
Abstract
Background:
Increasing evidence shows that advance care planning is effective in improving outcomes. However, its applicability and acceptability outside Western cultures remain unknown. Examination of relevant cultural adaptations is required prior to wider adoption.
Aim:
To examine the feasibility and acceptability of a culturally adapted advance care planning intervention in a Taiwanese inpatient hospital for advanced cancer patients, family members and healthcare professionals.
Methods:
A single-group, non-controlled, mixed methods feasibility study guided by a previously developed logic model. The culturally adapted advance care planning intervention represented a one-time intervention, comprising pre-advance care planning preparation and follow-up consultation. Qualitative interviews explored participants’ view on their involvement in the study. Patients’ medical records were examined to assess intervention fidelity. Findings from both data sets were integrated following analysis.
Results:
N = 29 participants (n = 10 patients; n = 10 family members and n = 9 healthcare professionals) participated in the intervention, of who 28 completed follow-up interviews. Of the 10 advance care planning interventions delivered, most components (n = 10/13) were met. Key contextual moderators influencing the intervention feasibility included: (1) resource constraints resulting in increased workload; (2) care decisions informed by relatives’ experiences of care; (3) the requirement for financial and policy support; and (4) a presumption for end-of-life care provision and surrogate decision-making. Six areas of intervention refinement were identified for future research.
Conclusion:
Implementing a culturally adapted advance care planning intervention in an inpatient hospital setting in Taiwan is possible. The participants reported the intervention to be acceptable. However, careful attention to the conceptual underpinning using local primary data is imperative for its success.
Advance care planning is considered beneficial to patients and family members. However, the transferability of the Western-oriented advance care planning to other cultures is inadequately understood.
It is essential to understand the feasibility and acceptability of a culturally adapted advance care planning intervention to optimise its implementation and inform the methods for a full trial.
Implementing a culturally adapted advance care planning intervention for people living with advanced cancer, their family members and healthcare professionals in a tertiary inpatient hospital in Taiwan is possible, and the participants reported the intervention as acceptable.
An integrated conceptual model is proposed, highlighting the contextual moderators, advance care planning implementation processes and potential research areas for future modification.
Key contextual moderators include (1) resource constraints resulting in increased workload; (2) care decisions informed by previous care experience of relatives; (3) requirement for financial and policy support; and (4) a presumption for end-of-life care provision and surrogate decision-making.
Careful attention to building the conceptual underpinning of the advance care planning intervention enables these properties to be achieved.
This conceptual model on advance care planning has applicability for other settings attempting to introduce advance care planning in the wider Asia-Pacific region and in settings where it has not previously been used.
A rigorous evaluation of this conceptual model in a full feasibility trial is required before proceeding to a full-scale trial.
Introduction
Advance care planning is intended to facilitate individuals of any age and at any stage of disease to express their life values and future care preferences to improve healthcare outcomes1,2 and is now widely accepted as a component of high-quality palliative care. 3 Increasing evidence demonstrates that healthcare outcomes can be improved when patients, and their family members, develop advance care plans. Benefits include increasing goal-concordant care provision and use of hospice and palliative care, and commensurate decreases life-sustaining treatments and hospital resources.4,5 However, most research examining advance care planning has been conducted in Western countries.6–10 Therefore, cultural adaptation is essential when initiating and embedding advance care planning into local clinical practice in non-Western contexts for people of different cultural backgrounds and ethnicities.8,11
In the Asia-Pacific region, the trend of involving patients in medical decision-making is receiving increasing attention.12–15 This has been driven by political initiatives and legislation (or guidance) that recognise an individual’s autonomy 16 (e.g. Patient Right to Autonomy Act in 2016 in Taiwan 17 and Mental Capacity Act in Singapore 14 ). This is particularly relevant to Taiwan where the number of people living with, and dying from, cancer is increasing. 18 However, little is known about the feasibility and acceptability of advance care planning for those living in the Asia-Pacific region. Examination of these issues associated with a novel intervention that aims to improve patient outcomes, make efficient use of scarce resources and obtain relevant metrics prior to full-scale trial is essential.19,20 This study aimed to examine the feasibility and acceptability of a culturally adapted advance care planning intervention (i.e. whether this intervention could be delivered? And how did the intervention work in a different context? Will patients and families be willing to take part in this study?) among advanced cancer patients, family members and healthcare professionals in an inpatient hospital in Taiwan.
Methods
Study design and theoretical underpinning
A single-group, non-controlled, mixed methods feasibility study using primarily qualitative methods with an embedded quantitative component was conducted from December 2018 to January 2019. The study was guided by a logic model developed from the integration of the findings from a systematic review 6 and a qualitative study. 21 In addition, the Medical Research Council Process Evaluation of Complex Interventions Guidance 22 and the ‘Theory of Change’ 23 were utilised to integrate the development work and evidence base to form a logic model detailing the key elements that underpinned the advance care planning intervention (see Figure 1). 6 We also evaluated recruitment, protocol adherence and explored participants’ views of intervention feasibility and acceptability. 24 Ethics approvals were obtained from King’s College London Research Ethics Committee (HR-18/19-8367) and Kaohsiung Medical University Hospital Research Ethics Committee (KMUHIRB-SV(II)-20180051).
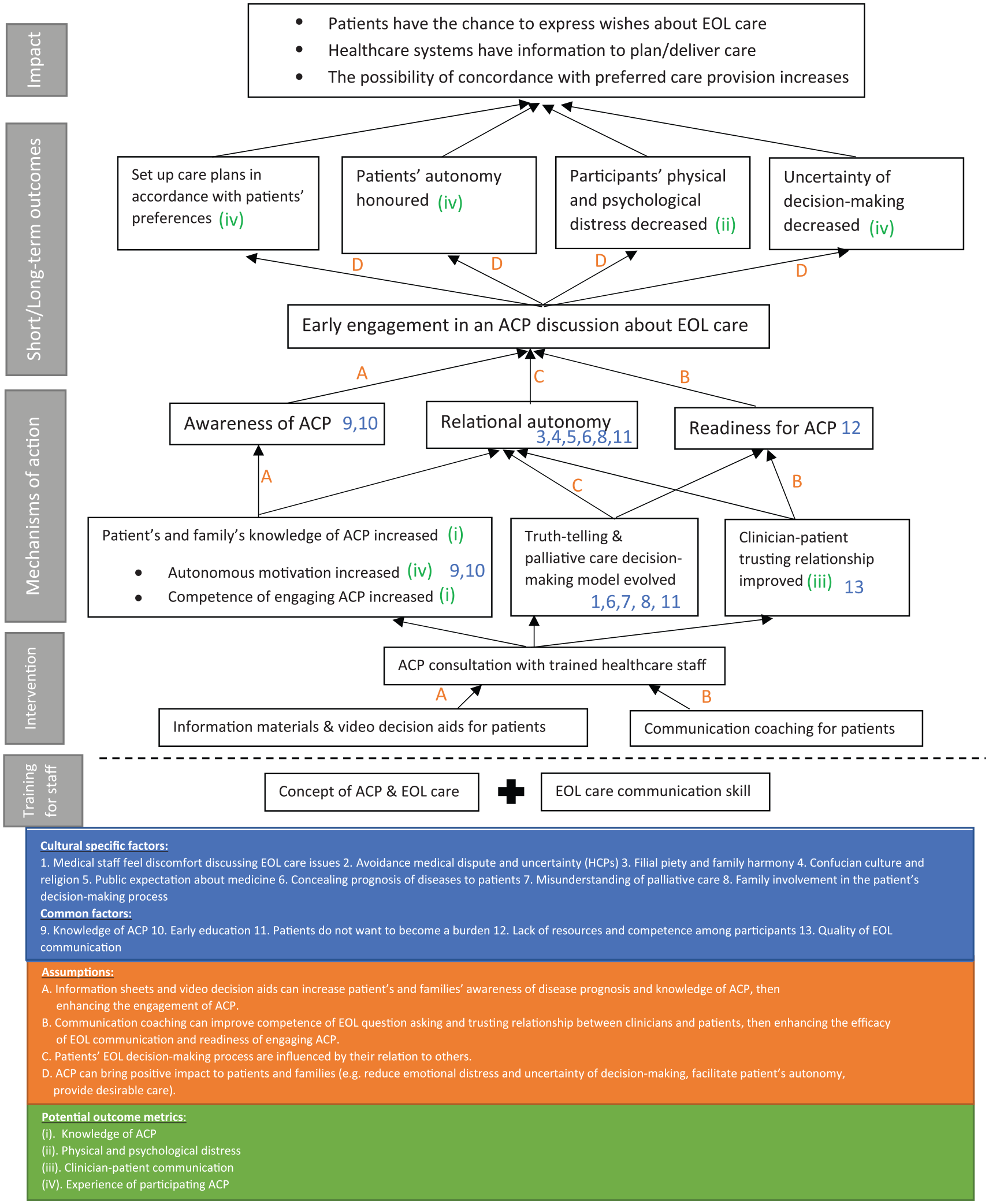
The theory of change of ACP intervention.
