
Abstract
Background:
People of Black and minority ethnic heritage are more likely to die receiving life supporting measures and less likely to die at home. End-of-life care decision making often involves adult children as advance care planning is uncommon in these communities. Physicians report family distress as being a major factor in continuing with futile care.
Aim:
To develop a deeper understanding of the perspectives of elders of Black and minority ethnic heritage and their children, about end-of-life conversations that take place within the family, using a meta-ethnographic approach
Design:
Systematic interpretive exploration using the process of meta-ethnography was utilised.
Data sources:
CINAHL, MEDLINE, PubMed and PsycINFO databases were searched. Inclusion criteria included studies published between 2005 and 2019 and studies of conversations between ethnic minority elders and family about end-of-life care. Citation snowballing was used to ensure all appropriate references were identified. A total of 13 studies met the inclusion criteria and required quality level using Critical Appraisal Skills Programme.
Results:
The following four storylines were constructed: ‘My family will carry out everything for me; it is trust’; ‘No Mum, don’t talk like that’; ‘I leave it in God’s hands’; and ‘Who’s going to look after us?’ The synthesis reflected the dichotomous balance of trust and burden avoidance that characterises the perspectives of Black and minority ethnic elders to end-of-life care planning with their children.
Keywords
Conversations around treatment decisions near the end of life are distressing for both health care professionals and families.
Physicians avoid discussions about limiting treatments at end of life due to the distress; this has been found to be exacerbated in families of Black and minority ethnic heritage.
Adult children play a major role as end-of-life decisions makers for their parents of Black and minority ethnic heritage. However, few adult children have had conversations with their parents about end-of-life preferences.
Elders of Black and minority ethnic heritage avoid end-of-life planning conversations with their children to protect them from distressing conversations.
Adult children block attempts by their parents to have end-of-life conversations with them.
Elders of Black and minority ethnic heritage express a preference for end-of-life decisions to be made by family proxies acknowledging that these decisions may not reflect their own preferences.
Focus is needed on the role played by adult children about their perspectives on having end-of-life conversations with their parents. This could lead the way for innovative community engagement in the development of public health palliative care that may result in more effective end-of-life care planning and engagement with palliative care provision.
Introduction
Conversations around treatment decisions near the end of life are distressing for both health care professionals and families.1,2 In Western societies, autonomous decision-making models for health matters are favoured. However, at the end of life, without early conversations having taken place, decision making is often left to family members, many of whom have little awareness of the preferences of the older person who is now dying. 3 In situations involving people of Black and minority ethnic heritage, formal end-of-life planning has been found to be low.4,5 The aim of this synthesis is to develop a better understanding of the experiences and preferences of elders of Black and minority ethnic heritage and their children around end-of-life care conversations within their families. This may inform ways of facilitating earlier family-based conversations around illness progression and potential outcomes and perhaps provide a first step towards improving the difficult conversations that need to happen when someone is dying. 6
Background
Impact of conversations on decision making at end of life
Many people receive treatments that do not prolong life nor provide a relief from suffering so are considered to be non-beneficial or futile in the last 6 months of their lives. 4 While improving the quality of the dying experience is an issue that is faced by all communities, people of Black and minority ethnic heritage are more likely to die receiving life supporting measures 5 and least likely to die at home. 7 One of the main drivers leading to the instigation of futile treatments is families’ insistence.8,9 The difficulties clinicians have in conducting potentially distressing conversations with Black and minority ethnic families about limiting treatment is often a deterrent to engaging in them at all. 9 Research with people of Black and minority ethnic heritage illustrate poor communication between health care professionals and families, and a lack of culturally competent end-of-life skills among these professionals when dealing with matters at the end of life. 10
In part, difficult conversations at the end of life arise when family conversations about the end-of-life wishes of the dying person have not taken place and cannot now be elucidated due to their deteriorating condition. 2 Many older people feel they do not need to discuss their end-of-life preferences with their families because their children will know what they would want.1,11 In general, older people do not want to live a long lingering existence and White majority populations find doing some kind of advance care planning is a comfort. 11 However with people of Black and minority ethnic heritage, discussing dying is thought to be taboo more often than in the White majority population which results in much lower levels of evidence of end-of-life family conversations.8,11,12 These geographical differences in the way communities discuss dying are illustrated and explored in some recent studies which show greater levels of end-of-life planning conversations taking place in societies that favour autonomous models of decision making over more collective societal and family-based decision-making norms.13–15
Research exploring end-of-life conversations and decision making in a variety of Black and minority ethnic communities reveals high levels of fear,16–18 worry or anxiety about dying which can inhibit a desire for palliative care. Fear can also inhibit discussions within communities or families about the potential death of a family member.8,12,19,20 Anxieties around end-of-life care are complicated by a prevailing distrust of written advance care plans and a lack of expression of preferences by the elders themselves.21–23 All these factors contribute to the difficulties encountered both by families and by health care teams when end-of-life care decision making is required in health care settings.
