
Abstract
Background:
Avoiding inappropriate care transition and enabling people with chronic diseases to die at home have become important health policy issues. Availability of palliative home care services may be related to dying at home.
Aim:
After controlling for the presence of hospital beds and primary care physicians, we examined the association between availability of home palliative care services and dying at home in conditions requiring such services.
Design:
Death certificate data in Japan in 2016 were linked with regional healthcare statistics.
Setting/participants:
All adults (18 years or older) who died from conditions needing palliative care in 2016 in Japan were included.
Results:
There were 922,756 persons included for analysis. Malignant neoplasm (37.4%) accounted for most decedents, followed by heart disease including cerebrovascular disease (31.4%), respiratory disease (14.7%) and dementia/Alzheimer’s disease/senility (11.5%). Of decedents, 20.8% died at home or in a nursing home and 79.2% died outside home (hospital/geriatric intermediate care facility). Death at home was more likely in health regions with fewer hospital beds and more primary care physicians, in total and per condition needing palliative care. Number of home palliative care services was negatively associated with death at home. The adjustment for home palliative care services disappeared in heart disease including cerebrovascular disease and reversed in respiratory disease.
Conclusion:
Specialised home palliative care services may be suboptimal, and primary care services may serve as a key access point in providing baseline palliative care to people with conditions needing palliative care. Therefore, primary care services should aim to enhance their palliative care workforce.
Most people prefer to die at home but the majority die in hospital.
Place of death is influenced by level of local healthcare availability.
Use of home palliative care services decreases visits to emergency department and hospital admission at the end of life.
Availability of home palliative care services was negatively associated with death at one’s own or a nursing home.
The adjustment for home palliative care services disappeared in heart disease including cerebrovascular disease and reversed in respiratory disease.
Availability of primary care physicians was related to greater likelihood of death at home in total and per condition needing palliative care.
Specialised home palliative care services may be suboptimal for the large population with conditions needing palliative care.
The palliative care workforce should be enhanced as a part of primary care services.
Introduction
Enabling people with chronic diseases to die at home has become an important health policy issue worldwide. As people are living to older ages, more of them are living with the effects of serious chronic illness towards the end of life. These people require palliative care, including care planning regarding the location in which they wish to die. 1 Most people would prefer to die at home,2,3 but the majority die in hospital.4,5 Hospital end-of-life care could be of lower quality, due to a wide range of factors including potentially burdensome and inappropriate hospital admissions, as well as aggressive treatments shortly before death.6,7 The use of non-beneficial treatments is widespread in acute hospitals at the end of life. 8 Therefore, palliative care policies have been introduced that are meant to make palliative and end-of-life care available for people with a wide range of chronic diseases at their usual place of residence.
Place of death is influenced by level of local healthcare availability. 9 The risk of in-hospital death is increased for residents of regions with greater hospital beds,10–12 smaller nursing home beds10,11 and less general practitioner availability. 11 Availability of palliative home care services may be related to the feasibility of dying at home. Home palliative care services are usually provided by a multidisciplinary team to terminally ill patients at their own home or nursing homes. The use of home palliative care services decreases visits to emergency department 13 and hospital admission at the end of life.14–17 Cancer patients who reside in a region with a palliative home care team are less likely to die in hospitals. 18
Japan is currently facing a super-ageing society, resulting in an urgent need to address increasing end-of-life and palliative care needs. 19 Unlike in western countries, Japan’s healthcare insurance programme covered palliative care only for inpatients in hospital care units until April 2006, when home end-of-life care clinics were introduced, providing home palliative care to people with advanced illnesses.20,21 Despite offering higher quality end-of-life care than inpatient palliative care units, home palliative care remains uncommon in Japan. 22 However, no population-level examination has been performed on the association between dying at home in conditions needing palliative care and availability of home palliative care services, after adjusting for availability of hospital beds and primary care physicians. Knowledge of the reality at the population level would offer health policy implications that could help people who need palliative care to die at home when that is their wish. The results of such research may even have implications for international palliative care policy, helping to address an escalating global need for palliative care. 23
This study examined the rate of death at home in conditions needing palliative care in relation to healthcare availability in the Japanese context. We hypothesised that greater availability of home palliative care services is significantly associated with higher death rates at home, even after controlling for availability of hospital beds and primary care physicians.
