both Asia and the Western world express information needs, these needs are purposefully neglected by family and healthcare professionals of Asian patients.66,68 Patients do express they appreciate to open communication about how their disease and situation affects their life.
Synthesized finding 2: Being connected
Findings concerning needs for relationships, love, affection, care, communication and support were abundant throughout the literature. Being connected was of overall importance. Figure 3 shows the construction of this synthesized finding.
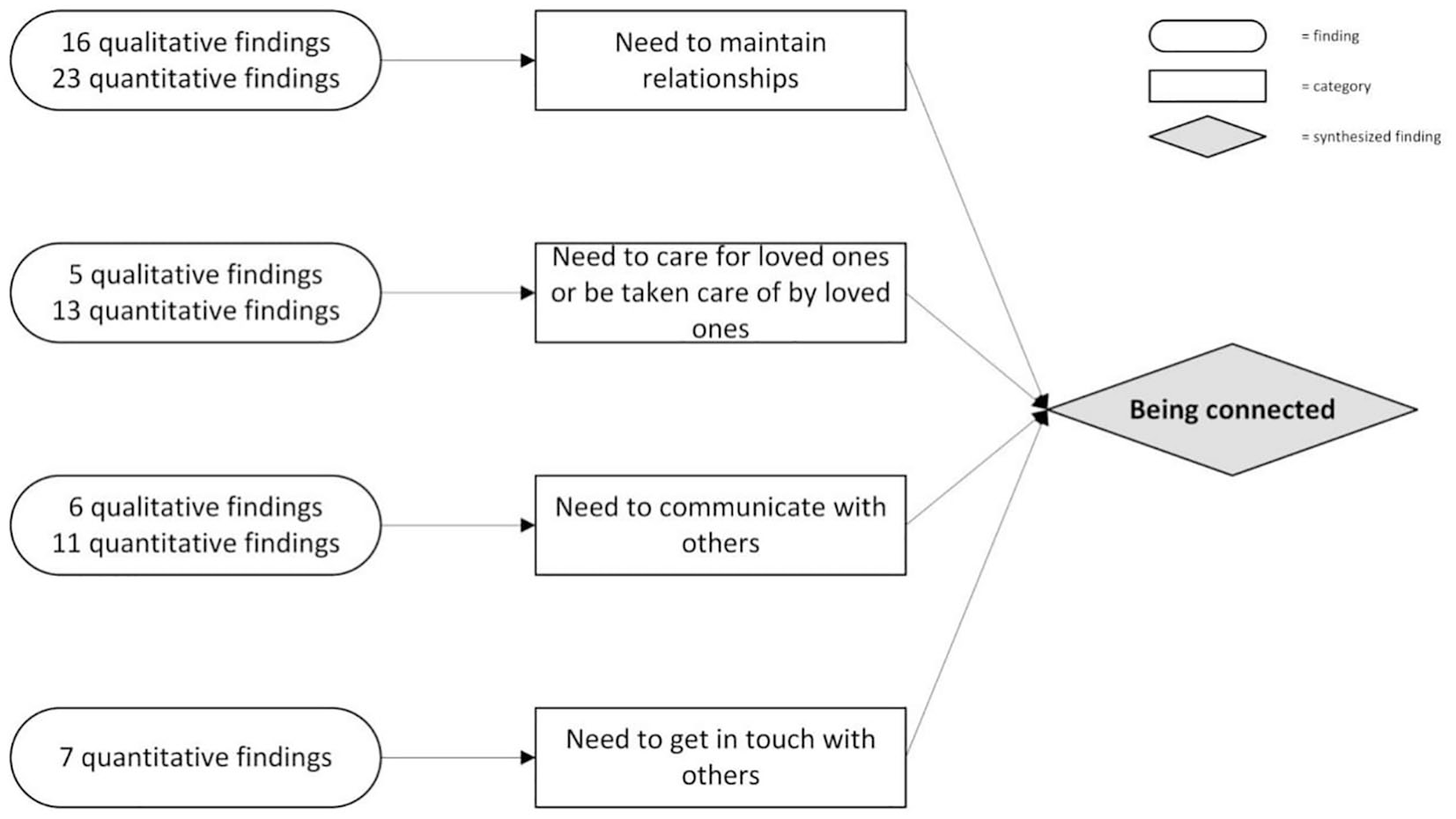
Synthesized finding 2: being connected.