There is also a consistent desire by elders of Black and minority ethnic heritage and families for family-based decision making around health care decisions that can be in conflict with the prevailing model of individual autonomy.8,24 Many elders of Black and minority ethnic heritage express trust that their family, in the majority of cases this being their adult children, will make the right decisions when needed.12,19,20 However, poor congruency between the wishes of these elders and those of their children around end-of-life treatment preferences has been demonstrated.3,25 Assumptions that elders of Black and minority ethnic heritage have a preference for continued interventions have not been supported by research. 8
The complexities involved in achieving good dying among diverse populations has received much international attention over the past 15 years; however, the nature of the interactions and conversations that take place between elders and their adult children and the impact this has on subsequent end-of-life decision making has not been considered in depth. 1
Definitions
To ensure consistency with public body work in the United Kingdom and contemporary culture as portrayed by the main stream media, the term people of Black and minority ethnic heritage has been used in this work, however, with an acknowledgement of the limitations of such terms. One of the risks that need to be overcome when undertaking research with ethnic minorities is that assumptions about homogeneity may be made. 26 Ideas of identity are complex ones and there is now a greater respect for the issues it can bring for people labelled by others. 27
Over the last decade, there has been an increasing debate over the best way to define care given to improve the way people die, with particular disparities around the terms palliative and end of life.28,29 For the purpose of this review, end of life was defined as the time when people are considered to be in the last 6 months of life, acknowledging this timing can be difficult to predict. End-of-life conversations refer to conversations regarding preferences around place of care, decisions about end-of-life care interventions and important end-of-life rituals. Care decision making can refer to decisions made by people for themselves or made by proxy decision makers when that person has lost the capacity to make decisions for themselves due to their deteriorating ill health. 30
The review
Selecting meta-ethnography and getting started
The aim of this review was to explore the views articulated by elders of Black and minority ethnic heritage and their children about having end-of-life conversations within the family. Meta-ethnography was chosen as the method to enable an in-depth exploration and greater understanding of prospective family conversations around end of life. The process of meta-ethnography aims to facilitate a greater understanding of a social phenomenon by synthesising the findings of qualitative studies retaining the rich context of the data through a seven-stage synthesis process (Table 1).31,32 It is designed to develop new overarching concepts and theories with an emphasis on preserving original contexts within the synthesis of data from multiple studies. 33
Process of meta-ethnography.
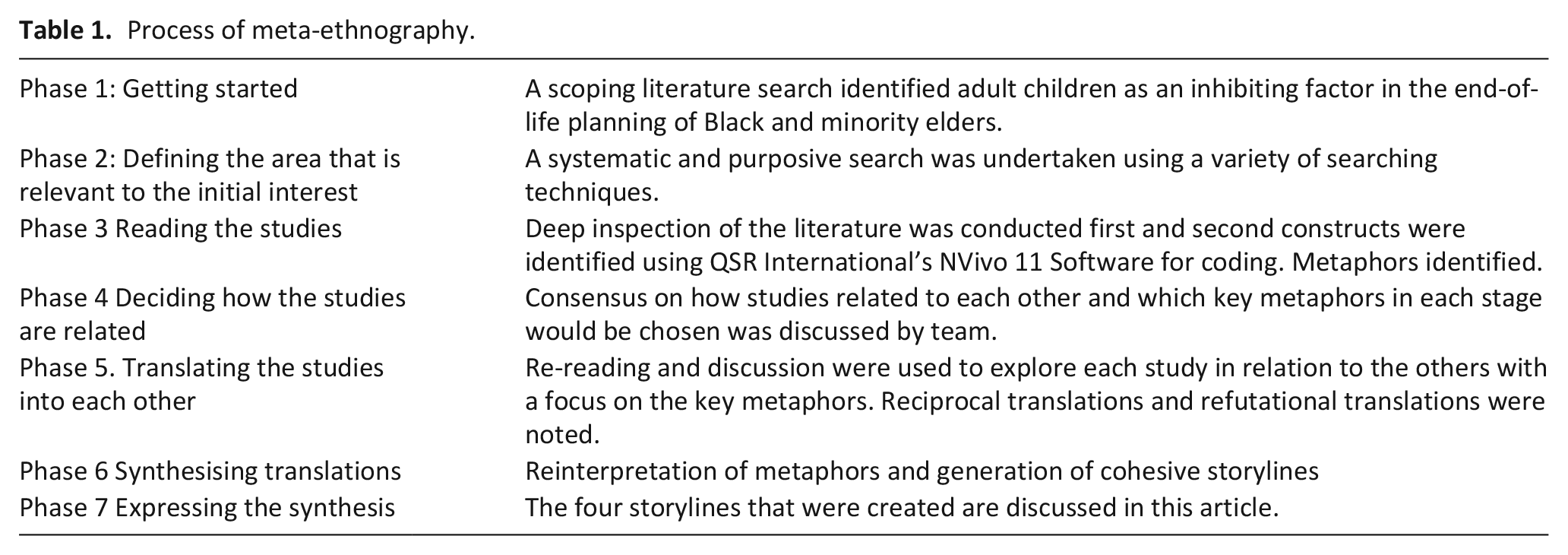
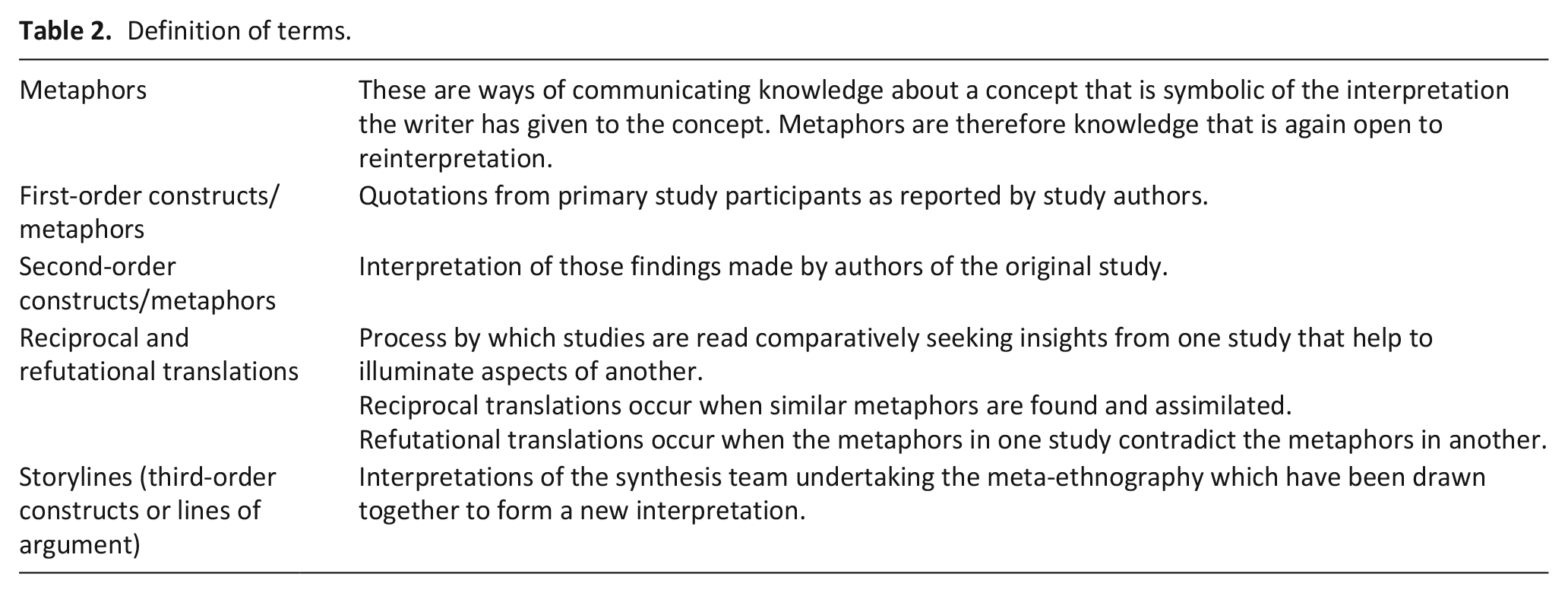
The data in existing studies consist of two forms: first- and second-order metaphors (see Table 2 for definition). A collaborative process of discussion of these metaphors was undertaken by the review team to seek links and translations between the studies being explored. The final stage involved developing overarching lines of understanding called lines of argument or storylines as a review team with an overall aim to develop new understanding rather than new knowledge.34,35
Definition of terms.
