
Abstract
Background:
Advance care planning for children with palliative care needs is an emotionally, legally and complex aspect of care, advocated as beneficial to children, families and health professionals. Evidence suggests healthcare professionals often avoid or delay initiation. An overview of evidence on the factors that influence and impact on the health care professional’s initiation of paediatric advance care planning process is lacking.
Aim:
To review and synthesise evidence on the factors associated with health care professional’s decision to initiate paediatric advance care planning.
Design:
Systematic integrative review using constant comparison method.
Data Sources:
Electronic databases (CINAHL, PubMed, PsycINFO, Ovid MEDLINE, EMBASE, Web of Science and Cochrane) using MeSH terms and word searches in Oct 2019. No limit set on year of publication or country. Grey literature searches were also completed.
Results:
The search yielded 4153 citations from which 90 full text articles were reviewed. Twenty-one met inclusion criteria consisting of quantitative (n = 8), qualitative (n = 6) and theoretical (n = 7) studies.
Findings revealed overarching and interrelated themes ‘The timing of initiation’, ‘What makes an initiator, ‘Professionals’ perceptions’ and ‘Prerequisites to initiation’.
Conclusions:
This review provides insights into the complexities and factors surrounding the initiation of advance care planning in paediatric practice. Uncertainty regarding prognosis, responsibility and unpredictable parental reactions result in inconsistent practice. Future research is required to inform intervention to assist health care professionals when initiating paediatric advance care planning conversations.
Keywords
Advance care planning in paediatrics is advocated however uptake remains low.
Evidence to date is from adult populations and questions exist around transferability to a paediatric population.
Delays in the initiation of advance care planning for this population result in discussions taking place at times of crises, perhaps when death is imminent which results emotionally charged discussions occurring.
Initiation of advance care planning in paediatrics is influenced by an array of personal, social, cultural and organisational factors.
It outlines important factors to consider when initiating paediatric advance care planning conversations with parents – such as developing a rapport, professional knowledge of paediatric advance care planning, educating the parent and approval to talk on the topic.
Initiation must happen as soon as opportune following recognition of a life limiting illness and should be rooted in the knowledge that paediatric advance care planning encompasses wishes whilst living as well as future planning and decision making and should not be focused solely on documenting restrictions to treatment and end of life plans.
Professionals must be aware of the complexities of initiation but must also recognise that these should not act as a barrier to ensuring meaningful conversations occur.
The use of a behaviour change theory in further research may provide evidence and on aspects of behaviour which could be adapted or changed to reduce the delay and avoidance behaviour evident in current practice.
A standardised approach supported by education, guidelines and clinical tools is required to ensure paediatric advance care planning is initiated as a process and not seen as an anxiety evoking ‘one time’ conversation.
Background
Globally, end of life planning, commonly referred to as advance care planning, is advocated in policy for both adult1,2 and paediatric palliative care.3 –6 Advance care planning is a term used to describe ongoing conversations, between a person and family members and health professionals about future care and preferences. In paediatrics, advance care planning is supported by parents7 –9 and professionals 10 and linked to positive outcomes such as enhanced quality of life, care, satisfaction and reduced distress for patients and families.10 –12 However, whilst it is recommended that paediatric advance care planning discussions start at the point of diagnosis or recognition of a life-limiting or life-threatening condition there are no formal national or international guidelines on how, when and where such conversations are conducted, and by whom. Consequently, the literature suggests it has not been systematically adopted in practice. 13
To date, the majority of evidence for paediatric advance care planning is derived from adult populations, 11 which does not recognise the substantial differences in terms of competence, legalities and degree of parental involvement. Existing research on paediatric advance care planning has focused on implementation, effectiveness8,14 –22 and the development of programs and documentation. It can be argued however that there has been less attention given toward the process of initiation of advance care planning in practice. According to Van der Steen et al., 23 in their work with patients with dementia, initiation of an advance care plan refers to starting a discussion/decision making process, not necessarily resulting in concrete plans. Studies undertaken to date recognise that health care professionals are ideally placed to initiate such discussions, however they are often reluctant to do this due to difficulties in prognostication and fears that parents lack understanding or are not emotionally ready to engage.8,15,18,24 –27 Although parents and minors are at liberty to start these discussions, the onus is on professionals to respond to parental and patient cues, or to ensure the conversation is started. Parental expections are that clinicians should take the lead. 28 Whilst the time and manner in which advance care plan discussions are initiated is recognised as ‘the critical juncture, upon which all else hangs’, 29 (p2) there is a paucity of data regarding the factors influencing the initiation of paediatric advance care planning from the health professional perspective.
