
Abstract
Background:
While several studies have examined ‘what’ families want with regard to the place of a child’s end-of-life care and death, few have explored ‘how’ parents reach a decision.
Aims:
(1) to develop a model explaining how parents of a child with a life-threatening illness in Greece decide about the place of end-of-life care and death; (2) to identify the factors affecting decision-making; (3) to consider the implications for clinical practice.
Design:
Grounded theory study of bereaved parents using semi-structured open-ended interviews following Strauss and Corbin’s principles of data collection and analysis.
Setting/participants:
Semi-structured interviews with 36 bereaved parents of 22 children who died at home (n = 9) or in a paediatric hospital (n = 13) in Athens, Greece.
Results:
(1) Decisions regarding place of care and death were reached in one of four ways: consensus, accommodation, imposition of professional decisions on parents or imposition of parents’ decisions without including professionals. (2) Six factors were identified as affecting decisions: awareness of dying, perceived parental caregiving competence, perceived professional competence, parents’ view of symptom management, timing of decision-making, and being a ‘good parent’. (3) Decisions were clear-cut or shifting. Few parents did not engage in decisions.
Conclusion:
Parents’ decisions about place of end-of-life care and death are affected by personal, interpersonal, timing and disease-related factors. Parents are best supported in decision-making when information is presented clearly and honestly with recognition of what acting as ‘good parents’ means to them, and opportunities to enhance their caregiving competence to care for their child at home, if they choose so.
What is already known about the topic?
Despite the fact that home is often advocated as the preferred place of death and as a ‘marker’ of a ‘good death’ for children, this is not supported by robust evidence.
Research on location of end-of-life care and death has been more outcome-focused, documenting parents’ and clinicians’ preferences or epidemiological trends with regard to the achieved place of death.
Studies focus on ‘what’ decisions parents make at the end of the child’s life, rather than ‘how’ these decisions are reached.
What this paper add?
Identification of six salient factors affecting decision-making about place of care and place of death: awareness of dying, perceived professionals competence, parents’ perceived competence to deliver care at home, parents’ view of symptom management, timing of decision-making, and being a ‘good parent’.
Identification of four distinct processes through which decisions are made: mutual consensus, accommodation, acceding to professional decisions and imposing decisions by excluding professionals.
Articulation of an explanatory model of parents’ decision-making for the place of care at the end-of-life and death, derived from empirical findings, situated in current context of care in Greece that has relevance beyond Greece.
What are the implications for practice, theory and policy?
Parents should be helped to make decisions about place of end-of-life care and place of death in such a way that they are not only truly informed by caring professionals but also presented timely with options so as to develop competence to deliver care at home, should they choose to do so.
Perceptions of what ‘good parenting’ entails, should be explored in deliberations with parents as decisions are reached.
Policy makers should improve end-of-life care at all sites since home and hospital are desirable to different families, for different reasons, at different times.
Background
Ida Martinson, in her pioneering work ‘Home Care Project for the Dying Child’, was the first to explore the feasibility, desirability, and effectiveness of home care as an alternative to hospitalisation.1,2 Since then, several studies have been undertaken to document family and clinicians’ preferences,3–6 epidemiological trends with regard to the achieved place of death,7–14 variables, such as socioeconomic status or type of disease, associated with different outcomes,15,16 and bereaved family’s adjustment following home or hospital end-of-life care.17–20
A review of the literature suggests that while home is often perceived as the preferred place of death, this view is not supported by robust evidence. 6 According to Dussel et al. 21 ‘the actual place of death may be less important than argued’, whereas ‘the opportunity to plan the location of death may be a better proxy for high-quality end-of-life care, one that is more inclusive and better aligned with palliative care principles’ (pp. 34, 40). Moreover, a ‘good death’ is not achieved in a linear or univocal way. Attention needs to be given not just to what parents want, but also to ‘how’ parents reach a decision when given a choice about the place of the child’s dying and death.
To date, only two studies, one conducted in England 22 and one in France, 23 have addressed the issue, both with families of children with cancer. Their findings suggest that decision-making is culturally and country specific and as such decision-making about place of care at the end-of-life should be studied in several contexts before drawing conclusions across contexts. The aim of this study was (1) to develop a theoretical framework grounded in empirical data to explain how parents in Greece decide on the location of their child’s end-of-life care and death, and (2) to explore how choices and service delivery affect bereavement. This article addresses the first aim.
Method
Study design
The larger study had a quantitative component comprising a structured questionnaire to explore parents’ perceptions of service effectiveness at the end-of-life and impact upon bereavement, and a qualitative component, following the principles of grounded theory articulated by Strauss and Corbin. 24 Two research questions guided the qualitative study: (1) how do parents decide where the child will be cared for at the end-of-life and die, and (2) what factors impact their decision?
In adopting a grounded theory methodology, we recognise that our study is underpinned by a post-positivist philosophical approach to the study of decision-making; acknowledging the researcher’s subjectivity, while striving to ensure maximum objectivity through a systematic approach to data analysis and the use of triangulation.
Population and setting
Bereaved parents were invited to participate. Their children had received end-of-life care services from ‘Merimna’, 25 the only Paediatric Palliative Home Care Service in Greece, or hospital services in specialised units located in a 400-bed public paediatric hospital of Athens. Paediatric hospice care is not available in Greece.