Development and implementation of the culturally adapted advance care planning intervention
Development of advance care planning intervention
The logic model detailed conceptually how the intervention influences the advanced cancer population with anticipated outcomes. 25 This also informed the components of the intervention and its associated mechanism of action, the requirement for staff training, and the procedure of implementation. 6 It emphasised the necessity to improve participants’ health literacy and increase their awareness and competence when engaging in advance care planning discussions by providing information materials (i.e. advance care planning leaflets and video decision aids), and communication coaching prior to these potentially difficult conversations. In addition, key components that required greater attention when delivering this culturally adapted advance care planning intervention in Taiwanese context included as follows: (1) the importance of family involvement in patients’ advance care planning preparation and consultation to support their decision-making in line with existing expectations that families take a role; (2) improving patients’ understanding of palliative care options due to low awareness of this approach to care; (3) respecting cultural norms of ‘filial piety’; and (4) providing high-quality end-of-life communication by skilled staff in regard to truth-telling of patients’ disease prognosis due to the current practice of concealment. 21 These components were used to inform the intervention (Figure 1). The local Taiwan legislation on advance care planning 17 was incorporated into the logic model to more closely align the intervention to the local context. The advance care planning intervention was further refined using Theory of Change 23 process of stakeholder consultation using a modified nominal group technique to generate recommendations, and explore consensus, on the advance care planning intervention, including the requirement for training and process of delivery in the clinical environment (see additional file 1 for detail of transparent expert consultation). 23
Advance care planning intervention
The advance care planning intervention was delivered by an advance care planning consulting team that followed the previously developed logic model 6 and local legislation in Taiwan. 17 The team consisted of at least three healthcare professionals representing different disciplines (i.e. a physician, a nurse and a medical social worker or a clinical psychologist). The advance care planning intervention consisted of two phases, including a ‘pre-advance care planning’ preparation phase followed by an ‘advance care planning discussion’ phase (see Figure 2).
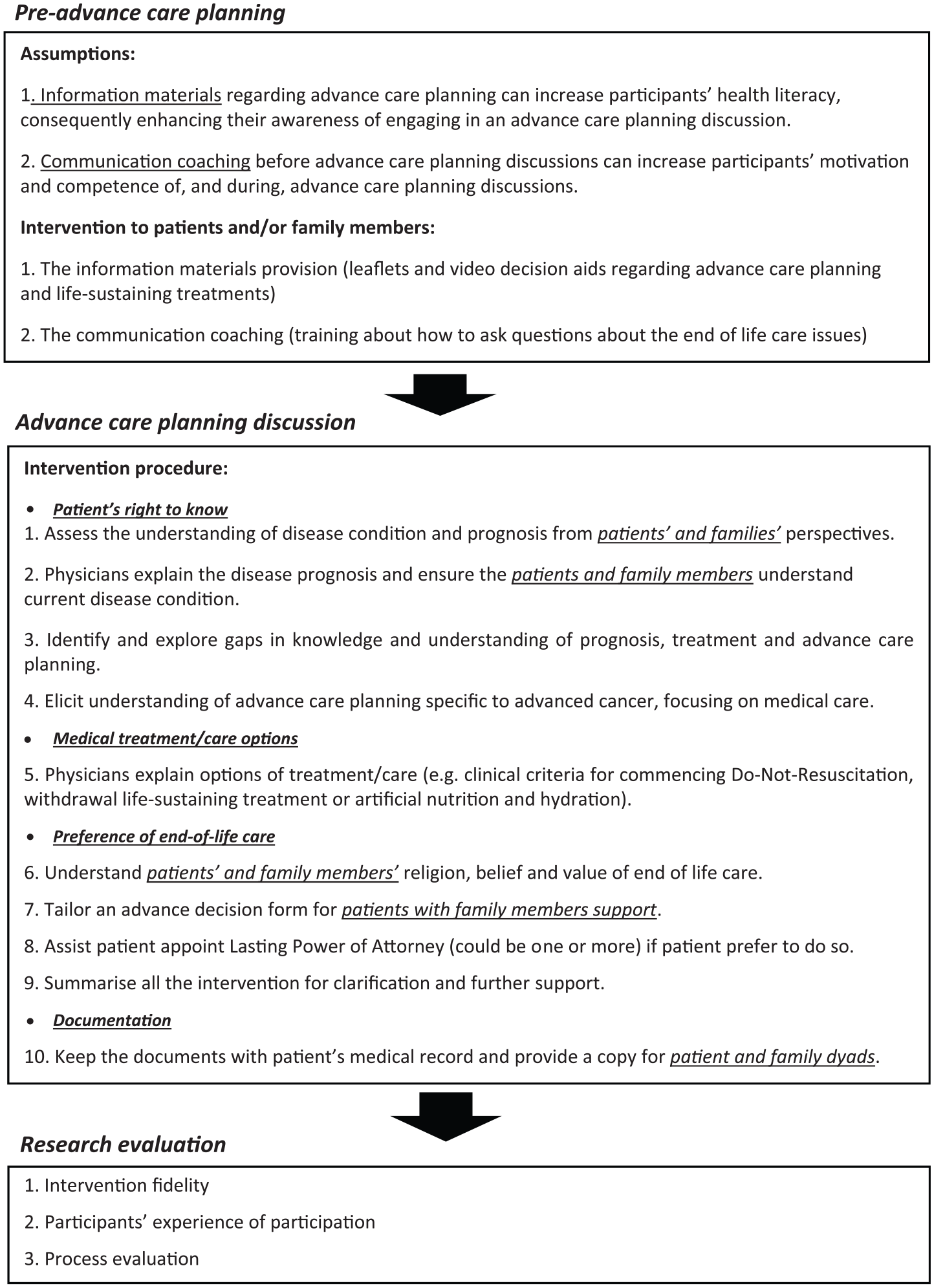
Advance care planning intervention and evaluation for advanced cancer patients and their families.
