
Abstract
Background:
The increased number of deaths in the community happening as a result of COVID-19 has caused primary healthcare services to change their traditional service delivery in a short timeframe. Services are quickly adapting to new challenges in the practical delivery of end-of-life care to patients in the community including through virtual consultations and in the provision of timely symptom control.
Aim:
To synthesise existing evidence related to the delivery of palliative and end-of-life care by primary healthcare professionals in epidemics and pandemics.
Design:
Rapid systematic review using modified systematic review methods, with narrative synthesis of the evidence.
Data sources:
Searches were carried out in Medline, Embase, PsychINFO, CINAHL and Web of Science on 7th March 2020.
Results:
Only five studies met the inclusion criteria, highlighting a striking lack of evidence base for the response of primary healthcare services in palliative care during epidemics and pandemics. All were observational studies. Findings were synthesised using a pandemic response framework according to ‘systems’ (community providers feeling disadvantaged in terms of receiving timely information and protocols), ‘space’ (recognised need for more care in the community), ‘staff’ (training needs and resilience) and ‘stuff’ (other aspects of managing care in pandemics including personal protective equipment, cleaning care settings and access to investigations).
Conclusions:
As the COVID-19 pandemic progresses, there is an urgent need for research to provide increased understanding of the role of primary care and community nursing services in palliative care, alongside hospices and community specialist palliative care providers.
Keywords
Primary healthcare services play an important role in the provision of palliative care during pandemics, such as COVID-19.
Pandemics and epidemics are associated with an increased number of deaths and increased need for palliative care in the community.
The increased number of deaths and new challenges in end of life care through the COVID-19 pandemic, including symptom profiles, video consultations and the need for personal protective equipment, has placed clear focus on the need for palliative care in all community settings, including care homes.
This review reveals a stark and concerning lack of evidence from previous pandemics related to primary healthcare services in palliative care provision within a pandemic.
Important factors in a successful primary healthcare palliative care response to pandemics include consistent and timely communication between policy makers and healthcare providers; education, training and debrief for the workforce; support for family carers; and continued delivery of equipment and access to necessary support services, such as diagnostic tests.
The review presents a compelling case for more research into the role and response of primary healthcare services in the delivery of palliative care during pandemics, as we progress through the next phases of the COVID-19 pandemic and for future pandemics.
A whole system response to the increased need for palliative care in the community is required, so the findings of this review and future research in this field are of relevance to hospice and specialist palliative care services, as well as policy makers.
Introduction
The provision of palliative and end-of-life care to patients, families and communities is core to the role and identity of primary healthcare clinicians. They are central to the provision of this care and in supporting, and advocating for, patients and their families.1–4 The primary healthcare workforce is diverse, including general practitioners (or family physicians), community nurses, healthcare and support workers. These professionals have the potential to deliver palliative care integrated into every encounter in the community when their working environment allows this, and with the support of specialist colleagues. 5 Prior to the COVID-19 pandemic, barriers to effective palliative and end-of-life care in the community from the perspective of United Kingdom general practitioners included a lack of time with patients and families, inadequate support services in the community, a need for more education and training, and inconsistent access to specialist palliative care services.6,7
The COVID-19 pandemic has been associated with an increased number of deaths in the community, including in care homes. 8 There are challenging new symptom profiles 9 and changes in the way consultations are conducted, with personal protective equipment required or consultations taking part via videoconference. 10 This has significant implications for primary healthcare care teams providing palliative care (the relief of suffering associated with life-threatening conditions) and care of the dying (end-of-life care), alongside providers of specialist palliative care, including hospices.
Palliative care has been recognised as a key part of national and international pandemic responses. 11 A rapid review of the role and response of hospices and specialist palliative care services conducted early in the COVID-19 pandemic highlighted the need for such services to respond rapidly and flexibly during pandemics, including shifting resources into the community. 12 However, a whole system approach is needed, and the role and response of primary healthcare teams and services must be considered alongside that of specialist palliative care services in order to establish collaborative ways of working to meet increased need. This aim of this review was to review the evidence base related to palliative care provision by primary healthcare teams during epidemics and pandemics, in order to inform policy and practice during the COVID-19 pandemic.
Methods
Patient and public involvement
A Patient and Public Involvement consultation exploring the challenges facing palliative care service users and their families during COVID-19 concluded there was an urgent need to provide improved care in the community. 13 The results of this consultation informed the review question and design. Further patient and public involvement took place as the review was conducted with The University of Sheffield Palliative Care Studies Advisory Group, a group of 15 lay advisors with personal experience of palliative care either as patients or carers. They were established through the University of Sheffield in 2009 and have regularly contributed to palliative and end-of-life care research. The group provided feedback on the key findings of the review and the recommendations, ensuring that these were relevant to the patient and family experience.