Aim
To appraise and synthesise current evidence regarding the factors influencing initiation of paediatric advance care planning discussions from the health professional perspective.
Methods
Design
A systematic integrative review using guidelines developed by Whittemore and Knafl. 30 This enabled the combination of diverse methodologies, providing a comprehensive review of the topic.31,32
Search strategy
A search for existing literature to identify relevant papers on the initiation of advance care plans for children and young persons (<18 years) by health professionals was conducted using five online databases: CINAHL (EBSCO), MEDLINE (Ovid), EMBASE (Ovid), PsycINFO (Ovid) and Scopus.
Informed by previous work by Van der Steen et al. 23 initiation was defined as (i) starting a discussion, not necessarily resulting in plans, (ii) starting the decision making or a decision-making process, i.e., actual planning of care or (iii) starting a written Advance care plan or Emergency care plan to be shared with health professionals, emergency services, educationalists etc. Multiple search terms were used informed by the literature.8,14 –21,33 –37
The search was extended from studies which were exclusively about initiation to include papers which included initiation as part of wider discussion. Papers on specific components of paediatric advance care planning such as end of life decision making and decisions on withdrawing and withholding treatment and resuscitation, which referred to initiation were also included. Keywords included: Advance care plan, Children, Palliative care, End of life care, Health care professionals, decision making, conversations, discussions or initiation. Full details can be found in (Appendix 1).
Medical Subject Headings (MeSH) and Boolean terms were used to efficiently identify the most relevant data, alongside free text, synonyms and truncation (Table 1) The search, screening and selection, was undertaken independently by two authors (KC & FH) and differences were mediated by a third reviewer (SM). The search was completed in October 2019 and was not limited by year of publication.
Search terms - Integrative Literature Review.
Truncation symbol.
A grey literature search of Ethos, Proquest, Open Grey, Prospero, Agency for Health Care Research and Quality, Google Scholar and Research Gate was also undertaken. Members of the International Children’s Palliative Care Network ICPCN (n = 1842) were contacted by e-mail to identify grey papers and guidance to ensure the search process was fully complete. Additionally, reference lists of relevant studies were hand searched. The search resulted in a sample of 4153 articles. Considering the inclusion and exclusion criteria, 21 studies remained (see Figure 1).
PRISMA Initiation of paediatric advance care planning integrative literature review.
Inclusion and exclusion
Following paper identification and de-duplication, titles and abstracts were screened, and full papers were assessed for eligibility.
The inclusion and exclusion criteria (Table 2) were applied to ensure only those papers applicable to the review aim were included. Neonatal and perinatal studies were excluded following a team discussion as deemed to be a highly specialised area requiring a separate search. Text and opinion papers were included if specific to the inclusion criteria.
Eligibility criteria.
Quality appraisal
Two reviewers (KC&FH) independently appraised the methodological quality of all the papers prior to their inclusion in the final review using Critical Appraisal tools from the Joanna Briggs Institute (JBI): for qualitative studies, 38 for quantitative 39 and for non-research text and opinion 40 (Appendix 2). The standardised JBI tools use a comprehensive checklist with Yes, No, Unclear and Not Applicable as possible answers to 9 or 10 questions such as ‘Does the source of opinion have standing in the field of expertise?’ Findings are extracted and assigned a level of credibility. 41 The methodological quality was assessed by assigning low (a score below 49%), medium (50–74%) or high (75+%) score. Scores were computed by counting the number of ‘Yes’ answers and expressing them as a percentage of questions in the tool (Appendix 2) to ensure fair comparison as the number of questions in the tools varied. Non-research (text and opinion) had five high and two medium, quantitative three high, four medium and one low and qualitative four high and two medium scores. No studies were excluded based on the ascribed quality rating although, it was included as a variable in the analysis stage and, in general, those of lower rigour contributed less.
Data extraction and analysis
Data was extracted from the final papers independently by two reviewers (KC&FH) using a generic data extraction form and disagreements mediated by a third reviewer (SM) (Table 3). The data extraction process was based on the four stages identified by Whittemore and Knafl
30
that is, data reduction, data display, data comparison and conclusion drawing. Finally, given the diversity of methodologies, the data were synthesised using constant comparison method
42
which facilitates the identification of patterns, variations and relationships.