Pre-advance care planning
Either the nurse or the medical social worker in the team provided participants (patients and family members) with the advance care planning information materials. These included a pamphlet on advance care planning and health literacy, and a video decision aid depicting decision-making processes about life-sustaining treatments for people nearing the end of life to improve their knowledge on advance care planning and palliative care. An individual-based communication coaching session was provided by the same healthcare professional to patient and family dyads in addition to information materials provided to enhance participants’ motivation and competence to be involved in the advance care planning discussions. The communication coaching enabled the patients and family members to identify and prepare for the relevant questions that might need to discuss in the following advance care planning discussion and included issues regarding the patient’s disease prognosis, treatment options and decisions, palliative care options and further lifestyle, among other issues. 6
Advance care planning discussion
After completing the pre-advance care planning phase, the patient (and where relevant patients’ families) received a one-time advance care planning discussion with the consultation team in a quiet and private space at the hospital. In the advance care planning discussion, the physician led the discussion and explored issues, which include the following:
The patient’s understanding about their illness and its prognosis.
The right to refuse certain life-sustaining treatments and artificial nutrition and hydration.
The procedure of completing an advance decision to record the patient’s preferences.
The right to appoint a lasting power of attorney to delegate if a patient loses the capacity to speak for themselves.
The right to amend all the documentation at any future time and how to do it.
During the advance care planning discussion, the patient’s goals of life and care were also discussed to assist the consultation team to tailor the plan in accordance with patients’ preferences. At least one member of the patient’s family was invited to attend the discussion to support the patient if they so wished. 17 Any disagreement regarding a future care plan between the patient and family member(s) was reconciled in the advance care planning discussion. A tailored advance decision form was then drafted by the consultation team to record the patient’s preferences on the end-of-life care and then confirmed with the patient and family.
Healthcare professionals training and support on delivering the advance care planning intervention
The training programme was informed by a review of literature, previous systematic review 6 and qualitative study. 21 The training programme was delivered by C.-P.L. in two 4-hour sessions (see additional file 2 for detail), repeated over 1 week to accommodate healthcare professionals’ working schedule. Healthcare professionals were supported by an ongoing meeting once per week with the research team to discuss and reflect on any obstacles regarding the delivery of the advance care planning intervention.
Evaluation methods
Setting
This study was conducted in a tertiary university hospital in Southern Taiwan, comprising 1688 inpatient beds. Palliative care is provided by a multidisciplinary team, comprising 4 physicians, 20 nurses, 4 hospice-combined care nurses, 3 hospice home care nurses, 1 chaplain, 1 social worker and a clinical psychologist. There are 20 inpatient beds in the hospice and palliative care unit that provide symptoms control, emotional support, and distress relief incorporating community and home care.
Participant eligibility criteria
The eligibility criteria for patient participants included the following: aged 20 years or older, diagnosed with metastatic cancer for at least 2 months, aware of their cancer diagnosis, able to speak Taiwanese or Mandarin and able to provide informed consent. Eligible family members were aged 20 years or older who were nominated by patients to attend the advance care planning discussion. Eligible healthcare professionals included those who completed the training provided by the research team and were willing to provide this culturally adapted advance care planning intervention to advanced cancer patients and families. All had to be willing to provide informed consent.
Participant recruitment and consent
C.-P.L. conducted a study launch meeting with all staff in the hospice and palliative care unit where the aims of the study and process of recruitment were explained. The clinical staff screened potentially eligible patients on hospital electronic databases before approaching them, to introduce the study to them. With permission from the patients, their details were shared with C.-P.L. for further explanation of the study detail and address any question. Family members (including close friends and significant others) were nominated by patients as providing support and care. The eligible healthcare professionals were those who completed the training (additional file 2) and were willing to provide the intervention to patients and family members. All the eligible participants had at least 24 h to consider study participation, after which written informed consents were obtained by those who wished to take part in the study.
To reduce patients’ burden, relevant demographic and clinical (data of cancer diagnosis, diagnosis and prognosis) information was collected from their medical records. This reduced the burden to the participants on the information provided by them during the advance care planning intervention and follow-up interviews. Medical records were only accessed once informed consents were provided by patients.
Qualitative data collection
Face-to-face semi-structured qualitative interviews were conducted by C.-P.L. with patients, family members and healthcare professionals to explore their experiences of study participation. Two topic guides (see additional files 3 and 4) for patients and families and healthcare professionals were developed and informed by the literature, our previous systematic review 6 and qualitative work. 21 The interviews commenced with questions about participants’ general experiences of advance care planning intervention participation followed by questions that focused on how they were asked to participate, intervention components, potential benefits or drawbacks regarding advance care planning, and their views about advance care planning. Interviews also focused on their views regarding the intervention delivery and improvements where relevant. Topic guides were piloted among academic and clinical colleagues in a multidisciplinary centre in London, United Kingdom, and an inpatient hospital in Taiwan and modified accordingly based on feedback. Given the nature of the potential sensitive topics that would be discussed in the interviews, all the interviews were conducted in a separate quiet room to ensure the privacy of participants. A distress protocol was developed to support participants where needed. All interviews were digitally audio-recorded, and field notes were taken after each interview by C.-P.L. to reflect any issues from interviewees’ responses during interviews.
Quantitative data collection
A study fidelity checklist, reviews of medical records and note-taking were used to examine the feasibility of the intervention and evaluate the process of delivery. One of the consulting team members who delivered the intervention completed the study fidelity checklist by ticking the box and providing free text responses if appropriate after each advance care planning discussion. The medical record review and note-taking were conducted by C.-P.L. The study fidelity checklist (Table 1) was developed specifically for this study and informed by our previous work on the development of advance care planning intervention.6,21 Information was also collected regarding the number of participants who were eligible, approached, recruited, and completed the intervention and the follow-up interviews.
Overview of the key components of this study within the fidelity checklist.
