
Abstract
Background:
There is a growing body of qualitative studies examining parents’ experiences of caring for a child with a life-limiting condition, coinciding with recent evidence that indicates an increasing incidence of paediatric life-limiting conditions. However, research focusing on fathers’ needs remains sparse and is often diluted among a predominant ‘mother’s voice’, raising questions about whether practices in clinical settings meet fathers’ needs.
Aim:
To provide an in-depth assembly of the current state of knowledge around fathers’ experiences of caring for their children diagnosed with life-limiting conditions and understand the implications for healthcare services and policies.
Design:
A meta-ethnography was conducted to synthesise findings from existing qualitative studies exploring fathers’ experiences of caring.
Data sources:
Four electronic databases (PubMed, PsycINFO, CINAHL and Science Direct) were searched up until April 2020. Qualitative studies exploring fathers’ care experience and published in English language were included. The Critical Appraisal Skills Programme (CASP) checklist was employed for study quality appraisal. No temporal limits were used.
Results:
Sixty-three studies met the inclusion criteria. Thirty life-limiting conditions were included. Based on responses from 496 fathers, a conceptual model was developed which translates key experiences within the fathers’ caregiving journeys. The overarching concepts identified were: the paradox of support, challenges in the caring process, ‘nobody thinks of men’, impact on family life and the fall of the curtain: an irrevocably altered world. These and associated sub-concepts are discussed, with recommendations for future research and practice provided.
Conclusion:
The findings indicate the value of a family-oriented approach to develop psychosocial interventions and support channels for fathers, thus empowering them whilst reducing the care-giving burden on the family unit.
Palliative care is a complex and gradual process aimed at supporting diagnosed children and their family members
Although children and their families may have many needs in common, research focusing on fathers’ experiences and contribution to their children’s healthcare is in its infancy
There is a need for further education of health care professionals and general practitioners regarding fathers’ needs and their experiences of caring for a child with a life-limiting condition
Fathers’ caregiving experiences are still shaped by assumptions about masculinity and fatherhood within medical care institutions and they often feel disconnected from and side-lined by health professionals
Fathers’ responsibilities in caring for their ill children and supporting the family unit as a whole are often under-represented in paediatric palliative care research and clinical settings
Fathers experience a multitude of difficult emotions and devastation at their child’s circumstances and own altered life, and attempt to manage these through a range of methods including dismissal, withdrawal, maintaining routine, acceptance and religion.
Understanding the types of caregiving that fathers offer their children may help to tailor the types and frequency of support a health professional might provide through the illness journey
Health professionals should acknowledge fathers’ involvement in the complexity of delivering care to their children, hold and provide opportunities for family members to work together to support each other in the process within a family-centred approach
A routine questionnaire to identify psychosocial risk factors for fathers (e.g. psychiatric disorder(s), depression, substance misuse) would help to highlight to clinicians those families at higher risk and in need of additional support
Introduction
Diagnosis of a life-limiting condition in paediatrics impacts the entire family, and there is an expanding body of qualitative research examining parents’ experiences in such circumstances, coinciding with recent evidence indicating an increasing incidence of paediatric life-limiting conditions.1,2 Although family members have care needs in common, 2 practices in the clinical setting that address parents’ needs, especially those of fathers, remain inconsistent and fragmented.3–7 This is exemplified by the sparsity of research exploring fathers’ experiences of caring for a child with a life-limiting condition. Research has predominantly explored the mothers’ role, either explicitly or within ‘parent’ or ‘family’ samples, without accounting for the different issues each parent faces.8–14 Mothers’ emotional and psycho-social caregiving needs have thus been extensively documented,9,15–18 whilst fathers are often the forgotten parent.1,19,20 In fact, research focusing solely on fathers is in its infancy, emerging less than two decades ago.4,21–24 This disproportion in the literature is not however reflective of the heavy responsibility fathers bear for their child’s personal and nursing care.7,25 We are seeing shifts in the traditional roles of ‘mother’ and ‘father’,3,25–28 and healthcare professionals need to be responsive to this trend7,21,29,30 and the changing needs of children and their families. 2
The complexity and varying morbidity of life-limiting conditions has been delineated by Together for Short Lives and international palliative care organizations into four broad categories, as follows: (a) conditions for which treatment may be feasible but can fail for example, cancer, cardiac anomalies, irreversible organ failures of heart, liver, kidney from anorexia, coeliac disease-related morbidities as oropharyngeal and oesophageal cancers; (b) conditions where long periods of intensive treatment are aimed at prolonging life and allowing participation in normal activities for example, Duchenne Muscular Dystrophy, cystic fibrosis; (c) progressive conditions without curative treatment options, where care is solely palliative and commonly extends over many years for example, metabolic or neurodegenerative conditions; and (d) irreversible but non-progressive conditions causing likelihood of severe disability and premature death through complications for example, severe cerebral palsy, multiple disabilities following brain or spinal cord injury, complex health care needs, and a high risk of an unpredictable life-threatening event or episode) (https://www.togetherforshortlives.org.uk/changing-lives/supporting-careprofessionals/introduction-childrens-palliative-care/categories-of-life-limiting-conditions/; http://www.icpcn.org/disease-categories/). Health policies internationally are advocating for children and parents’ active collaboration in health care decisions, stating it is key for the delivery of palliative care.31–36 There is therefore an immediate call to include fathers’ perspectives in their children’s care and treatment25,27 to inform appropriate psychosocial interventions and support channels. This would improve fathers’ understanding of the choices available in their child’s care 2 and participation in the advanced/anticipatory care planning.2,37 Synthesising available qualitative evidence is therefore timely, to enhance the usability of research-knowledge to date, in practice.
This meta-ethnography asks: what are fathers’ experiences of caring for their children with a life-limiting condition? This study aims to: (a) provide an in-depth assembly of the current state of knowledge around fathers’ experiences of caring for their children diagnosed with a life-limiting condition and (b) understand the impact of health care services and policies on fathers’ experiences. We aimed to generate a conceptual model, 38 which has not been previously attempted. However, one previous meta-synthesis focused on the care provided by fathers to their children with cancer under the influence of masculinities. 39 Other available meta-ethnographies have explored end-of-life decisions with parents of children with cancer, 40 parents’ experiences of their children’s life-limiting conditions,7,38 quality of life in children with brain tumours, 41 families’ experience of early discharge of their child with febrile neutropenia, 42 communication within primary care consultations 43 and parenting the infant in the neonatal intensive care unit. 44
Methods
Design
We used a meta-ethnographic approach 45 to synthesise studies on fathers’ experiences of caring for their children with life-limiting conditions. This meta-ethnography was reported according to the eMERGe reporting guidance,46,47 the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 48 and STARLITE 49 recommendations.