43
This resulted in
Data extraction table.
Results
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2015 guidelines for article selection 60 was used to report this review.
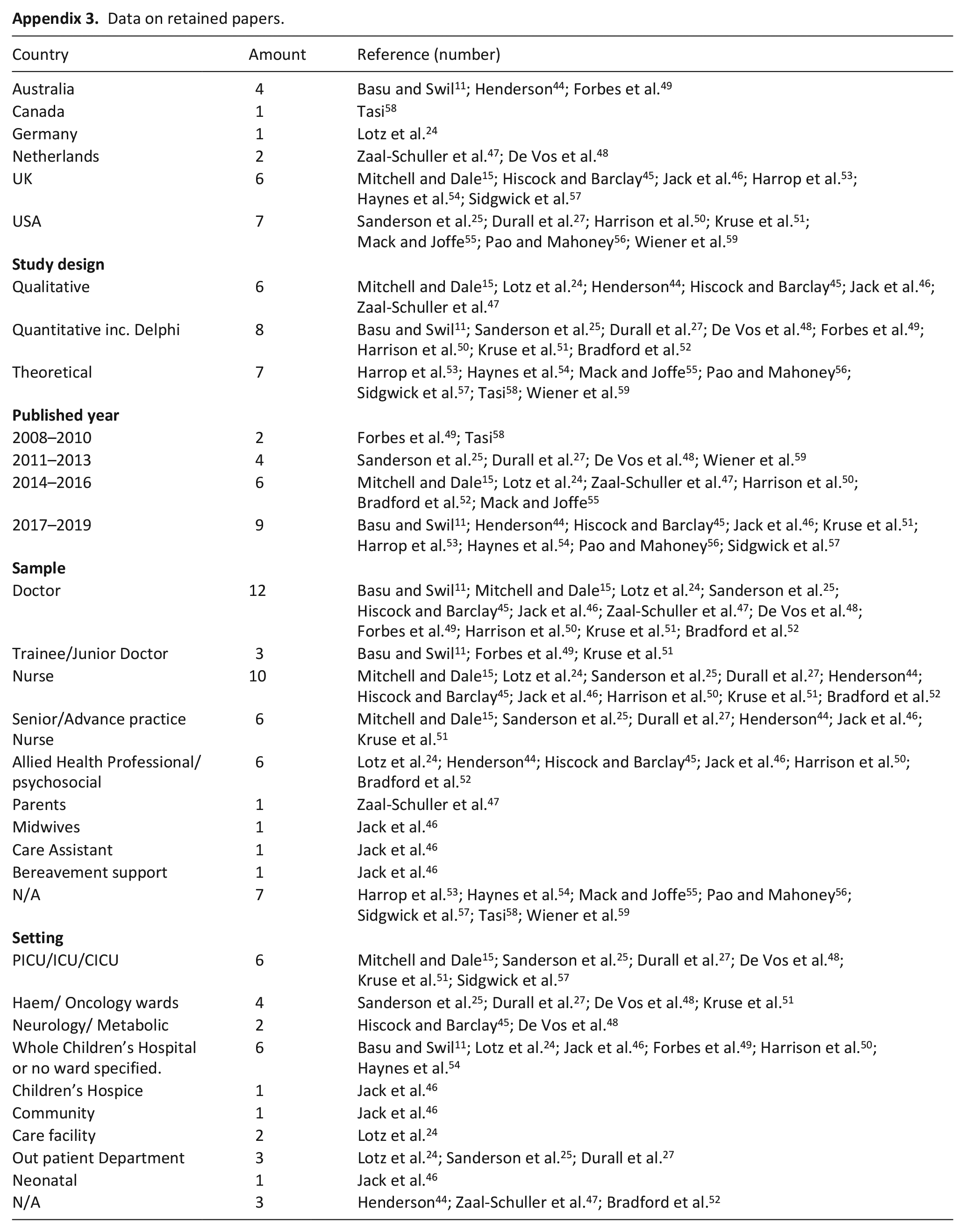
In total 21 papers were included in the final analysis. More than half of the papers were about the generalities of paediatric advance care planning 11,15,24,27,45,46,53 –56,58,59 with only one study focused exclusively on initiation of advance care planning in children. 11 The reminder of the papers centred on discussions and decision making about end of life,44,47,48,50,57 resuscitation,25,51 withdrawal of treatment 49 and one on components of early paediatric palliative care consultations. 52 All the papers stemmed from developed countries, seven from the United States,25,27,50,51,55,56,59 four from Australia11,44,49,52 one each from Canada 58 and Germany, 24 two from Netherlands47,48 and six studies from the United Kingdom.15,45,46,53,54,57
Fourteen papers were empirical i.e.: quantitative (n = 8)11,25,27,48 –52 of which one was a consensus-based method, 52 qualitative (n = 6).15,24,44 –47 Seven papers were professional reviews.53 –57,59 or position statements. 58 The earliest published paper was 2008 with nine published since 2017. The most common settings for initiation were intensive care15,25,48,51,57 and oncology wards25,27,48,51. Information re country, year, setting and sample for the included papers are available in Appendix 3.