Review question
The aim of this review is to address the research question:
‘What is the role and response of primary healthcare services in the delivery of palliative care in epidemics and pandemics?’
Design
This rapid review was conducted using modified systematic review methods, refined from the Centre for Reviews and Dissemination guidance for systematic reviews in healthcare 14 and informed by rapid review methods outlined by the Palliative Care Evidence Review Service, 15 with a refined review question, the search carried out within a limited set of databases, and transparency in the reporting. The structure and content of the review is informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Guidelines. 16 A protocol has been registered and published on the PROSPERO database (ref no: CRD42020186010).
Inclusion/exclusion criteria
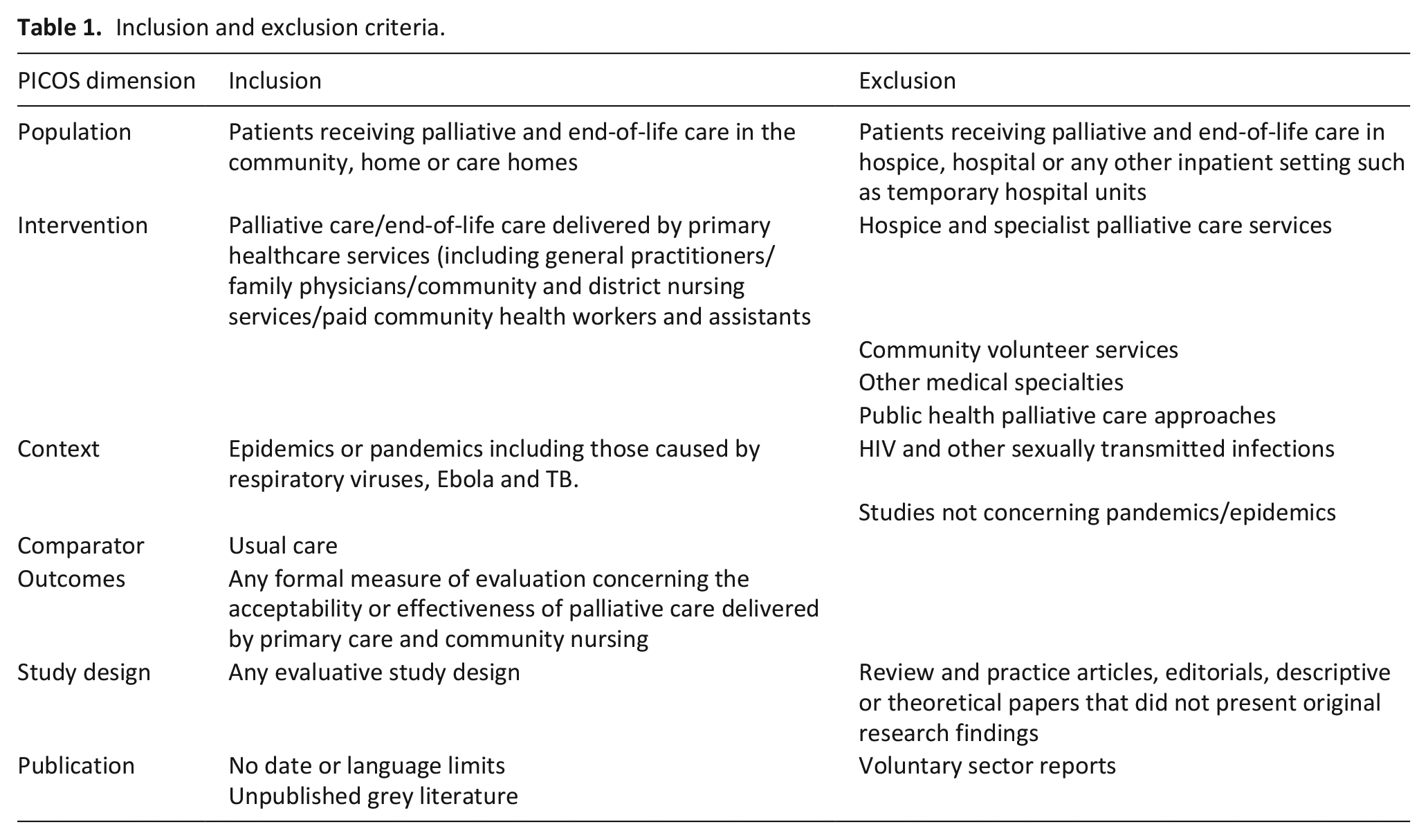
Table 1 provides details of the inclusion and exclusion criteria.