This collaboration aims to be reflexive with an acknowledgement of the inherent culturally laden assumptions that each reviewer brings to the process of interpretation. The interpretations are open to further discussion and debate by the reader. 34
The main purpose of this review is to increase the understanding of the ways some families of Black and minority ethnic heritage operate around end-of-life conversations. It is hoped that the findings of the review will help to identify ways of engaging people of Black and minority ethnic heritage to think about strategies to enable better awareness of each other’s preferences at end of life. An additional purpose of this review is to increase professionals’ understanding of end-of-life communication in and with Black and ethnic minority families. The following aim and review questions were formulated.
Review aim
The aim of this study was to develop a deeper understanding of the perspectives of elders of Black and minority ethnic heritage and their children, about end-of-life conversations that take place within the family, using a meta-ethnographic approach.
Review questions
How do older people of Black and minority ethnic heritage describe their experiences of having end-of-life conversations with their adult children?
How do children of elders of Black and minority ethnic heritage describe their experiences of having end-of-life conversations with their parents?
What influences do these experiences have on the way these elders feel and think about initiating discussions about their end-of-life preferences?
Deciding what is relevant
Search strategy
CINAHL, MEDLINE, PubMed and PsycINFO databases were searched for articles from 2005 to 2019; 2005 was used as a starting point as Jones 36 in the United Kingdom and Kwak and Haley 37 in the United States both published reviews of the current state of literature exploring ethnic differences in end-of-life experiences. Key words were matched to MeSH terms (Table 3). Seven studies were identified.
Search terms – facet analysis.
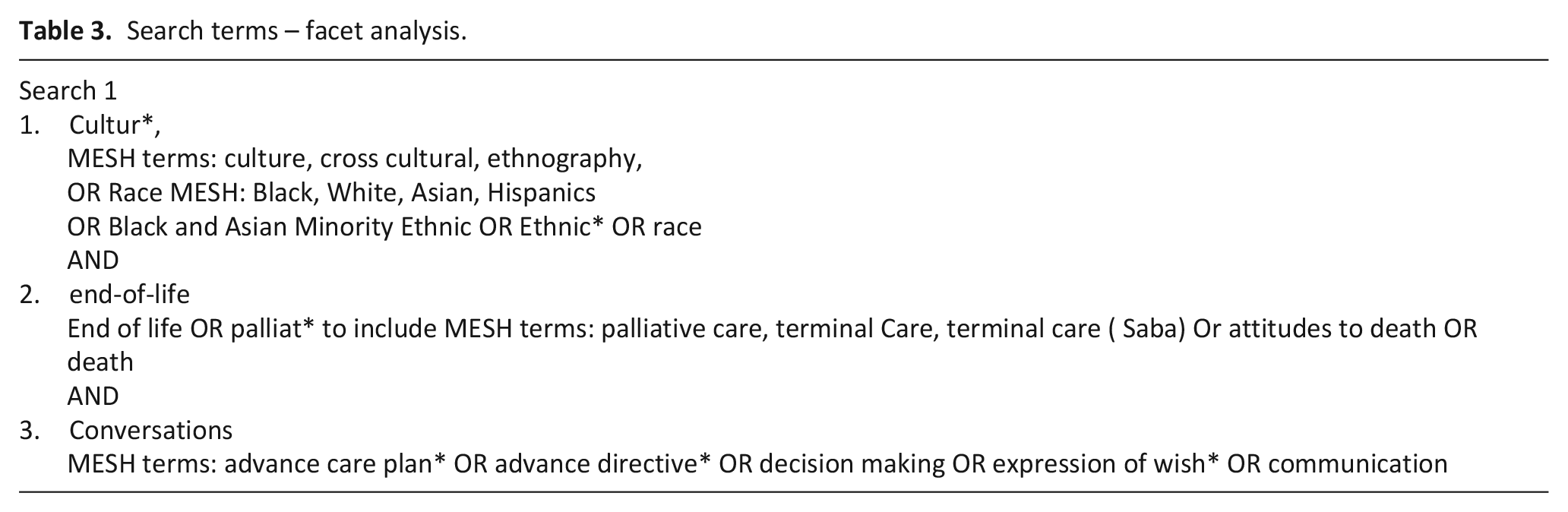
Generating a useful search was complex with search terms such as ‘adult children’ and minority generating large volumes of irrelevant hits. We found the most effective ways of choosing ethnicities to search was to use the term RACE which gave the MeSH headings of Black, White and Asian. We also included Hispanics as so many studies are done in the United States with this group. An analysis of all the MeSH terms linked to the initial 14 studies found by all types of searching was conducted; however, this identified that the chosen studies did not share any MeSH identifiers beyond generic terms such as human.31,38 Two of the main studies in this area39,40 had no MeSH headings associated with ethnicity, and Yonachiro-Cho had no end-of-life MeSH terms. Qualitative studies are not always identified by traditional search methods such as MeSH identifiers. Creative and purposeful searching is required. Citation snowballing 41 and information foraging 42 including Google Scholar searching were also employed to identify a further eight studies that fitted the inclusion criteria (PRISMA flow diagram; Figure 1). In total, 15 studies were selected for quality appraisal.