Four key themes emerged which were found to influence the initiation process, (1) Timing of initiation, (2) What makes an initiator, (3) Professionals perceptions and (4) Prerequisites to initiation.
Theme 1: The timing of initiation
All papers in the review advocated that paediatric advance care planning be undertaken, however discrepancies in the initiation process were evident with regards to timing. There is differing evidence on the appropriate timing and diverse triggers used for the initiation and/or delay of starting advance care planning conversations. Timing in all the papers referred to the stage in the illness trajectory, with only one referring to the time of their hospital experience i.e. discharge. 24 None of the papers indicated time of day for either family or professionals being significant and only two indicated that the professional needs to ensure enough time available15,57 with the time required acknowledged as a challenge 59 along with the acknowledgement of other clinical demands on the professionals. 15 Critically, one paper states that advance planning discussions in children need not necessarily be lengthy 56 if the groundwork of the relationship and permissions has been established indicating the importance of initiation.
In total, 20 papers11,15,24,25,27,44 –49,51–59 reported on the stage of the illness trajectory for the initiation of advance care plan discussions. A focus on the correct ‘time’ and the ‘right time’ for both health care professionals and the patient/family, underpinned this debate. Most studies advocate discussion to be started early, ideally close to diagnosis.11,24,25,27,46,54,58,59 However the stated timing triggers for initiation varied from occurring when the child was stable11,25,27,57 –59 or to when the goals of care changed,53,58 to responding to physical deterioration and not being expected to survive the next 12 months. 54 No paper however, provided clarity on what ‘early’, ‘close to diagnosis’, ‘end of life’, ‘late’ and ‘following deterioration’ means in practice though these were terms frequently used.
‘Early’ initiation was viewed as beneficial for the health professional, family and child. For example, it was believed to enable parallel planning to occur,46,57 relationships to be developed between the health professional and family11,15,44,46,47,52,53,56,59 and potentially result in less aggressive intervention and an increase in palliative care support. 55 Several studies indicated that starting discussions in a proactive manner enabled a staged approach with the more ‘difficult’ components of advance care planning being discussed when health professionals and families have had time to get to know each other and develop a relationship.11,15,44,46,47,52 –54,57,59 Using ‘natural’ triggers such as following an episode of deterioration,47,55 prior to paediatric intensive care admission15,55 and families’ asking leading questions 46 was indicated as an opportunity to introduce the topic or to assess family readiness to have an advance care planning discussion.
In practice however, it was recognised that paediatric advance care planning often occurs late, often when death is close,11,25,27,45,51 triggered by a crisis and often after multiple deteriorations.11,25,27,47 Several factors were cited as reasons to avoid starting these conversations, such as uncertain prognosis11,15,24,27,47,49,55,56,58 or lack of health care team consensus prior to speaking to parents.15,44,48,57 However, Henderson 44 warned awaiting consensus may result in a further delay in the initiation of advance care planning discussions. In addition, perceptions that families are reluctant to discuss future care decisions prior to physical deterioration24,25,27,45 –47,49,54,55,57 and family dynamics25,27,56,58 resulted in delays in conversations occurring. The presence of disagreement, or fear of creating conflict between the health care team and family24,44,47 –49,56 and within the family25,27,56,58 were also identified as influencing factors.
One paper recognised the need for families to process news such as diagnosis before being ready for advance care planning 24 and others identification of specified situations where extra time would be needed – that of differences in language and religion 48 whilst others cautioned on ensuring enough time was made available.15,48
Theme 2: What makes an initiator?