Inclusion and exclusion criteria.
Search strategy
Searches were conducted in Medline, Embase, PsychINFO, CINAHL and Web of Science, by a specialist librarian at the University of Sheffield on 7th March 2020. The search strategy included the following search terms and is detailed in Appendix 1.
Terms for palliative care, end-of-life care, primary care and family practice, community nursing, district nursing
Terms for pandemics and epidemics including specific named pandemics
Further relevant articles that were known to the authors were included. Others were identified through forward and backward citation searching of articles and the reference lists of guidelines from the COVID-19 pandemic.
Study selection
Title and abstracts were uploaded into EndNote and duplicates were removed. Two reviewers (SM and VM) screened article titles and abstracts for relevance independently. Those considered potentially eligible for inclusion were retrieved as full text articles, and three members of the review team (SM, VM and VL) assessed them against the inclusion and exclusion criteria, and discussed whether they would be included.
Data extraction
Data was extracted into a bespoke data extraction form in Microsoft Excel that included the study title, date, location, study design and key findings by two researchers (SM and VL) and independently checked for accuracy and detail by a third (VM).
Quality assessment
Quality assessment of the evidence was attempted using a method and tools proposed by the Palliative Care Evidence Review Service, outlined as suitable for rapid reviews in palliative care.13,16 This quality assessment was conducted by one reviewer (SM) and checked by two others (VM and VL) and disagreements were discussed.
Data synthesis
The included studies were compared in the data extraction table. There were no comparable statistics and therefore a narrative synthesis was undertaken, identifying cross-cutting themes from each study. The narrative synthesis was constructed using Downar and Seccareccia’s model that suggests a palliative pandemic plan should include focus on ‘systems’, ‘space’, ‘staff’ and ‘stuff’. 17 This was chosen to mirror Etkind et al.’s rapid review of hospice and specialist palliative care services, on the basis that primary healthcare services work alongside hospice and specialist services in the practical delivery of palliative care to patients. 11 The narrative was reviewed at intervals for relevance to clinical practice and family experience by the Oxford Centre for Evidence Based Medicine COVID-19 rapid reviews in palliative care group, and patient and public involvement representatives.