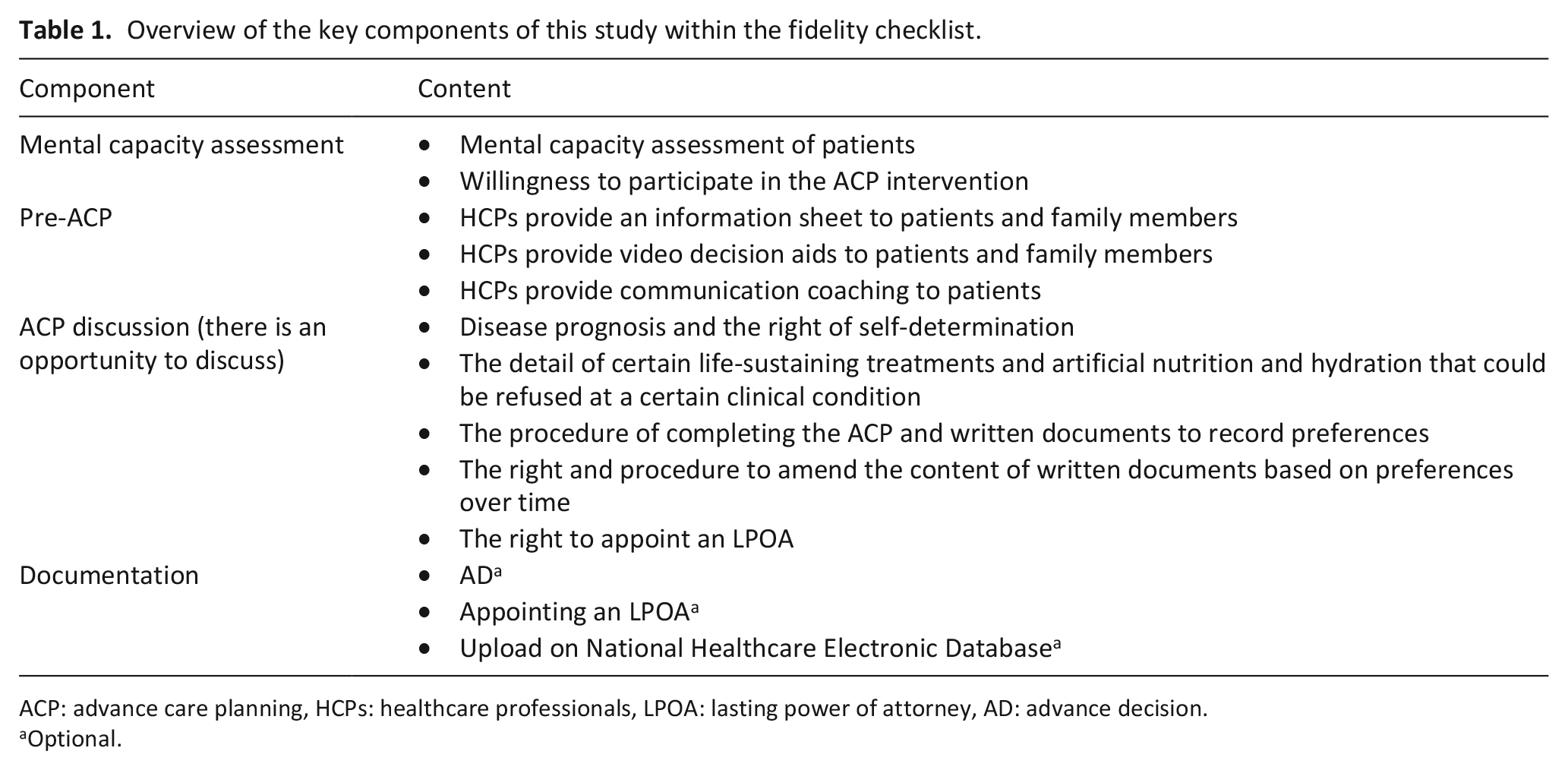
ACP: advance care planning, HCPs: healthcare professionals, LPOA: lasting power of attorney, AD: advance decision.
Optional.
Qualitative data analysis
All interviews were transcribed verbatim in Chinese (the official language at the study site) and imported to NVivo 12 26 to facilitate analysis. Thematic data analysis consisted of five stages: (1) familiarisation of the transcripts by repeated reading of the text; (2) developing initial codes; (3) applying codes systematically to generate themes; (4) reviewing themes with the initial codes and selected quotes for accuracy; and (5) reporting accordingly was adopted. 27 We applied the framework developed from our previous works6,21 (the logic model and decision-making models) to deductively analyse the data and to inductively generate new findings. C.-P.L. performed the thematic coding with review by P.-J.C. to check the accuracy of the coding and discuss areas of disagreement. We analysed the data in Chinese until themes and codes were generated to minimise the potential loss of meaning. 28 C.-P.L., a bilingual nurse and a researcher in palliative care, translated the themes, codes and selected quotes into English to discuss with other English-speaking authors (C.J.E., J.K. and R.H.). A bilingual palliative care physician in Taiwan and P.-J.C. checked the translation for accuracy and credibility. The coding frame was then discussed within the research team for consistency and amended where necessary. Quotes were selected across samples in each group, and the final version of the coding frame was confirmed by the research team. All the personal information including participants’ name, detailed personal background, relationship to family members, and other potentially identifiable information were pseudonymised to ensure confidentiality. 29
Quantitative data analysis
Descriptive data analysis was performed that included the number and proportion of eligible participants approached, recruited and retained, and the completion of intervention and follow-up interviews.
Results
Participant characteristics
A total of 29 participants comprising 10 advanced cancer patients, 10 family members and 9 multidisciplinary healthcare professionals were recruited between December 2018 and January 2019 (see additional file 5). The cancer patients were on average 63.8 years old (SD = ±13.9 years, range = 36–89 years). Most (n = 6) were educated to a high school level. The most common cancers were lung (n = 3) and lymphoma (n = 2). Family members were on average 52.7 years old (SD = ±13.6 years, range = 32–71 years). Most were the patients’ spouse (n = 4) or adult child (n = 3). The healthcare professionals included three physicians, three nurses, two social workers and a psychologist.
Feasibility of the culturally adapted advance care planning intervention
Recruitment and study participation
Overall, 145 potential participants (n = 64 patients were from hospice and palliative care unit; n = 81 patients were from other inpatient and outpatient units) were screened for eligibility by the consulting team and 123 patients were excluded. Twenty-two patients were approached and referred to C.-P.L. for study participation, of which 11 were recruited. Among the patients recruited, nine came from other inpatient and outpatient units and the remaining two were from hospice and palliative care unit. Recruitment was terminated at this time point due to sufficient sample size to explore the feasibility and acceptability of intervention in this study. Ten patients completed the advance care planning intervention in addition to 10 family members’ support. However, only nine patients completed the follow-up interviews (see Figure 3). A total of nine multidisciplinary healthcare professionals in hospice and palliative unit participated in the study and completed the training before commencing the intervention.
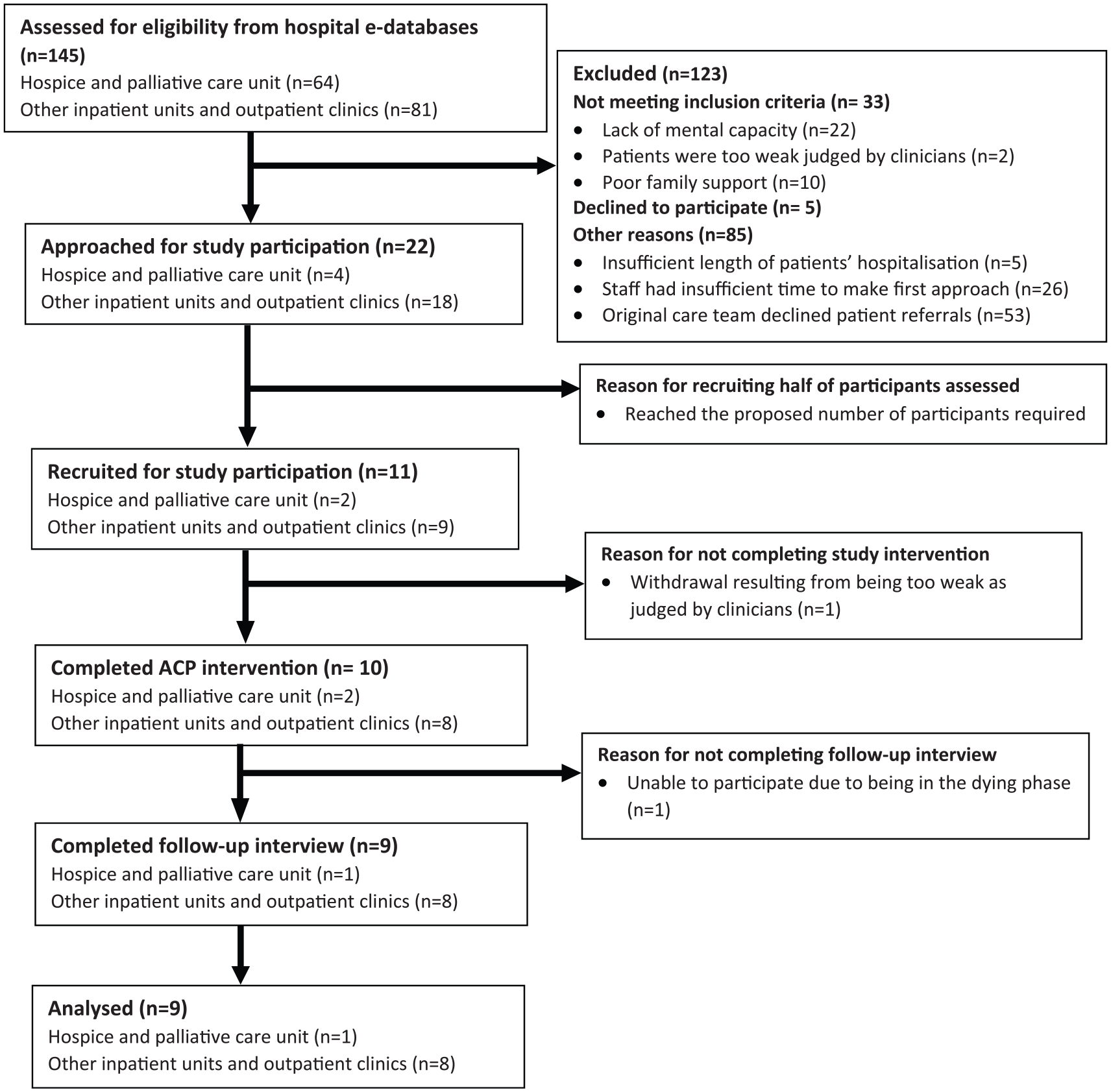
Flow diagram of study participation.