Search strategy
An initial bibliographic search for publications was undertaken using PubMed, PsycINFO, CINAHL and Science Direct. The comprehensive search was augmented, with hand searches of articles cited in reference lists and from relevant review papers.39,50 For papers that were unavailable online, authors were contacted to request copies. If access was not provided, they were excluded on the basis that the omission of some papers was unlikely to have a dramatic effect on the results. 51 Studies were included up until April 2020. Search terms available from the InterTASC Information Specialists’ Sub-Group Search Filter Resource 52 (www.york.ac.uk/inst/crd/intertasc/) were used to develop the search syntax. The full search strategy is provided in Supplemental online file 1.
Study selection
Published full text peer-reviewed qualitative studies exploring fathers’ experiences of their children’s life-limiting conditions were included. Studies were excluded if they failed to differentiate outcomes between mothers and fathers, focused on adjustment of children rather than fathers’ experiences, used quantitative methods, did not include children with life-limiting conditions, explored fathers’ experiences of children’s death and grieving or were not published in English. The archetypes set out in the Guide to Children’s Palliative Care 2 and the directory of life-limiting conditions 53 were used to select relevant papers. Studies that explored fathers’ experiences before and after a child’s death were included if findings had been reported separately.
Screening and data extraction
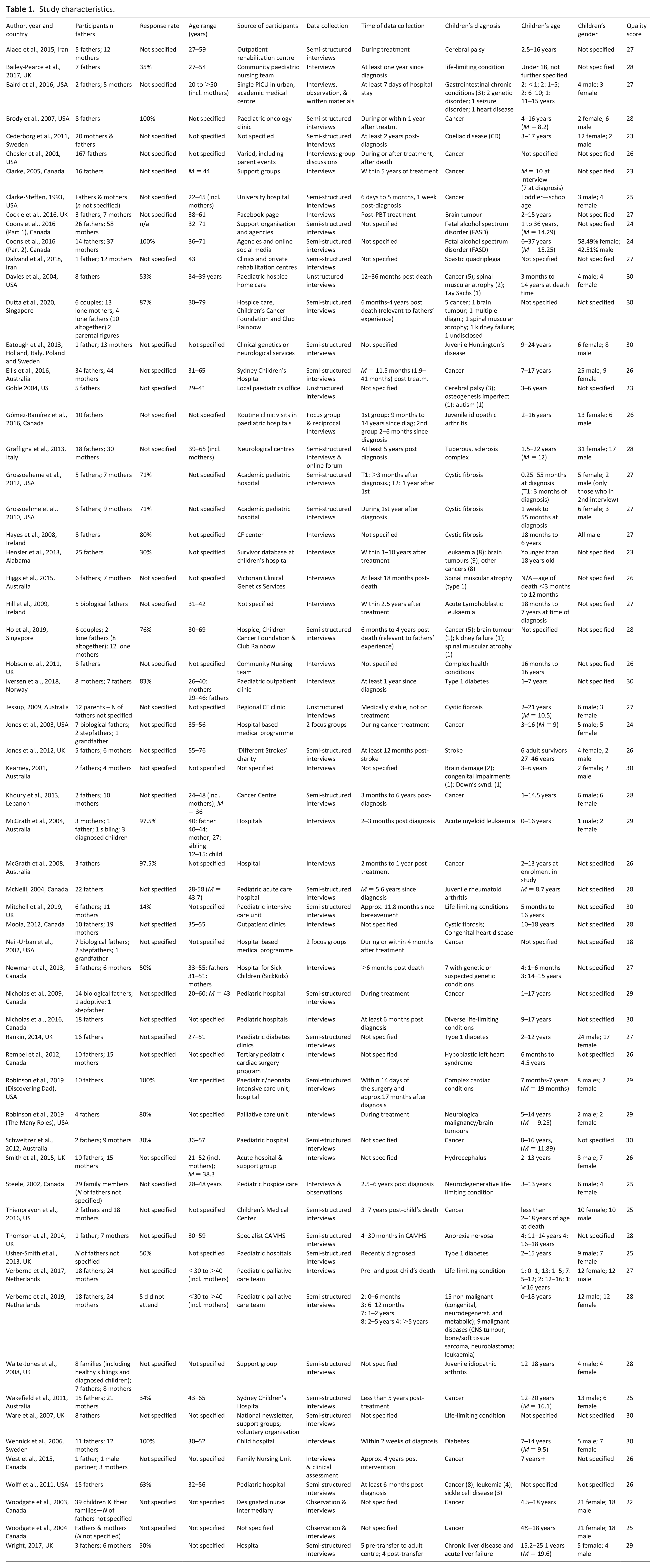
Search results were collated in an Excel database and duplicates deleted. The first and second authors independently screened titles and abstracts and reviewed the full-texts of retrieved articles. A priori inclusion/ exclusion criteria were applied at this stage. Any discrepancies were resolved by consensus. Data including study details (author, year of publication and country), participants’ characteristics (number, gender and age), response rate, source of participants, method and time of data collection and children’s characteristics (diagnosis, age, number and gender) were extracted (see Table 1). 54 Full replication of participants’ experiences expressed in original quotations in the papers (first-order data) and authors’ interpretations and conceptualisations (second-order data) were used across the full primary studies.45,46,54 Data was extracted in thematic tables. 51 If studies reported data on both parents, only findings relating to fathers’ experiences were extracted. In studies where data collection took place after the child’s death,4,55–61 only data relating to fathers’ experiences of illness and caregiving were extracted.
Study characteristics.