Findings
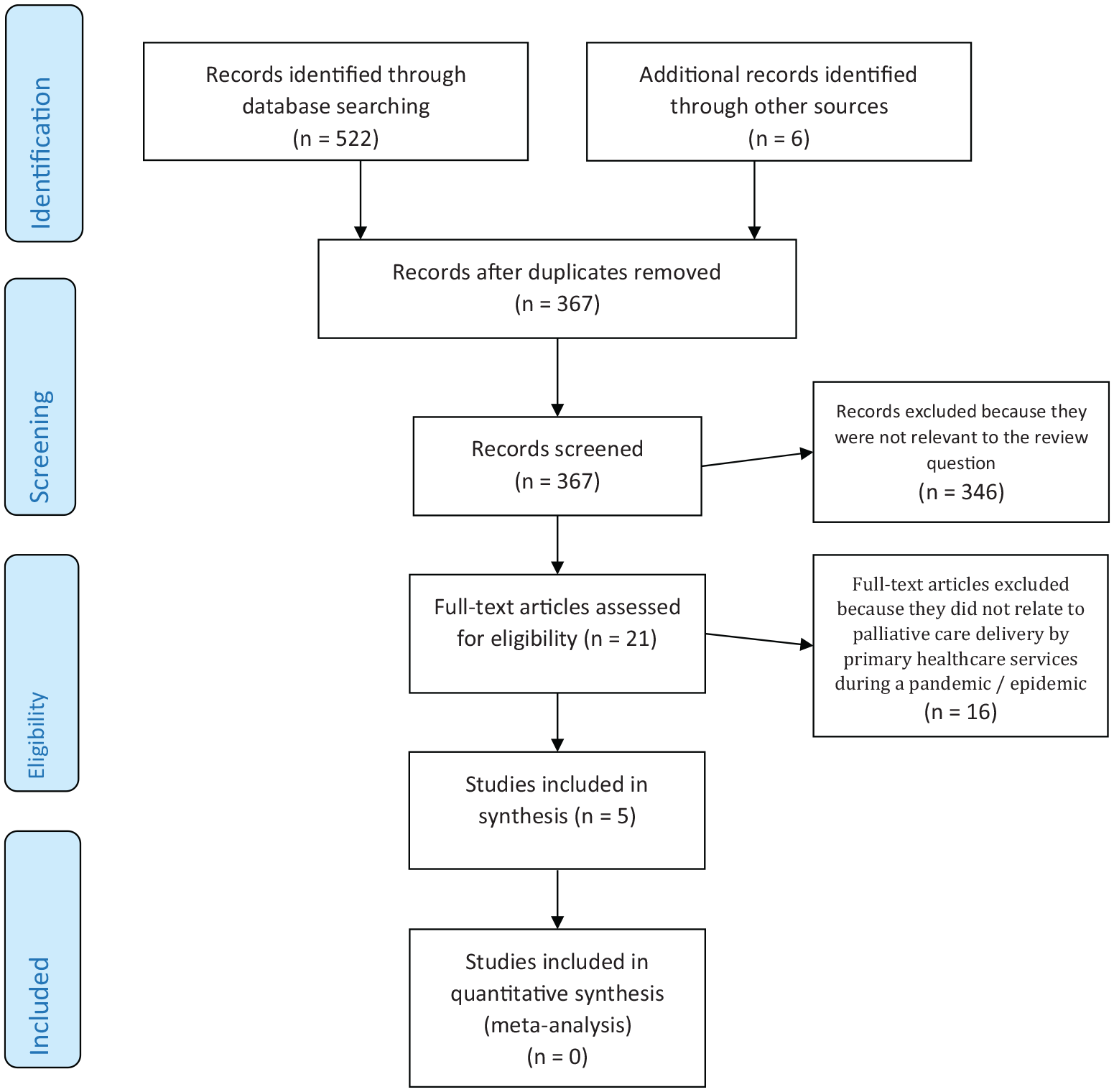
PRISMA flow diagram.
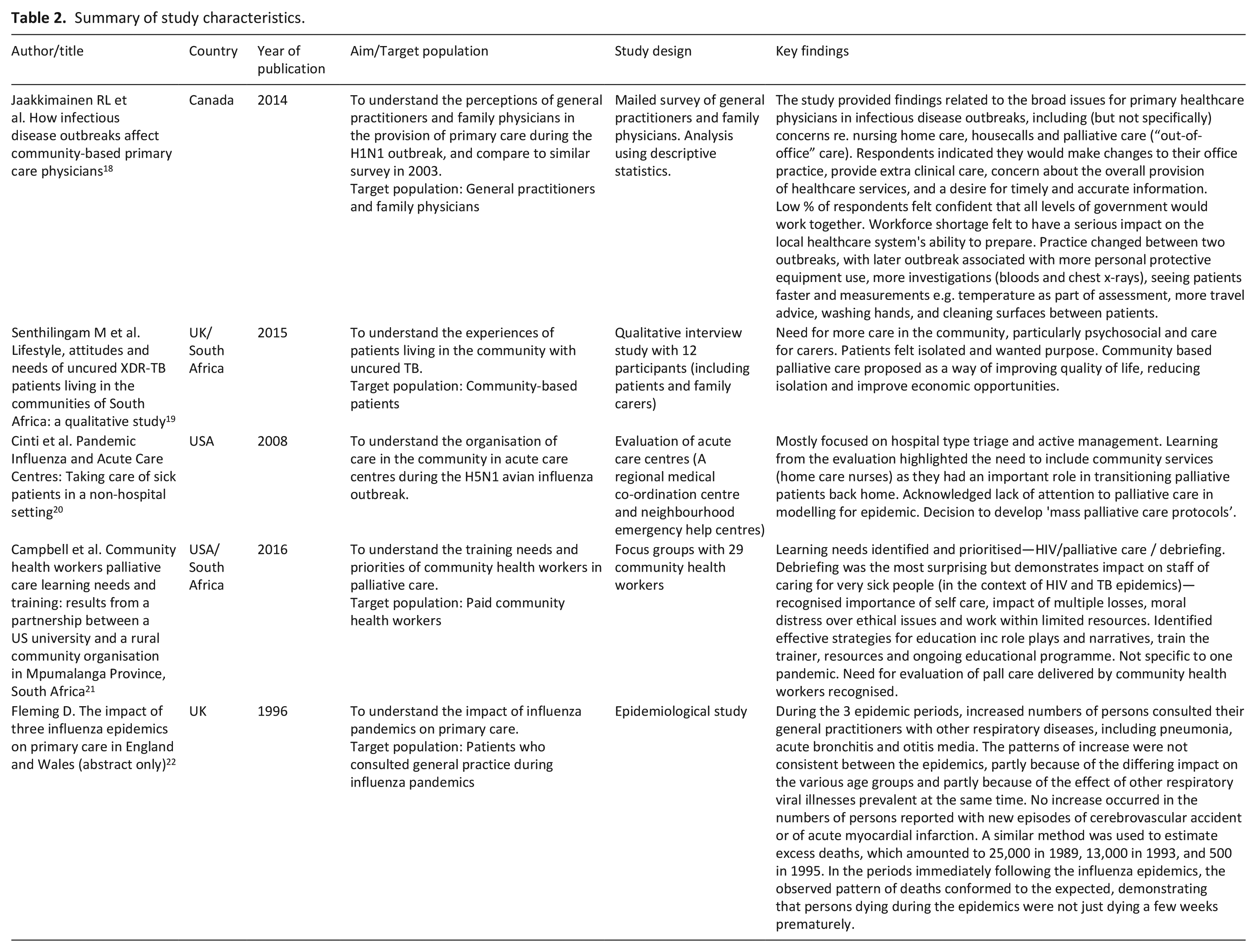
Study location: Of the five articles that met the inclusion criteria, one was from Canada, 18 one from the UK, 22 one from the USA 20 and the others written by collaboratively between teams in the UK and South Africa 19 and the USA and South Africa. 21
Study design: All of the identified studies were observational, there were no randomized-controlled trials or systematic reviews. One was a qualitative interview study of patients with uncured TB, 19 one was a survey of general practitioners and family physicians, 18 one was an evaluation of a community acute care centre, 20 one was a qualitative interview study of community support workers and evaluation of an educational programme, 21 and the other reported epidemiological data. 22
Study quality: Together the studies represented a heterogeneous and very small body of evidence. Quality appraisal was attempted on the four full-text articles, three of which were research studies.18,19,21 All had ethics approvals in place and acknowledged the limitations of the study design and findings. The fourth full-text article was a description of care centres and learning from their implementation, rather than a research study. 20 Quality appraisal was not conducted on the abstract as there was insufficient information available to do so. 22 So few articles were identified that none were excluded on the basis of the quality appraisal.
Study characteristics are summarised in Table 2.
Summary of study characteristics.
Key themes
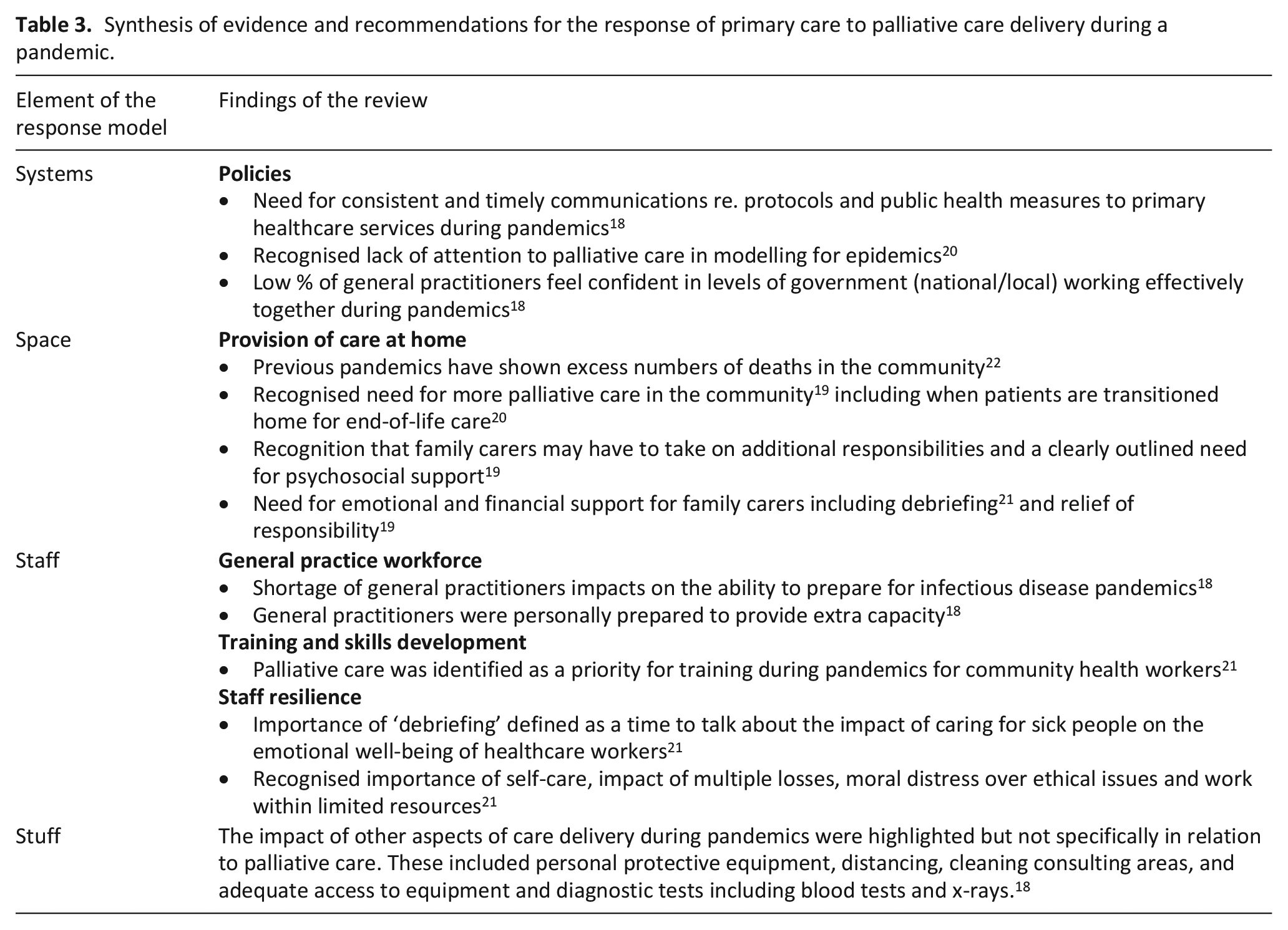
The articles together provided very limited insights into the role and response of primary healthcare services in palliative care delivery during pandemics. We therefore used the pandemic response framework 15 to categorise what little data that was available into ‘systems’ (data that provided insights into wider healthcare systems including policy), ‘space’ (insights into primary healthcare delivery of palliative care in the community), ‘staff’ (workforce concerns) and ‘stuff’ (all other relevant concerns; see Table 3). 17
Synthesis of evidence and recommendations for the response of primary care to palliative care delivery during a pandemic.