Lead taker
Whilst the literature recognises that parents play an essential role in the advance care planning process, 47 this role is less clear when it comes to initiation.27,53,58 At the initiation stage the role of health professionals was viewed as vital, with the onus on them to start the discussion or at least inform parents accurately about paediatric advance care planning.11,15,27,44,45,48,53,54,57 –59 However, no consensus on which professional group was best placed to do this was reported, instead it included doctors,27,54,58,59 advanced nurse practitioners, 27 or members of the multidisciplinary team (MDT) without specifying which member11,15,44,53 and the difficulty of identifying the ideal health professional in the team acknowledged. 57
Rather than naming a specific health professional who has responsibility, several papers11,53,56 –58 present criteria for appropriateness of the professional e.g. that it should be based upon quality of health professional and family relationship.53,56 –58 However, others suggest that the health professional should be the primary professional who has had responsibility for majority of care,11,58 or who is an expert in the disease, its pathway and the impact on the child’s quality of life. 53 Only one study 57 identified requirements for an ideal initiator – motivation, time, emotional capacity, expertise in the child’s condition and palliative care knowledge. Doctors were identified as the health professional who most often undertake these conversations49,50 however the nurse (grade unspecified) would provide the confirmation to the doctor of the patient’s physical decline and family dynamics which then acted as a catalyst for action.15,47
The choice of the doctor to start such conversations was justified based on the evidence that although they felt discomfort addressing paediatric advance care planning24,44,51,57,59 they were often more comfortable initiating discussions rather than nurses or psychosocial staff.50,51 However, reticence on the part of the health professional, including doctors, to initiate conversations was evident.24,44,51,59
Professionals’ learning processes
It was perceived a correlation existed between increased clinical exposure,11,49,57 knowledge and training, 50 regarding the attitude and ease of approach of the health professional. Doctors were often hesitant to take the lead citing a lack of knowledge and training as key reasons to avoid taking the role.11,15,24,44,51,59 Reports suggest that health professional knowledge and practice were learned in an ad-hoc manner on the job from observations and discussions with experienced colleagues.49,50,57 Furthermore, formulating the message and knowing how to verbalise difficult conversations, specifically, knowing the right words to use was indicated as problematic in several studies.11,24,27,44,46,53,55,56,58,59 Three papers indicated that health professionals did not know the right words to use.11,24,27 Prompts and conversation starter examples were suggested in eight papers.44,46,53 –56,58,59
Approach strategies
Preparing not just themselves but the family member prior to starting an advance care planning conversation was suggested in one paper 53 which advocated giving a warning shot that planning discussions would happen in the future. Another method of introduction was the use of parallel planning, identified in two papers46,57 where palliative care is introduced alongside curative care and the advance care plan reflected various potential directions the illness/treatment may take the child. Another introduction suggestion was extoling the benefits to parents, such as not having to repeat the same story every admission or to new health professionals. 46
Theme 3: Professionals perceptions
Central to the initiation of advance care planning discussions were health professionals’ sensitivities of family reactions and receptiveness, and their own perceptions on palliative care.
Professionals’ perceptions of families
Whilst the inclusion of parents in open and honest discussions was advocated,53,55,59 health professional’s perceptions of the family reaction 55 and concerns about causing distress,11,46,49,55 taking away hope24,55,56,58,59 or broaching topics for which the family are perceived either not to be ready24,25,27,46,47,49 or do not wish to engage in, 55 impacted on the initiation of conversations. Moreover, health professional’s assumptions of a family’s lack of understanding of the diagnosis, prognosis and treatment24,25,27,44,47,52,55 meant that this also acted as a deterrent to start discussions. Health professional worries about offending families of other religious and cultural backgrounds to their own11,15,24,49,55 was also found to impact who takes the lead, timing, and the message delivered. The cultural, religious and belief systems of the health professional was recognised as influencing the process, with research suggesting their attitude to death and advance care planning could influence their ability, confidence and process of initiation.11,55,56 However, one Australian study refutes these claims suggesting health professionals lack of understanding of families’ religious beliefs was of greater concern. 49
Professionals’ perceptions of palliative care
Health professionals were also found to hold beliefs relating to exclusivity of palliative care treatment and active treatment15,52,58 and a lack of certainty of when to refer to palliative care. 55 Many health professionals essentially viewed paediatric advance care planning as a decision-making process24,47,48,53,55,56,59 focusing on decisions relating to the withdrawal or withholding of life sustaining treatment and resuscitation.
Theme 4: Prerequisites to initiation
Findings illustrate that numerous prerequisites play a fundamental role in initiation of advance care planning discussions.