Protocol adherence: study fidelity assessment
Most components (n = 10/13) proposed were met by achieving 70% of the completion rate. However, only n = 6/10 patients receive communication coaching from healthcare professionals; very few of patients appointed a lasting power of attorney (10%) after the advance care planning discussion, and half of them chose to upload advance decision form on National Healthcare Electronic Database (see Table 2).
Study fidelity assessment of implementing culturally adapted advance care planning intervention.
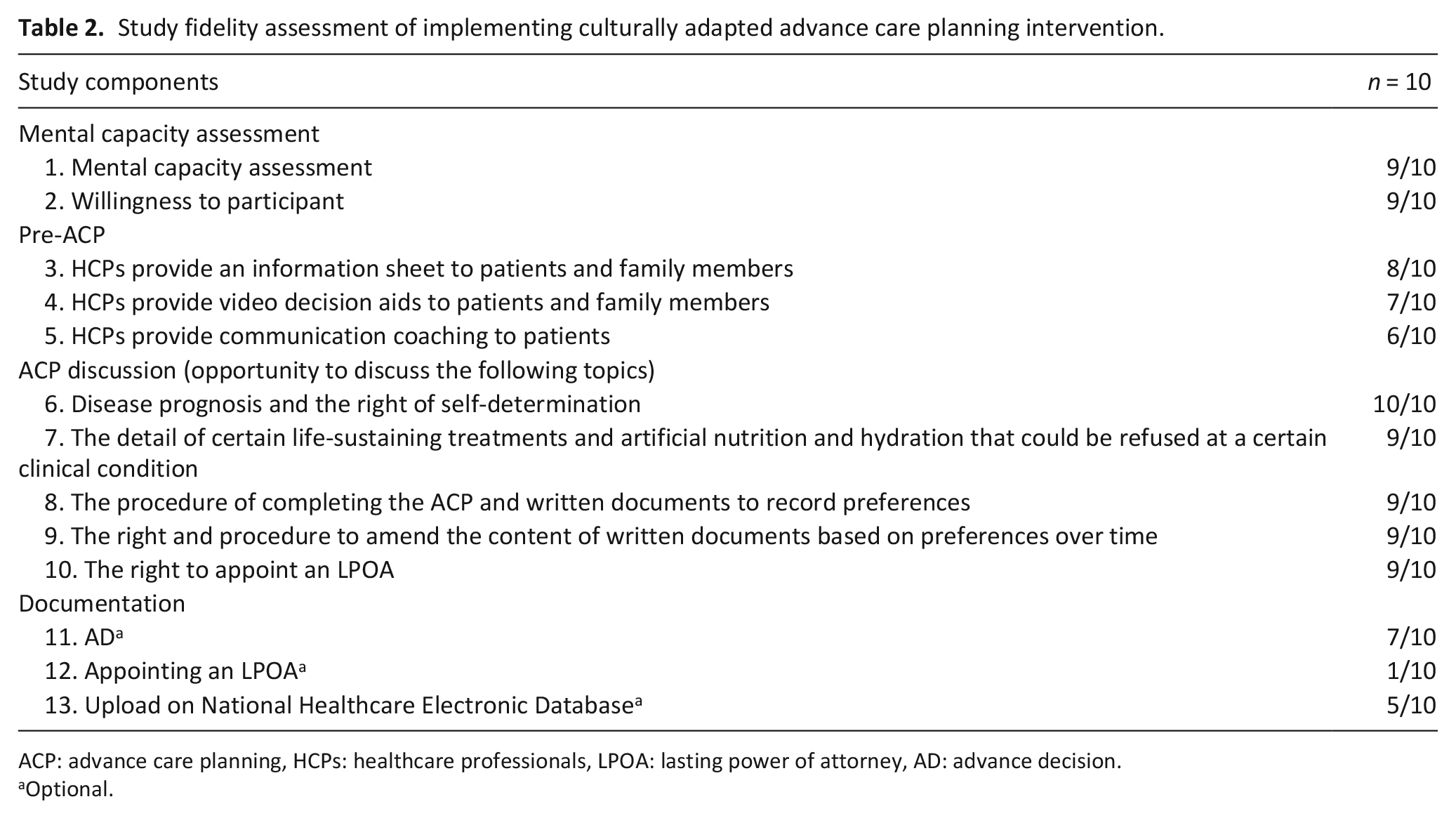
ACP: advance care planning, HCPs: healthcare professionals, LPOA: lasting power of attorney, AD: advance decision.
Optional.
Qualitative data: contextual moderators
Qualitative data were used to support the exploration of the feasibility of the advance care planning intervention. Four themes were identified that included as follows: (1) clinical situation and constraints; (2) knowledge and experiences; (3) healthcare system and environment; and (4) social expectation and norm.
Theme 1: clinical situation and constraints
Advance care planning was viewed as increasing staff workload in an already busy routine and additional resource was required to embed the intervention into clinical practice.
Advance care planning increased workload
Healthcare professionals reported that providing intervention to patients and their family members increased their clinical workload in an already very busy setting. They spoke of the tension between the limited time associated with their routine work and the requirement to deliver the intervention: In fact, our routine workload is already very busy and I (now) have to spend more time to do this [advance care planning]. I am actually in the dilemma of how long I should engage in the dialogue while at the same time I have to complete all my other daily assignments. (HCP08 hospice nurse)
Lack of supporting resources
The lack of adequate resources for implementing advance care planning was considered a barrier by healthcare professionals. This is best illustrated by a clinical psychologist who explained the importance of having adequate resources to deliver advance care planning to patients and family members: The reason why I think that we are not ready is all because of the [lack of] manpower and resources. (HCP04 clinical psychologist)
Theme 2: knowledge and experiences
This theme focused on the way in which participants’ previous knowledge and experience of end-of-life care influenced the advance care planning implementation.