Sampling and eligibility criteria
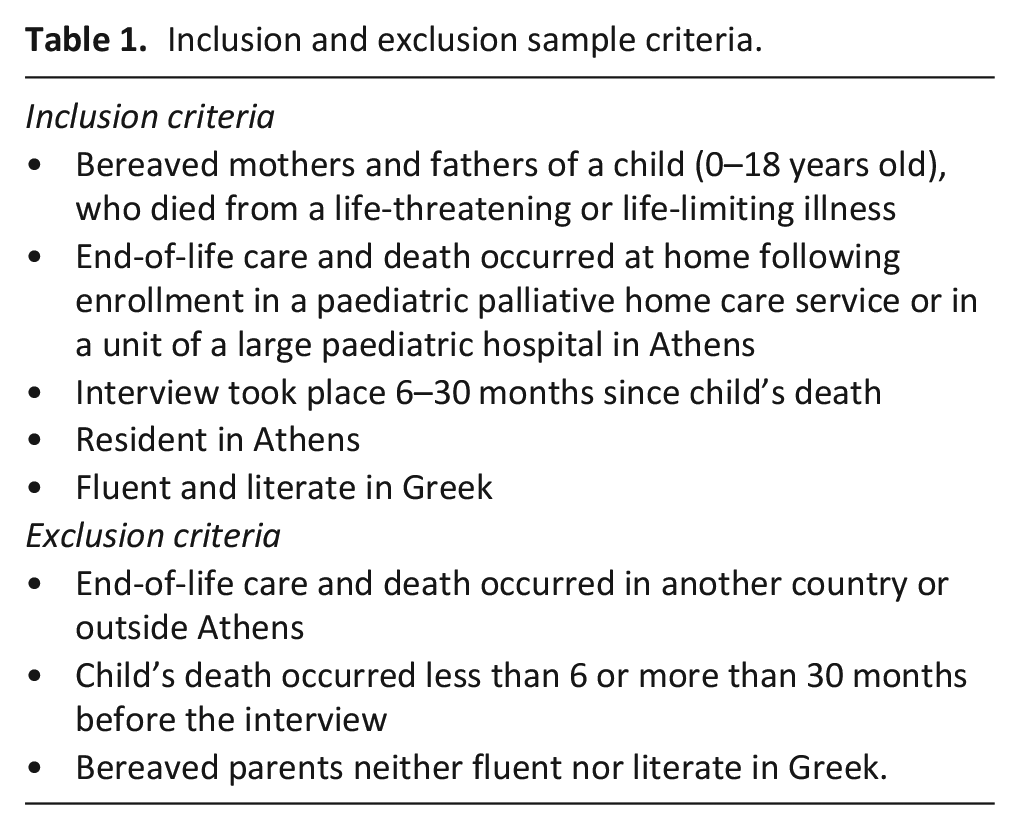
Families who participated in the study met the eligibility criteria outlined in Table 1. Theoretical sampling was adopted to ensure maximum variation in terms of disease, age, site of death (home, hospital specialised unit vs intensive care unit).
Inclusion and exclusion sample criteria.
Data collection
Data were collected over 2 years (2015–2016). Bereaved parents were contacted and informed about the study by the hospital’s or Merimna’s staff. Those who consented were invited to an interview with their spouse at a time and place that was most convenient to them. They signed a consent form and were informed that confidentiality would be preserved with data being anonymised.
The semi-structured interview was conducted in Greek with one or both parents. Interviews, which lasted from 45 to 180 minutes, were conducted by two psychologists and one social worker with post-graduate training in research and palliative care experience. Translation was not needed for Albanian parents, who read and spoke Greek fluently, having lived in Greece for over 10 years.
As per principles of grounded theory, data collection and analysis occurred concurrently and when new information emerged additional questions were added to the interview guide and new categories were refined in the analysis (e.g. shifting decisions, last minute change of place, communication patterns such as exaggerated prognostication).
Data analysis
Transcripts were analysed with attention to parents’ points of view on their decision-making. Data were initially broken down into small segments (codes) which were reassembled into categories and subcategories along the lines of their properties and dimensions (axial coding). Codes were raised to a higher level of abstraction (selective coding) through further refinement of categories, subcategories and their interrelations.
Regular meetings were held among three coders (V.K., E.K., P.L.) and the principal investigator (D.P.), throughout the analysis process, to minimise biases. When alternative codes and categories were proposed, consensus was reached through repeated data examination and the collection of additional accounts. This also enriched the theory that was progressively emerging. Data collection ended when data saturation was achieved and an empirically based model could be put forward.
Ethical issues
Ethical approval was obtained from the Scientific Committee of the Children’s Hospital P & A Kyriakou, and from the Ethics Committee of the Faculty of Nursing of the National and Kapodistrian University of Athens.