Separate from the requirements identified regarding time of initiation and the need for consensus of professionals involved, other health professionals’ prerequisites to initiation were identified within the 21 papers including: Training,11,15,24,44,51,59 with formal training linked to increased professional’s comfort in discussing death with families; 50 Associated with training, but not dependent on it, the possession of good communication skills15,44,49,50,56,58 was identified as a requirement; The need for parents to have an understanding of paediatric advance care planning prior to starting 54 and to indicate their readiness to participate24,25,27,46,53,54,56,59 was identified as necessary. Three papers also indicated that, where appropriate, the patient must also indicate participation readiness;45,56,59 The need to have a clear diagnosis and prognosis or, in the absence of these, evidence of a deteriorating condition or imminent death.25,27,47,49,54,59
Communication about paediatric advance care planning was seen to be interdependent on other difficult conversations such as the need for open discussions of disease progression and prognosis, including prognostic uncertainties;11,27,49 Four papers indicated the need and importance for an appropriate physical setting for the initiation of discussions24,44,46,56 and specified the disadvantage of engaging in such conversations in a busy clinical environment, recommending the importance of planning the environment44,46,56 and that health professionals initiate the discussion away from the child.44,46
Discussion
Main findings/results of the study
This integrative review approach uncovered a scarcity of evidence on the initiation of paediatric advance care planning with only one study, 11 focusing on this. There is diversity in practice across countries resulting in no international evidence base. There was no consistent practice regarding initiation, rather findings suggest this is a complex process influenced not only by actual issues such as diagnosis, or parent indication of readiness but also by perceived issues such as families potential negative reactions or that it was another professionals responsibility. The influence, if any, on the initiation process of the complexities of dealing with a varied range of diagnosis, family situations, parental obligation to protect and societal predisposition in favour of life 59 that envelops paediatric clinical care requires further exploration.
Papers revealed three overarching and largely interrelated areas which in turn result in indecision.
In
The making of an initiator
In the absence of a nominated leader for initiating advance care planning, uncertain qualities, skills and leadership influenced who took on the initiation role and how it was performed. For example, resistance to initiation was closely linked to health care professional’s own uncertainty in responding in a vulnerable situation.10,44 In the absence of tools and guidelines to assist professionals they relied on their instinctive feelings and perceptions to gauge a parent’s openness to engage in end of life discussions. This was further compounded by their lack of competence, knowledge and confidence about how to initiate, respond to and deal with such conversations.11,15,24,44,51,59
With regards to who takes the lead to initiate advance care plan discussions, some studies rationalised this as the doctor’s domain27,54,58,59 whilst others the responsibility of a specialist nurse. 27 Yet there was no consensus on whose role or responsibility it was to lead such discussions resulting in the ‘bystander effect’ occurring in practice, where health care professionals from one discipline waited for other professionals, or indeed families, to start the conversation. 62 Being part of a large group implied that no single person was necessarily identified as responsible for initiation therefore individuals could not be held responsible for inaction. 63 The hope is that someone who knows the child, family, condition, symptoms more, who is better placed timewise and who has the experience and confidence, that is – the professional with the capability, opportunity and motivation will step up and lead the advance planning.
The importance of
To counteract and respond to the uncertainty of who, how and when to initiate healthcare professionals developed pre-requisites to be in place, to facilitate the initiation. For example, prognosis uncertainty required an expert in the condition to be the lead role.53,57 The unpredictable outcomes of the parent and the professional’s lack of confidence could be tempered by having a relationship with the parents.15,52 However, regardless of the number of pre-requisites that exist, what is apparent is that initiating discussions about advance care planning is challenging and raises many dilemmas for healthcare professionals. In practice, professionals may need to realise that uncertainty may be unavoidable and inherent, and no universal guideline can address the unique situational, contextual, organisational and personal issues that surround such discussions. Harnessing, acknowledging and working with this uncertainty, through honest negotiations with parents, was recognised as necessary53 –55 with the overall aim that such discussions are initiated, rather than delayed.