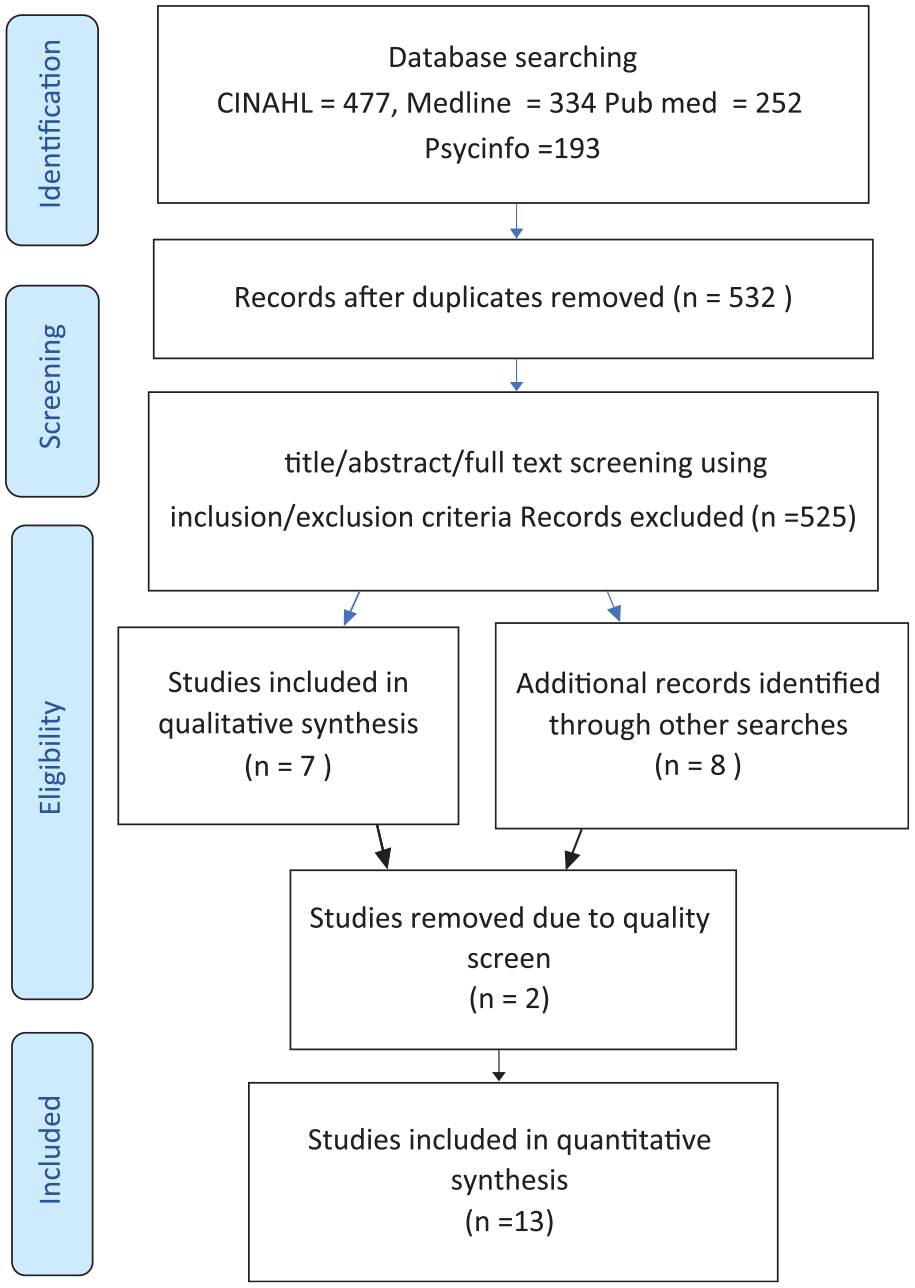
PRISMA 2009 flow diagram.
Study selection
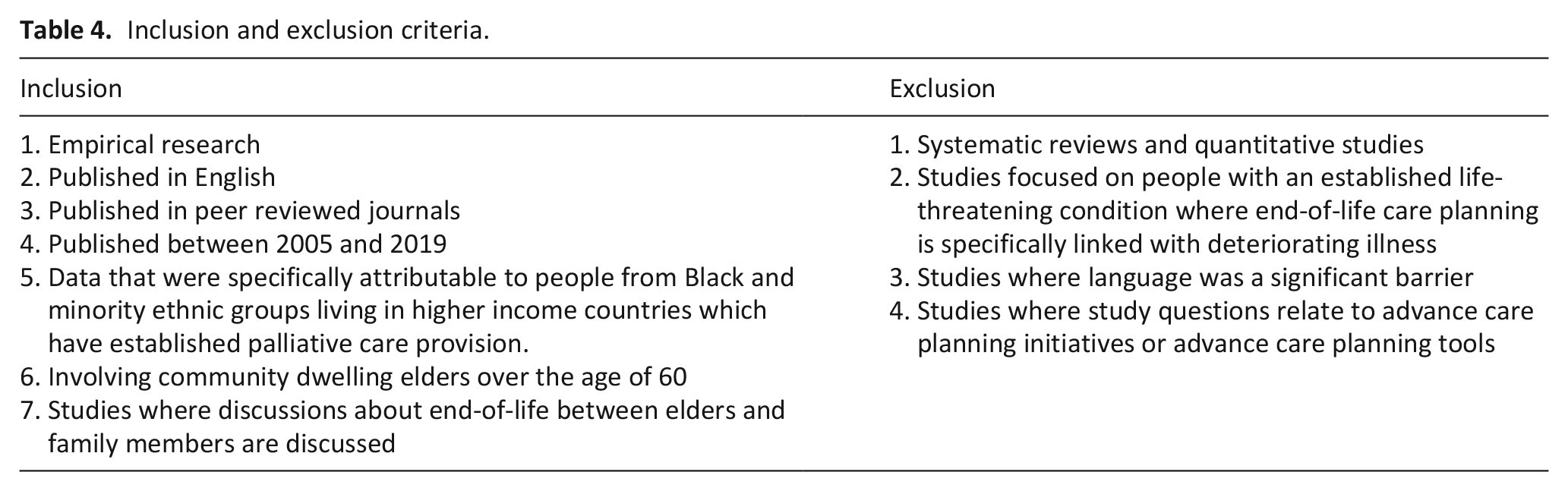
Studies that had a focus on conversations about end-of-life planning between elders and their adult children were included. Inclusion and exclusion criteria were applied (Table 4).