Appraisal
Quality appraisal was conducted using the Critical Appraisal Skills Programme (CASP) checklist. 62 Studies were not excluded on the basis of a given score, as a CASP cut-off point has not been recommended previously.63,64 (see Supplemental online file 2)
Data synthesis and conceptual model
We used Noblit and Hare’s seven-stage meta-ethnographic approach (see Supplemental File 4). 65 The first and second authors thematically analysed the full list of first and second-order constructs and organised them into categories through constant comparison63,66,67 to facilitate reciprocal translation. 52 The interpretative process and the development of the conceptual analysis were iterative and collaborative, and by reference to the original texts. 64 This helped identify whether constructs corresponded (reciprocal translation), contradicted (refutational translation) or expressed different aspects of the topic (line of argument). 68 Where authors used varied language to label the same phenomenon, we compared the constructs to identify patterns of shared meaning. 69
For example, if one study reported that fathers felt supported by health professionals1,28,55,59,70–77 and another where support did not meet their needs,5,21,78 these were considered refutational and translated into a new construct incorporating elements of both (e.g. ‘inconsistent healthcare support’). However, if a third study3,4 suggested fathers found it hard to receive support initially, but shifted to seeking and receiving support, all three interpretations were treated as reciprocal and translated into a construct encompassing all three. Sub-constructs were also developed; these helped reconfirm the construct names in the final list (see Supplemental online file 3) and explore the lines of argument.
Results
Review process
Nine hundred and thirty-one articles were identified for review (after removal of 9 duplicates); 778 were removed during title and abstract screening. The remaining 153 were reviewed in full, with further exclusions based on stated inclusion/exclusion criteria. 63 articles were included in the meta-ethnography (see Figure 1).
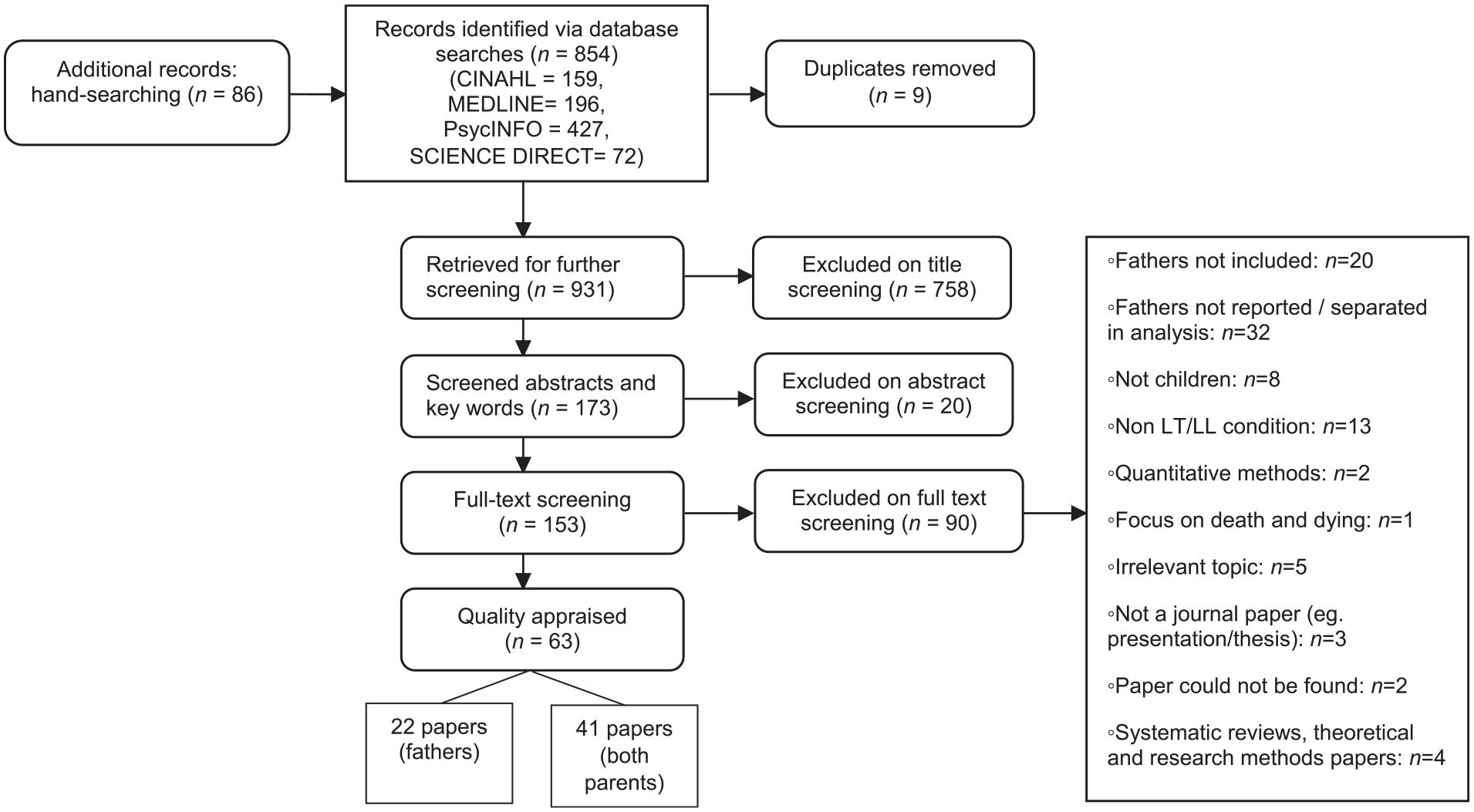
PRISMA flowchart.
Characteristics of included studies
The majority of the included studies were conducted in the USA (241 fathers, 15 studies), Canada (99 fathers, 14 studies), UK and Ireland (87 fathers, 14 studies) and Australia (63 fathers, 8 studies). The remaining were conducted in Europe (74 fathers, 7 studies) and Asia (14 fathers, 5 studies). 496 fathers were interviewed in total through a range of interviews and focus groups (not including 8 studies that did not specify number of fathers.60,78–84 The majority of included studies interviewed both parents (n = 41, 66%), with only 22 focusing solely on fathers’ experiences of caregiving.1,3–5,23,24,27,71,75,77,85–95 Children’s life-limiting conditions mainly included cancer,5,8,10,21,56,70,71,75–77,80,83,84,87–89,93,95–98 cerebral palsy,24,99 cystic fibrosis81,94,95,100–102 and type 1 diabetes.82,85,103 Some studies included varied life-limiting conditions,1,4,6,27,28,57,58,60,91,92,104 while others did not specify their type. 59
Synthesising translations: Line of argument
Studies all related to one another through contribution to a model (see Figure 2) encompassing five multifaceted overarching concepts: the paradox of support, challenges in the caring process, ‘nobody thinks of men’, impact on family life and the fall of the curtain: an irrevocably altered world. In the following sections, we discuss these concepts and associated sub-concepts, and provide recommendations for future research and practice.