Being connected appears to be of universal importance throughout all cultures covered by the included literature and is related to both the social and the spiritual dimension. Patients expressed the desire to be connected to family, friends and other loved ones,56,57,65–69,73,75,89,94,99 to a divine entity,63,73–76,85,87 and healthcare professionals. 65 Religious connection is a way of being connected and is therefore not seen as a distinct need. Being connected is expressed socially as a need for social support,57,96 financial support, 66 and social relations. 57 Spiritually, being connected concerned compassion, love and respect, 63 a sense of (religious) belonging63–65,69 and a sense of being more than an individual.82,84
Synthesized finding 3: Finding and having meaning
Patients expressed the need for meaning in the context of their disease.57,75,84 The construction of this synthesized finding is depicted in Figure 4.
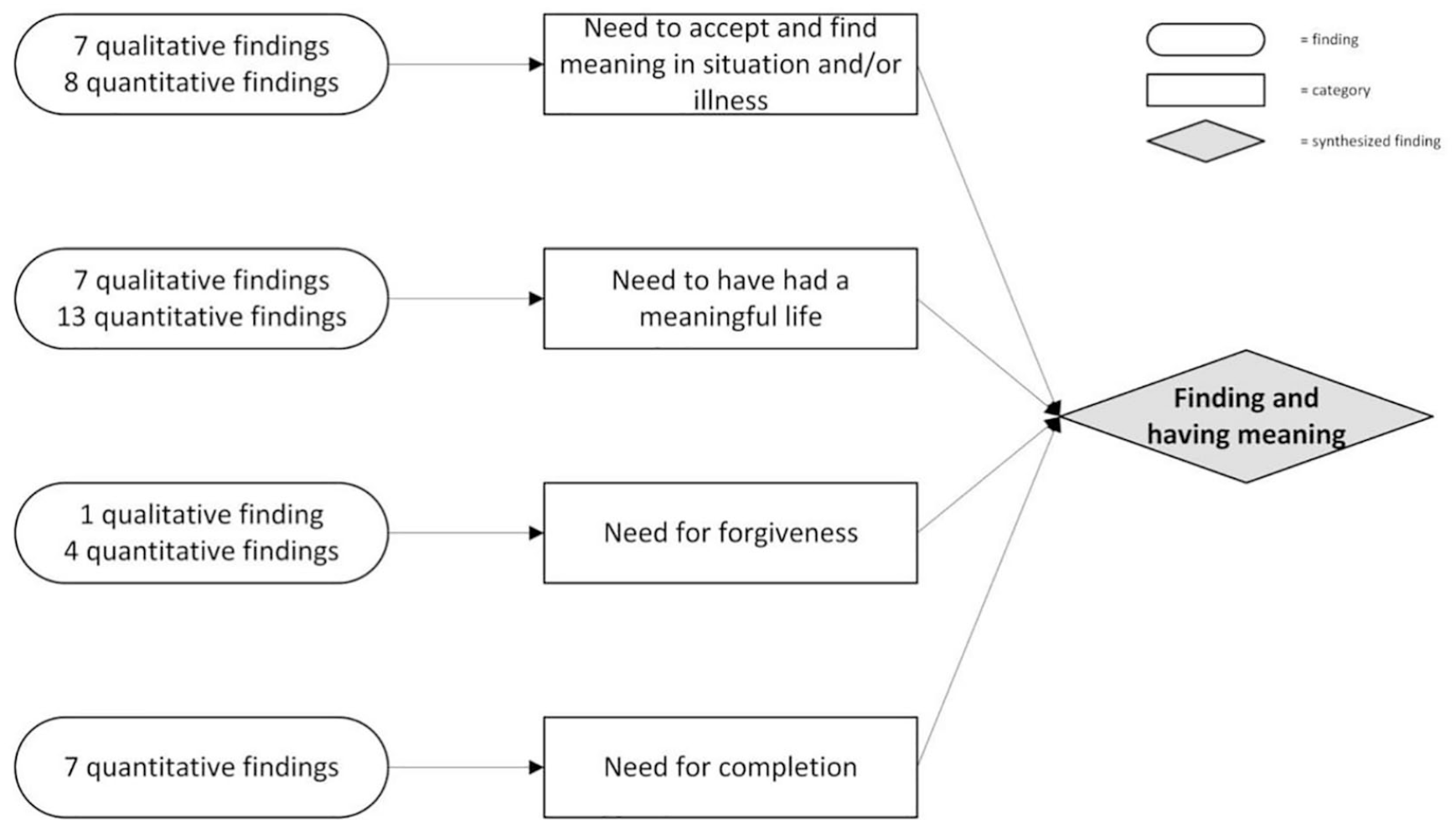
Synthesized finding 3: finding and having meaning.