Results
Participants’ characteristics
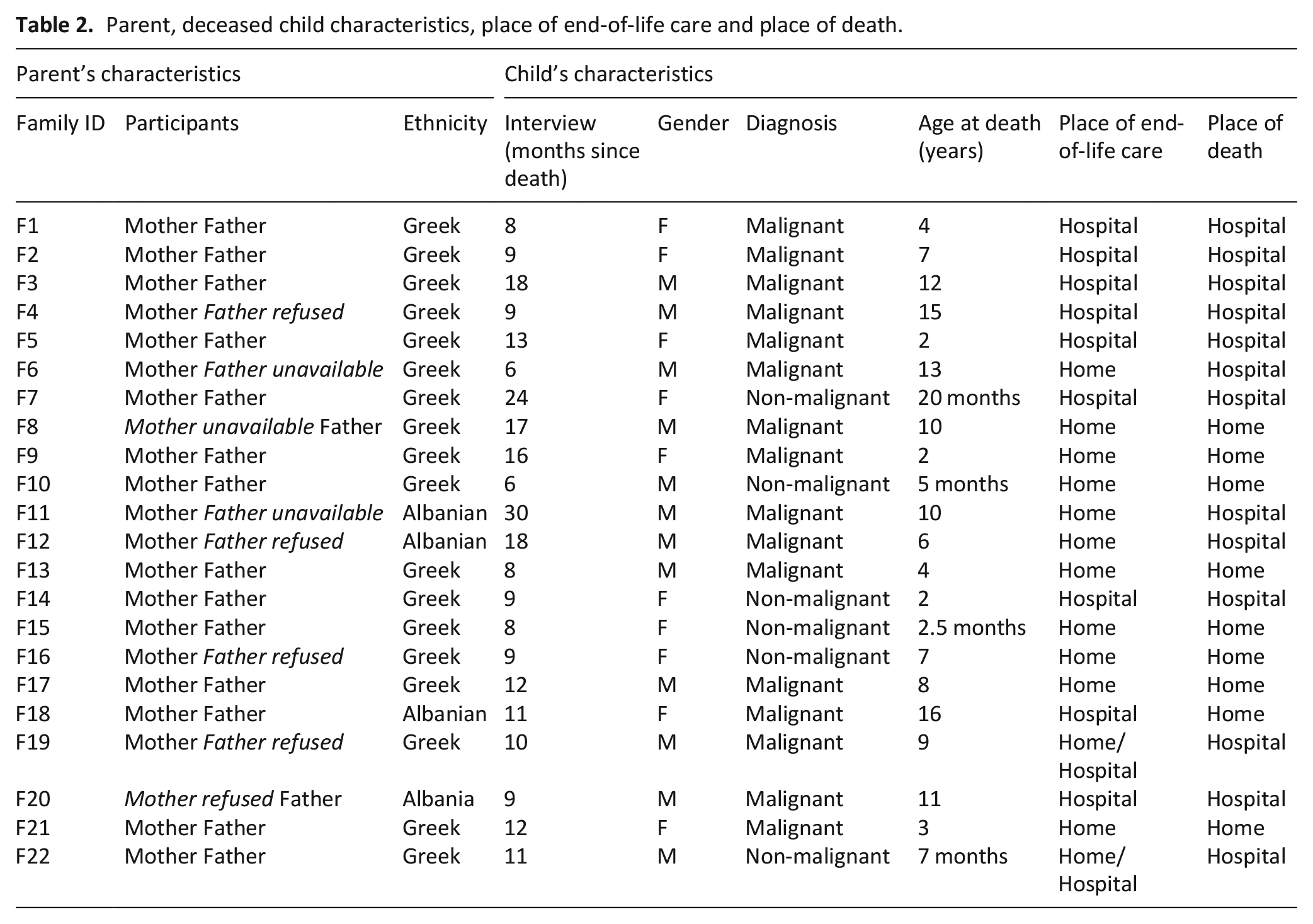
Twenty-seven families were invited to participate in the study; 22 consented (81% response rate) with 36 parents of 11 boys and 11 girls, attending the interview (Table 2). About 6 fathers and 2 mothers declined participation. About 28 were of Greek origin; 6 of Albanian origin. Children’s age at death ranged from 5 months to 18 years.
Parent, deceased child characteristics, place of end-of-life care and place of death.
Analysis of parents’ accounts reaveled three core categories: (1) the decision-making process about the place of end-of-life care and death, (2) factors affecting parents’ decisions, and (3) types of decisions reached.