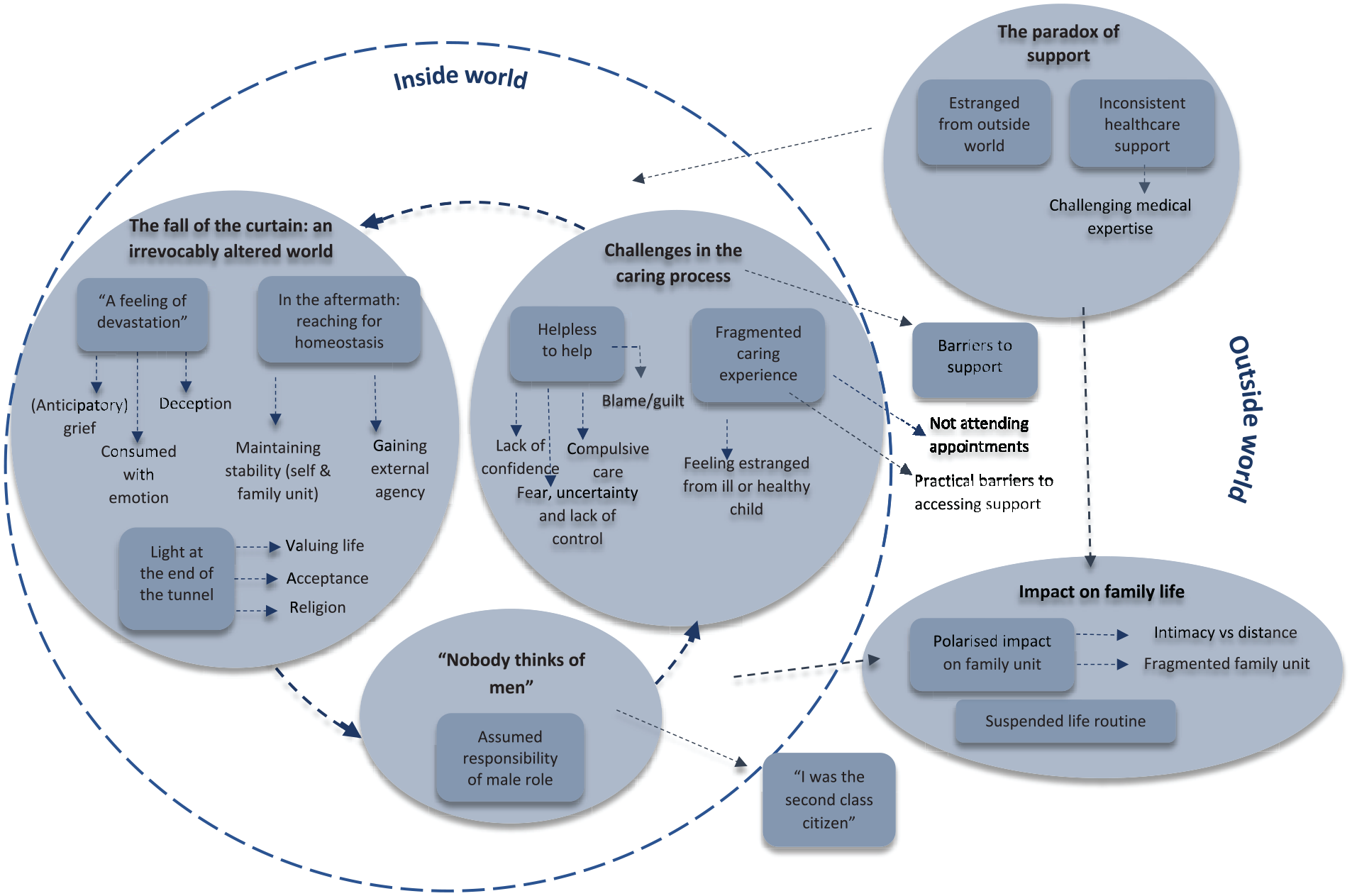
Conceptual model.
The paradox of support
Estranged from outside world
There was an acute feeling of estrangement from the outside world among fathers. They experienced loneliness and alienation from other families,9,21,91,102,105 and a sense of betrayal and lack of sympathy from their own families, friends and society, in general.3,6,9,21,27,28,74,87,91,106 At times, there seemed to be little concern for fathers; despite their struggle, they were perceived as managing well: People would constantly ask me how my son was doing, which was understandable, but then shift to, “How’s your wife taking all this?” I don’t ever recall anyone ever asking me, “How are you taking this”, I guess they just assumed I would be okay. I felt very alone.
21
Friends failing to offer help or not knowing how to be supportive exacerbated the feeling of loneliness. Some friends had difficulty managing their own reactions, or experienced resistance from fathers who were not open to help.
21
Many fathers were geographically or personally isolated in varying degrees from their extended families and needed to rely on internal resources (themselves or partners) or on services,
3
as their networks were perceived as distant, unsupportive and unsympathetic105,106:
we didn’t really have the family support because (…) I really do not think they have understood what we have gone through.
3
Having seen Carl turn blue and look like a skeleton you think, you know, I think my brother has no idea and I get cheesed off.
106
Their world became uncertain and alienated,
91
as their own family and/or friends failed to acknowledge or understand their anguish; this created distance and reduced opportunities for support over time. Some of the fathers intimated a continuing sense of betrayal by family or friends,
91
while others felt alone and misunderstood in society
9
: If you had not heard news about your child being given a death sentence, then you do not know how I feel (…) or cannot put yourself in my shoes.
102
it’s too much cause people don’t understand the stress.
27
Fathers felt inundated with negative messages, hopelessness and rejection, which culminated in feelings of anger, failure and despair.
6
Prejudice,
106
stressful and embarrassing moments were experienced in public when they received frowning looks from people if their child had an outburst,
74
or if they took measures to protect the child from health risks:
then people can often stare at as if you are crazy.
28
It feels like no one wants to touch us really.
9
Inconsistent healthcare support
Healthcare support was perceived as inconsistent, with some fathers having positive experiences and others feeling abandoned by or alienated from services. Positive experiences included fathers feeling that their needs were met by the healthcare team1,3,4,28,55,59,70–77 and their opinion in the care process was given credibility.
106
Staff members were perceived as knowledgeable
1
and empathic,72,77,93 which enabled positive and trusting relationships to build. In key decision moments, fathers put their faith in medical staff1,59; children were provided continuous and individualised care, and the trust relationship with doctors was vital, mainly when many other medical professionals were not willing to understand the child’s challenges.1,4,56,73,96,104,107 The help received from General Practitioners (GP) was also prompt and contact was regular. GPs and paediatricians were viewed as gatekeepers to accessing other services or support; although some medical professionals were not perceived as highly educated about the child’s illness, they proved efficient in managing medications, family issues
74
or supporting fathers to cope with the ordeal of treatment.