Methods
Study design
The study analysed data from death certificates, provided by the national mortality database of Japan. A detailed description of these data has been given elsewhere. 24 Data regarding deaths of Japanese residents aged 18 years or older were extracted from data regarding deaths that occurred in Japan between January and December 2016.
Data source
Data regarding the underlying cause of death were obtained from death certificates using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes. In Japan, death certificates are completed by a medical doctor within 7 days of death, and the underlying cause of death is identified.
Identification of conditions needing palliative care
Conditions needing palliative care were identified based on the underlying cause of death using the ICD-10 codes; they were malignant neoplasm, heart disease including cerebrovascular disease, renal disease, liver disease, respiratory disease, neurodegenerative diseases, dementia/Alzheimer’s disease/senility and HIV/AIDS (Supplementary Appendix 1). This is based on a well-established method for estimating palliative care need from death certificate data.12,25,26 The conditions selected are specific chronic diseases that are likely to involve complex physical, psychological, social and/or spiritual problems that can be improved by either specialist or generalist palliative care services.
Since renal disease, liver disease, neurodegenerative disease and HIV/AIDS accounted for less than 5% of deaths from conditions needing palliative care, they were grouped as ‘other conditions needing palliative care’ in the analysis.
Decedents
In total, 1,314,665 deaths were registered in Japan between January and December 2016, of which 1,314,356 involved Japanese residents. In addition, 1,309,813 deaths (99.7% of 1,314,356) occurred in people aged 18 years or older. Of the 1,309,813 adult decedents who had been resident in Japan, 1,003,331 (76.6%) died due to a condition needing palliative care.
Classification of place of death
Place of death was classified into the following categories on the death certificates: ‘hospital’, ‘intermediate geriatric care facility’ (rehabilitation facility aimed at home discharge), ‘nursing home’, ‘own home’, or ‘other place, unspecified’.
‘Nursing homes’ included special nursing homes and fee-based homes for elderly people; the former are the only facilities that provide permanent residence under long-term care insurance residential services, while the latter include housing facilities provided in accordance with the Public Aid for the Aged Act, which offer additional care and are comparable to assisted living in the United States and extra-care housing in England. Decedents’ own homes included group homes.
Places of death that were classified as ‘other place, unspecified’ were excluded from the analysis.
For our analysis, death at ‘own home’ (including group homes) or ‘nursing home’ was recoded as ‘death at home’. We included nursing home deaths because nursing homes in Japan are a common place of residence for older adults who require regular personal assistance but do not have acute or heavy healthcare needs. Death at hospital or geriatric intermediate care facility was recoded as ‘death outside home’.
Home end-of-life care clinics
Availability of home palliative care services was measured as the number of home end-of-life care clinics per 1000 inhabitants in health region. Home end-of-life care clinics were introduced into public healthcare insurance in April 2006 to provide medical and nursing care to people with advanced illnesses.20,21 Home care support clinics provide home visits upon request of patients as well as outpatient services.
Independent variables
The independent variables included individual characteristics, underlying cause of death and regional measures of healthcare availability. Information regarding sex, age at death, marital status, working status and municipality of residence was obtained from death certificate data.
Municipality of residence was used to link the death certificate data with regional measures of healthcare availability. Healthcare availability consisted of the number of home end-of-life care clinics per 1000 inhabitants, available hospital beds per 1000 inhabitants, primary care physicians per 1000 inhabitants, available special nursing home beds per 1000 inhabitants aged 65 years or older and available fee-based home beds per 1000 inhabitants aged 65 years or older. Regional data were obtained by summing the municipal data for each of the variables (Supplementary Appendix 2). The prefectural government allocates healthcare resources based on health regions (called ‘the secondary tier of medical care’), which usually include multiple municipalities.
Availability of primary care physicians was measured as the number of physicians working mainly at clinics per 1000 inhabitants in the health region. Japan does not have a general practitioner registration system that is generally accessible to any physician or hospital.
Statistical analysis
Percentages of deaths by place of death were calculated per the total population and per condition needing palliative care.