Patients’ and family members’ value and experience about end-of-life care issues
Healthcare professionals suggested that possessing experience in taking care of cancer patients enabled them to be more willing to be involved in advance care planning discussions: The people who have ever taken care of this kind of [cancer] patients would know better about the dilemma and relevant issues patients might experience in the disease trajectory. They will be more willing to come for the [advance care planning] consultation. (HCP01 hospice nurse)
This statement was also supported by the sentiment from a son of a patient with ovarian cancer who recounted witnessing his mother’s suffering and that provoked him to respect her choice to refuse life-sustaining treatments within her advance care planning discussions: I accept it because I have looked after her [the patient] and seen how her suffering. I would only prolong [her death] if I insisted, she needed to receive the [life-sustaining] treatments. (FY06 son of an ovarian cancer woman)
However, advance care planning and advance decisions were not considered essential if patients were unable to foresee the prognosis of their illness. The lack of knowledge was considered to be a barrier: What I don’t know the most is that what will happen [disease progress] one year later? Will I need this [advance decision] to inform my treatment and care two years later? (PT01 lung cancer woman)
Theme 3: the healthcare system and environment
This theme depicts how the healthcare system influenced the viability of advance care planning both at the individual and organisational levels. Patients and family members considered that advance care planning participation could increase their financial burden as they need to pay an out-of-pocket fee for each advance care planning consultation. Moreover, the hospital policy support was key for the embedment of advance care planning in clinical practice.
The financial burden of advance care planning participation
The value of advance care planning to assist healthcare professionals to provide care in accordance with patients’ preferences was recognised. However, participants stated that this was unlikely to happen if the patients did not possess adequate financial resources to realise their preferred wishes: Of course, [advance care planning] lets the medical staff understand more about what the patient wants. However, [receiving preferred care] won’t happen if he can’t afford it. (HCP06 hospice nurse)
Organisational policy support
Introducing and embedding advance care planning intervention into clinical routine care required the support of policy at an organisational level and was considered imperative to make advance care planning delivery possible: Is [advance care planning] possible as part of routine care in the hospital? I think it really depends on the hospital’s policy support. (HCP01 hospice nurse)
Theme 4: social expectation and norm
The theme focused on the influence of traditional social norm regarding medical service provision and surrogate decision-making about a patient’s medical care option.
Medical care services were taken for granted by the public and high prevalence of surrogate decision-making by the medical team
Healthcare professionals reported that most of the healthcare service costs for cancer patients were covered by National Health Insurance in Taiwan so that patients and family members were reluctant to pay the out-of-pocket fee for advance care planning consultations. In addition, they believed that the medical team would make the best decisions on medical care in the future for them, resulting in the less willing to engage in advance care planning discussions: They [patients] are used to a system where the medical care is provided without an extra fee, and also believe in the medical team will make the best decision on behalf of them [patients]. (HCP01 hospice nurse)
Acceptability of intervention and advance care planning areas warranting for further refinement
Participants reported that the culturally adapted advance care planning intervention was acceptable and satisfactory. No adverse effects were reported from patients after participating in the intervention: It was necessary to have an advance care planning discussion as it helped me to understand my rights [of self-determination] and both sides [patients and medical staff] benefited. It’s good stuff. (PT10 lung cancer man) I think this kind of consultation [advance care planning] is good, and I don’t think it’s harmful. (PT01 lung cancer woman)
Six areas for further refinement of the advance care planning intervention were suggested and included (1) early initiation of end-of-life care discussion in the cancer trajectory; (2) enabling patients to make informed decisions; (3) documentation to guide future care and reduce patient and family distress; (4) simplifying the intervention to make less abstract and more acceptable; (5) managing conflict between patients and family members around advance care planning; and (6) concordance with preferred care provision.
Area 1: initiating an end-of-life care discussion in advance
Advance care planning was deemed to be a means to initiate the end-of-life care discussions and create opportunities to exchange understandings in advance between patients, family members and healthcare professionals about the patients’ disease prognosis and their future care preferences. Previously, these had not occurred. This sentiment was highlighted both by family members and healthcare professionals: Through the advance care planning discussion, opportunity, understanding and expression of opinions between patients and families can be achieved, that did not happen in the past. (FY08 son of a pancreatic cancer woman) I think that it [advance care planning] has started the discussion that we all hope to die well. I think this is a very good initiative. (HCP06 hospice nurse)
Area 2: enabling patients to make informed decisions
Disease prognosis was generally little discussed with patients due to the fear of depriving individuals of hope and contributing to anxiety and depression. Patients felt satisfied with being involved in advance care planning discussions and learning about their illness, its prognosis and possessing the right to self-determination about their future care: After the explanation by the doctor, I was clear that I had autonomy and I could inform my family in advance [about my preferences]. Otherwise, no one dared to make decisions for me at the end of my life. It is good to have such an [advance care planning] consultation. (PT01 lung cancer woman)
Area 3: documentation to guide future care and relieve patients’ and family members’ distress
Documenting care preferences after the advance care planning discussion were considered important to patients to guide future care. Moreover, patients and their family members suggested that they felt a palpable sense of relief as they engaged in considering previously unthinkable issues: I think [advance care planning] it’s good. It can be a proof that we had discussions. Although we might forget the content [advance care planning] and decisions, we had already discussed it [the patients’ care preferences] and signed [advance decision] so we follow this form to provide future care. (FY05 wife of a rectal cancer man) There was a heavy stone in my heart before completing the [advance decision] form. After signing [advance decision]. . .because I was able to explain my care preferences to the doctor, I felt relieved. (PT10 lung cancer man)
Physicians could communicate with other colleagues and family members and justify their decisions regarding the end-of-life care for patients according to the documentation: In my clinical practice if I encounter such a [end of life] situation I can reasonably state that the patient had discussed this [end of life care] issues with me before and made the decisions. Then I can also advocate for him and inform his family or other [medical] team members that these [care] is in accordance with the patient’s preferences. (HCP09 palliative care physician)
Area 4: simplifying the intervention to make less abstract and more acceptable
Healthcare professionals worried that the complex nature of the advance care planning intervention might compromise patients’ and their families’ acceptance of the consultation: I think public acceptance won’t be high. No one really understands this [advance care planning] because it is too complex. (HCP04 clinical psychologist)
This sentiment was echoed by a family member who was equally concerned that the perceived complexity of advance care planning would detract from understanding what was required by patients to realise its benefits: It may not be possible to explain it [advance care planning] clearly and comprehensively in a short time. I really feel that it’s difficult to realise it [in a short consultation]. (FY08 son of a pancreatic cancer woman)
Area 5: potential for advance care planning to provoke conflict between patients and family members
Even though advance care planning was able to initiate the early end-of-life care discussion, it was viewed by some as potentially be a source of conflicts between patients and their families. However, healthcare professionals believed this was more likely to be a result of relieving stress rather than a devastating interaction: If the treatment he expects is not the same as what the family expects, a conflict might arise. But I think this conflict is not necessarily a negative consequence. . .Because sometimes in our Chinese society, family members are considered to be supportive to each other, but behind this relationship, [there] is actually lots of pressure and stress for the patients and also for the caregivers. With such a relatively open [advance care planning] discussion, even if there will be a conflict, it has actually created opportunities for dialogue. (HCP03 social worker)
Area 6: concordance with preferred care provision
Healthcare professionals and patients reported that reaching an agreement between patient and those caring for them might be more of a challenge than the advance care planning discussions and documentation itself. Specifically, the trusting relationships between patients, family members and healthcare professionals were considered crucial for ensuring patients received care which aligned with their wishes and that also calmed family members: The most difficult issue is not about discussing the advance decision or the Do-Not-Resuscitation form. It’s the action after that discussion. How could you promise the patient that he can always receive care to relieve his discomfort from the symptoms? How his family members could be pacified from being panicked. I think this is the most challenging task. (HCP09 palliative care physician)
This was also corroborated by several cancer patient participants: The implementation [of advance decision], rather than the discussion, is actually the key. The interaction between the patient and the medical team that implementing [advance decision] in the future is extremely crucial. It takes time to overcome this challenge. (PT02 lymphoma woman)
Discussion
This is a novel study assessing the feasibility and acceptability of a culturally adapted advance care planning intervention and view about involvement in a study among people living with advanced cancer, their family members and healthcare professionals in Taiwan. The results suggested that introducing the culturally adapted advance care planning intervention into clinical practice in a tertiary inpatient hospital in Taiwan is possible. The participants reported the intervention as acceptable. However, the recruitment of patients with advanced cancer patients is challenging with both nearness to end of life and uncertainty about the value and benefit of palliative care and advance care planning in Taiwan. An optimal conceptual model integrating findings from the previously developed works6,21 is proposed, which highlights the contextual moderators, training requirements, intervention components, mechanism of action, potential outcome measures and areas for future intervention modification (Figure 4).