75
Moreover, some health professionals were skilled in bringing the family together to communicate sensitive information or assist when parents were losing their child:
They inspired trust. I think our shell-shock would have lasted longer and our environment at home would have suffered, but they took everyone into the loop – dragged the whole family in.
70
Fathers appreciated the honest manner in which they were informed of their child’s prognosis and felt their questions were answered. 77 They felt part of the ‘team’ to ensure the best care for their child. 4 At difficult times, doctors advocated for the child or parents, and offered their support on days when they should have been off work. 59 Formal support groups were valued highly, as they provided a sense of community and belonging.55,73
Despite the positive experiences described, some fathers felt that few professionals had the specialist knowledge to help them.9,91 Fathers themselves struggled to understand the incomprehensible medical language and felt confused in relation to their involvement in the care process. Navigation of support services was not always smooth, caused by perceived inadequacy of follow-up after diagnosis, poor communication between staff across services,
91
delayed diagnosis and disproportionate care.5,9,72,77,91,104 Some described the health care system experience as ‘living hell’, as fathers felt little control over the processes or outcomes of care
27
:
All of our decisions that we had to make were split second decisions
4
There was an acute frustration around support1,5,59,71,73,74,78,93,103: support groups were not always aimed at fathers or did not meet their needs.
3
Medical services lacked a family-oriented approach and staff missed the whole picture of families’ lives and dynamics. Care decisions reflected the illness-induced interactions and did not necessarily meet families’ needs,3–5,21,78 even when the child was cared for at home
85
:
we had to lose our temper in front of the general practitioner with the paediatric homecare organisation before they understood our boundaries
28
Fathers did not feel encouraged, nor received emotional support from health professionals; they felt inundated with hopeless prognoses,1,6,78,85,86,105 which echoed their abandonment by staff and services:
…after he had come out of the coma, we were hit with the fact that he was `going to be a vegetable’
6
Challenging medical expertise and practice
The central theme of mistrusting healthcare services and staff recurred in many studies.1,4,5,59,78,81,91 Fathers felt that health professionals dismissed the impact of their communication or decisions on families’ lives, and subsequently trust in their competence was challenged. This experience contributed to an emerging self-doubt about their own ability to make key decisions relating to the child’s care; there was an intimated ambivalence towards the healthcare system, knowing that it failed them in the past:
I feel like I made a totally wrong decision by letting those wackos (crazy people) near my son.
78
Fuck what the doctors tell you a lot of times (…) they don’t live with child, they don’t understand, you know, I’m told they’ve got the latest research papers… that’s not living at home with someone 24/7 and understanding the condition from the inside out.
1
Some fathers reported incidents when nurses did not comply with required standards of practice,4,108 for example not using antiseptic techniques appropriately; although the child had many infections as a potential consequence, the father was excluded and the care was jeopardised after making a complaint:
Instead of them coming in and checking on him seven or eight times, it would drop down to five or six times or four times.
4
The support system was perceived as too bureaucratic and inconsistent; appointments were held at inflexible times or involved long periods of unnecessary waiting.
91
Fathers questioned the quality of services, which were not always adequate to their needs, lacked clarity or were duplicated; they felt that a key-worker would have eased the process and improved continuity of care.
91
There were moments when fathers took an active role as ‘nurses and watchdogs’, given their discontent about how their child was cared for:
we had to be careful. What things were administered to him and a lot of them we did ourselves (…) and when we were at home I was giving him injections
5
Although initially hesitant due to their previous experiences, fathers had no other option than to place their trust in healthcare professionals, mainly when they faced the ‘danger’ of losing their child.
1
In more extreme cases, fathers considered legal dispute: if I knew what I know now, he wouldn’t be going anywhere, because my lawyer would just make mincemeat out of him. I’ll never forgive him. He didn’t know what he was talking about (…) he was just a fool.
81
Are they all on the same page? Well, they probably were on the same page…. But if they’re not, we’ve got a fight on our hands
59
On other occasions, fathers became advocates for their children and read medical literature; gaining knowledge about their child’s condition empowered them to challenge information and work closely with health professionals to ensure the best care:
We heard other families saying that we should try these other drugs and so we kind of leaned towards those because they seemed to work (…), even though the neurologist thought something else would work (…)
4
Challenges in the caring process
Fragmented caring experience
Fathers experienced estrangement in relation to their unwell child, often finding that mothers assumed the primary care role. They felt side-lined, mainly when their partners resisted their opinions or contributions. There was a feeling of alienation stemming from their secondary or peripheral participation in their children’s care, due to lack of support or opportunities to be engaged more intensely.21,84,87,98,106,108 There were instances when parents had conflicting expectations in relation to the caregiving, mainly shaped by assumed gender roles:
I had to fight to stay with the baby in the hospital—my wife wouldn’t let me.
21
Fathers often assumed care responsibilities for healthy siblings to ensure they received as much attention,5,24 whilst others felt torn between their healthy and ill child.
93
They were unable to attend appointments due to work commitments, distance and siblings’ needs.
98
In some cases, parents made the role transition together, by exchanging household responsibilities, with the father being the primary caregiver for the unwell child21,92,98:
My wife and I have reversed the traditional roles. I stay at home with the kids while she works.
21
Helpless to help
Caring was experienced within a cloud of feeling helpless in relation to their child’s condition. Fathers felt hopeless in their ability to care for their child as a parent ‘should’, leaving them feeling unconfident and lost.1,6,24,27,55,77,83,87,91,108 Feeling unable to fulfil their perceived role of the ‘fixer’ as a parent and take away their child’s pain was a huge challenge, and some fathers described it as ‘a unique kind of horror’
1
:
as a parent, you feel that you can do everything for your child, and not being able to fix something that your child is going through is very, very difficult.
24
I’m afraid to be left alone with my sick daughter because I fear something will happen to her and I could never forgive myself if it did.
24
There was an intolerable self-blaming and guilt stemming from their helplessness.21,92 They experienced fear, uncertainty and lack of control over the illness.1,4,5,9,23,28,59,72,77,79,81,82,85–87,89,93,94,109 Fathers found themselves in a state of crisis; their emotional pain and children’s physical suffering seemed invincible and paralleled one another: I guess that’s the hardest part, dealing with the pain and suffering, just tremendous suffering. It’s just serious, serious pain and that just tears the guts out of you.