Inclusion and exclusion criteria.
Assessment of quality
The papers selected were assessed for quality using the critical synthesis form for qualitative studies, which is an adapted form of Critical Appraisal Skills Programme (CASP); 43 the scores were included in the data analysis table (Table 5). 52 Two UK-based studies were excluded at this point as they were written up as reports and did not contain enough details on methodology or results to be assessed and used.53,54 Thirteen studies were included in the synthesis.
Included studies.
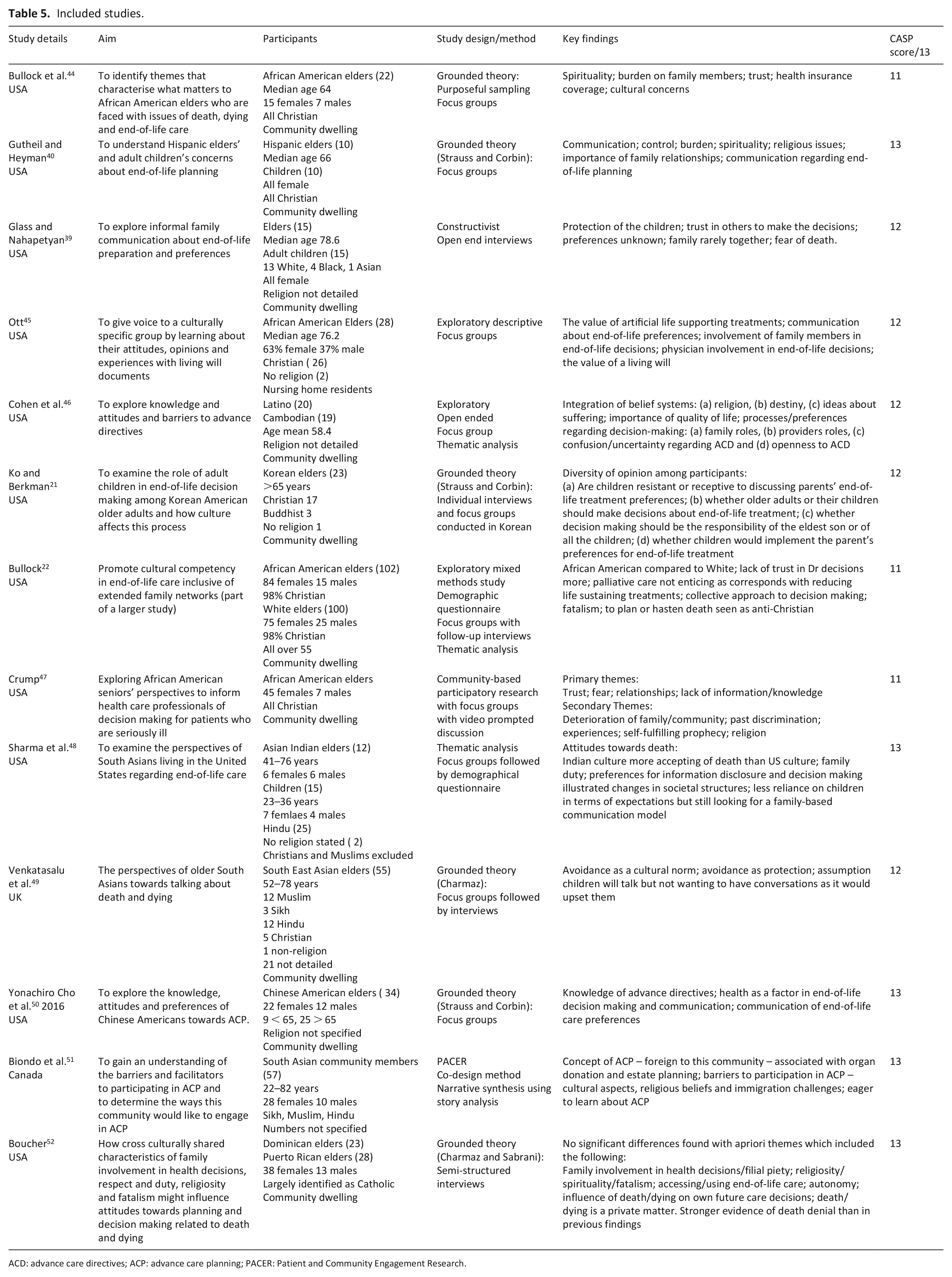
ACD: advance care directives; ACP: advance care planning; PACER: Patient and Community Engagement Research.
Reading the studies
Data extraction and synthesis
A data extraction form informed by the work of Campbell et al. 31 was used and results tabulated in chronological order (Table 5). Noblit and Hare 34 suggest reading should be in the form of deep introspection of the literature, exploring both the narrative patterns and also the meanings that are created in the mind of the reader. A more detailed data extraction table of the first- and second-order metaphors, using QSR International’s NVivo 11 Software, 55 was conducted by J.D.S. and developed through discussion between the members of the review team (Supplemental Table 7).