A multilevel binomial logistic regression analysis was employed using death at home versus outside home as an independent variable and availability of home palliative care services as dependent variable. Underlying cause of death, individual characteristics and healthcare availability were included as covariates. To examine whether availability of home palliative care services was consistently associated with dying at home across underlying causes of death, a stratified analysis was performed per condition needing palliative care (malignant neoplasm, heart disease including cerebrovascular disease, respiratory disease or dementia/Alzheimer’s disease/senility). The logistic regression model included ‘health region’ as a random effect, to account for correlations between decedents within a health region.
All statistical analyses were performed using Stata SE for Windows, version 15.1 (Stata Corp, College Station, Texas, USA). The two-tailed significance level was set at 0.05.
Results
Death caused by conditions needing palliative care
Of the 1,003,331 adult decedents due to a condition needing palliative care, 13,040 were classified as having occurred at ‘other place, unspecified’ and were excluded from the analysis. Of the remaining 990,291, there were 67,535 that lacked information regarding nationality (n = 566), marital status (n = 586), working status (n = 66,146) or municipality of residence (n = 237). The final sample included in the analysis consisted of 922,756 decedents (93.2% of 990,291).
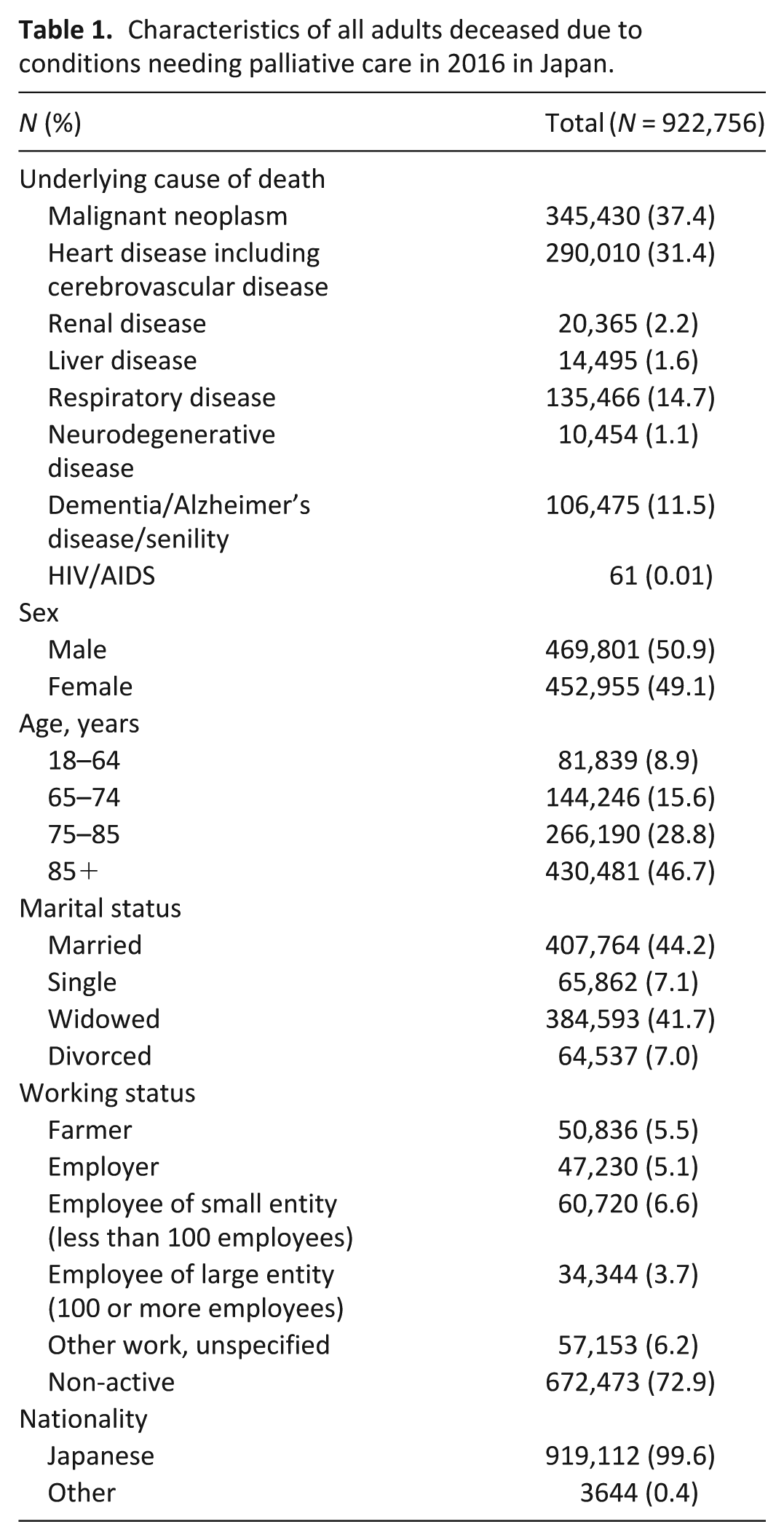
Malignant neoplasm (37.4%) and heart disease including cerebrovascular disease (31.4%) accounted for most deaths from conditions needing palliative care. During the entire study period, 50.9% of 922,756 adult decedents were men, with a mean age at death of 81.4 years. In addition, 41.7% of decedents were widowed at death and 72.9% were of non-active working status (Table 1).