23
Some fathers described compulsive caring to try to manage this lack of control,1,27,28,72,93,94 including excessive cleaning, 1 avoiding contact with others and ‘constantly watching’. 94
Practical barriers to accessing support
Fathers experienced practical barriers to support including difficulty gaining financial support9,60,99 and travel insurance, 72 and feeling unsupported at work. 88 There was limited flexibility to take time off work, which reduced opportunities to engage in caregiving or support wives. 21 They also found it difficult to find a suitable carer for their ill child24,106 and/or did not feel they had access to proper services72,88 or key workers.72,91
‘Nobody thinks of men’
Assumed responsibility of male role
Fathers’ experiences were shaped by assumptions about masculinity and fatherhood, embedded within the organisation of support systems and medical care institutions. 21 They took on an assumed responsibility to lead the family,4,88,89 which often meant putting aside or repressing painful emotions. Being the ‘strong’ one allowed them to fulfil the role of provider, and even protector, to look after mothers and their families.21,23,58,71,78,87,88,93,102, 106
Men still feel like there has to be some sort of stability in the family. That’s our job…I carried my grief to other places . . . or I experienced my grief when she wasn’t around so she couldn’t see it.
93
Fathers used strategies to gain legitimacy in their family and in society. They struggled between hiding their emotional response to prove they were strong, and showing others that they were suffering too. Fathers appeared to cope well, but over time, their internalised mask of bravery became difficult to handle:
Fathers have to be the tough guy, but I couldn’t take it. For 2 years, I just cried (…) I put my ‘stuf’, in a box and put the box on my shoulders. Then, I’m okay until my legs buckle.
21
Some fathers were reluctant or experienced guilt to seek support to enjoy time with their life partners.
24
Others avoided support networks to try and maintain a sense of normality.
105
However, the most recurrent theme was a belief that opening up about their emotional experience and seeking support was not acceptable1,3,5,23,27,87,88,93: You don’t show any vulnerability ever…You don’t let your guard down when it comes to that. You’re the rock that holds the place together so to speak.
3
‘I was the second class citizen’
A common felt experience was a lack of acknowledgment of fathers’ role in the care process, both at work3,21 and the hospital.5,77,78,90,108 A high number of fathers felt side-lined1,5,21,27,77,78,86,87,91,106 during interactions with health professionals, or when attempting to access services or information regarding their children. They felt that information was restricted,4,5,12,60,72,78,85,87,93 and subsequently fathers felt unvalued
1
or had an exacerbated sense of lack of containment and abandonment.
91
When they took part in communication with health professionals, they felt disconnected and that they received second-hand information; they did not feel that the medical professionals were alongside them as other human beings:
The help the staff offered, even their talk, was all geared toward the mom. None of the professionals there could relate to me.
21
I have to sit and wait.…I was the second class citizen. I want to know what’s going on…and they won’t say anything to me.
108
Fathers’ care occurred ‘behind the scenes’ most of the times, and their efforts were not recognised by medical staff. They did not feel listened to, valued, nor included in care plans. They felt undignified, and their basic needs and opinions were not accounted for: You’re nothing. They don’t give a s*** what you think or what you want. Anybody that’s an important part of the team, I can’t see an important person sleeping on the floor. But that’s where you sleep as a parent. You sleep on the floor. Does the doctor sleep on the floor? Does the patient? No. That kind of thing just pissed me off.’
78
Although in some circumstances the father was the child’s primary caregiver or the legal guardian, healthcare professionals prioritised the mother when information was provided:
Doctors and nurses and everything [should] realize that maybe you don’t have to come in and talk to the woman in the room, that maybe the man’s also involved in it a little bit more.
77
They had fewer opportunities to gain the same level of understanding about their child’s condition and treatment as mothers,
106
and were not involved in post-treatment decision making
98
:
I am sure if someone explained it we could really understand and get some knowledge. It’s not as though we’re stupid.
72
Fathers often appeared torn between wanting their emotional experience to be acknowledged,1,27,71,78,86,91,94 and an internalised view that they should not need or want their emotions tending to, because there was a consistently held view that women’s emotional experience takes priority.21,23,27,78,87,88,91,93,94,102
people don’t realize how much it does affect (…) I suppose the fathers probably are the ones that might be overlooked the most (…) I don’t know whether that is being sexist.
28
‘Did I feel left out? (….) There were times when I felt left out, … second wheel. It would be like they’d go to [the child’s mother], explain everything (…) and then, “oh, by the way, here [and then refer to the father]”, It seemed to me, at times, I was an afterthought.
27
Important practical insights surfaced from fathers’ narratives. They experienced taboo around intimate personal care for daughters3,106 as well as fears over the ability to continue to provide physical care as their child grew older. 24
I tend not to get involved in the personal care unless I absolutely have to and it’s not because I don’t want to get involved in changing nappies it’s just about what is and isn’t really appropriate.
3
There were also calls to improve services within medical institutions around pain and symptom management,
56
adults’ facilities for hygiene, healthy diet
75
and sleep.3,85 Finally, there were indications of trauma among some fathers’ narratives, calling for a need for holistic care that would address the emotional and physical needs of each family member.1,27 In general, fathers coped alone and mothers got support from others
21
:
if that gap in that window was big enough I’d force myself out of it right now cause I can’t cope (…) I lost my mind, went completely didn’t know what to do…I was gone.
1
Impact on family life
Suspended life routine
Children’s life-limiting conditions undeniably altered their fathers’ lives and family dynamics. Fathers had to take time off work,3,5,10,92 and found that many lifestyle choices were now influenced by the needs of their children.5,27,57,72,106 There was a sense of being unable to resume life,1,4,27,28,71,80,87,91,103,106 and limited flexibility in daily life compared to before.24,57,88,102,106,108,109
Polarised impact on family unit
Some fathers felt emotionally reunited with their partners,24,27,91 but many others reported a loss of intimacy.3,4,24,71,75,78,87,88,93,105,106,110 In some studies, this ambivalent impact on intimate relationships was well articulated.1,11 Family units were shaken, with some fathers describing fragmentation of relationships, including separation and divorces5,57,76,92,106 and others, family closeness.71,77,88,95,109
The fall of the curtain: An irrevocably altered world
‘A feeling of devastation’
Fathers experienced devastation on discovering their child’s life-limiting condition, enveloped by anticipatory grief relating to their inside and outside worlds. This stemmed from thoughts of losing their child4,55,59,88,109 and that their child would never be the same again.28,71,94,106,110 They also grieved for their own altered life3,9,55,84,93,102,105,108,110 and relationships. There was a sense of loss and sadness due to their limited involvement with the unwell child84,106 and the grief became atemporal and irreversible: It’s like you’re grieving for your own child because a certain amount of your child has actually died. You’re seeing it every day, you’re grieving for it every day.