Strengths and limitations
This is the first integrative review exploring the initiation of paediatric advance care planning from the health professional viewpoint. The methodology adhered to the PRISMA statement and the quality of all studies were critically assessed using methodological criteria. Although based on a comprehensive search and despite no geographic restrictions being placed on the search strategy all studies stem from developed countries with papers exclusively from only three continents (North America, Australia and Europe) which limits the generalisability of the findings. This review did not include the factors associated with parent initiation of advance care plans. Whilst comprehensive terms linked to initiation of paediatric advance care planning were used to guide the search it is recognised it may not have been able to capture all the available evidence. Recognition of the international heterogeneity in how paediatric advance care planning is defined, and analysed, questions the generalisability of the process and findings. This review was limited in that it included the initiation of discussions of components of paediatric advance care plans, such as treatment limitation, as well as papers specific to paediatric advance care planning. This broadening of the search was necessary due to the limited literature available specifically on the initiation of paediatric advance care planning and to recognise that many professionals see components, such as treatment limitations, as the focus of advance care planning rather than family and child goals and wishes with treatment decisions a component, not the main focus and entirety. Finally, this review only included papers with easily available translation into English therefore papers existing in other languages, were not included in this review.
What this study adds?
This study reinforces previous studies on components of paediatric advance care planning and highlights the lack of evidence in the general topic and specifically initiation. An array of personal, social, cultural and organisational factors influences how, who and when paediatric advance care planning is initiated. Developing a rapport, professional knowledge of paediatric advance care planning, educating the parent and approval to talk on the topic are some of the factors outlined as important to consider when initiating paediatric advance care planning conversation with parents.
Implications for practice, theory or policy
It is not possible to recommend effective ways of initiating paediatric advance care planning as the evidence base is limited therefore studies investigating behavioural aspects of current effective initiation are required. Initiation should be rooted in the knowledge that paediatric advance care planning encompasses wishes, future planning and decision making of the child and family whilst living and should not be focused solely on documenting restrictions to treatment, end of life and funeral plans. Therefore, to ensure families have the time to learn to make decisions and to consider options, initiation of paediatric advance care planning must happen as soon opportune following recognition of a life limiting illness and health professionals must recognise that they hold the key to this happening. Professionals must be aware of the complexities of initiation but must also recognise that these should not act as a barrier to ensuring meaningful conversations occur. The use of a behaviour change theory in further research may provide evidence and on aspects of behaviour which could be adapted or changed to reduce the delay and avoidance behaviour evident in current practice. A standardised approach supported by education, guidelines and clinical tools is required to ensure paediatric advance care planning is initiated as a process and not seen as an anxiety evoking ‘one time’ conversation.
Conclusion
This review found a dearth of evidence specifically focusing on the initiation of paediatric advance care planning. Overall evidence suggests that health professionals recognise early initiation to be the ideal, and they play a key role ensuring this. Yet ambiguity regarding prognosis, parents’ reactions, who leads, and the skills needed to engage in such conversations act as deterrents in initiating paediatric advance care planning in clinical practice. Consequently, advance care planning conversation occur too late without time for the child and parent to reflect and enact their goals or wishes. Further research is needed on the experience of the initiation process from the professional, parent and child perspective to enable strategies to be developed to ensure conversations occur earlier and are of benefit to all. The identification of behavioural factors impacting on initiation of paediatric advance care planning may inform the development of interventions and to ensure the focus is on the appropriate changeable aspects. Evidence is required, perhaps through the use of a behaviour change theory such as capability, opportunity and motivation theory (COM-B) 71 in further research to provide evidence on aspects of behaviour which could be adapted or changed to reduce the delay and avoidance behaviour evident in current practice and to ultimately make initiation work for everyone.
Footnotes
Appendix
Data on retained papers.