Characteristics of all adults deceased due to conditions needing palliative care in 2016 in Japan.
Trends regarding place of death
Hospital was the most common place of death from conditions needing palliative care (76.5%), followed by own home (12.8%), nursing home (8.0%) and geriatric intermediate care facility (2.7%). More than 80% of decedents with respiratory disease, malignant neoplasm and other conditions needing palliative care died at hospital. Less than half of decedents with dementia died at hospital (Table 2).
Place of death due to conditions needing palliative care in 2016 in Japan.
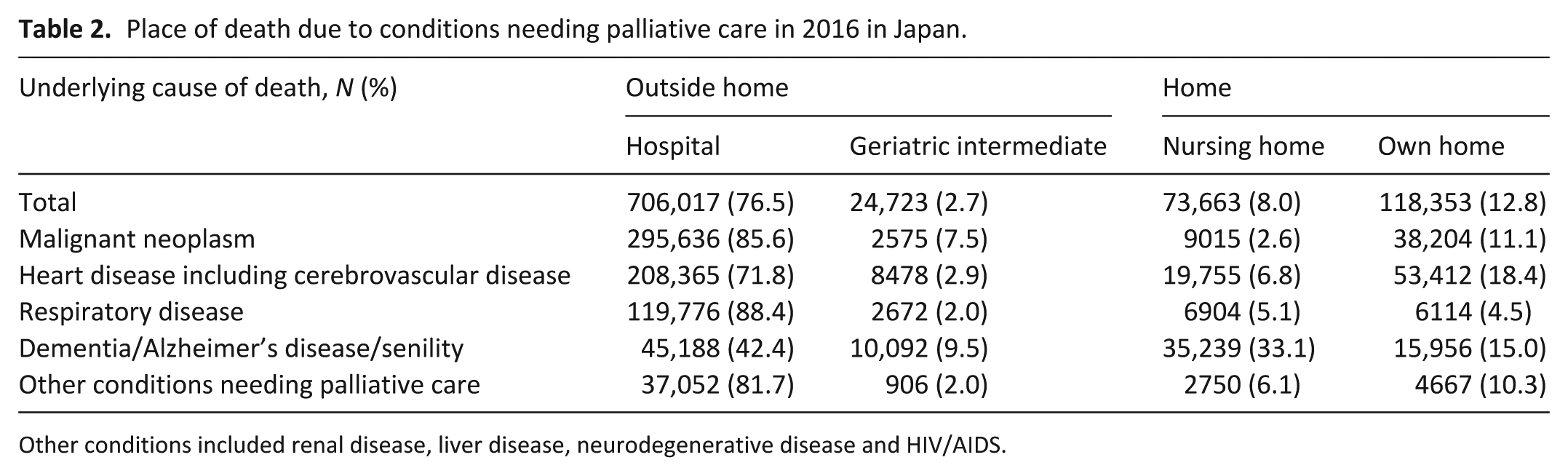
Other conditions included renal disease, liver disease, neurodegenerative disease and HIV/AIDS.