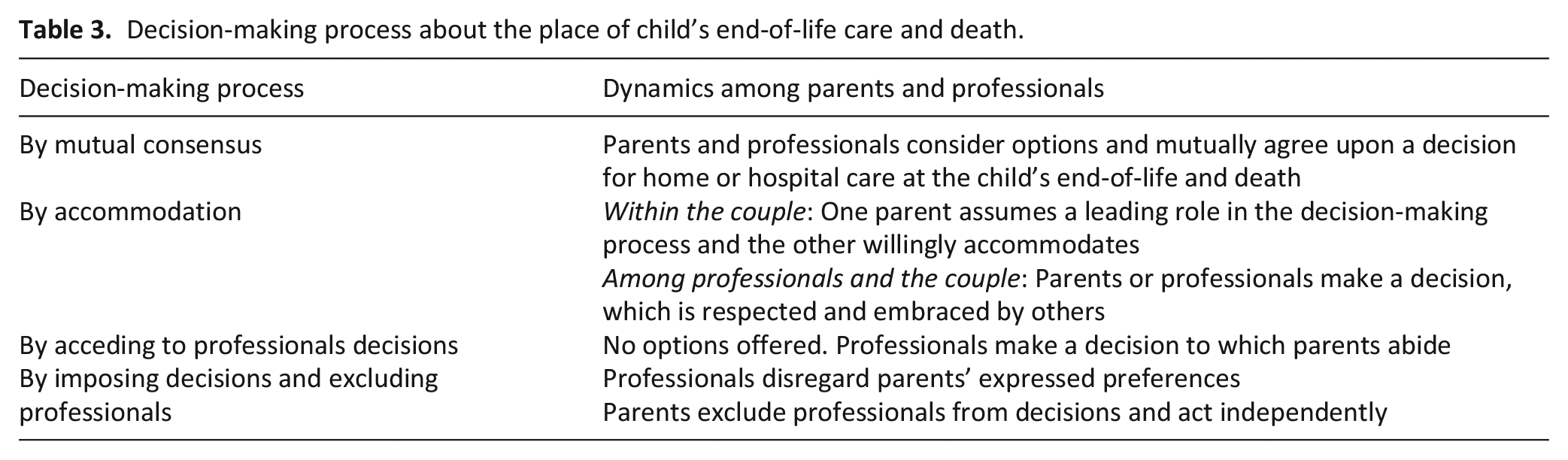
According to participants’ reports, discussions about the place of the child’s care and death were held among parents and clinicians, including an adult sibling. While children were not included in these discussions parents took their preferences into consideration. Decisions about the place of care were reached in four distinct ways (Table 3).
Decision-making process about the place of child’s end-of-life care and death.
After discussing with Dr. X the option of home care, I told her: ‘I am interested but I want first to meet the home care physician. Then, Dr. Z (paediatric palliative care specialist) came home. Along with my wife, we had a thorough discussion about the option of home care. When the physician left, I asked her: ‘What do you want?’ She replied: ‘I prefer home care’, and I said ‘Me too’. We came to a unanimous decision and that’s how it happened. (F13)
He (husband) is a reserved person, holds everything inside. In few words, he let me make all the decisions. (Μ12)
In other cases, professionals assumed a leading role and parents accommodated to the proposed option, which was in line with their preference. When parents refused the staff’s option, they offered an alternative proposal which was embraced by professionals who accommodated to their desires.
They (German professionals who were asked for a second opinion) proposed a medication which was at an experimental stage. We refused and told them: ‘Our desire is to go back to Greece and let her rest and sleep at home’. Deeply touched, these professionals realised we were determined; they showed respect, gave us a hug, and asked: ‘Where do you find such strength?’ (Μ9)
1.3.
Did the clinicians propose Merimna’s pediatric palliative care service?
No they didn’t suggest it. They [oncologists] told us: ‘Our job is finished. From now on, the home care team will help you until the end of her life’. That was all. Nothing else.
Did you have difficulty deciding about palliative home care?
No, we had no difficulty, because they did not give us a choice. (F21)
Some parents welcomed the clinician making the decision, expressing relief from the burden of responsibility of making a choice.
1.4.
We went back to Dr X and she told us about a new treatment (requiring hospitalisation), and I asked if it was experimental, and she replied: ‘No’. I asked about the success percentage and she replied they had no indications, so I assumed it was a clinical trial. ‘We will think about it, and we will let you know’, I told her. This lady thought she was dealing with idiots and said to us: ‘You know, I have the power and capacity to impose my decision, if I believe that this (treatment) is what your son should get’. It was the last time we saw her. We opted for home care. (M17)
We identified six factors affecting parents’ decisions: (1) awareness of child’s dying, (2) perceived professional competence, (3) parents’ perceived competence to deliver care at home, (4) parents’ view of symptom management, (5) timing of decision-making, and (6) being a ‘good parent’ (Figure 1).