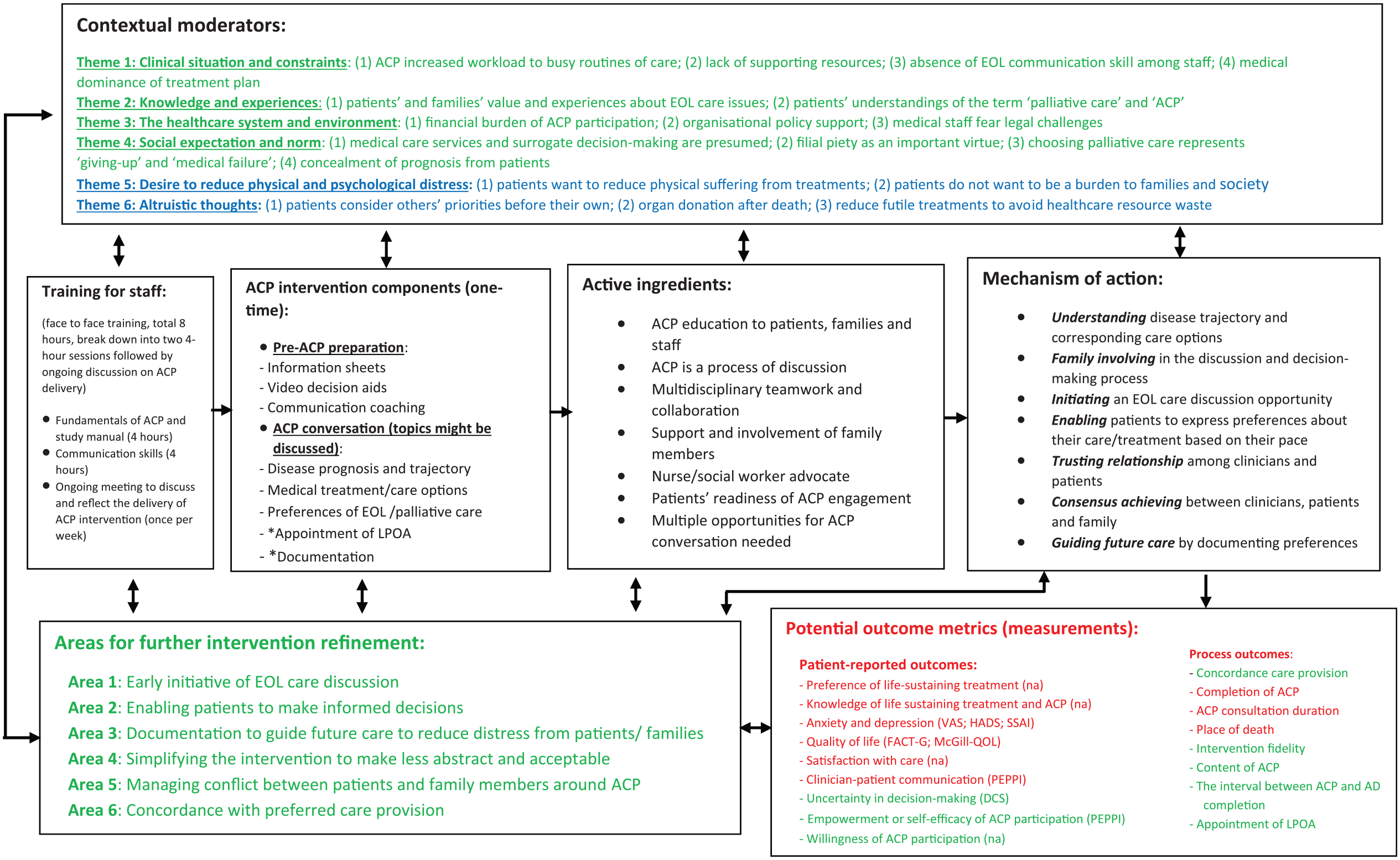
Conceptual model of culturally adapted advance care planning intervention for advanced cancer patients and their families in Taiwan.
In this study, we identified intervention components that shared similarities with the Western evidence (e.g. accessible information and communication coaching, and fostering shared decision-making between the clinician and patient). 6 However, four core components were identified requiring greater emphasis when delivering advance care planning in Taiwanese context, which include the following: (1) involving family members; (2) respecting of filial piety; (3) improving the patient’s understanding of palliative care; and (4) end-of-life care communication training for healthcare practitioners to facilitate open discussions with patients about their disease prognosis. Embedding advance care planning into routine care is a big shift in understanding and interpreting patient autonomy, which was unfamiliar for staff in Taiwan. When delivered by healthcare practitioners, the advance care planning process must include family members and respect filial responsibility while assisting the patient to make informed decisions. Advance care planning in Taiwan requires an emphasis on increasing the patient’s focus and accommodating this within the typical family-centric decision-making process. The use of advance care planning requires a cultural shift among clinicians (e.g. oncologists) and patients that this is not a medical failure, but beneficial to patients and their family. To ensure the success and sustainment of advance care planning in Taiwan, we identified six areas for future intervention refinement to facilitate the delivery of advance care planning in Taiwanese context.
The findings of this study highlight the possibility of implementing advance care planning specifically developed for advanced cancer patients and their family members in Taiwan and demonstrate high compliance with the intervention protocol and evaluation. With the exception of a few components (e.g. component 12: appointing a lasting power of attorney), the majority components of advance care planning intervention were successfully delivered. Discussing care options with surrogate decision-makers (often family members or patient’s close friends) and assisting patients to appoint a medical surrogate could potentially benefit both the patients (e.g. receiving concordance care) and the surrogates (e.g. reduce distress on substitute decision-making).30–32 However, the lasting power of attorney (surrogates for decisions about health care and treatment should the person lose the capacity to decide for themselves) 17 appointment rate in our study was low (n = 1/10, 10%) when compared to Detering et al.’s 30 research (n = 56/154, 36%). This might be explained by (1) the small sample recruited; (2) patients believed that physicians or family members would make the best decisions for them (contextual moderator – theme 4), therefore it was not necessary to officially appoint a surrogate; (3) the surrogates were not psychologically ready to play this role;31–33 (4) the patient’s preferences and views change over time; 14 and (5) a misunderstanding of the legal framework regarding advance care planning among stakeholders (e.g. patients, family members and healthcare professionals). 14 Advocating for the importance of appointing medical surrogate and preparing the patients and their family for complex decision-making are imperative.