Systems
Excess deaths in the community during a pandemic have an impact on primary healthcare services, 22 however a lack of attention to palliative care was noted in pandemic planning and service modelling in general practice and community services, despite the need for ‘mass palliative care protocols’ being raised during past pandemic influenza outbreaks. 20 In one study, a low number of general practitioner respondents felt confident that all levels of government would work together to provide the information that they needed to prepare their services for a pandemic. 18 There were also concerns that primary healthcare services were disadvantaged with respect to consistent and timely communications about policy and processes, such as screening protocols, treatment protocols, public health measure summaries and information from local hospitals, although this was not specifically in relation to palliative care. 18
Space
The studies provided limited insights into the importance of the community as a care setting, with a need for more palliative care in community settings during pandemics. Community based palliative care was proposed as a way of improving quality of life and reducing isolation. 19 The important role of community nurses in transitioning patients discharged from acute hospitals and care centres to receive palliative and end-of-life care in the community was specifically highlighted. 20
Only one study included patient data, relevant to the provision of palliative care in the community during pandemics. Patients stated that reasons for choosing to receive care at home included the trauma of seeing others die of the same disease in hospital, and the associated removal of hope. 19 The need for psychosocial care for patients who were at particular risk of feeling isolated due to their infection risk, and support for family carers in the community, were pressing concerns. 19 The importance of debrief for family members who were ‘chosen by healthcare services to be responsible’ for aspects of patient care was described, as well as the need for services to be able to provide occasional relief of some of that responsibility. 19
Staff