Home palliative care and other healthcare availability
There were 14,683 home end-of-life care clinics in Japan in March 2016, accounting for 14.5% of all 101,529 medical clinics. Availability of home palliative care services was 0.11 per 1000 inhabitants on average.
There were 0.80 primary care physicians and 9.09 hospital beds per 1000 inhabitants, and 15.77 special nursing home beds and 12.53 fee-based home beds per 1000 older inhabitants.
Factors associated with death at home
Multilevel binomial logistic analysis showed associations between death at home and smaller number of home palliative care services, greater number of primary care physicians, smaller number of hospital beds and/or greater number of nursing home beds. The strongest associations with place of death concerned underlying cause of death and availability of primary care physicians (Table 3).
Death at own or nursing home due to conditions needing palliative care.
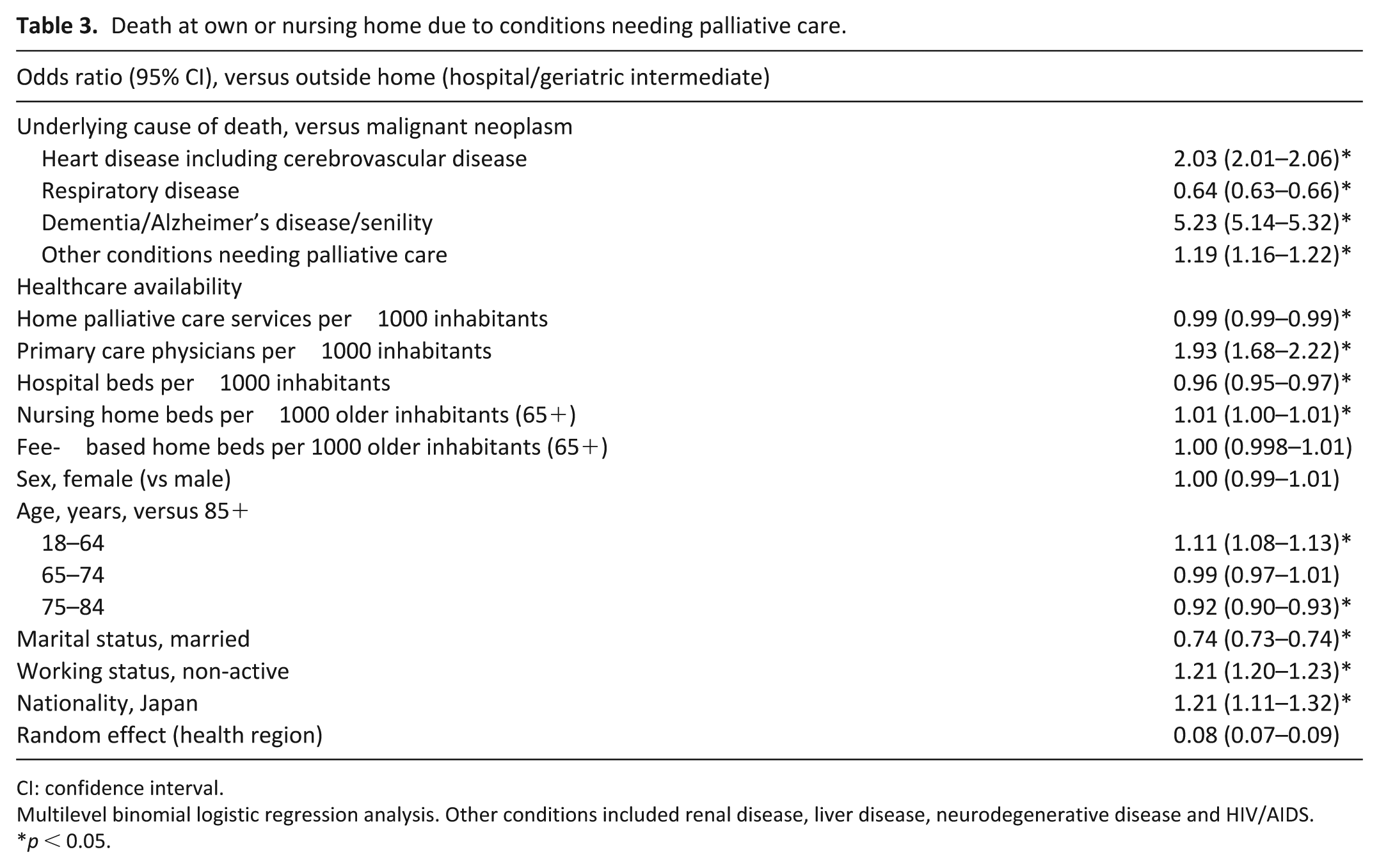
CI: confidence interval.