Determining how the studies are related
A decision was taken to focus on the first-order metaphors (direct reports from study participants) to explore the conversations and experiences expressed in the studies as they offered rich insights into the experiences of the participants. 52 First-order metaphors had been widely used to illustrate the findings of the original studies by the study authors, as a result there were limited second-order metaphors (author interpretations) developed. The second-order metaphors were included where they offered further insights.
Translating the studies into each other
Review team discussions, using a concept mapping process, enabled the process of translations. Contextual notations helped to elucidate patterns that were more represented by particular ethnic groups or in particular geographical locations. An example of this was the difference in attitude towards healthcare professional instigated advance care planning. There was more distrust of the system in the United States than in other countries, and attitudes towards advance planning were more positive in south East Asian heritage in the United States and Canada where educational levels were higher. These differences allowed for both reciprocal translations and refutable translations to take place (Supplemental Table 7).
Findings
Synthesising translations
Following the process of translation, overarching lines of argument or storylines were suggested by members of the review team. The studies were re-read as whole to consider what new interpretations were congruent with the primary data. Noblit 35 describes these as a new storyline which offers a new overarching interpretation of what is being related by the original study participants. Final extrapolation of the storylines took place following further discussion by the review team (Table 6).
Storylines.

The storylines
The storylines illustrated first the role elders envisioned their children will play in end-of-life decision making ‘My family will carry out everything for me; it is trust’. The second aspect was the perception that adult children inhibit end-of-life planning conversations: ‘No Mum, don’t talk like that’. The third was the sense of fatalism often associated with religious beliefs: ‘I leave it in God’s hands’. The fourth is the recognition of change and realisation that things may need to be done differently: ‘Who’s going to look after us?’ These storylines are explored below.
Storyline 1 ‘My family will carry out everything for me; it is a trust’: trust, dependence and importance of family
Elders in all of the studies expressed perceptions of the centrality of family in end-of-life decisions. The metaphor – ‘my family will do right by me’ – captured the sense of trust these elders had in their children’s role as carers and decision makers for them at the end of life and the assumption that their children would be proxy decision makers for them ‘when the time comes’. There was often no mention of spouses playing this decision-making role.
8
This sense of trust was linked to the metaphor ‘Basically, you have to take care of me’. It came from traditionally held views that as they had cared for their parents, their children would do the same:
Yo te pari y tu tiene que cuidame a mi . . . basically, you have to take care of me. (Puerto Rican elder,
52
p. 360)
This sense of responsibility being taken to the point of complete dependence and a reluctance to accept outside carers is a feature found in other studies of Black and minority ethnic elders coping with severe illness:
There was a common understanding among families that if a family member became sick, . . ., the family/children would naturally take care of them: I told my doctor that I have kids who will take care of me and I am comfortable with them . . . I don’t need home care. (Canadian South East Asian elder,
51
p. 916)
In the studies of African American communities, there was less notion of familial responsibility, but more emphasis on community:
There was a sense of comfort in knowing that there would be people of their own race or ethnic group available to care for them during the time of death and dying. ‘Usually black people are all one . . . if you don’t belong to a church, then you have a friend’. (African American elder,
44
p. 12)
A sense that the children would know the right thing to do without any prior discussions was expressed both as first- and as second-order metaphors:
‘I did not have a specific conversation with them, but they know what I want’. ‘My people will take care of me. They know’. (African American elder,
45
p. 120)
On questioning, we found many of them did not have a conversation with their families about their own wishes:
Leader: Well, have you talked to them? No, but they know what is best for me. (Canadian South East Asian elder,
45
p. 120) When anyone in the family is faced with a difficult situation, everyone intuitively knows what their role is and what to do, and then right decisions are just made without us planning ahead. (Canadian South East Asian elder,
51
p. 915)
This lack of discussion was a form of protection practised by both parties:
I don’t think people ask where you die. I think the family makes that decision, family would come forward to take responsibility and make any necessary decisions on behalf of their older relatives, and thus shelter their older relatives from topics perceived to be unpleasant. (Asian elder,
49
p. 399)
For some, this felt secure because it was in fitting with cultural expectations. However, what appears clear is these decisions by family members may be incongruent with the preferences of the elders themselves. Elders in seven of the studies expressed a preference for limiting life sustaining therapies at the end of life:
I don’t want those machines . . . if I am sick. (Hispanic elder,
40
p. 62)
Storyline 2. ‘No Mum, don’t talk like that’: burden and protection
This storyline offers insights from the experiences of these elders of the conversational dance that goes on between elders and their adult children, each looking to protect the other from what they perceive to be difficult burdens. There was an interesting mix of some elders not wishing to burden their children with end-of-life conversations and those not wanting to burden them with end-of-life decisions. In the two studies which included adult children’s perspectives,39,40 the children spoke of not wanting the burden of their parent’s end-of-life decision making. Several of the study authors,21,40,44,47,49,52 discussed this notion of burden and protection to be one of the most influential factors in conversations with children about end-of-life care planning.
A resonating metaphor in this storyline of protection and burden was the role adult children play, in limiting conversations about dying initiated by their elders or by others.3,21,22,40,39,57 Although Hispanic elders were comfortable to discuss end-of-life issues with their children, the responses they met was illustrated by the following:
They don’t want to hear us. (Hispanic elder,
40
p. 62)
This culture of inhibiting conversations was prevalent in many of the studies, across different ethnic groups:
When I tried to talk about this topic, my children were not willing to listen to me. They said, ‘Mom, please do not talk about such things. They get angry when they hear me saying such things’. (Korean elder,
21
p. 170) When I anticipate any unfortunate scenario, I am immediately told to shut up and not to dwell upon it. (Canadian South East Asian elder,
51
p. 916)
The elders felt the children did not want to have the conversations their parents were hoping for. An elder reported their child had expressly said,
No Mom don’t talk like that. (Hispanic adult child,
40
p. 62)
The child explained that it came from a fear of losing their parents:
We’re all educated, but we don’t want to talk about that [end of life] . . . Mom and Dad are not going to die. (Hispanic adult child,
40
p. 64)
One child suggested this reluctance to discuss dying was not just about facing the death of her parents but also linked to a cultural norm of avoiding conversations about dying:
may be a taboo across the generations. (Hispanic adult child,
40
p. 65) This is classic of the Latino family, the hiding. (Hispanic elder,
40
p. 62)
Adult children are not the only people reluctant to talk about dying to protect others from burden. The first-order metaphor ‘ If I tell them, they’re going to suffer; then I would suffer more seeing them suffer. (Hispanic elder,
40
p. 61)
This element of protection seemed to stem from three orientations. Avoidance as protection, 49 where the issue is protecting the children from having to think of these difficult things; avoidance as a cultural norm; 49 and finally a reluctance to play the role of a God who is viewed as the one who can give or take life and whose will cannot be known in advance.