| Country | Amount | Reference (number) |
|---|---|---|
| Australia | 4 | Basu and Swil 11 ; Henderson 44 ; Forbes et al. 49 |
| Canada | 1 | Tasi 58 |
| Germany | 1 | Lotz et al. 24 |
| Netherlands | 2 | Zaal-Schuller et al. 47 ; De Vos et al. 48 |
| UK | 6 | Mitchell and Dale 15 ; Hiscock and Barclay 45 ; Jack et al. 46 ; Harrop et al. 53 ; Haynes et al. 54 ; Sidgwick et al. 57 |
| USA | 7 | Sanderson et al. 25 ; Durall et al. 27 ; Harrison et al. 50 ; Kruse et al. 51 ; Mack and Joffe 55 ; Pao and Mahoney 56 ; Wiener et al. 59 |
|
|
||
| Qualitative | 6 | Mitchell and Dale 15 ; Lotz et al. 24 ; Henderson 44 ; Hiscock and Barclay 45 ; Jack et al. 46 ; Zaal-Schuller et al. 47 |
| Quantitative inc. Delphi | 8 | Basu and Swil 11 ; Sanderson et al. 25 ; Durall et al. 27 ; De Vos et al. 48 ; Forbes et al. 49 ; Harrison et al. 50 ; Kruse et al. 51 ; Bradford et al. 52 |
| Theoretical | 7 | Harrop et al. 53 ; Haynes et al. 54 ; Mack and Joffe 55 ; Pao and Mahoney 56 ; Sidgwick et al. 57 ; Tasi 58 ; Wiener et al. 59 |
|
|
||
| 2008–2010 | 2 | Forbes et al. 49 ; Tasi 58 |
| 2011–2013 | 4 | Sanderson et al. 25 ; Durall et al. 27 ; De Vos et al. 48 ; Wiener et al. 59 |
| 2014–2016 | 6 | Mitchell and Dale 15 ; Lotz et al. 24 ; Zaal-Schuller et al. 47 ; Harrison et al. 50 ; Bradford et al. 52 ; Mack and Joffe 55 |
| 2017–2019 | 9 | Basu and Swil 11 ; Henderson 44 ; Hiscock and Barclay 45 ; Jack et al. 46 ; Kruse et al. 51 ; Harrop et al. 53 ; Haynes et al. 54 ; Pao and Mahoney 56 ; Sidgwick et al. 57 |
|
|
||
| Doctor | 12 | Basu and Swil 11 ; Mitchell and Dale 15 ; Lotz et al. 24 ; Sanderson et al. 25 ; Hiscock and Barclay 45 ; Jack et al. 46 ; Zaal-Schuller et al. 47 ; De Vos et al. 48 ; Forbes et al. 49 ; Harrison et al. 50 ; Kruse et al. 51 ; Bradford et al. 52 |
| Trainee/Junior Doctor | 3 | Basu and Swil 11 ; Forbes et al. 49 ; Kruse et al. 51 |
| Nurse | 10 | Mitchell and Dale 15 ; Lotz et al. 24 ; Sanderson et al. 25 ; Durall et al. 27 ; Henderson 44 ; Hiscock and Barclay 45 ; Jack et al. 46 ; Harrison et al. 50 ; Kruse et al. 51 ; Bradford et al. 52 |
| Senior/Advance practice Nurse | 6 | Mitchell and Dale 15 ; Sanderson et al. 25 ; Durall et al. 27 ; Henderson 44 ; Jack et al. 46 ; Kruse et al. 51 |
| Allied Health Professional/psychosocial | 6 | Lotz et al. 24 ; Henderson 44 ; Hiscock and Barclay 45 ; Jack et al. 46 ; Harrison et al. 50 ; Bradford et al. 52 |
| Parents | 1 | Zaal-Schuller et al. 47 |
| Midwives | 1 | Jack et al. 46 |
| Care Assistant | 1 | Jack et al. 46 |
| Bereavement support | 1 | Jack et al. 46 |
| N/A | 7 | Harrop et al. 53 ; Haynes et al. 54 ; Mack and Joffe 55 ; Pao and Mahoney 56 ; Sidgwick et al. 57 ; Tasi 58 ; Wiener et al. 59 |
|
|
||
| PICU/ICU/CICU | 6 | Mitchell and Dale 15 ; Sanderson et al. 25 ; Durall et al. 27 ; De Vos et al. 48 ; Kruse et al. 51 ; Sidgwick et al. 57 |
| Haem/ Oncology wards | 4 | Sanderson et al. 25 ; Durall et al. 27 ; De Vos et al. 48 ; Kruse et al. 51 |
| Neurology/ Metabolic | 2 | Hiscock and Barclay 45 ; De Vos et al. 48 |
| Whole Children’s Hospital or no ward specified. | 6 | Basu and Swil 11 ; Lotz et al. 24 ; Jack et al. 46 ; Forbes et al. 49 ; Harrison et al. 50 ; Haynes et al. 54 |
| Children’s Hospice | 1 | Jack et al. 46 |
| Community | 1 | Jack et al. 46 |
| Care facility | 2 | Lotz et al. 24 |
| Out patient Department | 3 | Lotz et al. 24 ; Sanderson et al. 25 ; Durall et al. 27 |
| Neonatal | 1 | Jack et al. 46 |
| N/A | 3 | Henderson 44 ; Zaal-Schuller et al. 47 ; Bradford et al. 52 |
Acknowledgements
The authors would like to thank Kelly McCoo for her expert advice in generating the review search strategy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the UK Department of Employment and Learning (DEL) awarded to the lead author to undertake this research as part of a PhD.