The studies together described a range of primary healthcare professionals involved in palliative and end-of-life care during pandemics, including general practitioners, community nurses and community health workers. Workforce concerns included inadequate numbers of community nurses 21 and general practitioners, 18 with solutions including the employment of community health workers, 21 and individual general practitioners expressing a willingness to work longer hours and personally provide extra capacity during pandemics. 18
Palliative care was identified as a specific training need for community health workers during pandemics, with effective strategies for education including role plays and narratives, training the trainer, online resources and an ongoing educational programme. 21 The importance of ‘debriefing’, defined as a time to talk about the impact of caring for sick people, on the emotional wellbeing of healthcare workers, was described as ‘surprising’ finding, but was valuable to staff who were dealing with the impact of multiple losses, moral distress over ethical issues and work within limited resources. 21
Stuff
Palliative care was recognised as one aspect of care provided in primary healthcare of importance during pandemics, alongside many others. Other aspects of care provision during a pandemic that caused concern for the organisation of primary healthcare services included the need for personal protective equipment, distancing, regular of cleaning consulting areas, access to equipment and timely diagnostic tests including blood tests and x-rays. 18
Discussion
Main findings
This rapid review reveals a stark lack of evidence around the role of primary healthcare services in palliative care provision during pandemics. The five papers that were identified highlighted the need for more palliative care in the community during pandemics, and that primary healthcare services have a role in the provision of such care within their wider work and pandemic response. The limited evidence that was available could be aligned with a pandemic response framework for palliative care, 17 however there is currently insufficient evidence to support the development of a framework to either improve understanding of the role, or enabling the response of, primary healthcare services in the delivery of palliative care during pandemics. No evidence was identified that has been conducted in this area during the COVID-19 pandemic. The review provides a compelling case for research to capture the learning, experiences, effective innovations and service developments that are happening now in this important aspect of care in the community during the COVID-19 pandemic.