In all nine of the studies where personal preferences regarding decision control were raised, elders felt that end-of-life decisions should be made by the patient. However, several participants based this preference on a desire to spare family members the emotional burden of having to make difficult end-of-life decisions rather than on a desire to promote patient self determination.
Storyline 3. ‘I leave it in God’s hands’: spiritual reassurance
When exploring what elders said about end-of-life decision-making responsibilities, many referred to their religious faith.22,39,40,44,46,51,52 African American, Hispanic and Cambodian elders frequently used spiritual references to characterise how they cope with illness and death.22,39,44,47,48 Their sense of faith was pervasive in their conversations:
You just have to put your faith in the Lord. (Hispanic elder,
44
p. 9)
For many, this was intertwined with a sense of divine control illustrated by this quote:
God would ‘take care of everything’. (Canadian South East Asian elder,
51
p. 916)
Some people expressed a more fatalistic view that life and death matters were beyond people’s own control so necessitated little formal decision making regarding the future:
I live in life’s terms. If it happens, it happens. (Latino elder,
52
p. 359)
Storyline 4. ‘Who’s going to look after us?’ Ambiguity and change
As part of the process of meta-ethnography, it is important to consider the metaphors that contradict the emergent storylines. These may be in the form of first-order metaphors or the more interpretive second-order metaphors. This final storyline resonated against the general themes of the others. While elders talked of trust and faith in their children as their decision markers, in some cases there was an open acknowledgement that the children may not respect their wishes:
Even if I make a will indicating not to use life-sustaining treatment, there will be no one who will follow my will. Even if there is a will, they will all gather and discuss it together. (Korean elder,
23
p. 174)
One elder explains how this incongruence was not a major problem:
I don’t think we can force them to simply follow what we wish just because we want them to. We also have to consider their wishes. If children try their best, but parents die, there is nothing they can do about it. However, if we die because they turned the ventilator off because we asked them to do it, I think they will regret what they did after we die. They might think, I should have made more efforts to save my parents’ lives. (Korean elder,
21
p. 175)
An awareness of the complexity of reasons that wishes maybe questioned is captured by this second-order story:
One elder said her sister blamed her brother for carrying out their father’s wishes. Her sister went all the way to their brother’s house ‘saying that he killed our father’. (Hispanic elder,
40
p. 64)
These elders demonstrate a clear awareness of the complexities of this difficult work of end-of-life decision making and many seemed comfortable with this potential incongruence with their own stated wishes.
In most studies, an awareness that immigration and changing times might change cultural traditions was apparent. This was strongest in the South Asian heritage where there was more of an awareness of the cultural assimilation that was taking place. These populations had higher levels of tertiary education so this may be an influencing factor.
51
In the earlier studies, there is a brief acknowledgement of why things are changing with geographical reasons for the families not living so close to each other:
Family rarely together. (African American elder, p. 4) They’re not around much, but I told them. (African American elder living in a care home,
45
p. 120)
In the later studies, it is discussed more descriptively:
But then we have also expectations when we grow old and if we are in that situation. ‘Who’s going to look after us?’ It’s very selfish for us to expect that our children will come or move closer to us just to take care of us. At the same time, we expect that they should be there when we need them. So it’s more like an issue of moving from India to the US. Like those questions will never come to my mind if I was in India. (Canadian Asian Indian elder,
48
p. 314) ‘Kids are different now’ and ‘they have their own lives’. (Latino elder,
52
p. 360)
Others acknowledged that they themselves need to change and adapt, but that this may be difficult:
It’s very selfish for us to expect that our children will come or move closer to us just to take care of us. At the same time, we expect that they should be there when we need them. (Latino elder,
48
p. 315)
There was a growing receptivity to planning around end-of-life decision making particularly as a result of having been exposed to a culturally sensitive explanation or demonstration of advanced care planning. Many of them had a wealth of ideas of how perhaps culturally sensitive advanced care planning education could reach people in these diverse communities:
Such a great thing we are doing by bringing this awareness and that more should be done. (Canadian South East Asian elder researcher,
51
p. 917) Maybe you can have . . . like you have diabetes class, maybe you want to have a class for this [advance care directives] where you get ten or twenty people in the same place with somebody who’s knowledgeable. (Cambodian elder,
46
p. 1430)
Discussion
Expressing the synthesis
The aim of this review was to gain a deeper understanding into the perspectives of elders of Black and minority ethnic heritage and their children about having family conversations around end-of-life issues. Although the review sought the views of both elders and their children, most of the studies found reflected the views of the elders. From their responses, four storylines were constructed. The storylines illustrated the dependence and desire to rely on family proxies for end-of-life decision making with an understanding that proxy decisions may not reflect elders’ own preferences: ‘My family will carry out everything for me; it is trust’. The second aspect was the role adult children play in inhibiting end-of-life planning conversations: ‘No Mum, don’t talk like that’. The third was a continued relationship with a spiritual sense of fatalism often associated with religious beliefs: ‘I leave it in God’s hands’. The fourth is the recognition of change and potential desire for doing things differently: ‘Who’s going to look after us?’