110
For some, the period of diagnosis was turbulent and ambiguous, with indecipherable illnesses contributing to this.4,9,11,82,91,93,105 Others felt as though they had been knocked down to be brought back up.83,107 Not all fathers grew stronger: “This business about ‘coming out of it stronge’, is a bit of rubbish”
21
; the majority were consumed with emotions,5,21,27,71,78,83,88,90,94,102,106,107,109 including anger1,5,6,23 and shock1,4,23,55,59,70,72,86,87,91,93:
It was . . . so unexpected . . . I can’t really articulate the feeling aside from maybe just a numbness and a disbelief . . . that took over us’
55
It just went wooooooooosh… I remember …a weird 70’s puke green place with a window that only had about this much gap it was high up and she (Consultant) matter of factly said ‘yeh people with (diagnosis) only live till their about 28 uh yeh yo’,re guna need lots of help yeh its awful’ . . . I remember . . . thinking you fucking bitch
1
They wanted their emotional experience as a male to be acknowledged: “we have emotions, we break down, we cry”. 27
In the aftermath: Reaching for homeostasis
In response to their difficult emotional experience of having a child with a life-limiting condition, fathers tried to maintain stability of their inside and outside world. They often dismissed the impact of the diagnosis and associated emotions1,11,27,28,58,75,78,83,86,87,91,94,106 and withdrew from others.96,105,106 Fathers tried to maintain some normal family routine,4,5,103 which for some was achieved by negotiating independence with the unwell child.3,23,72,105–107,110 Finally, fathers reached for homeostasis through education and gaining experience in their child’s diagnosis.4,5,28,72,73,75,77,78,84,87,91
Light at the end of the tunnel
Fathers found solace by living in the present moment with their children.6,73,77,89,94,97,105 Through the hardship they learnt what was valuable for them.8,23,27,60,71,77,90–93,95 Some focused on hope and defiance to move forward in life,6,23,27,28,77,88,102 whereas others talked about the importance of acceptance.1,8,27,28,57,59,73,91,94,105,106 Religion was also a way to cope and manage the difficulty of the experience.4,23,27,28,77,88,91,95,100,101,111
Discussion
Practical implications
Included studies informed a model encompassing five multifaceted overarching concepts that explained fathers’ experiences of caregiving. These described their lived paradox of support, challenges in the caring process and impact on family life. In addition, fathers felt that nobody thought of them while looking after the ill child, and that their world was irrevocably altered. Our line of argument indicated that fathers had complex and varied experiences of caregiving inside and outside of family. They valued specialist knowledge and open communication across services, however, our findings suggest that they experienced ambivalence in relation to their role in their child’s caregiving. There was both disempowerment in the interaction with health professionals and reassurance that the staff sat alongside the ill child and the father.
Several recommendations to improve fathers’ experiences can be drawn from this meta-ethnography: (1) recognising the father’s experience should be an integral part of healthcare, and not an adjunct; (2) allowing an empathetic interpretation of fathers’ experiences so that tailored services support them to communicate rather than hide their emotions; (3) understanding the types of caregiving fathers offer their children and enabling more opportunities for them to be involved in their ill children’s care; (4) recognising the gender roles, social and economic determinants of father’s stress and isolation, and how these play out in the medical arena; (5) providing an opportunity for new interactions with surrounding social structures and institutions; (6) allowing them to be part of the advanced/anticipatory care planning.2,37
There is a need to recognise that increasing numbers of fathers are involved in general childcare, as well as in their ill children’s treatment, often provided in their homes. This may be due to changes in how the role of fathers is viewed in society and the increasingly family-friendly working policies that have been implemented in recent years. 112 However, there needs to be more information, guidance and support for fathers who provide intimate personal and complex nursing care for their ill children at an age when it is deemed to no longer be appropriate for them to do so, especially in public or commercial toilet facilities. 3 This is highly sensitive for fathers who look after their daughters with complex healthcare needs, as their role can be misconstrued as child abuse. 3 Child safeguarding and dignity of care policies should recognise fathers’ role in the palliative care process. This aspect of healthcare is critical to protect those fathers involved in general childcare while the mother looks after the ill child in hospital, or are the child’s primary caregiver/legal guardian.3,106 Our model indicates that fathers feared over the ability to continue to provide physical care as their child grew older. 24
There was evidence of practical discomfort when fathers tried to access a shower in the hospital as they had no other option than using the children’s facilities. 75 It was also suggested that there should be opportunities for the ill child and the parent on the ward to get a meal together in recognition of the moral support they provide and contribution to the care process. 75
Medical staff could assist fathers in the illness journey by providing the necessary information and support and by allowing them to be an integrated part of the healthcare system. However, as our model indicates, health professionals will need training and support to be able to assist them effectively.3–5,21,78 Furthermore, international policies need to emphasise the importance of family-centred paediatric palliative care 31 and prioritise collaboration between both parents and healthcare providers.2,37 On a societal level, gender is embedded in fathers’ experiences of their children’s life-limiting conditions and perception of traditional gender roles needs to change; despite fathers’ willingness to be involved in their ill children’s care, they still experience restrictions in accessing medical information. Indeed, some fathers prefer to leave the information gathering to the mothers. 75 However, rather than relying on the mother to update the father on the child’s progress,1,4,5,12,21,27,60,72,77,78,85,86,87,91,93,106 health systems should create channels of communication through which medical staff can engage with both parents. These would enable them to learn of their decisions regarding the care role, and their preferences if/how they would like to be involved. Although some health systems facilitate parents’ online access to children’s tests before appointments, 121 our recommendation is that international policies should prioritise such services to become a common practice. 21
More flexible appointments to enable equal access to information, opportunities for fathers to contribute to initial screening, consultations or treatments, and consent giving in relation to treatment and care plans, mainly when they are separated from the mothers, is another area that needs addressing. 91 Recent evidence signals new patterns of family formation alongside the more traditional one, rise in births outside marriage (with co-habiting couples or lone parents) and increased divorce rates, all with potential impact on clinical practice 119 ; therefore, fathers should be offered opportunities to provide their support in the care process.