Patients found and had meaning in the past, present and future. Firstly, patients expressed the need to feel their life has been meaningful,55,73,74 to remember their accomplishments,75,96 and to feel their lives were complete. 75 Secondly, patients needed to find meaning in the present: in their disease,56,81,85,89 their experience, 89 in nature and beauty,82,85 or through religion and religious rituals.56,67,69,74,87 Lastly, patients needed to find meaning in what had yet to come: they needed to complete their life through finishing or resolving unfinished business,73–75,85,96 and through setting new priorities in life.56,94 Having a meaningful life was lastly expressed through the need for forgiveness: forgiving others 87 or being forgiven by others and being free from guilt and blame.66,74,87 The need for forgiveness and the need to complete life were mainly expressed in quantitative studies. Only in one Asian study was the need for forgiveness found through qualitative inquiry. 56
Synthesized finding 4: Having a positive outlook
In the context of being faced with a life-limiting illness, patients expressed the need for a positive outlook through hope and peace of mind. Figure 5 shows how this synthesized finding is constructed.
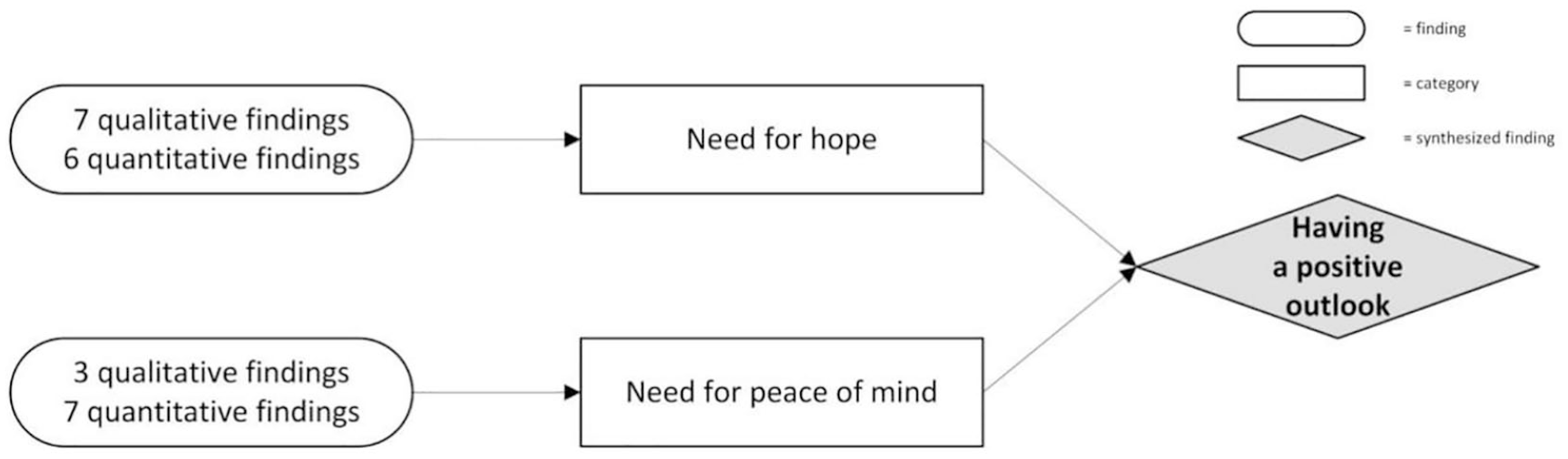
Synthesized finding 4: having a positive outlook.