Strengths and limitations
A strength of the study is its specific focus on primary healthcare services in the provision of palliative care during pandemics. However, the body of evidence included in this review was very small, and heterogeneous in terms of study design. All of the studies were observational, and the generalisability of their findings is limited. Palliative and end-of-life care in primary care was considered amongst many issues being studied in the research, rather than as a focus for research in it’s own right. Furthermore, the very specific focus of the review has excluded any previous research into the delivery of palliative care in primary care more broadly that also has relevance to the delivery of such care during the current COVID-19 pandemic and future pandemics.
What this study adds
Past pandemic plans and frameworks for primary care place focus on surge in demand for primary care services in their entirety, sustaining urgent and essential services, public health responsibilities including infection control and immunisation, ensuring clinical facilities and equipment are adequate, and maintaining business continuity. 23 There appears to be some disconnect between this and the need for more palliative care in the community during pandemics, including the current COVID-19 pandemic.11,24–26 This review highlights the need for more research into palliative and end-of-life care to inform future plans and frameworks for the response of primary healthcare services to a pandemic.
Observations in primary healthcare practice in the UK are that the provision of palliative and end-of-life care has been a significant role for these teams during the COVID-19 pandemic, including in care homes. Some aspects of palliative care, such as advance care planning, have received attention in national general practice policy documents with recommendations made during COVID-19 in the National Health Service in England. 27 However there are many more new challenges associated with COVID-19 and the delivery of palliative care in the community, and there is an imperative to learn from these now, particularly as COVID-19 becomes a longer term issue. 28 These challenges include the greater risk of virus transmission and lethality compared to other viruses, the need for personal protective equipment in consultations, concerns about limited drug supplies and the equipment necessary for symptom control, and patients being isolated from their families and carers at the end of their lives. Out-of-hours palliative and end-of-life care provision is also an important concern. This review suggests factors in a successful primary palliative care response to a pandemic include consistent and timely communication between policy makers and primary healthcare providers; education, training and debrief for the workforce; support for family carers; continued delivery of equipment and access to necessary support services, such as diagnostic tests. However, much more evidence is needed to inform such a response.
There are other important considerations in the role and response of primary healthcare services to palliative care in COVID-19 and future pandemics. The needs of family carers, who may be apart from their dying relatives or who may have to take on increased responsibility for hands-on care of a relative during pandemics, must be considered. They may have a need for psychosocial support, debrief and relief of the responsibility, as well as training, if they are to take on aspects of care including the administration of end-of-life drugs. 29 More research into the impact of COVID-19 deaths on subsequent bereavement is also necessary. 30 Recognition of the role and potential of primary healthcare teams, within the communities they serve is required, alongside consideration of the role and response of hospice and specialist palliative care services in pandemics, is required in order to deliver care to patients and families as effectively as possible. Local and regional variations in practice and the development of collaborative relationships between generalist and specialist providers of palliative care must be better understood to inform national policy and recommendations for service delivery during the next phases of COVID-19 and future pandemics.