Multilevel binomial logistic regression analysis. Other conditions included renal disease, liver disease, neurodegenerative disease and HIV/AIDS.
p < 0.05.
The stratified analysis per underlying cause of death endorsed associations between place of death and availability of primary care physicians and hospital beds. Availability of home palliative care services was significantly associated with less likelihood of death at usual place of residence for malignant neoplasm or dementia/Alzheimer’s disease/senility. However, the adjustment for home palliative care services disappeared for heart disease including cerebrovascular disease and was reversed in respiratory disease (Table 4).
Death at own or nursing home per condition needing palliative care.
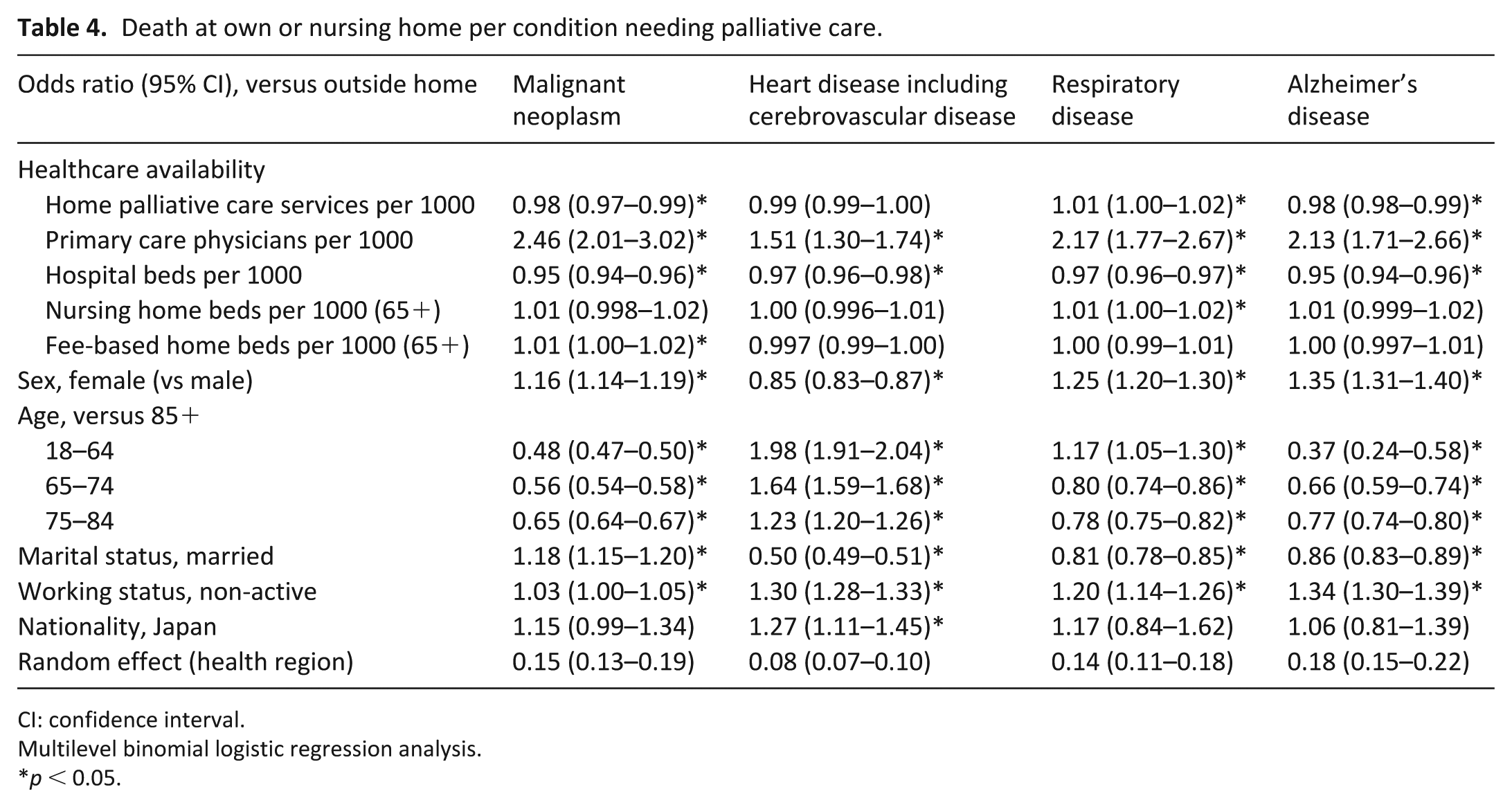
CI: confidence interval.