Patients spoke of hope as a positive outlook or positive thinking,66,82,89,99 reassurance, 67 strength, 65 peace of mind,56,85 and the wish that everything would end well. 84 They found hope through reassurances by healthcare professionals, 66 being told the truth about their situation55,66 or knowing healthcare professionals have done all they could.55,73 Staying strong also demanded inner peace from these patients.56,61,74,85
Synthesized finding 5: Dealing with dying and death
Patients indicate the importance of addressing the uncertainties and feelings that come with dealing with dying and death. Figure 6 shows how this synthesized finding is constructed.
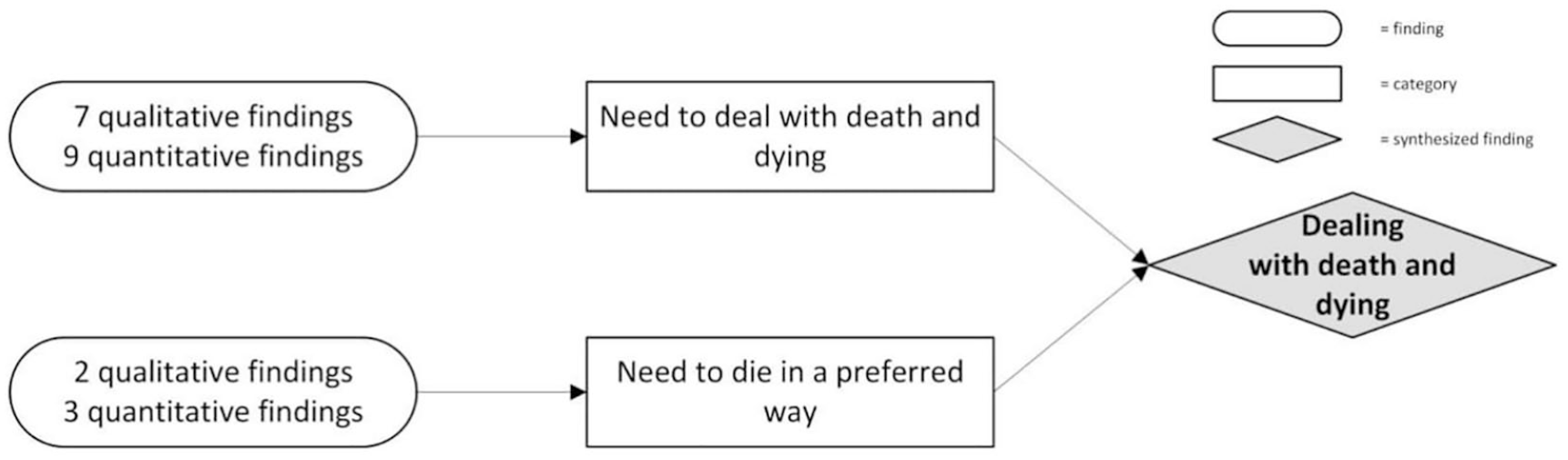
Synthesized finding 5: dealing with death and dying.
Patients expressed that they needed to deal with their spiritual issues and concerns about death and dying82,94,99 and difficulties concerning death’s meaning.76,81 Also, patients needed to reflect on the possibility of an afterlife.82,84,85,87 Patients expressed that they sometimes wanted to have conversations with a healthcare chaplain or other healthcare professionals about their impending death and its meaning.67,75,85,93 For some patients, it was vital that they could relate to their death through their religion.61,66 Patients also expressed socials needs considering their death: staying at home as long as possible, 57 planning the funeral64,75 and what should happen with their bodies after they died. 64 Moreover, patients expressed that they wanted to die in their preferred way. For some, this was a spiritual need, wanting to die with peace of mind.61,66 For others, this had to do with not dying alone or wanting to die at a preferred location, such as their own home.73,75
Discussion
This study aimed to gain insight into the social and spiritual needs of patients with a life-limiting illness and distinguish between these needs. This systematic review confirmed that these patients report various needs in the palliative phase of their illness, some of which are categorized as either social or spiritual needs. These needs can be summarized in five synthesized findings: being autonomous, being connected, having meaning, having a positive outlook, and dealing with death and dying.