Michael et al.’s 34 research supported the findings that advance care planning intervention motivates participants to think ahead and that it is beneficial. However, the findings from this study identified that it might precipitate conflict between patients and family members if they have different expectations about prognosis and future care plan. This highlighted again the requirement for family involvement and high-quality end-of-life communication provision by staff during advance care planning discussions as key culturally adapted emphasis in Taiwanese context. Structured and standardised guidance for communication training, particularly regarding truth-telling should be in place, has been reported to improve end-of-life communication between serious illness patients and staff.35,36
Several moderators were not identified from our study and included: (1) not feeling ready or interested in advance care planning; (2) considering the existing care plan to be sufficient; and (3) patients’ lives consumed with dealing with the present and their illness. 34 These moderators were considered very influential and hampered the further post of advance care planning, which should also be explored in future studies.
The difficulty of recruitment of studies like this for this type of patient population is not uncommon.37,38 The following concerns need to be considered for better recruitment: (1) referral from the lead clinical care team, for example, oncologists; (2) the time allocated to staff to successfully promote and deliver advance care planning; (3) many patients experienced advanced disease stage and lacked the capacity to engage in advance care planning discussion; (4) engaging in advance care planning for patients and families incurred a financial burden; and (5) Taiwanese people were unfamiliar with advance care planning and exercising their right of self-determination. Strategies to tackle these issues represent areas for further optimisation to refine the advance care planning intervention for this context include the importance of early intervention of education to patients, family members and clinical staff, most importantly, the general public, to arouse their awareness, motivation and competence of advance care planning participation.6,8,39,40 In addition, seeking an organisation’s support and securing funding for advance care planning implementation are crucial to redress the resource and absence of adequate staff labour suggested by international Delphi consensus works conducted in North America 1 and Europe. 2
We identify key areas for further refinement of the advance care planning model for better implementation and could be used to inform the potential outcome measures to evaluate advance care planning intervention. Several measures have been developed to examine the patients’ behaviour change 41 and their engagement 42 in advance care planning. However, measurements to examine the complexity of advance care planning, the conflict between patients and family members and concordance with preferred care provision are currently absent. 43 The development of reliable and validated measurements that include these issues should be a future research priority.
To improve the access of palliative care to diverse populations and facilitate patient autonomy in end-of-life care, the Patient Right to Autonomy Act 17 was adopted in 2016 in Taiwan and took effect in January 2019. The aim of the Patient Right to Autonomy Act is to emphasise an individual’s autonomy in medical decision-making and give the written documents (advance decisions) a legally binding nature. By doing so, the patient’s decisions in terms of future care, particularly related to end-of-life, could be known by families and healthcare professionals and archived on the government’s healthcare system (National Health Insurance system) and are safe from interference by others, including family members. Thus, the uncertainty of the end-of-life or palliative care for patients would be minimised. This demonstrated how the legislation drove the change of clinical practice, systematic training for staff and public awareness of end-of-life care decision-making in Taiwan. A notable element was that a multidisciplinary team comprising a physician, a nurse and a social worker or psychologist was required for advance care planning delivery based on local legislation. 17 The adoption of new legislation will have applicability for others when attempting to introduce legislation (guidance) or advance care planning intervention in the wider Asia-Pacific region.
Strengths and limitations
This study has several strengths: first, this study was underpinned by work developing the advance care planning intervention that informed the initial logic model,6,21 and refined through stakeholder consultation; second, we adopted multiple data sources (qualitative data from different groups and quantitative data) in a comprehensive approach to improve the trustworthiness and validity of the findings; 44 and third, discussions with different academics (C.J.E., J.K. and R.H.) and clinical experts (P.-J.C. and M.-F.H.) were sought to address the systematic bias from a single interviewer (C.-P.L.). 44 There are, however, several limitations that require caution when considering the study’s findings: first, although the sample size of the participants from each group is small, sample size and relevant parameter calculations were not the intentions of this study using a feasibility approach.19,45 The purpose was to recruit an adequate number of participants to obtain sufficient views to culturally adapt the advance care planning intervention and learn about the conduct of the study; second, the study design of delivering a one-time advance care planning intervention to patients and their family members could not examine the change in patients’ decision-making over time; third, the healthcare staff knew the researcher (C.-P.L.) and contributed to the intervention refinement and implementation. This may have influenced their willingness to criticise the intervention and overestimated the study fidelity; and fourth, the difference in languages used in this study might threaten the insight and meaning of the participants. However, we performed a rigour ‘forward and backward translation’ for all the themes and coding frames by bilingual researchers in palliative care (C.-P.L. and P.-J.C.) to address this issue. 46
Conclusion
Introducing the proposed culturally adapted advance care planning intervention for people living with advanced cancer and their family members in an inpatient hospital setting in Taiwan is possible. The study participants considered the intervention to be acceptable. However, recruitment of patients with advanced cancer is challenging with both nearness to end of life and uncertainty about the perceived value and benefit of palliative care and advance care planning in Taiwan. An integrated conceptual model proposed a potentially optimal process of advance care planning delivery, contextual moderators, its potential metrics and areas for further intervention refinement. This model should be considered for a nuanced approach to advance care planning for this population in Taiwan and more widely across the wider Asia-Pacific region. However, the difficulty of recruiting people with advanced cancer remains a challenge. Further research to improve recruitment strategies and test this model in a full feasibility trial is required.
Footnotes
Acknowledgements
The authors thank all the healthcare staff at Xin-Yuan hospice and palliative care unit in Kaohsiung Medical University Hospital, Taiwan, who implemented the culturally adapted advance care planning intervention to advanced cancer patients and their family members, and allowing the research team to collect data for this study. Besides, the authors appreciated all the patient and family participants for sharing their experiences.
Author contributions
C.-P.L., C.J.E., J.K., P.-J.C. and R.H. contributed in the conceptualisation of the study. C.-P.L. carried out the data curation. C.-P.L., C.J.E., J.K., P.-J.C. and R.H. developed the methodology for the study. C.-P.L., C.J.E., J.K., P.-J.C. and R.H. presented the data analysis and interpretation. C.-P.L. and P.-J.C. involved in the translation of the themes, coding and quotes. C.-P.L., P.-J.C. and M.-F.H. contributed to the project administration. C.J.E., J.K. and R.H. involved in the supervision of the study. C.-P.L., C.J.E., J.K. and R.H. contributed to writing and drafting of the manuscript. C.-P.L., C.J.E., J.K., P.-J.C., M.-F.H. and R.H. contributed to writing, reviewing and editing of the manuscript.
Availability of data and material
All the relevant data are available. The method of data collection and analysis is reported in this article. The sample characteristics and interview topic guides can be found in additional files in the supplementary materials.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval and consent to participate
The description regarding ethics approval is reported in this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: C.-P. L. was provided CLAHRC South London Thesis Write Up grant by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care South London at King’s College Hospital NHS Foundation Trust. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. C.J.E. was provided HEE/NIHR Senior Clinical Lectureship. The views and opinions expressed by the authors in this publication are those of the authors and do not necessarily reflect those of the National Health Service, the Health Education England or the National Institute of Health Research, Medical Research Council.