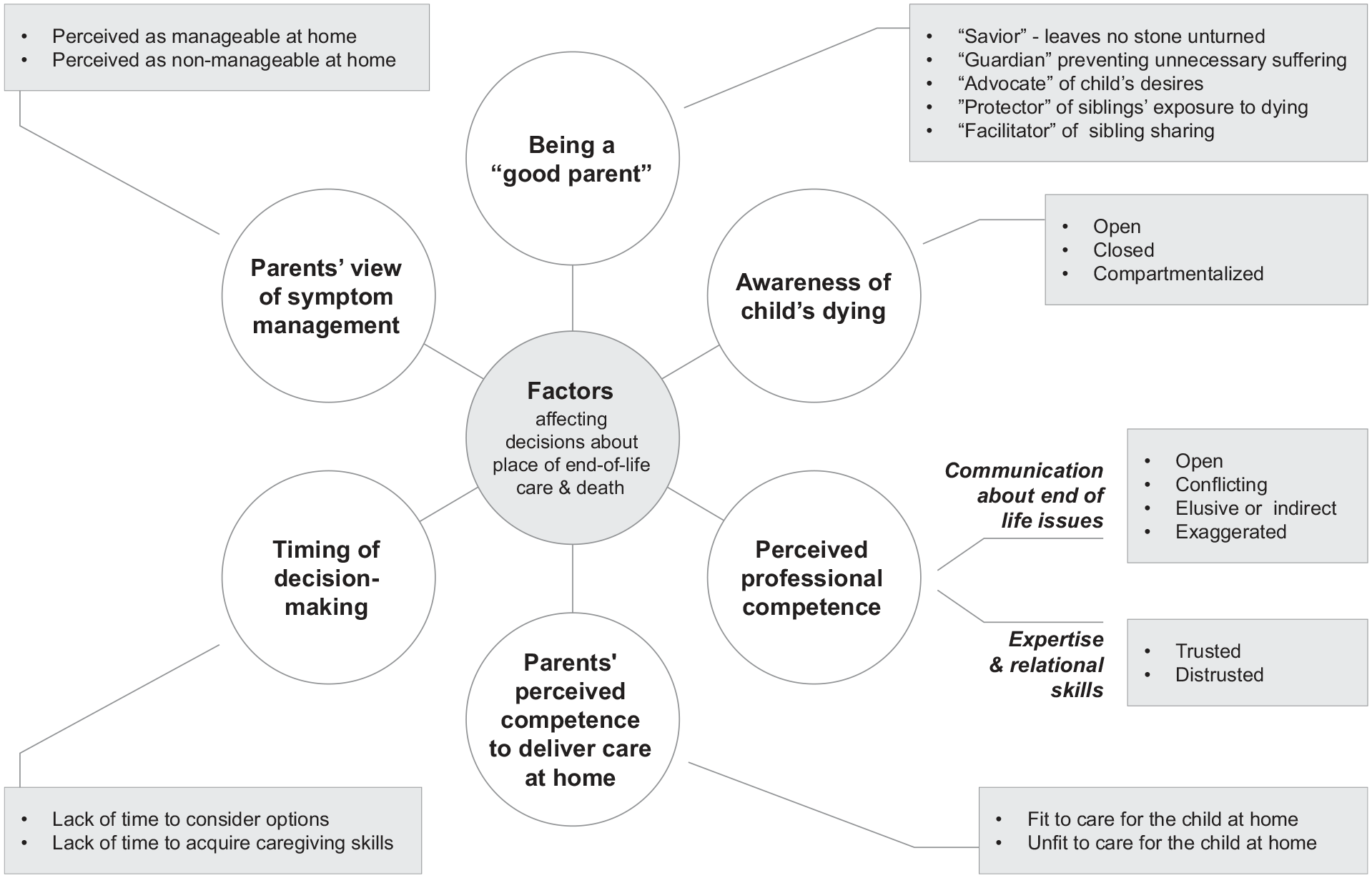
Categories and sub-categories associated to the factors affecting parents’ decisions.
I nursed, breast fed him, and told myself: ‘At some point this kid will leave this life’. I tried to make him laugh, sung, danced for him and he laughed. . . . When I was alone, I would let go and cry. It was difficult to come to terms that in one year, six or nine months, he will die. You tend to push the thought at the corner of your mind and tell yourself: ‘Now, I will make him laugh, now I will tickle him, now I will sing to him, now I will tell him stories’. (M10)
Open awareness was often facilitated by the children themselves, enabling parents to exchange direct or symbolic farewells.
‘He used three motorbike toys and told me: ‘The black is mine because I drive far ahead of you, and I am gone’. I replied: ‘I will reach you, and pass ahead of you’. ‘You can’t because I will be gone. You will stay behind me, to look after my young brother’. . . . I couldn’t hold my tears, and asked him: ‘What do you mean?’ He said: ‘I won’t say it again: I will leave’. (F13)
Even though she was in a terrible condition, I said to myself: ‘We will fight this and move on’. I didn’t want to consider the tought that this child would die in the future. I didn’t think about it. I believed in a miracle, yet in the back of my mind, the thought (of her death) was there. (M21)
While for some parents compartmentalisation led to choosing home care, for others it led to choosing hospitalisation in pursuit of a cure.
Hope never fades away. Until the very last minute, we believed that he wouldn’t die. I had read many things. . . . I was fully aware that scientifically he would not survive, but along with his mother, we couldn’t accept it; we hold on hope until the last moment. (F20)
They (palliative care staff) tried to prepare us. We didn’t accept it. . . . My husband didn’t want to be told such things. . . . and I simply thought they would be disconfirmed. I realised he was dying at the very moment of death. Until then, I believed in a miracle. (M19)
Even when children were aware of their terminal condition and tried to say goodbye, parents were unable to return the farewell.
She told me: ‘You are my favourite person in the world’. It was the last thing she said and never spoke again. I didn’t understand that she was going to leave’. (M18)
Parents’ decisions about place of care at the end of life varied by their awareness of the child’s terminal condition. For parents with compartmentalised or closed awareness their preference shifted from home to hospital, and vice-versa.
2.2.1.