These synthesized findings are consistent with literature focusing on patients’ social and spiritual needs. Primary studies, however, focus either on patients’ palliative care needs in general54,57,58,60,62,64,65,69–71 or on specifically patients’ spiritual needs,55,56,59,63,66–68,72,74,82,84,85,87 and focus less on social needs 61 as the primary outcome. Measurement instruments used in survey studies often pay less attention to social needs than they do to spiritual needs.
Looking at the synthesized findings, it becomes apparent that the expressed needs and analytical themes encompass both social and spiritual needs. “Being autonomous”, “being connected,” and “dealing with death and dying” encompass social and spiritual needs, whereas “having meaning” and “having a positive outlook” lean more toward spiritual needs alone.
Strengths and limitations
This study’s first strength is the extensive search using a search strategy that focused on “spiritual needs,” “social needs,” and related terminology. In contrast to other reviews, the aim was not to identify needs but to synthesize and aggregate the themes other studies identified. 31 Next, a multidisciplinary team of experienced researchers performed the analysis, enabling them to look at the results from different disciplines’ perspective and present them accordingly. Another strength lies in the inclusion of qualitative and quantitative studies, enabling the research team to cover the entire research field’s scope. The resulting meta-aggregation permitted the researchers to assess the themes that previous studies addressed and identified. 47 The use of an integrated design allowed both qualitative and quantitative studies in the meta-aggregation. 34 Previous reviews only incorporated qualitative studies.30–32 (Cagle, Bunting and Kelemen, 2017).
The choices that were made came with some setbacks. Firstly, this review’s search strategy included terms such as “social” and “spiritual,” thereby already narrowing the search in advance. Patients themselves do not frame their needs in this way. Therefore, a search strategy only including “needs” would have been more transparent. However, initial searches resulted in over 30,000 results this way, making the study unmanageable. Therefore, the research team decided against this option. Secondly, seeing patients’ needs in light of either the social or spiritual dimension will always be based on interpretations by the researchers conducting the analysis. Since definitions of the social and spiritual dimensions overlap, associating needs with these dimensions can always be disputed. We minimized this bias by interpreting reported needs in a multidisciplinary research team with shared expertise and competencies in chaplaincy and nursing and establishing a partnership with a delegation of social workers. Lastly, although the integrative design suits the research question well in this study, it also comes with limitations. This design is inherently less reproducible and transparent due to the design’s iterative nature. There may also be some issues concerning the combining of qualitative and quantitative methodologies of the included studies. While by qualitizing the data from quantitative studies, the findings become comparable, one might still oppose the design’s assumption that methodological differences can be minimized. 101
Socio-spiritual approach
As mentioned above, the synthesized findings reflect patients’ social and spiritual needs. However, patients themselves do not label their needs as “social” or “spiritual.” Needs often comprise multiple dimensions, including the social and spiritual dimension. Consequently, expressed needs are open to interpretation: the same expression might refer to both a social and a spiritual need depending on the patient’s point of view. Therefore, patients’ needs should not be interpreted based on their first expression. An in-depth exploration of these needs is necessary to recognize and understand, and subsequently, distinguish the underlying dimensions to provide appropriate care.
Within the framework of multidimensional symptom management, we propose a socio-spiritual approach to patients’ needs. This approach involves regarding social and spiritual needs as tantamount on a linguistic level but warrants distinguishing them when explored in-depth. This approach honors and preserves the real-life multidimensionality of patients’ needs and raises awareness of the linguistic similarities in the expression of social and spiritual needs.
The socio-spiritual approach fits and elucidates the first step in the method of palliative reasoning: mapping patients’ problems. 102 Physical and psychological symptoms and needs are often clearly expressed by patients and clearly understood by healthcare professionals. However, social and spiritual needs share a common terminology making it complex to understand them based on their expression alone. Therefore, in-depth exploration of social and spiritual needs is necessary for answering the question “what does it mean?” – as is the case for all multidimensional needs – and for answering an even more fundamental question “what does this mean to you?”.