Our model opens possibilities for support networks in the healthcare system. In recognition of the fact that fathers’ experiences are still shaped by embedded assumptions about masculinity and fatherhood within medical care institutions, 21 time should be reserved to determine what sorts of support they prefer, and tailor them according to their needs in the caregiving journey. Many studies have highlighted the difficult balance between acknowledging fathers’ emotional needs and experiences and their need to dismiss these at times to maintain their own sense of normality. There was a pattern towards mothers seeking and receiving more social support than fathers.21,23,58,71,78,87,88,93,102,106 On different occasions, fathers perceived a lack of adequate outlets to communicate their emotions or declined the support provided as they learnt effective and protective ways of brushing off suggestions for help.1,3,5,23,27,87,88,93 Gender-appropriate interventions may be useful in periods of crisis (diagnosis, relapse) and chronicity (active treatment, remission). Psycho-educational interventions could facilitate parental understandings of potential similarities and differences in coping and adjustment. Finally, although developed from studies of fathers of children with life-limiting conditions, our model may also be transferable to other long-term (non) life-limiting conditions. Further research would enable comparisons.
Strengths and limitations of the literature
Fifty-seven studies were of high quality (score ⩾ 80%). The remaining, while judged lacking in some quality (score 60%–79%), were still considered to constitute valuable research contributing to the existing knowledge. 65 Only one study scored exactly 60%. 71 Authors needed to provide clearer details regarding its aims, recruitment strategy and rigour of data analysis. Several literature limitations were noted. Studies typically focused on relatively small samples of fathers; even in mixed samples, there was a bias toward mothers’ opinions. Gender imbalance in paediatric research has been addressed previously, and reasons include mother-focused recruitment, data collection and reporting,85,113 fathers not being invited or available, relying on mothers as proxy respondents for fathers, inaccessibility of working fathers, lack of knowledge regarding father’s caregiving role and contact details, lack of or minimal relationship between fathers and health professionals7,114–116 and lack of trust in researchers. 117 Although the exclusion of fathers in paediatric studies has raised ethical concerns and has been described as inappropriate from a funding perspective,14,118 their under-representation has been rarely addressed as a study limitation.7,115 In some studies, fathers’ data has been minimally reported or excluded.85,99,113 In addition, there has been little-no focus on young parents (aged between 13–25 years). A wealth of research has examined the experiences of middle aged parents; five studies included parents aged over 20 years10,72,80,88,104 and six gave an account of parents over 65,9,58,60,73,74,110 however their gender and number in that specific age range has not been specified. In 27 studies (44%) parents’ age was not specified at all. In addition, the age of the children in some studies (e.g. fetal alcohol spectrum disorder: 1–37 years73,74; stroke: 27–46 years 110 ; Juvenile Huntington’s disease: 9–24 years 9 ) and time of data collection (up to 4–5 years post-treatment/intervention76,97,98; at least 5 years post diagnosis10,23,86,105 or up to 7 years after child’s death4,56,58,60) may have created a potential recall bias or an inaccurate or incomplete recollection of fathers’ experiences when their children were younger.
Strengths and limitations of the meta-ethnography
To our knowledge, this is the first meta-ethnography focusing on fathers’ experiences of caring for their children with life-limiting conditions and the first attempt to develop a conceptual model. Although fathers’ characteristics and settings varied greatly, this meta-ethnography conceptualised their experiences during their personal and family crises, generated by their children’s life-limiting conditions. It provides a dramatic window into the salience of these experiences in various stages of children’s illness and treatment. An important limitation however is the reliance on the data presented in the included studies, which may not fully reflect the original data. This may be exacerbated by the trend in the literature to focus on the mothers’ experience.
The need for future research
As identified by others, 120 more research should focus on the changing nature of the traditional parental roles in caring for ill children. Our meta-ethnography highlights that fathers and mothers experience significant emotional distress equally; however, more research is needed to explore the gender differences in parental responses to their child’s illness, protective mechanisms fathers use and their preferred types of support. This call is supported by recent research that has addressed resistance strategies used by fathers of children with cancer 88 and fathers’ engagement in paediatric palliative care research. 7 Our study suggests that services are more conducive to the recognition of maternal emotional experiences and needs; one potential area of research would be the development of tools to assess fathers’ mental health in clinical practice, which could lead to the design of gender-specific psychological interventions. An example would be well-being questionnaires, designed to capture psychosocial risk factors that would highlight to the clinician that the family may need additional support. For instance, if a father had a history of psychiatric disorder(s), anxiety, depression, substance misuse or another child with a chronic condition then it would highlight that the family were at higher risk and may require additional support. This could then prompt referral to appropriate services to help address those issues. These types of interventions already exist, for example, in paediatric diabetes clinics, 122 where information gathered through an annual questionnaire is used to guide whether additional support is required. However, using these support tools to assess and support parents is not commonplace, and this is therefore our recommendation
There is a lack of longitudinal studies to address fathers’ experiences at key time points in the dynamic illness trajectory and their adjustment to treatment and caregiving. It was not within the scope of this study to explore how factors such as age, duration of care and time of diagnosis affected the findings in our conceptual model, however this is recommended for future research. In addition, as already highlighted, there was a bias towards lower father participation in research, and more focus on mother’s experiences when data was reported. Future research should avoid this bias, 120 by facilitating more inclusive and flexible recruitment strategies, and involving fathers in research designs. There is a lack of multicultural research in the area of fathers’ role in palliative care, and the impact of cultural beliefs and taboos on the treatment and caregiving process. Some fathers in our meta-ethnography were the primary caregiver, the legal guardian or a single parent.3,106 More understanding of the experiences of families with complex structures119,120 and their palliative care needs is needed.
Supplemental Material
sj-pdf-1-pmj-10.1177_0269216320979153 – Supplemental material for A meta-ethnographic study of fathers’ experiences of caring for a child with a life-limiting illness
Supplemental material, sj-pdf-1-pmj-10.1177_0269216320979153 for A meta-ethnographic study of fathers’ experiences of caring for a child with a life-limiting illness by Gianina-Ioana Postavaru, Helen Swaby and Rabbi Swaby in Palliative Medicine
Footnotes
Acknowledgements
This work is in memory of the first author’s father, who had a significant impact on the design of this project, and sadly passed away during the write up stage of the paper.
Authorship
GP designed the study; GP and HS conducted data screening and extraction. All authors were involved in data analysis, paper write up and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.