They explained very clearly the negative and positive aspects of care. This was very helpful because they were straightforward. In other words, they did not leave us with ‘yes, but’, ‘may be’, ‘it could turn out this or that way’. (F7)
The key doctors didn’t tell us, ‘go home’, but the intern said to me, ‘there is no point staying here’. (M16)
He (child) was asking to go home and Dr Y suggested: ‘Don’t bring him to the hospital. I will send a physician to your home, who is a friend of mine, to help you. It is better to avoid tiring him with hospital visits and exams every 10 days’. I never imagined that the child would become bedridden at home and never get up again. (M11)
The physicians’ attitude was to include ‘difficulties’ in all their prognostications. . . Their prognoses and diagnoses were nightmarish. I didn’t believe them. I thought they would fight the disease and everything would turn out fine. (F3)
Just as awareness was associated with more or less stability in parents’ decisions regarding place of care, so too was clinicians’ communication. Conflicting or elusive communication was associated with vacillating decisions whereas open communication was associated with stability in decisions.
2.2.2.
At the hospital they all took special care of us and loved him very much. I received a lot of love from everybody. (M22)
They (palliative home care team) were interested in her as a ‘person’ and did not perceive her as a clinical case. The nurse and paediatrican became indinspensible to her. I was in peace because I had next to me, my own trusted people. (M21)
Parents who maintained trusted relationships with hospital personnel, were more likely to opt for hospital care whereas those who questioned the professionals’ competence, decided for home care and death.
We (spouses) agreed that our child wouldn’t die in a hospital setting where some nurses treated her adequately, whereas others put tape on her pacifier to prevent her from crying. . . . . . When I saw this, at a time she was actually dying, I decided to take her home, and hold her in my arms before she goes. (F15)
We didn’t know. . . We couldn’t manage anything on our own. (M7)
By contrast, those who felt competent in assuming care and were supported by a palliative care team they trusted, opted for home care.
You just become more ‘hardened’ than a parent with a healthy child; you see the blood and you know you must stop it. And you do it. You gain experience inevitably. . . . At home, you are not limited to a parental role, but you also assume a nursing role. (F13)
We wouldn’t be able to offer at home what professionals could offer at the hospital. I have no doubt about it. She underwent two mini surgeries at the end of her life, because she couldn’t urinate . . . . I couldn’t listen to her being in pain. She received a lot of morphine to prevent the suffering. (M2)
Things developed very fast and we didn’t know how to assume the care at home. (F7)
I didn’t expect this turnout. He died so suddenly, like in a road traffic accident. (F3)
We should do what needs to be done, with nothing weighing on our conscience, with no regret that we may have left 1/100 or 1/1000 possibility unexplored. (F14)
He perceived the hospital as a prison for the sick,
so we decided to return home.
If we would keep him in the hospital, he would have felt deserted by us, and we didn’t want this to happen. (F-M17)
Hospital care was also chosen by parents who perceived good parenting as ‘sibling(s) protector’ from exposure to dying and death, whereas home care was chosen by parents whose good-parent beliefs involved being a ‘facilitator of sibling sharing’.
They (brother and sister) interacted until the end, exchanged wishes and their love to each other. . . . . . Is there anything more beautiful, and more powerful? He was a bit more distressed after her death, but now feels better that he was at the bedside of his sister until the end. Both children would have been deprived of something precious if they were apart. (F8)
Decision-making led to two types of decisions. Few parents did not decide.
There was NO chance to take the child home, since his care was too demanding. (M4)
Our child should be in her environment with everything that is familiar to her; this was ‘magic’ to her at the very end of her life. (M9)
Yet other parents reported reaching a decision only after lengthy deliberation.
I knew nothing about home care. The day the oncologist informed me about this option, we met with the palliative care physician. I told the oncologist that I am interested in this option, but I want first to meet the physician. So, she came along with her colleagues, and we had a meeting with my wife and the oncologist. She explained how they provide home care services, what were the steps for enroling to their palliative care service. . . . and gained my trust. They had an answer for everything. I appreciated that very much. After this initial meeting, I discussed with my wife, and we both agreed to opt for home care. (F13)
What I experienced at home was beautiful. I wouldn’t have experienced all these special moments and family farewells in the hospital. . . . But at the very last moment, I do not know what I felt, but I had to do something, and called for an ambulance. The hospital physician warned me that the child could die on the road, and asked me if I was certain about my decision. And I said: ‘yes, I want to do that’. (M12)
I believed that we would give a fight. . . . and I was optimistic. . . . That is why it all came so suddenly and I was unprepared. I couldn’t imagine that things would develop in such a way. . . . Physicians informed us, but I didn’t want to believe them. I didn’t expect this evolution, and I realised only the very last day that we had come to the end. (F3)
The derived model (Figure 2) depicts the interrelation between (1) decision-making processes, (2) types of decisions reached, and (3) factors affecting the choice of place for end-of-life care and death.