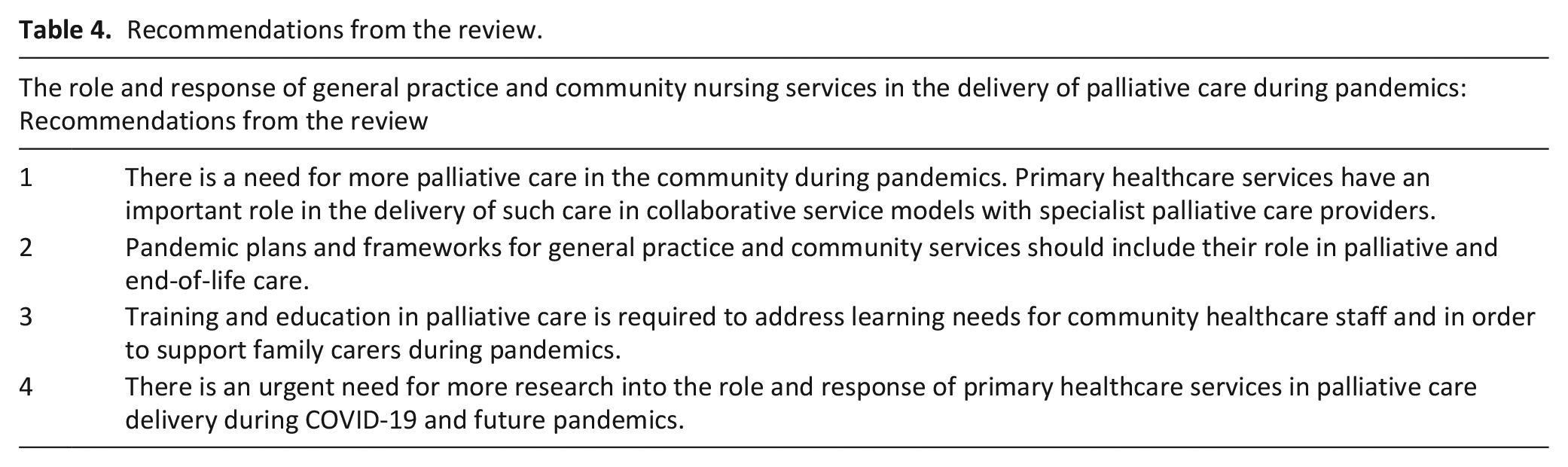
Taking the findings of the review, and working in partnership with patient and public involvement representatives, four very broad recommendations have been developed, summarised in Table 4. Group members supported the recommendations for shared learning, the need for emphasis on staff and family carer resilience and measures to foster this, and increased support for family carers. They raised further concerns around access to personal protective equipment for healthcare staff, support for care homes, and the extent to which community involvement in palliative care could and should continue post-COVID 19, all of which are important considerations for future research.
Recommendations from the review.
Conclusion
Primary healthcare services have an important role to play in the provision of palliative care to all who need it, alongside providers of hospice and specialist palliative care services. During a pandemic, there is a risk of increased numbers of deaths and primary healthcare services need to be able to respond effectively, alongside specialist palliative care services including hospices. This is an important consideration for clinicians, primary healthcare service managers and for policy makers. There is an urgent need for research to inform recommendations for how the response to increased need for palliative care in the community in primary healthcare, through both the COVID-19 pandemic and future pandemics, and for pandemic planning to include this aspect of patient care.
Footnotes
Appendix 1: Search details
All searches conducted on 7th May 2020
Database: Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily <1946 to May 06, 2020>
Search Strategy:
————————————————————————————————————————
***************************
Database: Embase <1974 to 2020 May 06>
Search Strategy:
————————————————————————————————————————
***************************
Database: APA PsycInfo <1806 to May Week 1 2020>
Search Strategy:
————————————————————————————————————————
***************************
CINAHL
————————————————————————————————————————
Web of Science
Databases = WOS, BCI, BIOSIS, CCC, DRCI, DIIDW, KJD, MEDLINE, RSCI, SCIELO, ZOOREC Timespan = All years
Search language = Auto
Acknowledgements
The authors would like to thank University of Oxford Centre for Evidence Based Medicine rapid reviews in palliative care team, Prof Irene Higginson (Kings College London), and the Sheffield Palliative Care Studies Advisory Group for their input and advice to this study. Thank you also to Anthea Tucker, specialist librarian at the University of Sheffield, for conducting the searches.
Authorship statement
SM designed the study. SM, VM and VL retrieved and analysed the data, and drafted the article. CG liaised with the PPI advisory team. CG and NJ revised the article critically for clarity and intellectual content. All authors have approved this version for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics
This is a rapid review of published literature. It did not require any ethical review and did not raise any ethical concerns in its conduct.