Adopting a socio-spiritual approach to identifying patients’ needs benefits both patients and healthcare professionals. Patients can express their needs in the way they seem fit and healthcare professionals can assess these needs holistically. This makes sure that the interpretation of patients’ needs is not prematurely reduced to categories that do not fully match with what is at stake for them. Next, being aware of the overlap between social and spiritual needs can encourage healthcare professionals to explore patients’ needs, thus guaranteeing appropriate interventions.
As such, the socio-spiritual approach facilitates and demands interdisciplinary teamwork to combine healthcare professionals’ expertise to decide which discipline is best suited to meet the needs.
Recommendations for healthcare practice and future research
Based on the findings of this review, the socio-spiritual approach is recommended in multidimensional symptom management. The overlap in the expression of social and spiritual needs can create confusion in day-to-day care. Therefore, social and spiritual needs should be carefully assessed and interpreted by the healthcare team to assign patient-tailored care. To understand and distinguish between patients’ social and spiritual needs and facilitate patient-tailored care, healthcare professionals of all disciplines require evidence-based information on exploring, assessing, and recognizing the overlap between these needs.74,82,103
Patient Reported Outcome Measures (PROMs) can help patients think about their own needs and wishes and help focus on what matters at the moment, supporting the in-depth exploration. 74 The use of PROMs can reinforce patient autonomy and improve patient-professional communication and communication between professionals. Furthermore, PROMs support monitoring needs throughout time, especially when continuity in day-to-day care cannot be guaranteed in person due to part-time work and irregular work hours.104,105
Hence, more clinical applicable PROMs should be developed and employed, for example, PROMs that are not too demanding for patients or too extensive in their setup, as is the case for research purposes. The Utrecht Symptom Diary – 4 Dimensional (USD-4D) is a PROM used in palliative care to signal and monitor patients’ symptoms and needs in all four dimensions: physical, psychological, social, and spiritual. Five items concern both the social and spiritual dimensions. A recent study showed that patients interpret these items as either social and spiritual, or both, depending on their context. 106 Since patients use the same vocabulary to express their social and spiritual needs, healthcare professionals should always be aware that they explore what patients mean when expressing their needs. As a result, patients can indicate how they interpret these items. This, in turn, helps healthcare professionals in appointing the appropriate disciplines when an intervention is necessary.
Future research should focus on patients’ needs being multidimensional and not referring to solely one dimension. This review showed how this holds for social and spiritual needs. In the long run, this could lead to the use of PROMs in which the physical, psychological, social, and spiritual dimensions are integrated so that patients’ needs are not drawn apart in advance along the boundaries of dimensions. Furthermore, more research should focus on the social dimension of palliative care as a separate domain.
Conclusion
This review identified five synthesized findings that encompass patients’ social and spiritual needs: being autonomous, being connected, having meaning, having a positive outlook, and dealing with death and dying. These findings were synthesized from both qualitative and quantitative studies.
Patients do not distinguish between social and spiritual needs themselves. However, healthcare professionals should do so to allocate appropriate, patient-tailored care. The socio-spiritual approach to patients’ needs raises awareness about linguistic similarities in expression between social and spiritual needs that should be explored in-depth. Hence, this approach honors and preserves the multidimensionality of patients’ needs and enables comprehensive palliative care. Clinical applicable multidimensional PROMs can support identifying and exploring patients’ social and spiritual needs.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163211010384 – Supplemental material for Toward a socio-spiritual approach? A mixed-methods systematic review on the social and spiritual needs of patients in the palliative phase of their illness
Supplemental material, sj-docx-1-pmj-10.1177_02692163211010384 for Toward a socio-spiritual approach? A mixed-methods systematic review on the social and spiritual needs of patients in the palliative phase of their illness by Tom Lormans, Everlien de Graaf, Joep van de Geer, Frederieke van der Baan, Carlo Leget and Saskia Teunissen in Palliative Medicine
Footnotes
Authorship
All authors contributed to the development of the conception and design of this work. TL and EdG acquired, analyzed, and interpreted the data, and drafted the article. JvdG contributed to conceptualizing this review and the data analysis. FvdB contributed to the analysis. CL and ST contributed to the concept analysis and interpretation of the data. All authors have approved this version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Zonmw supported this work (grant number 844001307, 2017).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.