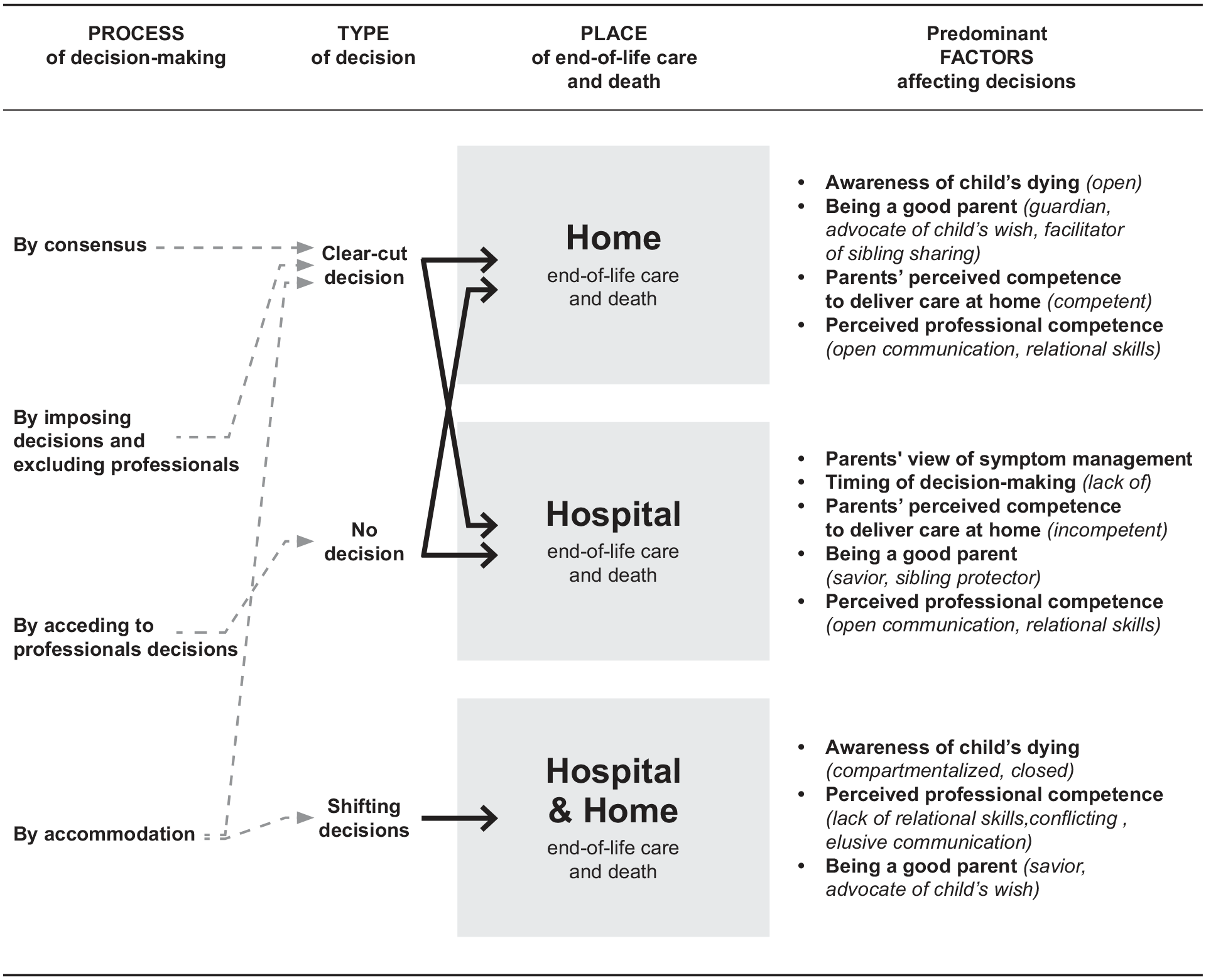
Model on parents’ decision-making about place of end-of-life care and death.
Decisions for hospital end-of-life care and death were most likely when (1) physical symptoms were perceived as uncontrollable, (2) parents felt they lacked the time to develop skills, (3) doubted their ability to care for the child at home, and (4) defined ‘good parenting’ as an act of leaving no stone unturned and of protecting siblings from exposure to death.
Decisions for home were most likely when parents (1) maintained open awareness of the child’s dying condition, (2) felt competent in caring for their child at home, (3) perceived good parenting to be ‘guardians’ by making decisions -to prevent unnecessary suffering, ‘advocates’ by fulfilling the child’s wish to be at home, and/or ‘facilitators’ of sibling sharing of a dignified death. Although painful, parents described their experience as unique and meaningful.
Clear-cut decisions for home or hospital were reached by mutual consensus, by accommodation, or by imposition of parental decisions on professionals who were in conflict with parents’ preferences. By contrast, shifting decisions were typical of parents with closed or compartmentalised awareness of the child’s dying, whose belief of being a good parent involved acting as ‘saviours’ of the child’s life or as ‘advocates’ of his or her wish to return home. Clinicians accommodated to these shifting decisions. No decision was typical of parents who maintained a closed awareness and acceded to professionals’ decisions.
Discussion
Main findings
The proposed model suggests that the decision to pursue home or hospital as the place of end-of-life care and death is complex and multidimensional. Six factors are involved: awareness of child’s impending death, parents’ perceived competence to deliver care at home, perceived professional competence, view of symptom management, timing of decision-making, and being a ‘good parent’. The salience of each of these factors differs in the choice of home versus hospital.
In the decision to go home, beliefs about what it is to be a ‘good parent’ emerges as the primary factor affecting choice among parents who were aware of death’s imminence; whereas in the decision to be in hospital parents’ views of symptom management is primary and affected by the severity of the child’s condition, the timing of decision-making – not long enough to become competent and confident in delivering care at home. ‘Perceived professional competence’ cross cuts both decisions suggesting that the clinicians’ ability to communicate honestly and relate with compassion affects parents’ decisions about the place of their child’s dying and death regardless of the chosen place.