Multilevel binomial logistic regression analysis.
p < 0.05.
Discussion
Main findings/results of the study
About three-quarters of all deaths in Japan (77%) are caused by conditions that would benefit from the provision of palliative care. Malignant neoplasm (37%) and heart disease including cerebrovascular disease (31%) accounted for the most deaths from conditions needing palliative care. Hospital death was common (77%) across all conditions needing palliative care. Availability of home palliative care services was negatively associated with death at own or nursing home. Death at home was more likely to occur for those who had resided in a health region with smaller number of hospital beds and/or greater number of primary care physicians per 1000 inhabitants.
Conditions needing palliative care
The estimated need for palliative care in Japan was found to be similar to figures in countries such as England (63%), 25 Portugal (71%) 12 and Ireland (80%). 27 Malignant neoplasm was the most common underlying cause of deaths from conditions needing palliative care, but still less than in a study of 14 other countries (where it ranged from 52% to 83%). 25 Given the rapidly ageing Japanese population, considerable palliative care need will continue to exist in relation to deaths from non-malignant as well as malignant conditions.
Most deaths from conditions needing palliative care in Japan occur in hospital – more than in Portugal (62%), 12 or several other countries in Europe (25%–66%) and the United States (38%–61%). 28 Hospital death was particularly common with respiratory disease (88%) and malignant neoplasm (86%), although somewhat different to findings from 14 countries that showed a greater likelihood of home death in chronic obstructive pulmonary disease compared to lung cancer. 29 Cultural issues may play a role in the frequency of hospital death in Japan – while the general public prefer to die at home in Japan30,31 as well as European countries, 32 Japanese palliative care physicians were less likely to regard dying at home as important. 33 In addition, the general public assumes that death at home is rare, regardless of their own wishes, because of increasing care burden for family members. 34 The desire to avoid burdening one’s family could have increased end-of-life hospital admissions in Japan.
Availability of home palliative care services
Contrary to our hypothesis, availability of home palliative care services was negatively associated with dying at home from conditions needing palliative care. This adjustment for home palliative care services disappeared in heart disease including cerebrovascular disease and was reversed in respiratory disease. The difference between causes of death may reflect diverse illness trajectories between terminal illness (malignant neoplasm), frailty (dementia) and organ failure (respiratory disease).35,36 The weak and mixed associations between dying at home and home palliative care services will likely have been caused by ineffective referral systems and limited access to home end-of-life care clinics in Japan. Home end-of-life care clinics usually start support for patients discharged from acute hospital with referral, 37 and patients with terminal illness or frailty may be referred back to the hospital at the end of life. Home death accounted for only 6%–7% of patients who received care from home end-of-life care clinics. 38 The capacity of specialised home palliative care services may be suboptimal for the large population with conditions needing palliative care in Japan. Early palliative care referral (>3 months before death) was associated with fewer emergency-room visits, hospitalisations and hospital deaths in the last 30 days of life. 39 However, home end-of-life care clinics were used for an average of 2 months, suggesting late referrals to these clinics. 22
Notably, effects of availability of home palliative care services were smaller than those of availability of primary care physicians and hospital beds. Availability of primary care physicians was consistently associated with dying at home overall and per condition needing palliative care. Primary care services may serve as a key access point to provide a baseline palliative care approach to people with conditions needing palliative care. In particular, palliative care offerings as part of primary care services would benefit continuity of care. However, availability of primary care physicians did not necessarily result in those physicians regularly following all older adults in the region. This study also lacked structural data on palliative care practices, meaning we could not determine how patients were identified for home palliative care and whether they were risk-stratified. Future research should evaluate intensity of services provided, as well as adherence to quality standards for end-of-life care, among both home clinics and primary care services.