The storylines around the importance of family, the preference for informal rather than formal end-of-life planning and thoughts of planning being linked to religious views about God’s timing are themes that had been identified in previous systematic reviews.8,12,20,58 Reliance on and expectation of adult children to play a major role in end-of-life decision making is perhaps cross cultural.1,11 However, in these studies of elders of Black and minority ethnic heritage, the absence of demonstrable involvement of spouses may reflect a phenomenon found in some studies where children born in the host culture hold a better understanding of the underlying cultural language and rules and so become the cultural interpreter and tour guide through not only the health system but also other societal processes. Facilitating more family-based conversational processes may need to be more creative than only occurring when family members can attend face-to-face health care appointments.
Protection is a major factor identified by elders of Black and minority ethnic heritage in these studies that prevents early end-of-life conversations. Elders want to protect their children from having to think about these difficult things such as the idea of their parent dying. In many cases, this is not an unfounded worry as when they raise the topic of their lives coming to an end with their children, they report the authoritative manner in which the children themselves close down those conversations. The interactions taking place here and the perspectives of both elders and children have been only sparsely explored with only one study indicating the burden this can then become for the children concerned. 39 Further research work is needed in this area in different cultural contexts to explore how anxiety around end-of-life conversations can be reduced.
Religiosity is a complex factor in relation to preparation for dying. In her review, Johnson et al. 59 found significant emotional distress regarding the acceptance of death in spiritual leaders and parish visitors in African American communities in the United States and suggest that ‘health care providers should not be surprised when the same person views death as a transition to a better life and as something to be avoided by obtaining medical interventions’ (p. 146). Spiritual fatalism that is accompanied by limited health literacy – particularly around serious illness and palliative care – plays alongside a sense that God is in control and will provide the support that is needed negating the need for anticipatory conversations. 60 Further research is needed to understand how religious communities explore end-of-life preparation and how work with leaders in these communities can be used to build better dying, rather than faith practices acting as barriers.
The fourth storyline captures a refutable metaphor. 34 This storyline of ‘Who’s going to look after us?’ changes direction from ideas expressed in the majority of studies and offers a sense of change in the perspectives of elders as they undergo a process of acculturation 61 into the prevailing majority cultures and start to see the role the children will play in their future care changing. This is a theme starting to emerge in many of the studies particularly in South East Asian cultures.11,62 The storyline of an expectation of children caring for their parents fully as they age is changing to being one where parents are becoming concerned about the burden this may place on those children and one, they want to avoid. Gott et al. 63 in their quantitative study with older people from a Maori heritage raises the need for a greater understanding of this changing storyline and for the development of culturally appropriate end-of-life care planning support.
People from Black and minority ethnic heritage appear to respond poorly to generic end-of-life planning initiatives through the media or governmental institutions. However, those who had been exposed to specifically targeted culturally adapted education demonstrated a desire for engaging with more formal ways of documenting preferences and initiating discussions.48,51,52,55 There is a need to develop a more co-operative and culturally resonant way of approaching the subject of end-of-life and how communities understand the challenges and opportunities and would wish to respond in ways that may be most effective for them. 64
What this synthesis adds
This synthesis offers an insight into the background of the prevailing preferences held by elders of Black and minority ethnic heritage and what appears to be a reluctance to discuss end-of-life issues within the family. A complex interplay between avoidance as protection 49 and a spiritual assurance of a world view that one’s children will be there to make the right decisions and that God has a plan shape the resultant silence. This insight can guide a more culturally sensitive approach to how to empower elders of Black and minority ethnic heritage and their adult children to engage in end-of-life conversations prior to situations where a serious deteriorating illness makes these types of conversations often more emotionally difficult.
The role that adult children play in shaping end-of-life conversations with their elders has emerged as a significant factor that merits further exploration. Understanding these dynamics is an important priority in helping to improve the current inequalities that existing in the achievement of enabling good dying across all communities.
Finally, the synthesis provides a clearer picture of the increasing receptivity of elders of Black and minority ethnic heritage to education initiatives around advance care planning as they recognise the need to be more self reliant as they age and face end-of-life issues.54,55
Limitations of the review
Methodologically, the literature searching for qualitative studies has been demonstrated to be challenging using online databases.42,44,53 Although multiple searches were conducted, some studies may have been missed. In addition, the processes of translation of studies are complex 65 and reflexive. As this is an iterative and interpretive piece of work, the studies chosen and the ways in which metaphors were selected are reflective of the interests of primarily the first reviewer who led the process but moderated by the review team. 34 Evaluating the integrity and reliability of meta-ethnographies has been limited so far. The use of EMERGE reporting guidelines for metathnographies 66 should help to enhance clarity of reporting and inclusion of the aspects important to the process. These guidelines were considered in the writing up of this meta-ethnography.
Conclusion
This meta-ethnography indicates the potentially inhibitory influence of adult children in the preparatory end-of-life decision making of their parents, particularly in Black and minority ethnic communities. It demonstrates the complexities of this influence when those children become the primary decision makers for their parents who are dying. It has explored a number of the reasons why there has been little discussion of the older person’s preferences, and the whole situation invokes a high level of anxiety for those adult children. Culturally curated education has been found to be helpful. Further exploration of what this might look like is needed, and how this may be also targeted at a range of family members. Understanding the perspectives and experiences of adult children of people from Black and minority ethnic heritage about having end-of-life conversations may be a useful next step in developing this work.
Supplemental Material
table_7 – Supplemental material for Perspectives of elders and their adult children of Black and minority ethnic heritage on end-of-life conversations: A meta-ethnography
Supplemental material, table_7 for Perspectives of elders and their adult children of Black and minority ethnic heritage on end-of-life conversations: A meta-ethnography by Joanna De Souza, Karen Gillett, Katherine Froggatt and Catherine Walshe in Palliative Medicine
Footnotes
Authors’ contribution
This expression of synthesis was written by JDS with contributions from the review team, KG, CW and KF. All authors have made a substantial contribution to the synthesis process and to the construction and review of this paper.
Data sharing
All the data used were from published studies that had themselves obtained ethical approval for their study dissemination.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This review was completed as part of a PhD at the Lancaster University, which has been supported by a Florence Nightingale Foundation Research Scholarship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.