Our findings also support four distinct processes through which decisions are made or avoided: ‘mutual consensus’, ‘accommodation’, ‘acceding to professional decisions’ or ‘imposition of parental decisions and exclusion of professionals’. Most parents eventually reach a clear-cut decision as to the place of dying and death; fewer vacillate between possible courses of action and change preferences as death becomes imminent. Parents who maintain closed awareness are unable to consider alternative options and avoid decisions altogether.
Several factors identified in this study have not been as prominent in other studies of parents’ end-of-life experiences26–28 or decision-making.29–38 Particularly, the parents’ perceptions of their competence and confidence in delivering care at home, suggests a new area deserving our attention in end-of-life decision-making theory and practice about place of care and death.
In contrast to the Hannan and Gibson 22 study which supports that parents react to places where their family feels safe or unsafe rather than decide, and to Montel’s et al. 23 findings which refer to parental motivations for home or hospital death, the present findings suggest that parents actively engage in decision-making, with the majority reaching, spontaneously or after deliberations a clear-cut decision for home or hospital. Parents are active agents in the care of their children, not passive recipients.
The identified perceptions of ‘good parenting’, resonate with some of the predominant explicit heuristics used in parents’ end-of-life decision-making. 39 These heuristics act as mental short-cuts that reduce parents’ cognitive burden associated with decision-making, 40 thus preventing a lingering on dilemmas over the location of care at the terminal phase. It further explains the parents’ increased reports of clear-cut decisions.
Definitions of ‘good parenting’ at the end-of-life 41 as well as changes over time in the ‘good parent belief system’ have been documented. 42 In the present study five definitions have been identified in parents’ reports: ‘saviour’, ‘guardian’, ‘advocate, ‘sibling protector’ and ‘facilitator of sibling sharing’. These definitions both confirm and enlarge prior evidence.
Compared to a Greek study conducted 25 years ago, 43 when hospital was the only option available for children dying of cancer, the present findings highlight how the introduction of palliative home care services may affect practices and decisions among parents and clinicians. Choosing to return home then meant that parents were on their own in caring for their dying child, whereas now the burden and responsibility for decision-making is shared with professionals and often achieved by consensus or accommodation.
Not surprisingly, parents who are overwhelmed by the child’s dying or the burden of decision-making value that clinicians decide on their behalf. However, the majority opt for a process described in the literature as ‘shared decision-making’44,45 and ‘collaborative communication’ at the end-of-life, 46 with the maintenance of the clinician–parent relationship as of outmost importance. 47 The proposed decision-making model further enriches the current evidence-based international mapping of end-of-life decision-making styles.36,48,49
Strengths and limitations
Methodological strengths include researcher triangulation in data collection and analysis, and theoretical sampling to ensure maximum variation and heterogeneity among mothers and fathers of children of different ages, with malignant and non-malignant diseases. However, the study shares some problems common to retrospective studies on bereaved parents, who may cope with the loss of their child by constructing a narrative they can live with. While questions about generalisability of findings to other cultures and health care systems beyond Greece can be raised, the articulation of an explanatory model derived from empirical findings has relevance beyond Greece, particularly in countries which are in the process of developing paediatric home care services. Helping professionals become knowledgeable of the complexity of factors and processes affecting parental decision-making, will enhance the quality of end-of-life care and positively affect the family’s adjustment to the child’s loss.
What this study adds
Findings illuminate for the first time how different decision-making processes, affected by a variety of interrelated factors, lead to distinct types of decisions about the place of a child’s end-of-life care and death.
Findings have clinical implications for health professionals who, in addition to providing clear and honest information, should explore options about the place of end-of-life care and death in a timely way so as to allow parents to develop competence and confidence to assume care at home, should they choose so. Policy makers should improve end-of-life care at all sites, since home and hospital are desirable to different families, for different reasons, at different times.
Footnotes
Authors’ contributions
All authors have approved the final version of the manuscript for publication. They have actively participated through the entire process in the design of the work, analysis and interpretation of data. D.P. was the principle investigator and was involved in the methodological design of the study, in data analysis and in the writing of article. V.K. and P.L. conducted the interviews with parents whose child received palliative care at home and were involved in the coding and data analysis. E.K. conducted the interviews with the parents whose child was cared for at the hospital. All researchers were clinicians and experienced in providing adult or paediatric palliative care. M.B-L. was involved in the design and data analysis, development of core categories and sub categories, drafting and redrafting of paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: The authors’ contribution was funded by their posts- Danai Papadatou by the National and Kapodistrian University of Athens, Vasiliki Kalliani, Eleni Karakosta, and Panagiota Liakopoulou by Merimna, and Myra Bluebond-Langner by the True Colours Trust and her research at GOS-ICH that is supported by NIHR Great Ormond Street Hospital Biomedical Research Centre.
Ethical approval
Approval to conduct the study was obtained by the Scientific Committee of the Children’s Hospital ‘P & A Kyriakou’ (667/17.01.2014), the Ethic Committee of the Faculty of Nursing of the National and Kapodistrian University of Athens (128/8.05.2014). Data collection and analysis began in 2015. All participants received information about the study, and provided written consent. Data was securely stored per regulation of the National and Kapodistrian University of Athens.