Strengths and weaknesses/limitations of the study
A major strength of our study lies in the examination of the association between regional availability of home palliative care services and place of death based on population data. Other strengths include generalisability across various conditions needing palliative care due to use of national data, broadly representative of the Japanese population. This study has taken the first crucial step towards the identification of priorities in national palliative care strategies. Primary care services should increase the workforce responsible for palliative care. Possible strategies include establishing training platforms for non-palliative care clinicians and dissemination of palliative care education for primary care teams, such as the End-of-Life Nursing Education Consortium (ELNEC) training programme 40 and the Center to Advance Palliative Care 41 in the United States.
However, our cross-sectional study design meant that a causal model between place of death and availability of home palliative care services could not be developed. In addition, the data from death certificates did not provide detailed information regarding changes in place of care when close to death, nor could in-hospital deaths of long-stay patients be distinguished from hospital transfers of dying residents from their own or nursing homes. We note that availability of home end-of-life care clinics did not necessarily reflect capacity of palliative care practices, as we lacked data on the number of physicians and patients in those clinics. We also did not have information on availability of informal care and deprivation index, both related to elevated risk of hospital deaths.12,42
What this study adds
Our study is the first to examine the association between regional availability of home palliative care services and place of death based on population data. The results imply that specialised home palliative care services may not adequately enable a growing palliative population to die at home. This may also apply to other aged countries with high need for palliative care. Addressing such needs will be an important starting point for tackling the increasing palliative care needs worldwide, especially in low- and middle-income countries. 23
Conclusion
Availability of home palliative care services was negatively associated with dying at home from conditions needing palliative care in Japan, although this adjustment for home palliative care services disappeared or reversed for some conditions. Availability of primary healthcare services was consistently associated with dying at home overall and per condition needing palliative care. Overall, to better provide for people with conditions requiring palliative care, primary care services should aim to increase the dedicated workforce that focuses on such individuals.
Supplemental Material
PMJ-19-0043Supple – Supplemental material for Availability of home palliative care services and dying at home in conditions needing palliative care: A population-based death certificate study
Supplemental material, PMJ-19-0043Supple for Availability of home palliative care services and dying at home in conditions needing palliative care: A population-based death certificate study by Miharu Nakanishi, Asao Ogawa and Atsushi Nishida in Palliative Medicine
Footnotes
Acknowledgements
The authors thank the Japanese Ministry of Health, Labour and Welfare for its permission to analyse and support in the analysis of national death certificate data.
Authorship
M.N. is principal investigator and conceived the study with A.O. and A.N. M.N. negotiated data access with the Ministry of Health, Labour and Welfare. M.N. and A.N. analysed the data and interpreted the results together with A.O. Finally, M.N. drafted the manuscript, and all authors read and approved the final manuscript.
Data availability
This study was based on the Japanese national death certificate data. The authors do not own these data and hence are not permitted to share them in the original form (only in aggregate form, for example, in research publications). All death certificate data are owned and maintained by the Japanese Ministry of Health, Labour and Welfare.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics and consent
The study was approved by the ethics review board at the Tokyo Metropolitan Institute of Medical Science (15-4), and the procedures were performed in accordance with the Declaration of Helsinki of 1975, as revised in 2013.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the JSPS KAKENHI through a Grant-in-Aid for Young Scientists (B), Grant Number JP15K20796; by the Japan Agency for Medical Research and Development, Research and Development Grants for Dementia, Grant Number 16dk0207024h0001; and by the Ministry of Health, Labour Sciences Research Grant (Grant Number 19189431) supported by the Ministry of Health, Labour and Welfare. The funding sources had no role in the study design; data collection, analysis or interpretation; or writing the report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.